

Abstract
Background:
Local anesthetic agents are more commonly used in dentistry to have painless procedure during surgical intervention in bone and soft tissue. There are many local anesthetic agents available with the wide selection of vaso-constrictive agents that improve the clinical efficacy and the duration of local anesthesia. Most commonly lignocaine with adrenaline is used in various concentrations. Systemically adrenaline like drugs can cause a number of cardiovascular disturbances while most are short lived, permanent injury or even death may follow in drug induced ventricular fibrillation, myocardial infarction or cerebro-vascular accidents. This study compared the efficacy and cardiovascular effects with the use of 2% lignocaine with two different concentrations.
Materials and Methods:
Forty patients underwent extractions of mandibular bilateral teeth using 2% lignocaine with two different concentrations - one with 1:80000 and the other with 1:200000.
Results:
There was no significant difference in the efficacy and duration with the 2% lignocaine with 2 different concentrations. 2% lignocaine with 1:80000 adrenaline concentration has significantly increased the heart rate and blood pressure especially systolic compared with the lignocaine with 1:200000.
Conclusion:
Though 2% lignocaine with 1:80000 is widely used in India, 1:200000 adrenaline concentrations do not much affect the cardiovascular parameters. So it is recommended to use 2% lignocaine with 1:200000 for cardiac patients.
Keywords: Adrenaline, inferior alveolar nerve block, lignocaine (2%), local anesthesia
Introduction
Local anesthetic agents are chemicals that reversibly block the transmission1 of action potential of nerve membrane. An essential pre-requisite to success in dentistry is to achieve good quality local anesthesia (LA). Local anesthetic agents are normally associated with absence of pain during surgical intervention in bone and soft tissue. There are many local anesthetic agents, lignocaine being the gold standard2 available with the wide selection of vaso-constrictive agents that improve the clinical efficacy and the duration LA.
Lignocaine diffuses readily through interstitial tissues and lipid rich nerves, giving rapid onset of action. Its vasodilating effect is more than that of prilocaine and mepivacaine.3 Adrenaline prolongs the duration as well as the depth of anesthesia. It is effective in preventing or minimizing blood loss during surgical procedures. Due to vaso-constrictive effects of adrenaline, absorption of LA and systemic toxicity are reduced. If adrenaline is not added to lignocaine, vasodilating effect of lignocaine limits pulpal anesthesia to only 5-10 min. 0.2 mg Adrenaline is a safe maximum dose in healthy patients and it is best to limit the total dose to 0.04 mg in cardiac patients. It should be kept to a minimum amount capable of producing adequate results. Adrenaline acts directly on both α and β-adrenergic receptors. Systemically adrenaline like drugs can cause a number of cardiovascular disturbances while most are short lived, permanent injury or even death may follow drug induced ventricular fibrillation, myocardial infarction or cerebro-vascular accidents.4
Purpose of the study
To compare the efficacy of 2% lignocaine with two different concentrations of adrenaline - 1:80000 and 1:200000.
To study the cardiovascular effects of LA with adrenaline in two different concentrations.
To recommend the ideal concentration of adrenaline to the elderly and ASA III and ASA IV risk patients with the history of cardiovascular problems.
Materials and Methods
Forty cases were selected randomly who needed extraction of bilateral mandibular teeth. Irrespective of the number of teeth extracted, inferior alveolar and lingual nerve blocks were administered (long buccal whenever necessary). Unilateral extractions were carried out in a single sitting and the other side was done on next visit. All the cases were carried out by a single operator. The patients who had any systemic illness like hypertension, cardiac problems and diabetes etc. were excluded from the study.
The following data were collected during the procedure:
Time of administration of LA,
Onset of anesthesia noted as subjective and objective symptoms (Subject: tingling and numbness in the lower lip and tongue, Objective: absence of pain on instrumentation).
Amount of LA used.
Pulse rate and blood pressure (BP)were recorded using automated multi-nodular monitor - Before the administration and immediately, 10 mins, 30 mins and 60 mins.
Evaluation of analgesia was done by the operator as successful, partial success and failure.
Intra operatively pain was scored on visual analogue scale (VAS)5 as reported by the patient. The VAS was presented in the form of a printed ruler numbered 0-10.
Any sign of systemic toxicity was recorded.
Results and Statistical Analysis
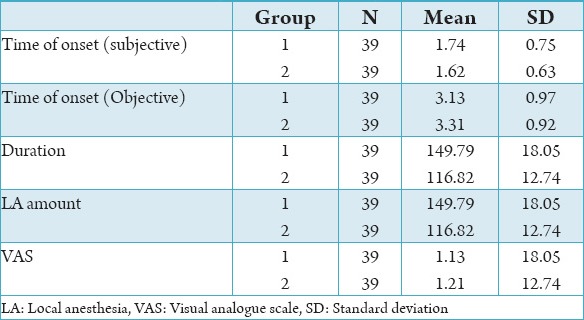
Safety and efficacy of the two solutions with two different concentrations of adrenaline were studied in 40 patients. The age varied from 18 to 80 while the mean age is 47. There were 23 males and 17 females. There was one case of anesthetic failure for both solutions. No systemic toxicity was observed. As observed in the Table 1 and Graph 1, there was no significant change in both the groups in the point of view of time of onset. With regard to the duration of action of LA, 1:80000 adrenaline concentrations showed more than that of 1:200000. This is due to the faster absorption of LA when used with less concentration of adrenaline. The amount of LA used for both the groups does not show any significant change. As shown in the Table 1, there was no change in the VAS scale as both the solutions had same efficacy.
Table 1.
Time of onset, duration, amount of LA used and pain (VAS) comparison in two groups.
Graph 1.
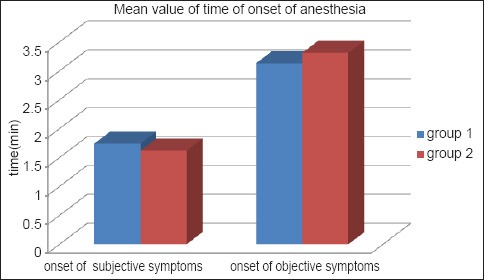
Comparing the onset of anesthesia in two groups subjectively and objectively.
There was significant rise in the pulse rate immediately when LA with 1:80000 adrenaline concentrations was used and it came to the normal gradually after 60 min as seen in the Graph 2.
Graph 2.
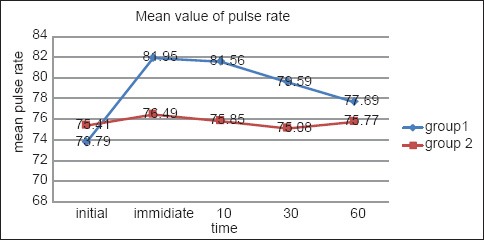
Variations in pulse rate.
But when LA with 1:200000 adrenaline concentrations was used, there was no significant rise in the pulse rate. While assessing the systolic BP, there was rise significantly when LA with 1:80000 adrenaline concentrations was used whereas there was no major change observed when LA with 1:200000 was used as shown in Graph 3. There was slight rise in diastolic BP when LA with 1:80000 adrenaline was used but there was decrease when LA with 1:200000 adrenaline concentration as seen in the Graph 4.
Graph 3.
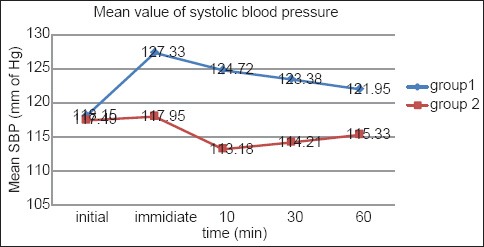
Comparison of systolic blood pressure.
Graph 4.
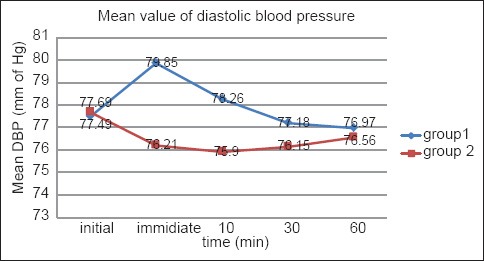
Comparison of diastolic blood pressure.
Discussion
Though there are many LA agents available in the market, lignocaine is the most widely used in dentistry. Most of the time, LA agents are used with vasoconstrictors, though the concentrations may vary. The presence of a vasoconstrictor in the anesthetic cartridge has a major influence on the duration of anesthesia.6 The ability of vasoconstrictors to retard the systemic absorption of injected LA agents is the basis for their widespread use.4 Vasoconstrictors employed in local anesthetic solutions have the potential for interacting with the wide variety of drugs.7 Physiological responses associated with local anesthetic solutions containing a vasoconstrictor have included changes in heart rate and BP, dysarrythmias, ischemic changes (ST segment and T wave), the release of endogenous catecholamines, endocrine response to surgery and hypokalemia.8 Local aesthetic agents with adrenaline as the vasoconstrictor used for the surgical soft tissue and bone interventions in the oral region tend to cause more post-operative pain than LA without adrenaline as the vasoconstrictor.9
In our study, comparison of two different concentrations of adrenaline is evaluated (efficacy as well as cardiovascular effects). The efficacy of both the solutions is not significantly different. So the epinephrine concentration does not affect the clinical efficacy of local anesthetic agent as reported by the study conducted by Santos et al. and Dagher et al.10,11 The time of onset of anesthesia as well as the amount of LA used in our study is similar to the study conducted by Malamed et al.12
Significant cardiovascular effects were observed in the study as seen in the statistical analysis, there was significant rise in the mean pulse rate when 1:80000 adrenaline used whereas no significant change observed in 1:200000 used. There was significant rise in the systolic and diastolic BP when LA with 1:80000 adrenaline used while 1:200000 adrenaline did not bring any significant change. Elad et al. (2001)demonstrated significant cardiovascular changes 10 mins after the injection of lidocaine with the higher adrenaline concentration of 1:80000.8 Gregorio et al. has reported after his study that it is important to stress that with articaine and other local anesthetic solutions in general, 1:100000 and 1:50000 epinephrine concentrations are associated with greater cardiovascular stimulation than 1:200000 epinephrine formulations.13
For an adult healthy patient, LA with any of the concentration of adrenaline can be used as the efficacy is not altered in both the solutions. But in elderly and cardiac patients, LA with 1:200000 adrenaline concentration is preferred. Since the duration of anesthesia is significantly different for both the solutions, LA with 1:80000 is preferred in case of long procedure. For hypertensive patients, some physicians advise LA without adrenaline but LA with 1:200000 could be used taking the advantage of adrenaline and avoiding complications as the adrenaline concentration is insignificant.
Conclusion
The present study of two types of 2% lignocaine with two different concentrations showed that both of them have the same efficacy. Coming to the cardiovascular effects, 1:80000 adrenaline concentrations showed significant rise in pulse rate as well as BP as compared with the other drug. For the cardiac and elderly patients, 1:200000 adrenaline concentration is recommended as it showed better cardiac stability. When treating any patient taking medication, one should be aware of the potential medical complications and always use the least concentrated solution of vasoconstrictor that allows for deep anesthesia during a period of time. LA with a lower concentration of adrenaline will not compromise the profundity and success of anesthesia and would be safe for this group of patients.
Footnotes
Conflicts of Interest: None
Source of Support: Nil
References
- 1.Caviedes-Bucheli J, Rojas P, Escalona M, Estrada A, Sandoval C, Rivero C, et al. The effect of different vasoconstrictors and local anesthetic solutions on substance P expression in human dental pulp. J Endod. 2009;35(5):631–3. doi: 10.1016/j.joen.2008.12.020. [DOI] [PubMed] [Google Scholar]
- 2.Kanaa MD, Whitworth JM, Corbett IP, Meechan JG. Articaine and lidocaine mandibular buccal infiltration anesthesia: A prospective randomized double-blind cross-over study. J Endod. 2006;32(4):296–8. doi: 10.1016/j.joen.2005.09.016. [DOI] [PubMed] [Google Scholar]
- 3.Malamad SF. Handbook of Local Anesthesia. 4th ed. St. Louis: Mosby-Year Book; 1997. [Google Scholar]
- 4.Yagiela JA. Adverse drug interactions in dental practice: Interactions associated with vasoconstrictors. Part V of a series. J Am Dent Assoc. 1999;130(5):701–9. doi: 10.14219/jada.archive.1999.0280. [DOI] [PubMed] [Google Scholar]
- 5.Haase A, Reader A, Nusstein J, Beck M, Drum M. Comparing anesthetic efficacy of articaine versus lidocaine as a supplemental buccal infiltration of the mandibular first molar after an inferior alveolar nerve block. J Am Dent Assoc. 2008;139(9):1228–35. doi: 10.14219/jada.archive.2008.0338. [DOI] [PubMed] [Google Scholar]
- 6.Hersh EV, Hermann DG, Lamp CJ, Johnson PD, MacAfee KA. Assessing the duration of mandibular soft tissue anesthesia. J Am Dent Assoc. 1995;126(11):1531–6. doi: 10.14219/jada.archive.1995.0082. [DOI] [PubMed] [Google Scholar]
- 7.Yagiela JA, Duffin SR, Hunt LM. Drug interactions and vasoconstrictors used in local anesthetic solutions. Oral Surg Oral Med Oral Pathol. 1985;59(6):565–71. doi: 10.1016/0030-4220(85)90181-1. [DOI] [PubMed] [Google Scholar]
- 8.Elad S, Admon D, Kedmi M, Naveh E, Benzki E, Ayalon S, et al. The cardiovascular effect of local anesthesia with articaine plus 1: 200,000 adrenalin versus lidocaine plus 1: 100,000 adrenalin in medically compromised cardiac patients: A prospective, randomized, double blinded study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105(6):725–30. doi: 10.1016/j.tripleo.2008.02.005. [DOI] [PubMed] [Google Scholar]
- 9.Hanvold KI, Vigen EC, Jorkjend L, Aass AM, Skoglund LA. Increase in volume of dental local anaesthetic solution while maintaining the tissue lidocaine and adrenaline concentration does not increase acute postoperative pain after gingivectomy. Br J Oral Maxillofac Surg. 2008;46(3):218–22. doi: 10.1016/j.bjoms.2007.10.004. [DOI] [PubMed] [Google Scholar]
- 10.Santos CF, Modena KC, Giglio FP, Sakai VT, Calvo AM, Colombini BL, et al. Epinephrine concentration (1: 100,000 or 1: 200,000)does not affect the clinical efficacy of 4% articaine for lower third molar removal: A double-blind, randomized, crossover study. J Oral Maxillofac Surg. 2007;65(12):2445–52. doi: 10.1016/j.joms.2007.04.020. [DOI] [PubMed] [Google Scholar]
- 11.Dagher FB, Yared GM, Machtou P. An evaluation of 2% lidocaine with different concentrations of epinephrine for inferior alveolar nerve block. J Endod. 1997;23(3):178–80. doi: 10.1016/S0099-2399(97)80271-3. [DOI] [PubMed] [Google Scholar]
- 12.Malamed SF, Gagnon S, Leblanc D. Efficacy of articaine: A new amide local anesthetic. J Am Dent Assoc. 2000;131(5):635–42. doi: 10.14219/jada.archive.2000.0237. [DOI] [PubMed] [Google Scholar]
- 13.Gregorio LV, Giglio FP, Sakai VT, Modena KC, Colombini BL, Calvo AM, et al. A comparison of the clinical anesthetic efficacy of 4% articaine and 0.5% bupivacaine (both with 1: 200,000 epinephrine)for lower third molar removal. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106(1):19–28. doi: 10.1016/j.tripleo.2007.11.024. [DOI] [PubMed] [Google Scholar]