

Abstract
Purpose
Kienbock's disease is considered a “rare disease” and currently affects less than 200,000 people in the U.S. Given the inherent challenges associated with researching rare diseases, the intense effort in hand surgery to treat this uncommon disorder may be susceptible to publication bias in which positive outcomes are preferentially published. The specific aim of this project is to conduct a systematic review of the literature with the hypothesis that publication bias is present for the treatment of Kienbock's disease.
Methods
We conducted a systematic review of all available abstracts associated with published manuscripts (English and non-English) and abstracts accepted to the 1992-2004 American Society for Surgery of the Hand (ASSH) annual meetings. Data collection included various study characteristics, direction of outcome (positive, neutral/negative), complication rates, mean follow-up time, time to publication, and length of patient enrollment.
Results
Our study included 175 (124 English, 51 non-English) published Kienbock's manuscripts and 14 Kienbock's abstracts from the 1992-2004 annual ASSH meetings. Abstracts from published manuscripts were associated with a 53% positive outcome rate, which is lower than the 74% positive outcome rate found among other surgical disorders. Over the past 40 years, studies have become more positive (36% to 68%, p = 0.007) and are more likely to incorporate statistical analysis testing (0% to 55%, p <0.001). Of the 14 abstracts accepted to ASSH, 11 (79%) were published in peer-reviewed journals. Ten of the 14 accepted abstracts (71%) were considered positive, and there was no significant difference in publication rate between studies with positive (n = 10) and non-positive (n = 4) outcomes (p = 1.000).
Conclusions
The acceptance rate for negative outcomes studies regarding Kienbock's disease is higher than for other surgical disorders. This may indicate a relative decrease in positive outcome bias among published Kienbock's studies compared to other surgical disorders. However, the increasing positive outcome rate for published Kienbock's studies over time may suggest a trend of increasing publication bias among journals toward Kienbock's studies.
Keywords: Kienbock's disease, systematic review, publication bias
Kienbock's disease, or avascular necrosis of the lunate, is classified as a “rare disease” by the Office of Rare Diseases (ORD) of the National Institutes of Health (NIH), and therefore affects less than 200,000 people in the U.S.1 Since the initial description of this condition by Robert Kienbock in 1910, surgeons have described over 20 different procedures aimed at treating this disease.2-4 The low prevalence and unclear etiology of Kienbock's disease present unique challenges with regards to conducting large, clinically meaningful comparative effectiveness trials. As a result, there is little evidence-based data to support any particular method of operative treatment, or to indicate their superiority over conservative measures.3 Thus, hand surgeons may be inadvertently driven to treat Kienbock's patients with procedures that have the most recent or prevalent data presented in the literature, rather than based on objective comparative outcomes.
Publication bias refers to the tendency of researchers, peer reviewers, and journal editors to submit or accept manuscripts for publication based on the direction or strength of study findings.5-6 This includes: 1) factors that influence the undertaking/performance of research (prepublication bias); 2) acceptance or rejection of an abstract/manuscript (publication bias), and; 3) acceptance or interpretation of previously published research as evidenced by citations in future research and inclusion in systematic reviews/meta-analyses (postpublication bias).6-8 The most serious potential consequence of publication bias at any stage would be overestimation of treatment effects or risk-factor associations in published papers that could lead to inappropriate decisions concerning patient management or health policy.9-11 Previous studies have demonstrated an association between positive outcomes, the presence of statistical significance, more advanced study design, study size, and increased likelihood of ultimate publication.9-17 Due to the limited number of individuals affected with Kienbock's disease and the inherent difficulties associated with conducting research for rare disorders, the intense effort in hand surgery to treat this uncommon condition may be susceptible to publication bias.
Although several studies have assessed publication bias in various surgical specialties, there is a lack of specific data evaluating publication bias within the field of hand surgery.9,13-16 The purpose of this study is to conduct a rigorous evaluation of all available literature regarding the surgical treatment of Kienbock's disease and identify potential areas of publication bias. Using data from published abstracts in both the English and non-English language, we will present a systematic review assessing study characteristics, quality of reporting, and direction of outcomes (positive or neutral/negative) for all published Kienbock's studies. In addition to our evaluation of published abstracts, we will collect the same data from abstracts presented at the 48th-60th annual scientific meeting of the American Society for Surgery of the Hand (ASSH; 1992-2004). By comparing the study characteristics and outcomes of unpublished abstracts to abstracts accepted for publication, we aim to determine factors that were positively or negatively associated with achieving ultimate publication.
Materials and Methods
Literature Search and Abstract Selection
Systematic searches of all available literature from the MEDLINE, EMBASE, and SCPOUS databases (1902-2009) were performed using the key words Kienbock, avascular necrosis, revascularization, and lunate. The resulting titles and abstracts were then screened to rule out non-primary, biomechanical, non-surgical, non-human, non-Kienbocks, anatomical, or diagnostic imaging studies. Studies evaluating pediatric patients or patients with concomitant joint, collagen, or vascular disease were also excluded. Relevant abstracts for analysis consisted of primary studies assessing outcomes for specific procedures used to treat Kienbock's disease. Abstracts containing multiple indications were included as long as the results for Kienbock's patients alone were able to be extracted. Due to the paucity of published research regarding Kienbock's disease, we included both English and non-English studies as long as the non-English studies contained a published English abstract.
In addition to our assessment of abstracts in published manuscripts, we also evaluated the same study characteristics and outcome parameters for abstracts accepted to the 48th to 60th annual scientific meeting of the ASSH (1992-2004). Abstracts prior to 1992 and abstracts from other hand conferences were not available for review. Publications corresponding to the accepted abstracts were identified through a computer search of the MEDLINE database using authors' names and key words from the title. We choose to review abstracts presented until the year 2004 based on previous research which demonstrated that over 90% of abstracts that will eventually lead to publication will publish within 5 years of abstract presentation.12
Data Extraction and Analysis
For each published manuscript and ASSH abstract included in our analysis, data regarding study characteristics (primary language, country of journal origin, study size), outcome direction (positive, negative, or neutral), and complications were collected. In addition, the following time-to-event information was collected for studies with available data: 1) length of patient enrollment, 2) mean follow-up time, and 3) time from completion of patient enrollment to publication. The presence of statistical analysis, designated by the presence of a p value (regardless of the value), was used as a crude indicator of study quality.
All manuscripts and abstracts were analyzed by two reviewers (L.S. and E.P.) with discrepancies resolved between each other by consensus. The results of each study were classified as positive, neutral, or negative. Positive outcomes were defined as present if the authors directly recommended a procedure or stated that the intervention was generally beneficial, irrespective of absolute outcome values or the presence of statistical significance; negative outcomes were defined as present when the authors advised against the intervention or presented only negative results; and neutral outcomes were defined by the absence of author recommendations or the presence of both positive and negative comments/results.13-16 For studies comparing more than one intervention for Kienbock's disease, outcomes were considered positive if the authors specifically recommended at least one of the procedures included in the study.
Statistical Analysis
Various categorical (primary language of study, country of study origin, procedure type, outcome, and presence of statistical analysis) and interval (number of Kienbock's wrists per study, complication rate, follow-up time, time to publication, and length of patient enrollment) data parameters were collected for each abstract. The statistical significance of relationships between categorical variables was evaluated using either chi-square tests (if all expected values were > 5) or Fischer's exact tests (if any expected value was ≤ 5). For comparison of mean interval data parameters, either a two-tailed t test (two groups) or analysis of variance (more than two groups) was performed. P values of less than 0.05 were considered statistically significant and all statistical analyses were performed using SAS statistical software (version 9.1; SAS, Cary, North Carolina).
Results
Published Kienbock's Abstracts
One thousand five hundred eighty seven citations were identified through the MEDLINE, EMBASE, and SCPOUS databases (Figure 1). Of the 253 relevant titles that underwent abstract review, 175 studies (124 English and 51 non-English) met all of our inclusion/exclusion criteria and formed the basis for our systematic review (Appendix A). Fourty-five articles were eliminated due to inextractable data for Kienbock's patients and thirty-three articles were eliminated because they lacked an associated English abstract. Although both English and non-English articles were primarily composed of studies from Europe (42% and 86%, respectively), English articles contained a greater proportion of studies from non-European countries (p < 0.001, Table 1). English articles were also more likely to include some form of statistical analysis (40% vs. 3%, p < 0.001, Table 1).
Figure 1. Flowchart of primary database search and data collection.

Table 1. Study Characteristics of Published Kienbock's Abstracts.
| Total Abstracts (n = 175) | English Article (n = 124) | Non-English Article (n = 51) | P Value | |
|---|---|---|---|---|
| Country of Journal Origin | <0.001δ | |||
| US | 63 | 63 (51%)† | 0 (0%)‡ | |
| Europe | 96 | 52 (42%)† | 44 (86%)‡ | |
| Asia | 12 | 8 (6%)† | 4 (8%)‡ | |
| Other | 4 | 1 (1%)† | 3 (6%)‡ | |
| Procedure Type* | 0.257ζ | |||
| Joint Leveling | 51 | 32 (25%)† | 19 (33%)‡ | |
| Implant/Transposition Arthroplasty | 36 | 26 (20%)† | 10 (17%)‡ | |
| Partial Wrist Fusion | 25 | 17 (13%)† | 8 (14%)‡ | |
| Vascular Bone Graft/Pedicle | 18 | 10 (8%)† | 8 (14%)‡ | |
| Salvage | 22 | 18 (14%)† | 4 (7%)‡ | |
| Other | 36 | 27 (21%)† | 9 (16%)‡ | |
| Overall Outcomes | 0.053ζ | |||
| Positive | 92 | 71 (57%)† | 21 (41%)‡ | |
| Neutral/Negative | 83 | 53 (43%)† | 30 (59%)‡ | |
| Mean Number of Wrists per Studyα | 19.8 | 18.8 | 22.3 | 0.415ε |
| Complication Rateβ | 17.7% | 17.0% | 22.7% | 0.435ε |
| Mean Follow-Up (months) γ | 71 | 68 | 83 | 0.276ε |
| Presence of Statistical Analysis | 52 | 50 (40%)† | 2 (4%)‡ | <0.001ζ |
| Time to Publication (years)π | 5.1 | 5.4 | 3.5 | 0.103ε |
| Length of Patient Enrollment (years) Ω | 10.0 | 10.4 | 7.3 | 0.117ε |
Data presented as number of English abstracts (% of total English abstracts)
Data presented as number of non-English abstract (% of total non-English abstracts)
For studies including more than one surgical procedure, separate entries were made for each procedure type
Only includes wrists corresponding to surgical Kienbock's patients
Data presented as the average complication rate for studies with available data; Reported in 78 of 124 English articles (63%) and 11 of 51 non-English articles (22%)
Data reported in 110 of 124 English articles (89%) and 30 of 51 non-English articles (59%)
Data presented as time from end of patient enrollment to publication; Reported in 75 of 124 English articles (60%) and 12 of 51 non-English articles (24%)
Data reported in 75 of 124 English articles (60%) and 12 of 51non-English articles (24%)
Statistical analysis using Fisher's exact test
Statistical analysis using two-tailed t-test
Statistical analysis using chi-square test
Overall, our data show that 53% of Kienbock's abstracts were associated with positive outcomes, which is much lower than the 74% positive outcome rate found among top orthopaedic and general surgery journals (Table 2).13 Positive outcomes were associated with lower complication rates (p = 0.006, Table 3) and increased presence of statistical analysis (p = 0.001, Table 3). We found no correlation between positive outcomes and study of journal origin (p = 0.071), primary language of article (p = 0.053), study size (p = 0.987), and mean follow-up time (p = 0.481, Table 3). Of note, we also found no statistically significant association between negative outcomes and increased time to publication (p = 0.747) or length of patient enrollment (p = 0.264), which has been suggested in previous research regarding publication bias.21
Table 2. Factors Associated with Positive Outcomes.
| Total Abstracts (n = 175) | Positive Outcomes (n = 92) | Non-Positive Outcomes (n = 83) | P value | |
|---|---|---|---|---|
| Country of Journal Origin | 0.071ε | |||
| US | 63 | 40 (43%)† | 23 (28%)‡ | |
| Europe | 96 | 45 (49%)† | 51 (61%)‡ | |
| Asia | 12 | 4 (4%)† | 8 (10%)‡ | |
| Other | 4 | 3 (3%)† | 1 (1%)‡ | |
| Language of Article | 0.053ε | |||
| English Article | 124 | 71 (77%)† | 53 (64%)‡ | |
| Non-English Article with English Abstract | 51 | 21 (23%)† | 30 (36%)‡ | |
| Mean Number of Wrists per Study α | 19.8 | 19.8 | 19.9 | 0.987δ |
| Complication Rate β | 17.7% | 12.4% | 25.8% | 0.006δ |
| Mean Follow up Time γ | 71.2 | 67.7 | 75.5 | 0.481δ |
| Presence of Statistical Analysis | 52 | 37 (40%) | 15 (18%) | 0.001ε |
| Time to Publication (years) π | 5.1 | 5.2 | 5.0 | 0.747δ |
| Length of Patient Enrollment (years)Ω | 10.0 | 10.8 | 9.0 | 0.264δ |
Data presented as number of positive abstracts (% of total positive abstracts)
Data presented as number of negative abstract (% of total negative abstracts)
Only includes wrists corresponding to surgical Kienbock's patients
Data presented as the average complication rate for studies with available data; Reported in 54 of 92 studies with positive outcomes (59%) and 35 of 83 studies with non-positive outcomes (42%)
Data reported in 78 of 92 studies with positive outcomes (85%) and 62 of 83 studies with non-positive outcomes (75%)
Data presented as time from end of patient enrollment to publication; Reported in 47 of 92 studies with positive outcomes (51%) and 40 of 83 studies with non-positive outcomes (48%)
Data reported in 47 of 92 studies with positive outcomes (51%) and 40 of 83 studies with non-positive outcomes (48%)
Statistical analysis using two tailed t-test
Statistical analysis using chi-squared test
Table 3. Outcomes, Complications, and Quality of Reporting According to Country of Journal Origin.
| US (n = 63) | Europe (n = 96) | Asia (n = 12) | Other (n = 4) | P value | |
|---|---|---|---|---|---|
| Overall Outcomes | 0.071δ | ||||
| Positive† | 40 (63%) | 45 (47%) | 4 (33%) | 3 (75%) | |
| Neutral/Negative† | 23 (37%) | 51 (53%) | 8 (67%) | 1 (25%) | |
| Mean Number of Wrists per Study‡ | 20.7 | 19.4 | 20.4 | 14.8 | 0.939ε |
| Complication Rate α | 12.3% | 24.3% | 7.6% | 0.1% | 0.067ε |
| Mean Follow-Up β | 73 | 72 | 55 | 66 | 0.894ε |
| Statistical Analysis Present† | 29 (46%) | 20 (21%) | 3 (25%) | 0 (0%) | 0.004δ |
| Time to Publication (years) γ | 5.8 | 4.5 | 5.4 | NA | 0.267ε |
| Length of Patient Enrollment (years) π | 11.6 | 8.1 | 12.3 | NA | 0.093ε |
Data reported as number of abstracts (% of total abstracts for given geographic region)
Only includes wrists corresponding to Kienbock's patients
Data presented as the average complication rate for studies with available data; Reported in 42 of 63 US studies (67%), 42 of 96 European studies (44%), 3 of 12 Asian studies (25%), and 2 of 4 studies published in another country (50%)
Data reported in 59 of 63 US studies (94%), 68 of 96 European studies (71%), 9 of 12 Asian studies (75%), and 4 of 4 studies published in another country (100%)
Data presented as time from end of patient enrollment to publication; Reported in 38 of 63 US studies (60%), 42 of 96 European studies (44%), 7 of 12 Asian studies (58%), and 0 of 4 studies published in another country (0%)
Data reported in 38 of 63 US studies (60%), 42 of 96 European studies (44%), 7 of 12 Asian studies (58%), and 0 of 4 studies published in another country (0%)
Statistical analysis using Fisher's exact test
Statistical analysis using ANOVA
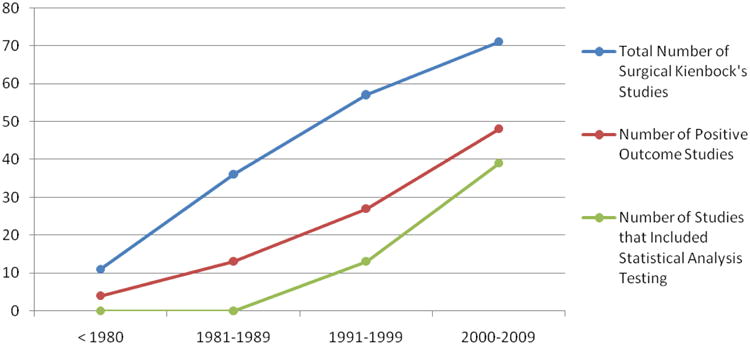
Figure 2 demonstrates trends in surgical Kienbock's research over the past 40 years. As awareness of Kienbock's disease has grown, the number of primary clinical trials pertaining to Kienbock's disease has increased substantially from 11 studies during 1970-1979 to 71 studies during 2000-2009. Over time, results from published studies have become more positive (36% to 68%, p = 0.007) and are more likely to incorporate statistical analysis testing (0% to 55%, p <0.001, Figure 2). These findings could be the result of improved management of Kienbock's disease and improved study quality over time. However, the increasing positive outcome rate for published Kienbock's studies over time may suggest a trend of increasing publication bias among journals toward Kienbock's studies.
Figure 2. Trends in Surgical Kienbock's Research Over Time.
Abstracts Accepted to ASSH
Twenty-four abstracts pertaining to Kienbock's disease were identified from the 1992-2004 annual ASSH meetings (Table 4). Ten abstracts were considered inappropriate for review (2 diagnostic/imaging, 2 non-human, 1 non-operative, 5 inextractable data) and thus eliminated from our analysis. Of the 14 abstracts included in our study, 11 (79%) were ultimately published in peer-reviewed journals with an average of 2.2 years to publication. The presence of positive outcomes or statistical analysis had no significant impact on ultimate publication (p = 1.000, p = 1.000, respectively).
Table 4. Study Characteristics of Kienbock's Abstracts Presented at the 1992-2004 ASSH Annual Meeting†.
| Variables | Number of Abstracts | Published (%) | P value |
|---|---|---|---|
| Country of Study Origin | 1.000‡ | ||
| US | 6 | 5 (83%) | |
| Other | 8 | 6 (75%) | |
| Total Number of Wrists | 0.506‡ | ||
| < 20 | 9 | 8 (89%) | |
| > 20 | 5 | 3 (60%) | |
| Result | 1.000‡ | ||
| Positive | 10 | 8 (80%) | |
| Neutral/Negative | 4 | 3 (75%) | |
| Statistical Analysis | 1.000‡ | ||
| No | 7 | 5 (71%) | |
| Yes | 7 | 6 (86%) | |
| Complications | 0.096‡ | ||
| Not recorded | 7 | 7 (100%) | |
| ≤ 10% | 3 | 2 (67%) | |
| > 10% | 4 | 2 (50%) | |
14 abstracts were included in our analysis; 10 abstracts were eliminated (2 diagnostic/imaging, 2 non-human, 1 non-operative, 5 inextractable data for Kienbock's patients or for specific procedure)
Statistical analysis using Fisher's exact test
When comparing study characteristics of the 14 ASSH meeting abstracts with the manuscripts published during the same time period from our systematic review (n = 128), we found that abstracts presented at ASSH had a slightly higher positive outcome rate (71% vs 59%), a shorter average time to publication (2.2 years vs. 5.4 years), and were more likely to include some form of statistical analysis testing (50% vs 41%) compared to published manuscripts during the same time period. These results may indicate that Kienbock's studies presented at the ASSH have better outcomes and are of better quality than studies ultimately published in the literature which ultimately results in a faster time to publication.
Discussion
Ever since the advent of scientific and medical periodicals in the late 17th century, the publication of medical research has provided a basis for the common understanding of medical diseases and their associated treatment options. However, it was not until the early 1980's that direct evidence of publication bias within the medical literature became widely recognized.5,9,25-31 Over the past three decades, medical researchers have become increasingly conscientious of the potential consequences of publication bias (overestimation of treatment effects and inappropriate risk factor associations) on patient management and health policy. Recent studies have demonstrated a clear bias toward publishing research with positive outcomes, increased sample size, and statistically significant results.5,8,11,14,31 More specifically, evaluation of the surgical literature has found that top surgical journals are at increased risk for publication bias due to the low prevalence of high-level clinical studies and variable complication rates between different surgical centers.13,23-24 This problem is further exacerbated for rare surgical disorders with poorly defined management strategies, such as Kienbock's disease. Due to the low prevalence, unknown etiology, poorly defined treatment algorithm, and lack of outcomes/complication data for Kienbock's disease, hand surgeons are more likely to base management decisions on randomly dispersed case reports/series in the published literature and presentations at national conferences. Thus, the presence of publication bias either in the published literature or among abstracts presented at national meetings has a greater propensity to directly affect patient care.
In this study, we present an analysis of all world literature (English articles and non-English articles with an English abstract) pertaining to the surgical management of Kienbock's disease. Overall, we did not find any evidence of positive outcome bias among published Kienbock's manuscripts. This conclusion is supported by the low percentage of positive outcome studies for Kienbock's disease (53%) compared to other surgical disorders (74%), and the failure to demonstrate a relationship between positive outcomes in abstracts presented at annual ASSH meetings and achieving ultimate publication.13 However, the lower positive outcome rate for Kienbock's studies could be the result of poorer expected outcomes for the surgical management of Kienbock's disease rather than decreased positive outcome bias among published Kienbock's abstracts.
Our results also demonstrated a higher publication rate of Kienbock's studies (79%) compared to the publication rate of other hand disorders (52%) presented at the ASSH annual meetings which could indicate potential selection bias at the national conference level prior to manuscript submission (pre-publication bias).32 This theory is further supported by the slightly higher positive outcome rate (71% vs 59%), shorter average time to publication (2.2 years vs. 5.4 years), and increased likelihood of including some form of statistical analysis testing (50% vs 41%) among ASSH abstracts compared to published manuscripts during the same time period. However, the limited sample size of our analysis (14 ASSH abstracts) makes it impossible to draw any firm conclusions from these results and their interpretations should be reviewed with caution. Our goal of including this analysis in our study was to increase awareness among hand surgeons of potential selection bias among abstracts presented at national conferences and to encourage discretion when using these results to make patient management decisions.
Study Limitations
As with any systematic review, our study was limited by the quality of available literature. This limitation was especially challenging for Kienbock's disease. Forty-five published studies were unable to be incorporated into our analysis because they involved multiple procedures and/or multiple indications without providing specific outcomes data for Kienbock's patients. Of the remaining 175 published studies included in our analysis, most were small non-comparitive case series.
In an attempt to compensate for the lack of published Kienbock's studies and also to reduce publication bias within our own systematic review, we choose to include both English and non-English literature. However, because of language barriers, we were only able to review the English abstracts associated with non-English articles. This hindrance may have considerably reduced our sample size for various data parameters and consequently impaired our ability to determine statistically significant results.
Another limitation unique to studies analyzing positive outcome bias for specific conditions is the fact that various conditions will have different rates of positive outcomes based on inherent differences in management efficacy. For example, one would expect an inherently lower positive outcome rate for studies researching treatment for pancreatic cancer compared to studies researching management for distal radius fractures simply because distal radius fractures are easier to treat successfully. Thus, an apparent publication bias, as measured by positive outcome rate, does not necessarily imply a flaw in the editorial process.
For our study we were unable to determine whether the cause of our observed low positive outcome rate (53%) was the result of poorer expected outcomes among surgically managed Kienbock's patients or decreased publication bias among published Kienbock's studies. Other studies assessing publication bias for other conditions have attempted to correct for this issue by comparing study characteristics between published and non-published manuscripts or abstracts either accepted or not accepted to national conferences.8,12 However, the authors of this study did not have access to non-published literature or ASSH abstract submissions prior to acceptance.
Due to the paucity of available literature, varied outcome measures, and our inability to review the entirety of non-English articles, we were unable to perform a comprehensive comparative analysis of surgical Kienbock's procedures. Although we recognize the need for a formal evidence-based comparative evaluation of Kienbock's procedures, the purpose of our analysis is to provide a systematic, critical review of the existing literature, identify any evidence of publication bias, and highlight research challenges facing rare surgical diseases.
Future Recommendations
Research regarding rare diseases has historically suffered from decreased attention, inadequate funding, and poor patient recruitment.33-36 As a result, clinical studies of rare diseases often lack randomized controlled trials and formal statistical analyses, thus making them more prone to experience publication bias.33-36 This means that physicians treating such rare diseases must form their clinical judgment solely on the basis of (potentially biased) observational studies, experience, and anecdote.33 In 1993 the NIH founded the Office of Rare Diseases Research (ORDR), which coordinates and supports research of rare diseases.1 Recent studies examining publication bias and challenges specific to rare disease research have promoted increased utility of the national clinical trial registry (www.clinicaltrials.gov), which provides information regarding all prospective clinical trials.35-37 However, this design is poorly suited for many surgical disorders due to the predominance of retrospective outcome analysis. Furthermore, our study demonstrates that a considerable portion of surgical Kienbock's research is conducted outside the United States. We recommend the formation of an international patient database for Kienbock's disease that would provide standardized information regarding outcomes, complications, and follow-up for all surgical treatment methods. This would facilitate the development of clear evidence based outcomes regarding surgical management of this rare disease and enable determination of optimal treatment algorithms.
Acknowledgments
Supported in part by a Midcareer Investigator Award in Patient-Oriented Research (K24 AR053120) from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (to Dr. Kevin C. Chung).
Appendix A
English Abstracts
| Author | Year | Journal | Outcomes | |
|---|---|---|---|---|
| 1 | Ozalp | 2009 | Archives of Orthopaedic and Trauma Surgery | Positive |
| 2 | Gay | 2009 | Plastic and Reconstructive Surgery | Positive |
| 3 | Mathoulin | 2009 | Microsurgery | Positive |
| 4 | Aly | 2009 | Orthopedics | Positive |
| 5 | Meena | 2009 | Indian Journal of Orthopaedics | Neutral |
| 6 | Croog | 2008 | Journal of Hand Surgery (American) | Positive |
| 7 | Waitayawinyu | 2008 | Journal of Hand Surgery (American) | Positive |
| 8 | Altay | 2008 | International Orthopaedics | Positive |
| 9 | Arora | 2008 | Journal of Hand Surgery (American) | Positive |
| 10 | Streich | 2008 | International Orthopaedics | Positive |
| 11 | Watanabe | 2008 | Journal of Bone and Joint Surgery (American) | Positive |
| 12 | Lumsden | 2008 | Journal of Hand Surgery (American) | Positive |
| 13 | Jones | 2008 | Journal of Hand Surgery (Euroepan Volume) | Neutral |
| 14 | Kawoosa | 2007 | International Orthopaedics | Neutral |
| 15 | Hermans | 2007 | Scandinavian Journal of Plastic and Reconstructive Surgery and Hand Surgery | Neutral |
| 16 | Tatebe | 2007 | Journal of Hand Surgery (American) | Positive |
| 17 | Raven | 2007 | Clinical Orthopaedics and Related Research | Positive |
| 18 | Tambe | 2007 | Acta Orthopaedica Belgica | Negative |
| 19 | El-Mowafi | 2006 | Acta Orthopaedica Belgica | Neutral |
| 20 | Schweizer | 2006 | Journal of Hand Surgery (American) | Neutral |
| 21 | Tatebe | 2006 | Hand Surgery | Positive |
| 22 | Gong | 2006 | Journal of Bone and Joint Surgery (British) | Positive |
| 23 | Vanden Dungen | 2006 | Chirurgie de la Main | Negative |
| 24 | Lu | 2006 | Annals of Plastic Surgery | Positive |
| 25 | Moran | 2005 | Journal of Hand Surgery (American) | Positive |
| 26 | Yasuda | 2005 | Scandinavian Journal of Plastic and Reconstructive Surgery and Hand Surgery | Positive |
| 27 | Daecke | 2005 | Journal of Hand Surgery (American) | Neutral |
| 28 | Daecke | 2005 | Journal of Hand Surgery (American) | Positive |
| 29 | Zafra | 2005 | Acta Orthopaedica Belgica | Positive |
| 30 | Tambe | 2005 | International Orthopaedics | Positive |
| 31 | Zenzai | 2005 | Journal of Hand Surgery (British and European Volume) | Positive |
| 32 | DeSmet | 2005 | Journal of Hand Surgery (British and European Volume) | Positive |
| 33 | Sakai | 2004 | Hand Surgery | Neutral |
| 34 | Meier | 2004 | Journal of Hand Surgery (British and European Volume) | Positive |
| 35 | Yajima | 2004 | Scandinavian Journal of Plastic and Reconstructive Surgery and Hand Surgery | Positive |
| 36 | Thomas | 2004 | Journal of Hand Surgery (American) | Positive |
| 37 | Leblebicioglu | 2003 | Arthroscopy | Neutral |
| 38 | Watson | 2003 | Journal of Hand Surgery (American) | Neutral |
| 39 | Koh | 2003 | Journal of Hand Surgery (American) | Positive |
| 40 | Kuhlman | 2003 | Acta Orthopaedica Belgica | Positive |
| 41 | Gabl | 2003 | European Surgery | Positive |
| 42 | Chillemi | 2003 | Journal of Orthopaedics and Traumatology | Positive |
| 43 | Iwasaki | 2002 | Journal of Bone and Joint Surgery (British) | Positive |
| 44 | Wada | 2002 | Journal of Hand Surgery (British and European Volume) | Neutral |
| 45 | Laing | 2002 | European Journal of Orthopaedic Surgery and Traumatology | Positive |
| 46 | Gabl | 2002 | Journal of Hand Surgery (British and European Volume) | Neutral |
| 47 | Oishi | 2002 | Plastic and Reconstructive Surgery | Positive |
| 48 | Minami | 2002 | Current Opinion in Orthopaedics | Positive |
| 49 | Soejima | 2002 | Journal of Hand Surgery (American) | Positive |
| 50 | Wintman | 2001 | Orthopedics | Positive |
| 51 | Takase | 2001 | Journal of Bone and Joint Surgery (American) | Positive |
| 52 | Illarramendi | 2001 | Journal of Hand Surgery (American) | Positive |
| 53 | Kakinoki | 2001 | Hand Surgery | Neutral |
| 54 | Bengoechea-Beeby | 2001 | Journal of Hand Surgery (American) | Neutral |
| 55 | Sauerbier | 2000 | Annals of Plastic Surgery | Positive |
| 56 | Lamas | 2000 | Journal of Hand Surgery (American) | Neutral |
| 57 | Salmon | 2000 | Journal of Bone and Joint Surgery (British) | Positive |
| 58 | Makino | 2000 | Journal of Reconstructive Microsurgery | Neutral |
| 59 | Menth-Chiari | 1999 | Arthroscopy | Positive |
| 60 | Ueba | 1999 | Journal of Orthopaedic Science | Neutral |
| 61 | Nakamura | 1998 | Journal of Hand Surgery (British and European Volume) | Positive |
| 62 | Kaarela | 1998 | Journal of Hand Surgery (British and European Volume) | Negative |
| 63 | Delaere | 1998 | Journal of Hand Surgery (British and European Volume) | Negative |
| 64 | Moneim | 1998 | Iowa Orthopaedic Journal | Positive |
| 65 | Yajima | 1998 | Journal of Hand Surgery (American) | Positive |
| 66 | Garcia-Elias | 1998 | Annales de Chirurgie de la Main | Neutral |
| 67 | Shayfer | 1998 | Orthopedics | Neutral |
| 68 | Steenwerckx | 1997 | Acta Orthopaedica Belgica | Neutral |
| 69 | Carroll | 1997 | Clinical Orthopaedics and Related Research | Neutral |
| 70 | Quenzer | 1997 | Journal of Hand Surgery (American) | Neutral |
| 71 | Trail | 1996 | Journal of Hand Surgery (British and European Volume) | Positive |
| 72 | Watson | 1996 | Journal of Hand Surgery (American) | Positive |
| 73 | Zelouf | 1996 | Journal of Hand Surgery (American) | Positive |
| 74 | Guo | 1996 | Annals of Plastic Surgery | Neutral |
| 75 | Miura | 1996 | Journal of Hand Surgery (American) | Positve |
| 76 | Wheatley | 1996 | Annals of Plastic Surgery | Positive |
| 77 | Rhee | 1996 | Journal of Korean Medical Science | Neutral |
| 78 | Sennwald | 1995 | Journal of Hand Surgery (American) | Positive |
| 79 | DeSmet | 1995 | Acta Orthopaedica Belgica | Negative |
| 80 | Tomaino | 1994 | Journal of Hand Surgery (American) | Neutral |
| 81 | Bochud | 1994 | Journal of Hand Surgery (British and European Volume) | Neutral |
| 82 | Yajima | 1994 | Journal of the Japanese Orthopaedic Association | Neutral |
| 83 | Begley | 1994 | Journal of Hand Surgery (American) | Positive |
| 84 | Minami | 1994 | Journal of Hand Surgery (American) | Positive |
| 85 | Amillo | 1993 | International Orthopaedics | Positive |
| 86 | Inoue | 1992 | Archives of Orthopaedic and Trauma Surgery | Neutral |
| 87 | Voche | 1992 | Journal of Hand Surgery (British and European Volume) | Positive |
| 88 | O'Flanagan | 1992 | Journal of the Royal College of Surgeons of Edinborough | Negative |
| 89 | Inoue | 1992 | Acta Orthopaedica Scandinavica | Neutral |
| 90 | Nakamura | 1991 | Journal of Bone and Joint Surgery (American) | Positive |
| 91 | Weiss | 1991 | Journal of Bone and Joint Surgery (American) | Positive |
| 92 | Rock | 1991 | Journal of Hand Surgery (American) | Positive |
| 93 | Inoue | 1990 | Acta Orthopaedica Scandinavica | Positive |
| 94 | Hasselgren | 1990 | Journal of Hand Surgery (British and European Volume) | Positive |
| 95 | Alexander | 1990 | Journal of Hand Surgery (American) | Negative |
| 96 | Kawai | 1988 | Journal of Bone and Joint Surgery (American) | Neutral |
| 97 | Viljakka | 1987 | Acta Orthopaedica Scandinavica | Neutral |
| 98 | Schattenkerk | 1987 | Acta Orthopaedica Scandinavica | Neutral |
| 99 | Ekerot | 1986 | Scandinavian Journal of Plastic and Reconstructive Surgery | Neutral |
| 100 | Kato | 1986 | Journal of Hand Surgery (American) | Positive |
| 101 | Evans | 1986 | Journal of Hand Surgery (British and European Volume) | Neutral |
| 102 | Watson | 1985 | Journal of Hand Surgery (American) | Neutral |
| 103 | Blanco | 1985 | Journal of Hand Surgery (American) | Neutral |
| 104 | Backaert | 1985 | Acta Orthopaedica Belgica | Neutral |
| 105 | Sundberg | 1984 | Clinical Orthopaedics and Related Research | Neutral |
| 106 | Pardini | 1984 | International Orthopaedics | Neutral |
| 107 | Ishiguro | 1984 | Journal of the Japanese Orthopaedic Association | Positive |
| 108 | Eiken | 1984 | Scandinavian Journal of Plastic and Reconstructive Surgery | Positive |
| 109 | Kinnard | 1983 | Canadian Journal of Surgery | Positive |
| 110 | Armistead | 1982 | Journal of Bone and Joint Surgery (American) | Positive |
| 111 | Ramakrishna | 1982 | Journal of Bone and Joint Surgery (American) | Neutral |
| 112 | Almquist | 1982 | Journal of Hand Surgery (American) | Neutral |
| 113 | Lichtman | 1982 | Journal of Hand Surgery (American) | Positive |
| 114 | Hedeboe | 1982 | Scandinavian Journal of Plastic and Reconstructive Surgery | Positive |
| 115 | Bertini | 1982 | Italian Journal of Orthopaedics and Traumatology | Positive |
| 116 | Stark | 1981 | Journal of Bone and Joint Surgery (American) | Negative |
| 117 | Grassi | 1978 | Italian Journal of Orthopaedics and Traumatology | Positive |
| 118 | Inglis | 1977 | Journal of Bone and Joint Surgery (American) | Positive |
| 119 | Lichtman | 1977 | Journal of Bone and Joint Surgery (American) | Neutral |
| 120 | Roca | 1976 | Journal of Bone and Joint Surgery (American) | Neutral |
| 121 | Barber | 1974 | Journal of Bone and Joint Surgery (British) | Positive |
| 122 | Codega | 1973 | International Surgery | Neutral |
| 123 | Nahigian | 1970 | Journal of Bone and Joint Surgery (American) | Neutral |
| 124 | Graner | 1966 | Journal of Bone and Joint Surgery (American) | Positive |
Non-English Abstracts
| Author | Year | Journal | Outcomes | |
|---|---|---|---|---|
| 1 | Von-Maydell | 2008 | Handchirurgie, Mikrochirurgie, Plastische Chirurgie | Neutral |
| 2 | Lecomte | 2007 | Revue de Chirurgie Orthopedique et Reparatrice de l'Appareil Moteur | Neutral |
| 3 | Baronetti | 2006 | Minerva Ortopedica e Traumatologica | Neutral |
| 4 | Khorbi | 2005 | Tunisie Medicale | Neutral |
| 5 | Adel | 2005 | Tunisie Medicale | Positive |
| 6 | Amillo-Garayoa | 2005 | Revista de Ortopedia y Traumatologia | Positive |
| 7 | Lu | 2003 | Chinese Medical Journal | Positive |
| 8 | Welby | 2003 | Chirurgie de la Main | Negative |
| 9 | Das Gupta | 2003 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Positive |
| 10 | Altay | 2002 | Artroplasti Artroskopik Cerrahi | Positive |
| 11 | Sauerbier | 2001 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Positive |
| 12 | Trankle | 2000 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Positive |
| 13 | Siala | 2000 | Revue de Chirurgie Orthopedique et Reparatrice de l'Appareil Moteur | Positive |
| 14 | Jiang | 1999 | Chinese Journal of Reparative and Reconstructive Surgery | Positive |
| 15 | Dautel | 1999 | Main | Neutral |
| 16 | Sauerbier | 1998 | Langenbecks Archiv für Chirurgie. Supplement. Kongressband. Deutsche Gesellschaft für Chirurgie. Kongress | Positive |
| 17 | Bartelmann | 1998 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Negative |
| 18 | Schulz | 1998 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Neutral |
| 19 | Renner | 1998 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Positive |
| 20 | Wustner-Hofmann | 1997 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Neutral |
| 21 | Staudenmaier | 1997 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Positive |
| 22 | Thomas | 1997 | Annales de Chirurgie de la Main et du Membre Superieur | Neutral |
| 23 | Ducarmois | 1997 | Annales de chirurgie de la main et du membre supérieur | Neutral |
| 24 | Garbuio | 1996 | Annales de chirurgie de la main et du membre supérieur | Neutral |
| 25 | Wachtl | 1994 | Schweizerische Rundschau fur Medizin Praxis | Negative |
| 26 | Gomis | 1994 | Revue de Chirurgie Orthopedique et Reparatrice de l'Appareil Moteur | Positive |
| 27 | Allieu | 1991 | Annales de Chirurgie de la Main et du Membre Superieur | Positive |
| 28 | Allieu | 1991 | Annales de chirurgie de la main et du membre supérieur | Positive |
| 29 | Voche | 1991 | Revue de Chirurgie Orthopedique et Reparatrice de l'Appareil Moteur | Positive |
| 30 | Ham | 1990 | Nederlands Tijdschrift voor Geneeskunde | Neutral |
| 31 | Buck-Gramcko | 1990 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Negative |
| 32 | Kawai | 1990 | Annales de Chirurgie de la Main et du Membre Superieur | Neutral |
| 33 | Shibata | 1989 | Journal of the Japanese Orthopaedic Association | Neutral |
| 34 | Lesur | 1989 | Revue de chirurgie orthopédique et réparatrice de l'appareil moteur | Neutral |
| 35 | Yang | 1989 | Chinese Journal of Surgery | Neutral |
| 36 | Ehall | 1989 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Positive |
| 37 | Prommersberger | 1988 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Neutral |
| 38 | Kern | 1988 | Zeitschrift fur Orthopadie und Ihre Grenzgebiete | Neutral |
| 39 | Bruser | 1986 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Neutral |
| 40 | Rajani | 1985 | Ugeskrift for Laeger | Positive |
| 41 | Erbs | 1984 | Handchirurgie Mikrochirurgie Plastische Chirurgie | Neutral |
| 42 | Razemon | 1984 | Chirurgie | Positive |
| 43 | Schmitt | 1984 | Zeitschrift fur Orthopadie und Ihre Grenzgebiete | Positive |
| 44 | Saffar | 1982 | Annales de Chirurgie de la Main | Neutral |
| 45 | Roullet | 1982 | Annales de Chirurgie de la Main | Negative |
| 46 | Comtet | 1982 | Annales de chirurgie de la main | Neutral |
| 47 | Naett | 1981 | Handchirurgie | Neutral |
| 48 | Kerschbaumer | 1981 | Orthopade | Positive |
| 49 | Kerschbaumer | 1979 | Handchirurgie | Negative |
| 50 | Codega | 1973 | Polski Przeglad Chirurgiczny | Neutral |
| 51 | Sommelet | 1970 | Revue de chirurgie orthopédique et réparatrice de l'appareil moteur | Neutral |
Footnotes
We appreciate the assistance of Soo Young Kwak with the statistical analyses portion of this review.
References
- 1.National Institutes of Health Office of Rare Diseases – Rare Disease Terms. [Accessed June 30 2009]; Available at: http://rarediseases.info.nih.gov/Default.aspx.
- 2.Schuind F, Eslami S, Ledoux P. Kienbock's disease. J Bone Joint Surg (Br) 2008;90B(2):133–139. doi: 10.1302/0301-620X.90B2.20112. [DOI] [PubMed] [Google Scholar]
- 3.Luo J, Diao E. Kienbock's disease: An approach to treatment. Hand Clin. 2006;22(4):465–73. doi: 10.1016/j.hcl.2006.07.003. [DOI] [PubMed] [Google Scholar]
- 4.Wagner JP, Chung KC. A historical report on Robert Kienbock (1871-1953) and Kienbock's Disease. J Hand Surg (Am) 2005;30(6):1117–21. doi: 10.1016/j.jhsa.2005.08.002. [DOI] [PubMed] [Google Scholar]
- 5.Dickersin K. The existence of publication bias and risk factors for its occurrence. JAMA. 1990;263(10):1385–9. [PubMed] [Google Scholar]
- 6.Chalmers TC, Frank CS, Reitman D. Minimizing the three stages of publication bias. JAMA. 1990;263(10):1392–95. [PubMed] [Google Scholar]
- 7.Callaham M, Wears RL, Weber E. Journal prestige, publication bias, and other characteristics associated with citation of published studies in peer-reviewed journals. JAMA. 2002;287(21):2847–50. doi: 10.1001/jama.287.21.2847. [DOI] [PubMed] [Google Scholar]
- 8.Callaham ML, Wears RL, Weber EJ, Barton C, Young G. Positive-outcome bias and other limitations in the outcome of research abstracts submitted to a scientific meeting. JAMA. 2002;280(3):254–7. doi: 10.1001/jama.280.3.254. [DOI] [PubMed] [Google Scholar]
- 9.Simes RJ. Publication bias: the case for an international registry of clinical trials. J Clin Oncol. 1986;4(10):1529–41. doi: 10.1200/JCO.1986.4.10.1529. [DOI] [PubMed] [Google Scholar]
- 10.Yoshimoto Y. Publication bias in neurosurgery: lessons from series of unruptured aneurysms. Acta Neurochir. 2003;145:45–48. doi: 10.1007/s00701-002-1036-0. [DOI] [PubMed] [Google Scholar]
- 11.Easterbrook PJ, Berlin JA, Gopalan R, Matthews DR. Publication bias in clinical research. The Lancet. 1991;337:867–72. doi: 10.1016/0140-6736(91)90201-y. [DOI] [PubMed] [Google Scholar]
- 12.Krzyzanowska MK, Pintilie M, Tannock IF. Factors associated with failure to publish large randomized trials presented at an oncology meeting. JAMA. 2003;290(4):495–501. doi: 10.1001/jama.290.4.495. [DOI] [PubMed] [Google Scholar]
- 13.Hasenboehler EA, Choudhry IK, Newman JT, Smith WR, Ziran BH, Stahel PF. Bias towards publishing positive results in orthopedic and general surgery: a patient safety issue? Patient Saf Surg. 2007;1(1):4–9. doi: 10.1186/1754-9493-1-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Harris IA, Mourad M, Kadir A. Publication bias in abstracts presented to the annual meeting of the American Academy of Orthopaedic Surgeons. J Orthop Surg. 2007;15(1):62–6. doi: 10.1177/230949900701500114. [DOI] [PubMed] [Google Scholar]
- 15.Okike K, Kocher MS, Mehlman CT, Heckman JD, Bhandari M. Nonscientific factors associated with acceptance for publication in the Journal of Bone and Joint Surgery (American volume) J Bone Joint Surg Am. 2008;90(8):2432–7. doi: 10.2106/JBJS.G.01687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Okike K, Kocher MS, Mehlman CT, Heckman JD, Bhandari M. Publication bias in orthopaedic research: an analysis of scientific factors associated with publication in the Journal of Bone and Joint Surgery (American volume) J Bone Joint Surg Am. 90(3):595–601. doi: 10.2106/JBJS.G.00279. [DOI] [PubMed] [Google Scholar]
- 17.Ioannidis JP. Effect of the statistical significance of results in the time to completion and publication of randomized efficacy trials. JAMA. 1998;279(4):281–6. doi: 10.1001/jama.279.4.281. [DOI] [PubMed] [Google Scholar]
- 18.Burdett S, Stewart LA, Tierney JF. Publication bias and meta-analyses: a practical example. Int J Technol Assess Health Care. 2003;19(1):129–34. doi: 10.1017/s0266462303000126. [DOI] [PubMed] [Google Scholar]
- 19.McAuley L, Pham B, Tugwell P, Moher D. Does the inclusion of grey literature influence estimates of intervention effectiveness reported in meta-analyses? Lancet. 2000;356:1228–31. doi: 10.1016/S0140-6736(00)02786-0. [DOI] [PubMed] [Google Scholar]
- 20.Vickers A, Goyal N, Harland R, Rees R. Do certain countries produce only positive results? A systematic review of controlled trials. Control Clin Trials. 1998;19:159–66. doi: 10.1016/s0197-2456(97)00150-5. [DOI] [PubMed] [Google Scholar]
- 21.Hopewell S, Clarke M, Stewart L, Tierney J. Time to publication for results of clinical trials. Cochrane Database Syst Rev. 2007;18(2):MR000011. doi: 10.1002/14651858.MR000011.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chalmers I. Underreporting research is a scientific misconduct. JAMA. 1990;263(10):1405–8. [PubMed] [Google Scholar]
- 23.Syin D, Woreta T, Chang DC, Cameron JL, Pronovost PJ, Makary MA. Publication bias in surgery: implications for informed consent. J Surg Res. 2007;143:88–93. doi: 10.1016/j.jss.2007.03.035. [DOI] [PubMed] [Google Scholar]
- 24.Chang DC, Matsen SL, Simpkins CE. Why should surgeons care about clinical research methodology. J Am Coll Surg. 2006;203:827–30. doi: 10.1016/j.jamcollsurg.2006.08.013. [DOI] [PubMed] [Google Scholar]
- 25.Dickersin K, Chan S, Chalmers TC, Sacks HS, Smith H., Jr Publication bias and clinical trials. Controlled Clin Trials. 1987;8:343–53. doi: 10.1016/0197-2456(87)90155-3. [DOI] [PubMed] [Google Scholar]
- 26.Sommer B. The file drawer effect and publication rates in menstrual cycle research. Psychol Women Q. 1987;11:233–42. [Google Scholar]
- 27.Dudley HAF. Surgical research: master or servant. Am J Surg. 1978;135:458–460. doi: 10.1016/0002-9610(78)90084-3. [DOI] [PubMed] [Google Scholar]
- 28.Goldman L, Loscalzo A. Fate of cardiology research originally published in abstract form. N Engl J Med. 1980;303:255–9. doi: 10.1056/NEJM198007313030504. [DOI] [PubMed] [Google Scholar]
- 29.Meranze J, Ellison N, Greenhow DE. Publications resulting from anesthesia meeting abstracts. Anesth Analg. 1982;61:445–8. [PubMed] [Google Scholar]
- 30.McCormick MC, Holmes JH. Publication of research presented at the pediatric meetings. AJDC. 1985;139:122–6. doi: 10.1001/archpedi.1985.02140040020017. [DOI] [PubMed] [Google Scholar]
- 31.Chalmers I, Adams M, Dickersin K, Hetherington J, Tarnow-Mordi W, Meinert C, et al. A cohort study of summary reports of controlled trials. JAMA. 1990;263:1401–4. [PubMed] [Google Scholar]
- 32.Gavazza JB, Foulkes GD, Meals RA. Publication patterns of papers presented at the American Society for Surgery of the Hand Annual Meeting. J Hand Surg (Am) 1996;21A:742–5. doi: 10.1016/S0363-5023(96)80185-7. [DOI] [PubMed] [Google Scholar]
- 33.Lilford RJ, Thornton JG, Braunholtz D. Clinical trials and rare diseases: a way out of a conundrum. BMJ. 1995;311(7020):1621–5. doi: 10.1136/bmj.311.7020.1621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Behera M, Kumar A, Soares HP, Sokol L, Djulbegovic B. Evidence-based medicine for rare diseases: implications for data interpretation and clinical trial design. Cancer Control. 2007;14(2):160–6. doi: 10.1177/107327480701400209. [DOI] [PubMed] [Google Scholar]
- 35.Hampton T. Rare disease research gets a boost. JAMA. 2006;295(24):2836–8. doi: 10.1001/jama.295.24.2836. [DOI] [PubMed] [Google Scholar]
- 36.Dickersin K, Rennie D. Registering clinical trials. JAMA. 2003;290(4):516–523. doi: 10.1001/jama.290.4.516. [DOI] [PubMed] [Google Scholar]
- 37.National Institutes of Health. [Accessed June 30 2009]; ClinicalTrials.gov. Available at: http://www.clinicaltrials.gov/ct2/home.