

Abstract
Background:
To investigate the proper modifications and usefulness of side-hairline correction surgery in Korean female patients depending on different zygomatic bone structures.
Methods:
Different zygomatic bone structures were classified according to their maximum transverse width among 310 cases of hairline correction surgery in Korean women. The widest transverse width was located on the anterior zygomatic malar area in type 1, on the mid-zygomatic arch in type 2, and on the posterior zygomatic arch in type 3; there was no difference in the transverse width between the anterior and posterior zygomatic arch in type 4. Various modifications of side-hairline correction surgery were performed among the 310 cases according to the zygomatic bone classification.
Results:
Among 310 patients, 74 had a type 1 zygomatic structure, 106 had type 2, 46 had type 3, and 50 had type 4. Thirty-four patients exhibited different left and right transverse widths: type 1 + 2 (n = 26), type 2 + 3 (n = 6), type 1 + 3 (n = 1), and type 3 + 4 (n = 1). Satisfactory results were obtained in all patients without noticeable side effects. A minor touch-up procedure was performed in 14 patients to achieve density reinforcement 10 months postoperatively, and all 14 patients expressed satisfaction with the results.
Conclusions:
In East Asian patients, both side-hairline correction surgery and zygoma reduction can be considered eligible treatment options for the purpose of midface slimming. Especially in patients with a type 3 zygomatic bone structure, side-hairline correction surgery may be more effective than zygoma reduction surgery for midface slimming.
East Asians tend to have a brachycephalic facial type characterized by a relatively low nose bridge, prominent cheekbones, and a wide face. A series of aesthetic procedures including mandible angle reduction, zygoma reduction, and others are available to slim the facial contour.
A procedure in which the hairline is corrected by hair transplantation is being performed with increasing frequency to make the face of Korean women appear smaller and slimmer. For East Asians with a wide and prominent zygoma, the transverse width of the midface is often reduced by zygoma reduction.1 Either hairline correction surgery or zygoma reduction can be an ideal option for reducing the transverse width of a wide midface. However, no information is available on the criteria for choosing either one of these 2 procedures or on the optimal surgical technique when reducing the width of the midface. The objective of the present study was to identify the most effective hairline correction techniques according to different zygomatic bone structures.
MATERIALS AND METHODS
The author performed side-hairline correction surgery in 310 female Korean patients who visited our clinic for side-hairline correction surgery from November 2011 to September 2013. None of the patients underwent any zygomatic bone surgeries. All surgeries were performed by a single well-experienced surgeon. All patients’ medical photographs and records were retrospectively reviewed. The structure of the zygomatic bone was examined in all 310 patients. The patients’ age ranged from 19 to 58 years with a median age of 29.4 years. The zygomatic bones were classified into 4 different types as described below. Patients with a history of surgical zygoma reduction were excluded.
The zygomatic bones were divided into the anterior third, middle third, and posterior third, and the transverse width of each part was measured for further classification. The widest transverse width was located on the anterior zygomatic malar area in type 1, on the mid-zygomatic arch in type 2, and on the posterior zygomatic arch in type 3; there was no difference in the transverse width between the anterior and posterior zygomatic arch in type 4. This classification process was aided by visual inspection, palpation, and measurement with Vernier calipers (Mitutoyo, Kawasaki, Japan) (Figs. 1–3).
Fig. 1.

Measurement with Vernier calipers (Mitutoyo).
Fig. 3.
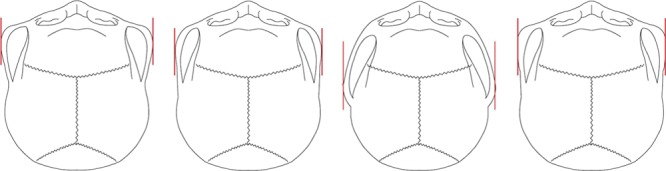
Types 1–4 zygomatic bone structures.
Fig. 2.
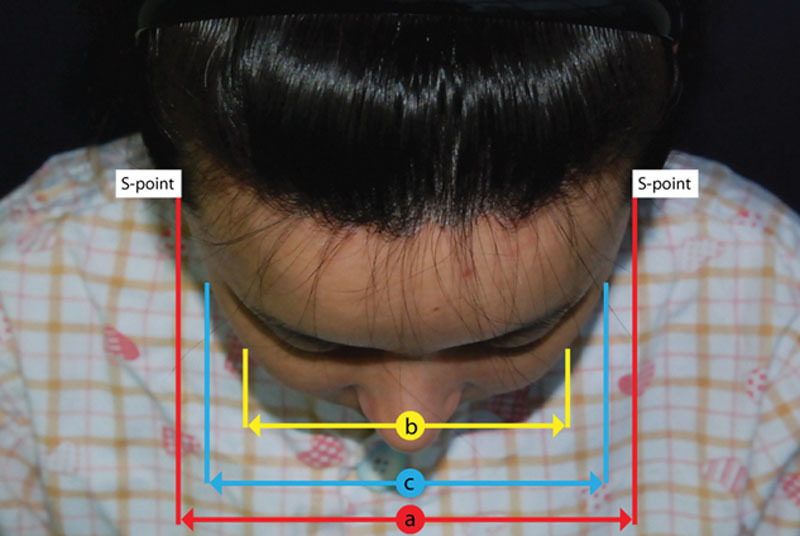
Measurement standards for the transverse width of the zygomatic bone. The distance a between the S points on both sides and the bimalar width b are measured using Vernier calipers (Mitutoyo). The greatest transverse width of the mid-zygomatic arch is labeled c. The S points are the most anterior points at which the sideburns start. Thus, distance a is the width between the posterior zygomatic arches on both sides. If a – b is >10 mm, the zygoma is classified as type 3.
Among the 310 patients, the side-hairline correction surgery included S-point advancement or sideburn reconstruction in place of zygoma reduction in 46 patients with type 3 zygomas to achieve a narrower midface. In patients with a type 1, 2, and 4 zygoma bone structure, side-hairline correction surgery was performed only in the M area, temple area, and infratemple area without S-point advancement (Fig. 4).
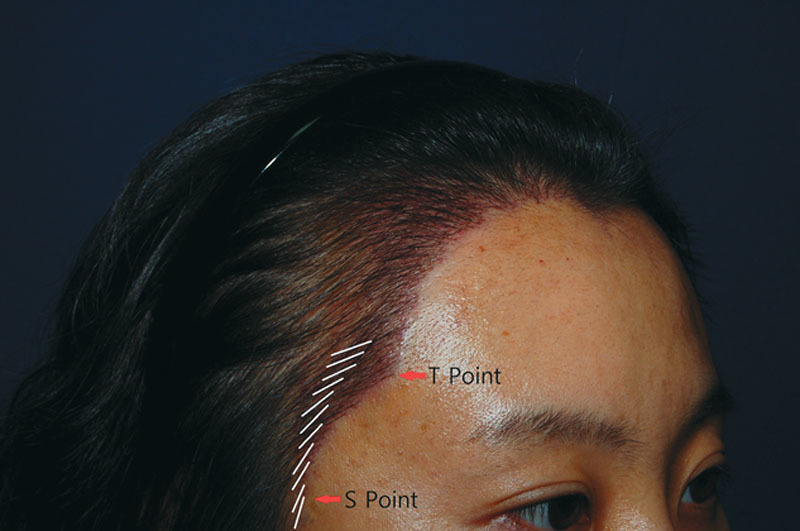
Fig. 4.

Landmarks in side-hairline correction surgery. M area indicates M-shaped frontotemporal recess area; S point, most anterior point at which the sideburn starts; T point, most anterior point of temporal peak area.
The new hairline design was drawn during the preoperative consultations. The new hairline for the transplant was determined after a thorough consultation with the patients, who actively participated in the process by looking at themselves in a mirror. An elliptical donor area was designed in the occipital region. Incisional donor harvesting was performed under local anesthesia in the prone position. Follicular units (FUs) of donor tissue were dissected and harvested under microscopic visualization. At the time of dissection, the grafts were divided into 5 major categories based on their thickness: very thin, vellus-like 1-hair FU; thin 1-hair FU; thick 1-hair FU; 2-hair FU; and 3- and 4-hair FU.
The transplantation procedure was performed with the patient in the supine position. After cleansing and aseptic preparation of the surgical area, a local anesthetic (solution of 1:100,000 epinephrine:lidocaine) was infiltrated. Starting from the far posterior side of the M area, 3-hair FUs were transplanted, and 2-hair FUs were then transplanted in front of this region. The graft density reached approximately 15–30 FU/cm2. Only 1-hair FUs were implanted in the transition zone, about 1 cm from the frontal hairline, in the temple areas, in the infratemple areas, and in the sideburn areas. Within the transition zone, only thick 1-hair FUs were implanted in the posterior region of the transition zone, and only thin 1-hair FUs were implanted in the area immediately in front of this. Next, only vellus-like, very thin 1-hair FUs were implanted on the very frontal part, thereby producing a natural gradation of FUs. The implant density of the anterior hairline zone of the M area was approximately 35–55 FU/cm2 and that in the infratemple and sideburn areas was 15–30 FU/cm2. The stitches were removed from the donor area 10 days postoperatively.
RESULTS
Of all 310 female patients, 74 had a type 1 zygomatic structure, 106 had type 2, 46 had type 3, and 50 had type 4. Thirty-four patients had different left and right transverse widths: type 1 + 2 (n = 26), type 2 + 3 (n = 6), type 1 + 3 (n = 1), and type 3 + 4 (n = 1). The distance a between the S points on both sides measured 12.7–14.5 cm (average, 13.7 cm). The bimalar width b measured 11.8–14.1 cm. The measured values among the different zygomatic bone types are presented in Table 1.
Table 1.
Measured Values According to Different Zygomatic Bone Types

In patients with a recessed T point (wide infratemple area), the T point was advanced to the anterior or inferior side. If the S point was recessed as in a type 3 zygoma, the S point was advanced to the anterior side.
The number of transplanted grafts per patient ranged from 608 to 1944 (average, 1252). The follow-up period spanned from 8 to 34 months (average, 12.4 months). Satisfactory results were obtained in all 310 patients with no noticeable side effects. Fourteen patients underwent a minor touch-up procedure for density reinforcement 10 months postoperatively. All 14 patients were rechecked at 6 months postoperatively and expressed satisfaction with the results of their touch-up procedure. Four patients developed a minor case of folliculitis at the transplant site that resolved spontaneously soon thereafter with no further problems. A representative case of a 28-year-old female patient who underwent side-hairline correction surgery is shown in Figures 5–7.
Fig. 5.

Preoperative view of a 28-year-old female patient with a type 3 zygoma. The temporal peak is posteriorly recessed. The distance a between the S points on both sides measured 13.5 cm, and the bimalar width measured 12.3 cm. Thus, a – b measured 1.2 cm.
Fig. 7.

Thirty-two-month postoperative view. The facial contour has been slimmed.
Fig. 6.

Preoperative design. To ensure an adequate facial size reduction effect with an adequate graft transplanting area in both M areas and infratemple areas, the T point was designed in line with the anterior and inferior movement and the S point was designed to move anteriorly by 1–2 rows.
DISCUSSION
East Asians have facial and hair-related characteristics distinct from those of most whites. First, East Asians tend to have a brachycephalic facial type featuring a relatively low nose bridge, prominent cheekbones, and a wide face.1,2 Accordingly, facial aesthetic procedures performed among many of these patients include augmentation rhinoplasty, zygoma reduction, and mandible angle reduction.
Zygoma reduction involves the creation of an osteotomy about 1 cm from the posterior zygomatic arch; the zygomatic body and arch are then fractured and pushed medially for proper adjustment and alignment. Zygoma reduction was first introduced by Onizuka et al1 in 1983. A variety of modifications have since been developed based on the aforementioned surgical techniques and procedures.2–4
The temporomandibular joint is located directly below the posterior zygomatic arch. Therefore, the area 1 cm from the posterior zygomatic arch is difficult to access during zygoma reduction because of the risk of damage to the temporomandibular joint. Accordingly, zygoma reduction surgery is ineffective if the midface is too wide secondary to the posterior zygomatic arch being wider than the anterior malar area or mid-zygomatic arch. Park and Moh5 described a camouflaging technique with hairline correction in the infratemple area for patients complaining of a wide midface following zygoma reduction surgery.
East Asians also have distinctive hair-related characteristics. Their hair is thick and black with a substantial contrast between the skin and hair color. Additionally, the number of single hair follicles in East Asians is much higher than that in whites. Only 1-hair FU grafts must be placed along the anterior and side hairlines.
A very awkward and unnatural result may be obtained if hairline correction surgery is not performed based on the proper techniques of placing the grafts at exactly the same angle, in the same direction, and with the same thickness as the preexisting hair with an equitable degree of density. Thus, the use of magnifying loupes that provide at least 3× magnification is advised to obtain adequate visibility during the grafting procedure.
Jung et al6 described a basic classification system of and technique for performing hairline correction surgery in Asian women. However, few studies on side-hairline correction surgery, which connects the temple areas, infratemple areas, presideburn areas, and sideburn areas, have been performed despite the significance for many East Asians of having a prominently wide face.
The most important landmarks when designing the infratemple and sideburn areas are the T point, which is the most anterior point of the temple area, and the S point, which is the most anterior point at which the sideburn starts (Fig. 8). After creating a straight line connecting the T point and S point, a contour similar to the concave shape of the lateral orbital rim is created from behind the imaginary straight line. When the T point is posteriorly recessed, it must be advanced either anteriorly or inferiorly to obtain adequate reduction space in the infratemple areas. When the T point is anteriorly advanced, an extremely precise technique is required because the hair being transplanted to this area is readily noticed after the surgery.
Fig. 8.

Landmarks and design for side-hairline correction.
If the hair is very thick and coarse during the preoperative assessment, the T-point advancing design should be avoided because such thick hairs are not a good match to the preexisting thin hairs. Only the very thinnest hair harvested should be implanted in the most frontal area of the T point.
A very acute angle should be maintained while the implants are placed in the infratemple areas connecting the T point to the S point. Additionally, extra care should be taken in this area to match the progressive change in direction of the hair. Implants at the T point should maintain an almost horizontal level with a gradual change in direction to become more vertical (Fig. 9).
Fig. 9.
Gradual directional change in the infratemple area.
At the S point, the direction should change to become almost perpendicular. The implants should be placed slightly posteriorly, about 3–4 degrees, to obtain an outcome close to the original appearance. Some patients have a recessed S point, undeveloped sideburns, or lost sideburns following a midface lift surgery. Sideburn reconstruction can be performed in such patients. The appropriate size of sideburns in women is either up to the upper end of the tragus or up to the zygomatic arch level. Only 1-hair FUs should be used for S-point advancement and sideburn creation. The implants should be placed about 3–4 degrees posteriorly to the S point. In patients with curly hair, precise matching of the hair curliness should be performed to ensure that the hair curls into the backward position. A very unnatural look may be obtained if the hair curls into the forward position.
The authors have achieved fair results by modifying the side-hairline correction surgery according to the patient’s zygoma type. In patients with type 3 zygomas, side-hairline correction surgery including S-point advancement should be performed instead of zygoma reduction surgery.
In patients with type 1, 2, and 4 zygomas, the widest point of the midface on the frontal view is in the anterior malar or mid-zygomatic arch areas. Thus, the S point is obscured, and S-point advancement would not help to narrow the transverse width of the midface in such patients. The S point can only be seen in type 3 zygomas on the frontal view, where the posterior zygomatic arch is wider than the anterior zygomatic arch. Therefore, patients with type 3 zygomas would only benefit from hairline correction surgery involving S-point advancement, not zygoma reduction surgery.
By further advancing the S point, the midface can become narrower. An advancement of about 3–4 mm on each side can be made without much difficulty. When the S point is advanced by a larger amount, such as more than 4–5 mm on each side, the frontal view of the face may appear slimmer. However, the sideburns may appear wider from the lateral view, which is often seen as a masculine characteristic. Hence, proper preoperative consultations should be performed with a particular focus on the pros and cons of the procedures to better meet the patient’s specific needs.
In East Asian patients with type 1, 2, and 4 zygomas, either zygoma reduction surgery or hairline correction surgery excluding S-point advancement is the optimal method by which to achieve a slimmer midface (Figs. 10, 11).
Fig. 10.
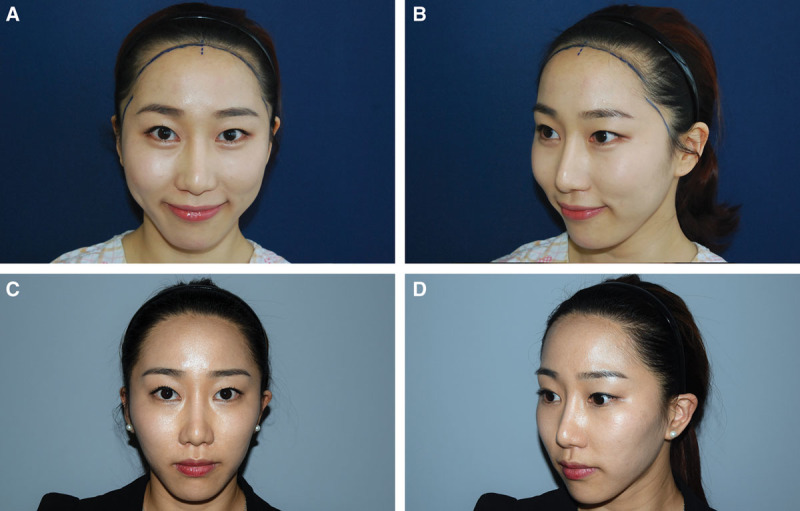
M area and side-hairline correction without S-point advancement in a 27-year-old female patient with a type 2 zygoma created a narrow facial contour. (A and B) Preoperative view. (C and D) 2-year postoperative view.
Fig. 11.
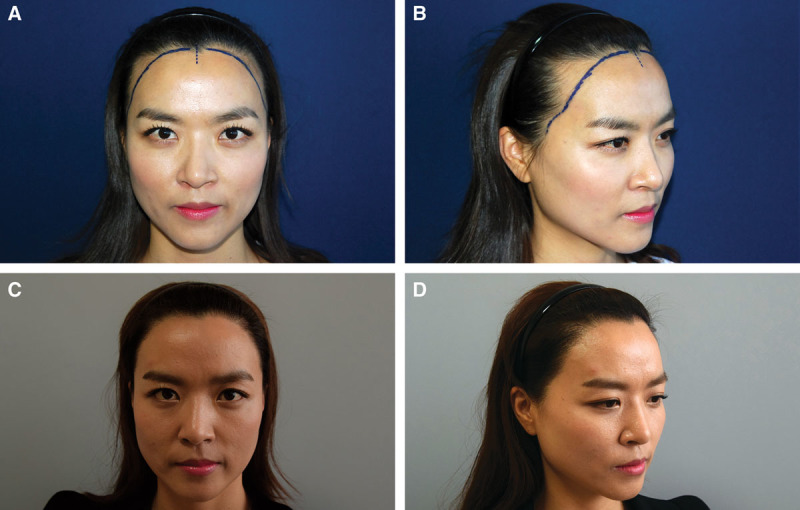
A 33-year-old female patient with a type 1 zygoma underwent M area and side-hairline correction surgery without S-point advancement, which achieved a narrow and attractive feminine facial contour. (A and B) Preoperative view. (C and D) 2.6-year postoperative view.
CONCLUSIONS
Both side-hairline correction surgery and zygoma reduction can be considered as an optimal method of creating a slimmer midface in East Asian patients. Satisfactory outcomes can be obtained by modifying the hairline correction surgery according to the patient’s zygoma shape. Various techniques may be used depending on the specific zygomatic bone structure of the patient.
Footnotes
Disclosure: The author has no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the author.
REFERENCES
- 1.Onizuka T, Watanabe K, Takasu K, et al. Reduction malar plasty. Aesthetic Plast Surg. 1983;7:121–125. doi: 10.1007/BF01571117. [DOI] [PubMed] [Google Scholar]
- 2.Baek SM, Chung YD, Kim SS. Reduction malarplasty. Plast Reconstr Surg. 1991;88:53–61. doi: 10.1097/00006534-199107000-00009. [DOI] [PubMed] [Google Scholar]
- 3.Hinderer UT. Malar implants for improvement of the facial appearance. Plast Reconstr Surg. 1975;56:157–165. doi: 10.1097/00006534-197508000-00007. [DOI] [PubMed] [Google Scholar]
- 4.Sumiya N, Kondo S, Ito Y, et al. Reduction malarplasty. Plast Reconstr Surg. 1997;100:461–467. doi: 10.1097/00006534-199708000-00031. [DOI] [PubMed] [Google Scholar]
- 5.Park JH, Moh JS. Camouflaging the posterior zygomatic arch protrusion after zygoma reduction surgery. Aesthet Surg J. 2012;32:661–664. doi: 10.1177/1090820X12448816. [DOI] [PubMed] [Google Scholar]
- 6.Jung JH, Rah DK, Yun IS. Classification of the female hairline and refined hairline correction techniques for Asian women. Dermatol Surg. 2011;37:495–500. doi: 10.1111/j.1524-4725.2011.01910.x. [DOI] [PubMed] [Google Scholar]