

Abstract
Background:
This study was aimed to compare the diagnostic accuracy and feasibility of cone beam computed tomography (CBCT) with phosphor storage plate (PSP) in detection of simulated occlusal secondary caries.
Materials and Methods:
In this in vitro descriptive-comparative study, a total of 80 slots of class I cavities were prepared on 80 extracted human premolars. Then, 40 teeth were randomly selected out of this sample and artificial carious lesions were created on these teeth by a round diamond bur no. 1/2. All 80 teeth were restored with amalgam fillings and radiographs were taken, both with PSP system and CBCT. All images were evaluated by three calibrated observers. The area under the receiver operating characteristic curve was used to compare the diagnostic accuracy of two systems. SPSS (SPSS Inc., Chicago, IL, USA) was adopted for statistical analysis. The difference between Az value of bitewing and CBCT methods were compared by pairwise comparison method. The inter- and intra-operator agreement was assessed by kappa analysis (P < 0.05).
Results:
The mean Az value for bitewings and CBCT was 0.903 and 0.994, respectively. Significant differences were found between PSP and CBCT (P = 0.010). The kappa value for inter-observer agreement was 0.68 and 0.76 for PSP and CBCT, respectively. The kappa value for intra-observer agreement was 0.698 (observer 1, P = 0.000), 0.766 (observer 2, P = 0.000) and 0.716 (observer 3, P = 0.000) in PSP method, and 0.816 (observer 1, P = 0.000), 0.653 (observer 2, P = 0.000) and 0.744 (observer 3, P = 0.000) in CBCT method.
Conclusion:
This in vitro study, with a limited number of samples, showed that the New Tom VGI Flex CBCT system was more accurate than the PSP in detecting the simulated small secondary occlusal caries under amalgam restoration.
Keywords: Cone-beam computed tomography, dental caries, dental radiograph, digital radiograph
INTRODUCTION
Dental caries can be detected by different methods such as probing, visual examination, transillumination, intra oral images including conventional films, and digital sensors.[1,2] Digital sensors comprising a phosphor storage plate (PSP), has been reported to have the same image quality of conventional films.[1,3,4,5,6] Bitewing radiographs play an important role in detecting secondary caries; however, the radiopacity of the restoration and superimposition of other structures on the carious lesion may cause misinterpretation.[7] The accuracy of bitewing images in the diagnosis of carious lesions adjacent to the class II restorations was investigated and the sensitivity was reported to be just 51.2%.[8]
Cone beam computed tomography (CBCT) is a new imaging modality for dentists to collect data and improve treatment plan's options since this new technique can demonstrate images in axial, sagittal, and coronal planes and generate three-dimensional (3D) data.[7]
CBCT images are valuable due to their convenience and simplicity in handling, and they are able to offer a set of multiplanar cross-sectional and 3D images from data yielded by a single scan.[9] Therefore, CBCT is usually used in many dental practices such as endodontics, implant assessment, orthodontics, locating the impacted teeth and assessment of the temporomandibular joints.[1,10,11]
Recently, many researchers have evaluated the supremacy of CBCT images in detecting the in vitro carious lesions. Most of them concluded that CBCT was not superior to the intraoral films, digital radiographs by charged coupled device (CCD) sensors or PSP systems for inclusive detection of proximal carious lesions.[12,13,14,15,16,17,18] However, it is still a matter of controversy whether CBCT is superior to the conventional modalities in the diagnosis of dental caries or not.[19,20,21]
In some studies, regarding the detection of non-cavitated proximal caries, the diagnostic accuracy of CBCT was similar to the PSP and conventional films.[12,15] However, another study declared that the CBCT was better in assessment of the depth of the proximal caries than the PSP and radiographic films.[22] With broad implementations of CBCT in various fields of dental practice, a guideline is published for its adoption based on the evidence-based studies. Neither this guideline nor the advisory statement from the American Dental Association,[23] recommend the CBCT for diagnosis of dental caries.[24,25]
Considering the present controversies about the accuracy of CBCT in the detection of caries and inadequate number of published research on this issue, we conducted the present study to compare the feasibility and diagnostic ability of CBCT and PSP in the detection of simulated occlusal secondary caries.
MATERIALS AND METHODS
In this descriptive — comparative experimental study, 80 non-carious non-restored extracted human permanent premolars were used. The sample teeth were extracted for orthodontic treatments.
All the teeth were randomly divided to two equal groups (n = 40); one group as the study and the other as the control group. Standard occlusal cavities were prepared on all teeth using number 245 pear diamond bur. In the study group, round bur ½ (0.6 mm in diameter-Tizkavan, Iran) was used for preparing a hole on the pulpal surface of the occlusal cavity to simulate an artificial secondary caries. The location of the artificial holes on the base of the cavity was random. In the study group, after filling the holes of each tooth with rose wax (Coltθne/Whaledent, Switzerland), the occlusal cavities were filled with amalgam (Sinalux; Dr. Faghihi, Dental Co., Iran).
The same procedure was done for the control group without artificial secondary caries preparation. All the teeth were randomly embedded in the wax blocks. Each block held four teeth consisting of one testing tooth and three non-testing teeth (one premolar and two molars) simulating the normal anatomical position. The radiographies were taken from the teeth using PSP and CBCT respectively.
The lingual surfaces of the teeth, in each block, were fixed close to the intra-oral phosphor plates (Digora Optime; Sordex, Finland) and then radiographs were taken mimicking the bitewing technique. The X-ray unit (Planmeca; Helsinki, Finland) was operated at 65 kV, 8 mA, 2.6 mm Aluminum equivalent filtration, 0.10 s exposure time, and 30 mm focal spot to film distance. A 20 mm — thick acrylic block was placed in front of the tooth block to produce soft tissue-equivalent scattering effect. The plates were scanned with a Digora Optime scanner (Soredex; Helsinki, Finland) [Figure 1].
Figure 1.
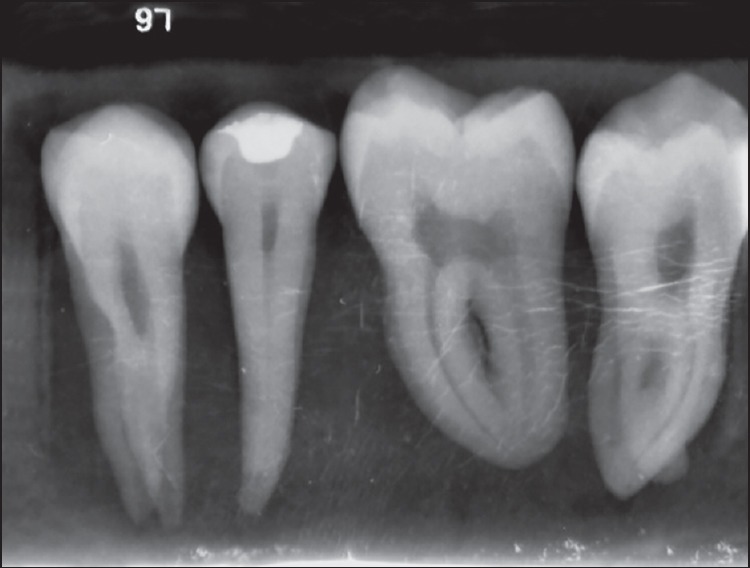
Example of a phosphor storage plate image showing the presence and absence of secondary caries
For taking the CBCT images, each block was placed on the chin rest to be radiographed using New Tom VGI Flex (Image work Co., USA) CBCT system. The CBCT system operated at 85 kVP, 3.5 mA with 6 cm × 6 cm field of view (FOV) and 5.7 s scanning time, high resolution settings and the acquired data were reconstructed with 1 mm thickness [Figures 2 and 3]. All 3D sections (axial, coronal and sagittal) were evaluated.
Figure 2.
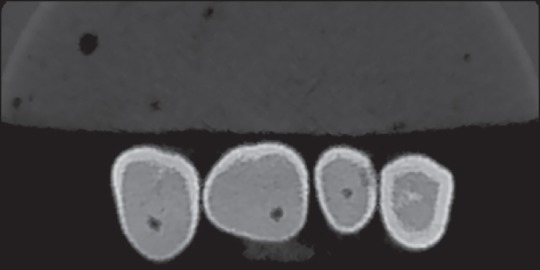
Example of an axial cut of cone beam computed tomography data showing secondary caries associated with the second premolar
Figure 3.
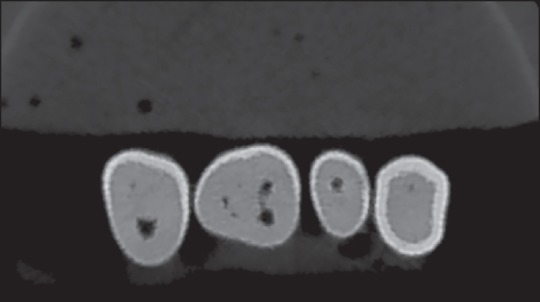
An axial cut of cone beam computed tomography data showing the pulp horn of the second premolar
Three calibrated observers, two expert Oral and Maxillofacial Radiologists and a postgraduate student of Oral and Maxillofacial Radiology evaluated all radiographs on two separate occasions with at least 1 week interval.
All images were displayed on a 19-inch LCD monitor (Dell Inc., Round Rock, TX, USA) with a resolution of 1280 × 1024 pixel in a dimmed light room. No extra adjustment of brightness and contrast were allowed.
The images were arranged in random, but it was the same for all three observers. Regarding the presence of secondary carious lesion, a 5-point confidence level was used: 1 = definitely no caries, 2 = probably no caries, 3 = questionable, 4 = probably caries, 5 = definitely caries.[7]
SPSS version 19 (SPSS Inc., Chicago, IL, USA) was adopted for statistical analysis. The area under (Az) the receiver operating characteristic (ROC) curve was used to evaluate the diagnostic accuracy. The difference between Az value of bitewing and CBCT methods were analyzed and compared by using pairwise comparison method.
Kappa analysis was used to evaluate the inter- and intra-operator agreement. Differences were considered to be statistically significant when P < 0.05.
RESULTS
A total of 80 separate PSP images from each block and 80 CBCT images were recruited in this study.
The ROC curves are demonstrated in Figure 4. The mean Az value for bitewings and CBCT was 0.903 and 0.994, respectively. Significant differences were found between PSP and CBCT (pairwise comparisons, P = 0.010). We experienced that axial images with biggest Az value were more useful. The kappa value for inter-observer agreement was 0.68 and 0.76 for PSP and CBCT respectively.
Figure 4.
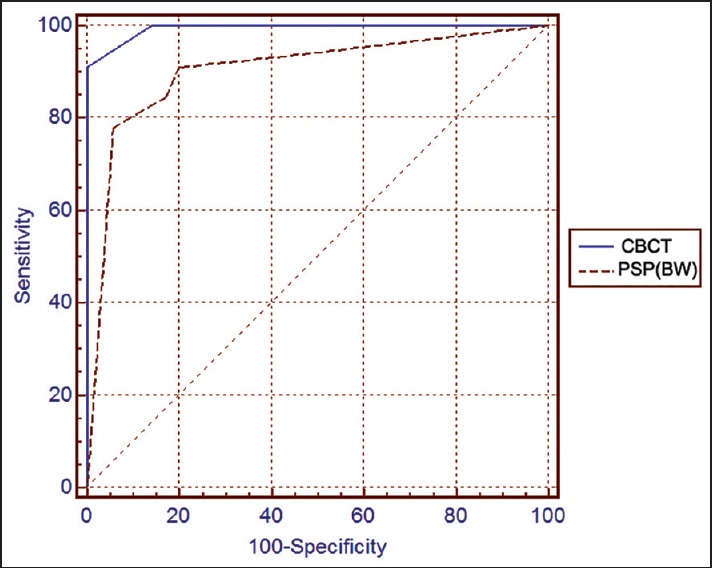
Receiver operating characteristic curves for the combined observer performances in each imaging system
The kappa value computed for intra-observer agreement, was 0.698 (observer 1, P = 0.000), 0.766 (observer 2, P = 0.000) and 0.716 (observer 3, P = 0.000) in PSP method, and 0.816 (observer 1, P = 0.000), 0.653 (observer 2, P = 0.000) and 0.744 (observer 3, P = 0.000) in CBCT method.
DISCUSSION
With favorable applicability of CBCT images in many clinical situations, CBCT provides a satisfactory resolution for dental and maxillofacial diagnosis and emits a rather low dose of radiation when compared with computed tomography (CT) used in conventional medical radiology. Since dental radiography is the most possible method for detecting proximal carious defects and that the clinical practice of CBCT should be optimized, it would be justified to compare the diagnostic accuracy of digital radiological images with images obtained by CBCT technique.[26]
In the present study, three observers evaluated 80 teeth with occlusal amalgam fillings and found that the diagnostic accuracy of CBCT images (Az= 0.994) was significantly higher than that of the bitewing radiographs (Az= 0.903).
Few studies have been enrolled regarding caries detection by using CBCT and comparing whether the CBCT systems are superior to the conventional methods or not and this is why this issue is still a matter of controversy.[12,13,14,15,16,17,18,19,20,21,27]
It seems that up to now, only one study revealed that CBCT was more accurate in estimating lesion depth than a film and a PSP system,[22] and another study showed that CBCT had higher sensitivity in detecting the dentinal caries compared to the CCD digital sensors.[18]
Kayipmaz et al.[12] studied both proximal and occlusal surfaces to compare CBCT images with ekta-speed film and PSP. They observed that CBCT was superior to the conventional radiographs and PSP in detecting occlusal caries; however, there was no significant difference between the employed techniques in detecting the proximal caries. Their voxel size was 0.2 mm thick and with respect to the slice thickness and voxel dimension, CBCT images could provide advantages in the detection of occlusal caries. Their results were in line with the findings of the current study.
Haiter-Neto et al.[14] found that the sensitivity of the two systems of CBCT (Accuitomo and New Tom) was high but their specificity was low; therefore, previous experience with CBCT images could reduce the false positive results. New Tom 3G CBCT with lower spatial resolution than the Accuitomo system had a lower diagnostic accuracy for detection of caries. It also had a lower diagnostic accuracy than Digora fmx and film. In the current study, we employed the New Tom VGI Flex CBCT system and experienced that the CBCT images yielded by this device were more accurate in finding the secondary occlusal caries than PSP system.
Kamburoğlu et al.[13] compared the usefulness of intra oral digital CCD sensor images with CBCT images (with different voxel resolutions) in occlusal caries detection. The authors concluded that CBCT images of all voxel sizes could be used in detecting the occlusal caries.
Charuakkra et al.[7] compared the Pax 500ECT and Promax CBCT systems with conventional film-based bitewing technique. They observed one hundred and twenty proximal surfaces with class II cavities restored with composite and amalgam restorations and concluded that CBCT images were better than bitewing radiographs in detection of artificial secondary caries. They also found that axial cuts are more favored sections to study. Eventhough their study were conducted on the proximal caries, their results were concurrent with our findings. It is noteworthy that we employed the New Tom VGI Flex CBCT system in our study.
The Az value of CBCT images in our study (0.903) was similar to that of Charuakkra et al. study,[7] but the Az value obtained for bitewing images in our study was higher than their study. They used F-speed films while we employed PSP imaging system.
The Az values of the CBCT images and bitewing images in our study were higher than the values obtained by Kayipmaz et al.[12] study. The possible explanation would be the smaller FOV used in the current study.
Park et al.[19] reported the superiority of CBCT systems in detection of occlusal caries and deep lesions. However, they believed that the enrolled studies regarding this issue did not follow a unique guideline.[19]
Metallic restorations can produce artifacts in CBCT images and negatively affect its diagnostic ability. Metal streak artifacts are dark lines beneath the margin of the amalgam restoration in CBCT images that cause misinterpretation in caries detection. Streak artifact can decrease the diagnostic quality of the CBCT images. This situation is the same as what will happen in the oral cavity. We made blocks containing four teeth with three non-testing teeth and one tooth with amalgam filling to mimic the environment of the oral cavity and the arches.[1,3,4,5,6]
We evaluated all 3D sections (axial, coronal and sagittal), and we experienced that axial images with biggest Az value were more useful, compatible with the previously published studies.[1,3,4,5,6] The most important reason for that would be the eliminated streak artifacts which were caused by each amalgam filling. Inter-operator kappa agreement value in CBCT images was higher than that for the PSP images. This shows that the diagnosis of carious lesions in the CBCT images is more accurate and that reveals the potential of new radiological technologies like CBCT in detecting a common dental problem like the secondary caries.
In the present study, secondary caries were created by a round bur, 0.6 mm in diameter, and consequently this round, well defined caries with high contrast might have caused different interpretation from typical caries. In order to create caries more similar to the natural decalcifications, artificial caries can be created chemically in the future studies.
The observers in our study were informed that artificial caries were created using a round bur on the pulpal floor of the restoration; therefore, they were expecting round well defined radiolucencies in the margin of the restoration that might have biased the observers.
Concerning the current results and also considering the radiation exposure dose, using CBCT for caries detection would be more accurate than the conventional bitewing taken by digital radiographs like PSP In clinical practice, CBCT has many likely advantages over conventional radiography, which include better image acquisition in the three dimensions (axial, sagittal and coronal) and developed accuracy.[11] CBCT delivers more accurate diagnostic information to determine the relationship of impacted third molars to the mandibular canal,[28] in linear measurements for evaluation of mandibular canal location compared to multi-slice CT,[29] and for the clinical evaluation of condylar position in patients with normal function of temporomandibular joints.[30]
Belém et al.[26] in their study stated that although CBCT is not the method of choice for detecting dental caries, dental practitioners should be aware of its practicality for detecting secondary caries, whenever this kind of imaging method is required. If the patient already has taken CBCT images, the data should be better analyzed to be used as a diagnostic aid for many pathologic lesions, including dental carious lesions. In some clinical circumstances, if the CBCT scans are available and well interpreted, no other imaging modalities need to be ordered or demanded.[26]
The authors recommend using CBCT images, taken for other reasons, for more accurate detection of secondary caries while respecting the principles of ALARA (as low as reasonably achievable) which states that bitewing imaging is benefitting from less X-ray exposures. The authors also respect the SEDENTEXCT guidelines[24] which advocate that CBCT images should not be used for caries detection.
CONCLUSION
This in vitro study, with a limited number of samples, showed the New Tom VGI Flex CBCT system (Az = 0.994) was significantly more accurate than the PSP (Az value = 0.903) in detecting the simulated secondary occlusal caries under amalgam restoration.
It is concluded from the results of this study that CBCTs, taken for other diagnostic reasons, can be evaluated for caries detection and can be included in the radiology reports and would inevitably help the referring clinicians.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.White SC, Pharoah MJ. 6th ed. St. Louis: Mosby; 2009. Oral radiology principles and interpretation. [Google Scholar]
- 2.Roberson TM, Heymann HO, Swift EJ. 6th ed. St. Louis: Mosby; 2012. Sturdevant's Art and Science of Operative Dentistry. [Google Scholar]
- 3.Hintze H, Wenzel A. Influence of the validation method on diagnostic accuracy for caries. A comparison of six digital and two conventional radiographic systems. Dentomaxillofac Radiol. 2002;31:44–9. doi: 10.1038/sj/dmfr/4600645. [DOI] [PubMed] [Google Scholar]
- 4.Hintze H, Wenzel A, Frydenberg M. Accuracy of caries detection with four storage phosphor systems and E-speed radiographs. Dentomaxillofac Radiol. 2002;31:170–5. doi: 10.1038/sj/dmfr/4600686. [DOI] [PubMed] [Google Scholar]
- 5.Møystad A, Svanaes DB, Risnes S, Larheim TA, Gröndahl HG. Detection of approximal caries with a storage phosphor system. A comparison of enhanced digital images with dental X-ray film. Dentomaxillofac Radiol. 1996;25:202–6. doi: 10.1259/dmfr.25.4.9084274. [DOI] [PubMed] [Google Scholar]
- 6.Wenzel A, Borg E, Hintze H, Gröndahl HG. Accuracy of caries diagnosis in digital images from charge-coupled device and storage phosphor systems: An in vitro study. Dentomaxillofac Radiol. 1995;24:250–4. doi: 10.1259/dmfr.24.4.9161170. [DOI] [PubMed] [Google Scholar]
- 7.Charuakkra A, Prapayasatok S, Janhom A, Pongsiriwet S, Verochana K, Mahasantipiya P. Diagnostic performance of cone-beam computed tomography on detection of mechanically-created artificial secondary caries. Imaging Sci Dent. 2011;41:143–50. doi: 10.5624/isd.2011.41.4.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Espelid I, Tveit AB, Erickson RL, Keck SC, Glasspoole EA. Radiopacity of restorations and detection of secondary caries. Dent Mater. 1991;7:114–7. doi: 10.1016/0109-5641(91)90056-5. [DOI] [PubMed] [Google Scholar]
- 9.De Vos W, Casselman J, Swennen GR. Cone-beam computerized tomography (CBCT) imaging of the oral and maxillofacial region: A systematic review of the literature. Int J Oral Maxillofac Surg. 2009;38:609–25. doi: 10.1016/j.ijom.2009.02.028. [DOI] [PubMed] [Google Scholar]
- 10.Patel S, Dawood A, Ford TP, Whaites E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J. 2007;40:818–30. doi: 10.1111/j.1365-2591.2007.01299.x. [DOI] [PubMed] [Google Scholar]
- 11.Scarfe WC, Farman AG, Sukovic P. Clinical applications of cone-beam computed tomography in dental practice. J Can Dent Assoc. 2006;72:75–80. [PubMed] [Google Scholar]
- 12.Kayipmaz S, Sezgin ÖS, Saricaoğlu ST, Çan G. An in vitro comparison of diagnostic abilities of conventional radiography, storage phosphor, and cone beam computed tomography to determine occlusal and approximal caries. Eur J Radiol. 2011;80:478–82. doi: 10.1016/j.ejrad.2010.09.011. [DOI] [PubMed] [Google Scholar]
- 13.Kamburoğlu K, Murat S, Yüksel SP, Cebeci AR, Paksoy CS. Occlusal caries detection by using a cone-beam CT with different voxel resolutions and a digital intraoral sensor. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:e63–9. doi: 10.1016/j.tripleo.2009.12.048. [DOI] [PubMed] [Google Scholar]
- 14.Haiter-Neto F, Wenzel A, Gotfredsen E. Diagnostic accuracy of cone beam computed tomography scans compared with intraoral image modalities for detection of caries lesions. Dentomaxillofac Radiol. 2008;37:18–22. doi: 10.1259/dmfr/87103878. [DOI] [PubMed] [Google Scholar]
- 15.Zhang ZL, Qu XM, Li G, Zhang ZY, Ma XC. The detection accuracies for proximal caries by cone-beam computerized tomography, film, and phosphor plates. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111:103–8. doi: 10.1016/j.tripleo.2010.06.025. [DOI] [PubMed] [Google Scholar]
- 16.Senel B, Kamburoglu K, Uçok O, Yüksel SP, Ozen T, Avsever H. Diagnostic accuracy of different imaging modalities in detection of proximal caries. Dentomaxillofac Radiol. 2010;39:501–11. doi: 10.1259/dmfr/28628723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tsuchida R, Araki K, Okano T. Evaluation of a limited cone-beam volumetric imaging system: Comparison with film radiography in detecting incipient proximal caries. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:412–6. doi: 10.1016/j.tripleo.2007.02.028. [DOI] [PubMed] [Google Scholar]
- 18.Young SM, Lee JT, Hodges RJ, Chang TL, Elashoff DA, White SC. A comparative study of high-resolution cone beam computed tomography and charge-coupled device sensors for detecting caries. Dentomaxillofac Radiol. 2009;38:445–51. doi: 10.1259/dmfr/88765582. [DOI] [PubMed] [Google Scholar]
- 19.Park YS, Ahn JS, Kwon HB, Lee SP. Current status of dental caries diagnosis using cone beam computed tomography. Imaging Sci Dent. 2011;41:43–51. doi: 10.5624/isd.2011.41.2.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wenzel A, Hirsch E, Christensen J, Matzen LH, Scaf G, Frydenberg M. Detection of cavitated approximal surfaces using cone beam CT and intraoral receptors. Dentomaxillofac Radiol. 2013;42:39458105. doi: 10.1259/dmfr/39458105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Valizadeh S, Tavakkoli MA, Karimi Vasigh H, Azizi Z, Zarrabian T. Evaluation of cone beam computed tomography (CBCT) system: Comparison with intraoral periapical radiography in proximal caries detection. J Dent Res Dent Clin Dent Prospects. 2012;6:1–5. doi: 10.5681/joddd.2012.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Akdeniz BG, Gröndahl HG, Magnusson B. Accuracy of proximal caries depth measurements: Comparison between limited cone beam computed tomography, storage phosphor and film radiography. Caries Res. 2006;40:202–7. doi: 10.1159/000092226. [DOI] [PubMed] [Google Scholar]
- 23.American Dental Association Council on Scientific Affairs. The use of cone-beam computed tomography in dentistry: An advisory statement from the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2012;143:899–902. doi: 10.14219/jada.archive.2012.0295. [DOI] [PubMed] [Google Scholar]
- 24.Fryback DG, Thornbury JR. The efficacy of diagnostic imaging. Med Decis Making. 1991;11:88–94. doi: 10.1177/0272989X9101100203. [DOI] [PubMed] [Google Scholar]
- 25.Pauwels R, Beinsberger J, Collaert B, Theodorakou C, Rogers J, Walker A, et al. Effective dose range for dental cone beam computed tomography scanners. Eur J Radiol. 2012;81:267–71. doi: 10.1016/j.ejrad.2010.11.028. [DOI] [PubMed] [Google Scholar]
- 26.Belém MD, Tabchoury CP, Ferreira-Santos RI, Groppo FC, Haiter-Neto F. Performance of a photostimulable storage phosphor digital system with or without the sharpen filter and cone beam CT for detecting approximal enamel subsurface demineralization. Dentomaxillofac Radiol. 2013;42:20120313. doi: 10.1259/dmfr.20120313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Qu X, Li G, Zhang Z, Ma X. Detection accuracy of in vitro approximal caries by cone beam computed tomography images. Eur J Radiol. 2011;79:e24–7. doi: 10.1016/j.ejrad.2009.05.063. [DOI] [PubMed] [Google Scholar]
- 28.Dalili Z, Mahjoub P, Sigaroudi AK. Comparison between cone beam computed tomography and panoramic radiography in the assessment of the relationship between the mandibular canal and impacted class C mandibular third molars. Dent Res J (Isfahan) 2011;8:203–10. doi: 10.4103/1735-3327.86041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Naser AZ, Mehr BB. A comparative study of accuracy of linear measurements using cone beam and multi-slice computed tomographies for evaluation of mandibular canal location in dry mandibles. Dent Res J (Isfahan) 2013;10:15–9. doi: 10.4103/1735-3327.111759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Dalili Z, Khaki N, Kia SJ, Salamat F. Assessing joint space and condylar position in the people with normal function of temporomandibular joint with cone-beam computed tomography. Dent Res J (Isfahan) 2012;9:607–12. doi: 10.4103/1735-3327.104881. [DOI] [PMC free article] [PubMed] [Google Scholar]