

Abstract
Background:
Quality of services, making communications with target groups, and educating them are among the most important success factors in implementation of family planning programs. Provision of public access to contraception and related methods, counseling services, and paying attention to social specification and cultures are important in promotion of service quality. With regard to applicability of health education theories and models, the present study aimed to find the impact of an educational program based on BASNEF model to choose contraceptive methods in women referring to health care centers in Minoodasht in 2012.
Materials and Methods:
This is a quasi-experimental study. Data were collected using BASNEF questionnaire by the researcher from women referring to health care centers in two groups of study and control (n = 100 in each group). Educational intervention (in the form of four educational 1-h sessions once a week during 1 month and two additional review sessions) was conducted in the form of group and face-to-face discussions and educational booklets were distributed. Data were analyzed by Chi-square, analysis of covariance (ANCOVA), paired t-test, and t-test through SPSS version 14.
Results:
After intervention, mean score of knowledge was significantly higher in the study group compared to control (P < 0.003). Intervention led to a better attitude in the study group (P < 0.0001). Mean score of subjective norms and enabling factors after intervention was significantly higher in the study group compared to control (P < 0.0001). The change in practice had a significant increase in the study group (54%) compared to control (9%).
Conclusions:
BASNEF-based educational intervention was effective in increasing women's knowledge, attitude, and practice. As family and educational facilities are among the influencing factors on contraceptive method selection, interventional planning is hoped to be based on educational model.
Keywords: BASNEF model, contraceptive method, withdrawal
INTRODUCTION
Family planning is done for future pregnancies with the goal of prevention from unplanned pregnancies,[1,2] which plays a major role in the improvement of maternal health, especially in developing countries.[3]
The negative outcome of not using a reliable contraceptive method is an unexpected pregnancy,[4] which has physical, mental, and socioeconomic destructive effects on the maternal health as well as negative consequences including mothers’ death, illegal abortions, delayed antenatal care, neonatal low birth weight, and reduction in breast feeding.[5,6] Half of the pregnancies are unplanned, resulting from not using a contraceptive method, application of an inefficient contraceptive method, fear of complications, lack of health services,[7] lack of education, lack of a constant method, and finally, failure of contraceptive methods.[8] Health problems and modern methods have been reported as the most common reason for following the traditional methods in Turkey.[9] Research shows that 70% of women have no sexual desire for a pregnancy, while 49% face unexpected pregnancies and half of them are involved in pregnancy termination method[2,10] (abortion). Although about 120 million women in the world have no desire for pregnancy, they do not use any contraception method. The related reasons have been reported as low availability of services and facilities, and spouse's or relative's disagreement. In Iran, although 5.9% of married women have no desire for pregnancy, they use no contraceptive method.[11] If a method is appropriately and constantly applied, it can have the highest efficiency. The most important factor to be considered in the selection of a method by the individuals is its efficiency.[12] Planning of better and high-quality family planning services needs actual participation of the society and is associated with the level of social recognition and knowledge of the necessity to conduct such programs and apply appropriate contraceptive methods. Family planning helps the couples regulate their number of children based on their economic and physical and mental power through knowledge, insight, and accountability, with the help of one of the contraceptive methods.[1] Women's knowledge concerning appropriate contraception is a key element in the prevention of mortality and in conducting family planning programs.[2,10] Selection of an appropriate method plays a key role in the level of learning and desire for behavior change in relation with individuals’ health and practice. The educator should primarily consider the efficiency of various educational methods and learner's educational and socioeconomic level before planning and select the most efficient educational methods accordingly.[1,13,14] Various studies concerning family planning have been conducted globally and in Iran, but fewer systematic studies using educational methods have been carried out in this issue. In fact, the value of health educational programs depends on their efficiency and proper use of health education theories and models.[15] Behavior studying models can be effective on people's approach toward healthy behaviors. Educational theories and models are responsible for defining and detecting the obstacles in behavioral change and for their adjustment with existing socio-cultural contexts.[16] BASNEF is a comprehensive and complete model which is adopted to study behaviors and plans to change them and to define the factors effective on individuals’ decision making. Based on this model, individuals develop a new behavior when they believe it is beneficial for them. Then, their evaluation leads to formation of their attitude toward their behavior. Parallel to this process, key persons in one's life can influence his/her decision for a new behavior and act either as a facilitator or as an inhibitor. Individuals’ subjective norms are determined by their beliefs. In other words, how the new behavior is confirmed or rejected by the people is important in one's mind. Combination of attitude and subjective norms leads to formation of individuals’ decision making to attain a new behavior. On the other hand, factors such as skill, money, costs, etc., can be effective on the transformation of an intention to an efficient behavior. These factors should exist prior to occurrence of a behavior.[16,17] Among the already conducted studies on BASNEF model in Iran, Sharifirad's study on breast feeding,[18] study on the effective factors on dormitory students’ smoking,[19] Taghdisi's study on safety practice of coke workers in steel mill corporation,[20] and Ebadiazar's study on prevention behavior concerning adolescents’ mental health[21] can be pointed out. What prompted the researchers to adopt BASNEF model was the fact that existing problems in other behavior change models (health beliefs, behavior intention), such as lack of consideration of subjective norms and enabling factors, have been modified in this model, and almost all factors of health belief model, behavior intention, and Precede behavioral factors have been included in it. Important elements in the selection and change of a behavior in Iran are among the important scales of BASNEF model which is specified for developing countries.[17] Literature review showed no study conducted in Iran based on BASNEF model; therefore, this study aimed to define the impact of an educational program based on BASNEF model in choosing contraceptive methods in women referring to health care centers in Minoodasht in 2012.
MATERIALS AND METHODS
This is a quasi-experimental study. The study population comprised women not using any contraceptive methods or using traditional contraceptive methods, meeting the inclusion criteria, and referring to the health care centers (number 1 and number 2 of Minoodasht) during Aug.-Sept. 2012. Based on existing studies and ethnical and cultural structures and due to lack of precise studies, the sample size was finally calculated as 100 subjects with consideration of possible number of subjects dropping out in each of study and control groups (total of 200), with a confidence level of 95% (α = 0.05, Z1-α/2 = 1.96) and a power of 80 (β = 0.20, Z1-β = 0.84). Health care centers with number 1 and number 2 were randomly assigned to the study and control groups, respectively. Due to possible contamination of the subjects, it was decided to select the subjects in the study and control groups from separate centers. The subjects were left out of the study in case of spouse's death or divorce. Minoodasht has two health care centers (number 1 and number 2) which were randomly assigned to the study and control groups. As the town is not so big and there was possibility of subjects’ contamination, the population was divided into two parts and each one of it was associated with one center. All the study and control subjects were selected from a unique center. The subjects were selected based on the inclusion criteria which were as follows: married women, Muslim, Iranian, fertility age of 10-49 years, healthy with no history of a known disease (contraindication for contraceptive methods), not using any contraceptive methods or on natural contraception (traditional), no desire for pregnancy, and literate enough to read and write. The exclusion criteria were: spouse's death, divorcee, and unwilling to participate in the study. Data collection tool was a researcher-made questionnaire including demographic characteristics and a section including age, length of marriage, education, occupation, number of pregnancies, deliveries and abortions, history of former deliveries and unexpected pregnancies, history of use of contraceptive method, and economic status, as well as a BASNEF questionnaire including six subscales of knowledge (7 questions), attitude (11 questions), subjective norms (5 questions), enabling factors (7 questions), behavior intention (2 questions), and practice (1 question). Since practice and behavior refer to selection of a contraceptive method in the present study, the behavior intention is the intention to select a method, which was measured by three questions. Practice was also determined concerning the method selection and the type of method by one question. Content validity was adopted for testing the validity of the questionnaire. To confirm reliability, the questionnaire was filled by 20 women from a target group (not attending the study), and then was modified and checked with a confidence level of 95% (Cronbach's alpha = 84%). The questions were scored as follows. Knowledge scores included seven questions and measured women's information in a multiple choice answer format. Attitude questions were 11 in number of which the first 7 were on personal beliefs and were scored 1-5 by Likert's scale as absolutely agree (score 1) to absolutely disagree (score 5), so that a positive attitude obtained a score of 1. Subjective value comprised five questions of which three were of yes/no type and two were multiple choice questions in relation to the individuals and groups effective on women's decision making. Questions on enabling factors were seven in number of which three were yes/no questions and four were multiple choice questions on the available resources and facilities, education, family support, and skills. Questions on behavior intention were three in number and were yes/no questions with the responses which showed women's intention after the intervention and were answered during follow-up of practice at 3 months after the intervention. Practice was measured by one yes/no question which was answered 3 months after the intervention during a follow-up and was considered positive if a contraceptive method was used by the w omen. All questions were scored, so that questions with correct answers were given a score of 1 and those with negative responses were given score. Questions of attitude were scored in Likert's scale, wherein the respondents chose answers of “absolutely agree,” “agree,” “no idea,” “disagree,” and “absolutely disagree” and the answers were scored 1-5 with a different value for each item. As negative and positive directions of questions should be considered in Likert's scale, an answer key was prepared to give the highest score in a positive phrase to the option of absolutely agree and vice versa. After obtaining the approval of ethics committee and on confirmation of questionnaire validity and reliability, the researcher referred to the selected centers. After obtaining authorities’ permission and consent from the women qualified for the study, the questionnaire was filled through an interview. Primary data were analyzed, and educational intervention and its content were designed through valid scientific references accordingly. After obtaining the sample size, BASNEF-based education was conducted in five intervention groups (each containing 20 subjects). The period of the intervention was 3 months in the form of four educational sessions. Firstly, group educational sessions were held face to face with women for 1 month. Then, two review sessions were held with 1- and 2-month time intervals. Finally, an educational session was held for the families (individuals effective on women's decision making). The participants were informed the Gooya telephone number 149 (for spreading health messages) and it was emphasized that they obtain most of their needed information through this source. The persons who used a contraceptive method were invited during sessions and most of the subjects’ questions were answered through group discussion. To increase subjects’ motivation, conducting course exam and quiz tests and giving gifts were considered. With regard to use of condoms, practical education also (with the help of a moulage) was conducted. During the sessions, women's knowledge of family planning programs and beliefs in relation with contraceptive methods was discussed in group discussion. BASNEF-based education improved the subjects’ knowledge through lecture method, group discussion, film show, health quizzes, practical education, and poster panel. The educational booklet and pamphlet were prepared and distributed to subjects in the intervention group. At the end of the fourth session, the timetable of families’ classes was charted out. Researchers’ phone numbers were given to the women in case they needed to contact the researchers. After women's education (four sessions), an educational class was held for the group that was already determined in pre-test (subjects’ spouses, their mothers, their mothers in law, etc.). Unexpected pregnancy complications and high-risk pregnancy were shown in a film, and the subjects were given examples of those involved in such complications and, through which the researcher tried to change subjects’ attitude. For those absent in the sessions, face-to-face education was provided at home visits. Control group was given an educational booklet. One and two months after the educational program (four educational sessions for women and one for families), two follow-up sessions were held. Three months after, post-test was conducted and all subscales of BASNEF questionnaire (knowledge, attitude, subjective norms, enabling factors, behavior intention, and practice) were filled for both groups. The obtained results were analyzed by independent t-test, Chi-square, paired t-test, McNemar, and regression tests through SPSS version 14.
Ethical considerations
The Ethics Committee of Tehran University of Medical Sciences’ Faculty of Nursing andMidwifery approved the study.
RESULTS
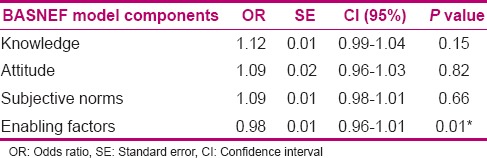
Independent t-test showed no significant difference in mean age of control and study groups [27.23 (6.22) and 27.72 (6.37) years, respectively] and mean length of marriage in the control [7.30 (5.94) years] and study groups [7.62 (6.23) years]. Findings showed that most of the subjects in the control (85%) and study (90%) groups were homemakers and their level of education was high school diploma (36% and 29%, respectively). Most of the subjects in the control and study groups (68% and 70%, respectively) had one to five pregnancies, and 27% of women in the control group and 19% in the study group had no history of pregnancy. Mean numbers of abortion in the control and study groups were 26 and 31 cases, respectively. History of unexpected pregnancy in the control and study groups was 19% and 23%, respectively. About 55% of the subjects in each group had history of contraception. Chi-square test showed no significant difference in the control and study groups concerning occupation, education, type of former delivery, history of unexpected pregnancy, and use of a contraceptive method. number 1and number 2 shows that there was no significant difference in the score of knowledge before education in the study and control groups (P = 0.291), but there was a significant difference after education (P = 0.003). Comparison of mean scores of women's attitude showed a significant difference in the study and control groups after intervention (P < 0.0001). Analysis of covariance (ANCOVA) showed a significant difference in mean scores of attitude before and after intervention in the study group (P < 0.0001). Meanwhile, this difference in the control group was not significant (P = 0.271). With regard to effect of education on enabling factors, independent t-test showed a significant difference in the study and control groups before and after educational intervention (P < 0.0001). Paired t-test showed no significant difference before and after educational intervention in the control group (P = 0.099). Meanwhile, this test showed a significant difference in the study group before and after educational intervention (P < 0.0001). Independent t-test showed a significant difference in subjective norms in the study and control groups before and after educational intervention (P < 0.0001). Paired t-test showed no significant difference before and after educational intervention in the control group (P = 0.106). Meanwhile, this test showed a significant difference in the study group before and after educational intervention (P < 0.0001) [Table 1]. McNemar test showed a significant difference in relation to spouse and health care personnel in the study group before and after educational intervention (P < 0.0001). Paired t-test showed no significant difference before and after educational intervention in the control group (P = 0.106). Meanwhile, this test showed a significant difference in the study group before and after educational intervention (P < 0.0001) [Table 2]. McNemar test showed a significant difference in relation to spouse and health care personnel in the study group before and after educational intervention (P < 0.0001), but no significant difference in relation to spouse's family, wife, and friends. This test showed no significant difference in relation to spouse, wife's family, friends, and health care personnel in the study group before and after intervention, but the difference in relation to spouse's family was significant (P < 0.0001). Chi-square test showed a significant difference in women's practice in the study and control groups after intervention (P < 0.0001) and it was the same before education in both groups (they had no contraception). Through logistic regression test and step-by-step analysis, the best subscale of BASNEF model in prediction of women's contraceptive method selection was considered. The best introduced model and its enabling factors in prediction of women's contraceptive method selection have been presented in Table 3.
Table 1.
The mean scores of different structures of BASNEF model in the two groups after intervention
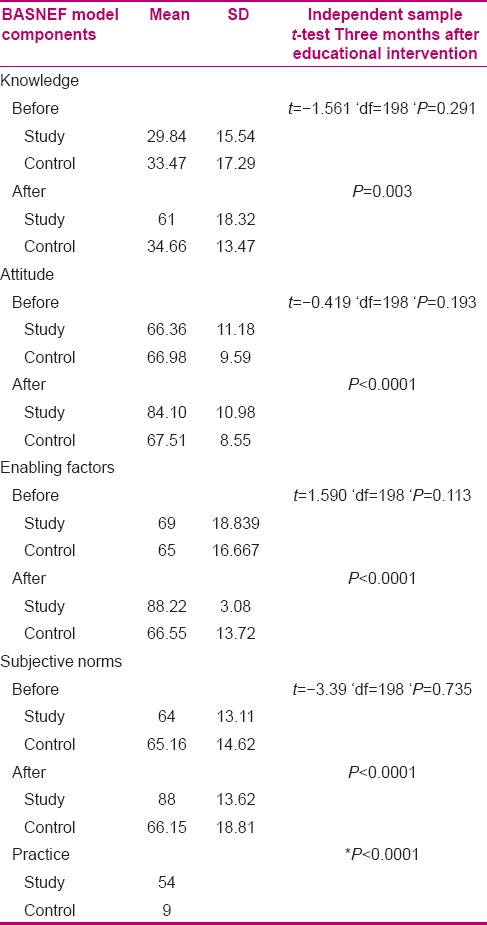
Table 2.
The mean scores of different structures of BASNEF model in two groups after intervention
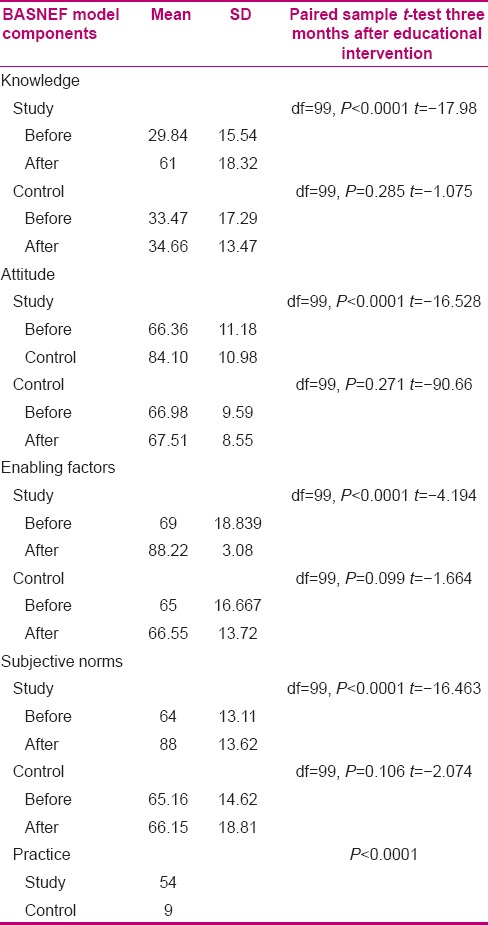
Table 3.
Step-by-step regression model of knowledge component effect on women's practice change
DISCUSSION
Nowadays, family planning is considered as the main part of life as it has a reciprocal association with health. Provision of appropriate family planning services necessitates existence of trained forces, the required facilities and equipments, and appropriate planning. The main problem in use of contraceptive methods is low knowledge and an indifferent or negative attitude toward contraceptive methods which act as the main reasons for no referrals to health care centers.[22,23] In a similar study conducted in 1985 on the effect of an educational model and women's contraceptive behavior, Robertson reported that use of health belief model directly influences the understanding, attitudes, and mental beliefs of contraception users as well as those not using any contraceptive method (25). The latter study showed that BASNEF-based educational intervention is effective on women's knowledge, attitude, and practice. Our findings showed that despite conducting education in health centers, women had low knowledge, which is consistent with the reports of Sharifirad et al. (19) and Hazavehei et al. Bogale observed that the knowledge concerning contraceptive methods was low in most of the women, which is consistent with the result of the present study.[18,24,25] Mean scores of knowledge significantly increased 3 months after intervention, which reveals the effect of BASNEF-based educational intervention on increase of women's knowledge, which is in line with the studies conducted on BASNEF model.[24,26,27] The obtained results show that the mean score of women's attitude notably increased after educational intervention in the study group, revealing the efficiency of BASNEF-based educational intervention in the domains of belief, continuity, and preservation and improvement of women's attitude toward selection of a contraceptive method, which is in line with other studies.[25,28] Bani Aghil and Khoddam showed that education through increase of knowledge leads to motivation, and attaining more knowledge and a better attitude due to educational session results in practice of using contraceptive methods.[13] Three months after intervention, the attitude showed a little increase in the control group, which can possibly be due to increase of knowledge in this group leading to a more positive attitude among them. This finding is consistent with that of Kohzadi.[28] In our study, the enabling factors showed a significant difference before and after educational intervention in the study group (P = 0.0001), which reveals the positive role of family in supporting women in using a contraceptive method. In this regard, the results of Sharifirad et al. 37 concerning breast feeding behavior of pregnant women and Pirzadeh et al. on students’ nutritional education, as well as those of Alizadeh concerning workers’ safety[29] and Mohamaei on the prevention of cardiac risk factors[30] are consistent with the results of the present study. Meanwhile, Taghdisi et al., in a study on evaluation of BASNEF model efficiency in health promotion of cancer patients, observed significant difference in enabling factors.[19,20,24,31] In the present study, enabling factors such as efficient education, time of giving service, educational facilities, and trained person had an active role in transformation of individuals’ intention to change behavior to select a safe contraceptive method, which is consistent with the report of Jeihouni et al. Laveist (1995) showed that enabling factors are much more important than cultural and behavioral differences to develop a behavior.[32,33] In the present study, mean score of subjective norms significantly increased after educational intervention in the study group. This increase resulted from BASNEF-based educational intervention conducted in the study group as well as involvement of families, especially mothers and mothers in law. In this regard, studies showed that efficient education of mothers and mothers in law through BASNEF-based education leads to increase in the participation trend of women and their behavioral change, but some influencing persons (spouse and health care personnel) showed no significant difference (P < 0.0001). Present study is consistent with Pirzadeh's study on students’ nutritional education in this regard.[34] One of the key factors in developing a behavior is the subjective nor ms. In the present study, subjective norms effective on women's behavior were detected as spouse, health care personnel, and wife's and spouse's family, respectively, which is consistent with the report of Cherkazi et al. concerning health care personnel, while Jeihouni et al. found that the most influencing persons were health care personnel, physicians, and the family.[32,35] Stewart et al., in a study in North Ireland, emphasized that improper value worsens mothers’ correct behavior; therefore, there should be a social approach in educational programs.[36] Carmack et al. conducted a study on theory of planned behavior applied to condom use among African American adolescents and found that health education models including theory of planned behavior are effective on attitude, subjective norms, and individuals’ intention either to develop or change a behavior, which is consistent with the present study.[37] The most frequent source of information was health care personnel in both groups, which reveals that these personnel play an efficient role in the selection of contraceptive method among women. Therefore, staffs’ education and their promotion of counseling skills can be effective in this regard. In some studies,[38,39] mass media was reported as the most common source of information, but it had a lean role in this regard in the present study.[30,37] In the present study, improvement of model components ultimately led to promotion of subjects’ practice in the study group, so that it raised from zero (no contraception) to 54% after intervention, which reflects the effect of BASNEF-based intervention on women's practice and is consistent with the results of other studies on BASNEF model.[40,41] In order to investigate the effect of BASNEF model subscales on the change in practice, the effect of each change on practice was, along with other factors, investigated in a regression analysis (ANCOVA), and it showed that enabling factors were the most effective factors in the components of the model. With regard to subjective norms in Iranian culture and enabling factors, use of an educational model which contains these components, like BASNEF, is recommended. With respect to the important goal of family planning program (prevention from unexpected pregnancies) and importance of mothers’ mortality (as an important index for development), it seems that if the model is precisely used, efficient steps could be taken toward prevention of unexpected pregna ncy and, consequently, improve maternal health.
CONCLUSION
There may be problems and obstacles for behavioral change, such as cultural values and norms. Educational models and patterns play a role in their definition and diagnosis, as well as their adaption to socio-cultural structures.[42] It seems that through application of BASNEF model, an association was made between women's knowledge, attitude, intention and behavior, and selection of a contraceptive method. This is a principle of BASNEF model.[16,17,43] With regard to the subjective norms in Iranian culture and enabling factors, the fallowing issues are suggested for promotion of women's health:
Holding BASNEF-based educational sessions in health centers and hospitals for women, concerning appropriate pregnancy spacing
Application of models in education
Application of BASNEF model in selection of delivery type
As the present study showed that BASNEF model is effective on women's selection and behavior concerning use of a contraceptive method, this model is suggested to be used in selection of delivery type (natural or cesarean section).
ACKNOWLEDGMENTS
Authors acknowledge the heads of health care centers and all related staffs in urban health centers in Minoodasht as well as all the participants.
Footnotes
Source of Support: Tehran University of Medical Sciences’ Faculty of Nursing and Midwifery
Conflict of Interest: None declared.
REFERENCES
- 1.Hatami H, Razavi SM, Eftekhar AH, Majlesi F, Sayed Nozadi M, Parizadeh SMJ. 2nd ed. Teharan: Argomand Press; 2008. Persian text book of public health. [Google Scholar]
- 2.McGarry KA, Tong IL. London: Lippincott WilliamsandWilkins; 2007. The 5-minute consult: Clinical compansion to womens health. [Google Scholar]
- 3.Hong R, Montana L, Mishra V. Family planning services quality as a determinant of use of IUD in Egypt. BMC Health Serv Res. 2006;6:79. doi: 10.1186/1472-6963-6-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Moos MK. Unintended pregnancies: A call for nursing action. MCN Am J Matern Child Nurs. 2003;28:24–30. [PubMed] [Google Scholar]
- 5.Bagheri A, Abbaszade F, Mehran N. Contraceptive methods in over 35-year old women and their related factors in Kashan. Journal of Kashan University of Medical Sciences. 2009;1:48–54. [Google Scholar]
- 6.Hapkins J. Family planning: A global Handbook for providers. Center for communication programs and world Health organization. 2011 [Google Scholar]
- 7.Matteson KA, Peipert JF, Maureen JA. Unplanned Pregnancy and Contraception. Am Coll Obstetricians Gynecologists. 2006 1073241. [Google Scholar]
- 8.Lete I, Doval J, Pérez-Campos E, Sánchez-Borrego R, Correa M, Viuda E, et al. Factors affecting women's selection of a combined hormonal contraceptive method: The TEAM-06 Spanish cross-sectional study. Contraception. 2007;76:77–83. doi: 10.1016/j.contraception.2007.04.014. [DOI] [PubMed] [Google Scholar]
- 9.Yurdakul M, Vural G. Reasons for using traditional methods and role of nurses in family planning. Cotraception. 2002;65:347–50. doi: 10.1016/s0010-7824(01)00313-4. [DOI] [PubMed] [Google Scholar]
- 10.Khosravi F. Ministry of Health and Medical Education (In Persian) Tehran: Ministry of Health and Medical Education; 2009. Indicators of health in the Islamic Republic of Iran. [Google Scholar]
- 11.Mirahmadi Zadeh A, Rahmanian F. Hand Book for Midwives (In Persian) Tehran: 2003. Principles of contraceptive methods. [Google Scholar]
- 12.Bani Aghil AS, Khoddam H. Impact of group and individual education of family practice of women. J Gorgan Univ Med Sci. 2005;7:46–43. [Google Scholar]
- 13.Ghasemy S. Effectiveness of family planning education program study on practical promotion women worker in Tehran. J Arak Fac Nurs Midwifery. 2001;2:24–31. [Google Scholar]
- 14.Allahverdipoor H. Passing through traditional health education towards theory oriented health education. Health Promot Educ Mag. 2005;1:75–9. [Google Scholar]
- 15.Didarlu A, Shogaeezadeh D, Mohamadian H. Tehran: Sobhan Publication; 2009. Planning health behavioral change models based on 2009. [Google Scholar]
- 16.Safari M. Tehran: Sobhan Publication; 2010. Health education theories and models of health. [Google Scholar]
- 17.Sharifirad GH, Golshiri P, Shahnazi H, Barati M, Hasanzadeh A. The impact of educational program based on BASNEF model on breastfeeding behavior of pregnant mothers in Arak. amuj. [Lastaccessed on 2012 Apr 06];2010 13:63–70. Available from: http://www.amuj.ir/browse.php?a_code=A-10-544 . 1andslclang=enandsid=1. [Google Scholar]
- 18.Sharifirad GR, Amran A. Effective factors on smoking behavior based on basnef model in dormitory students of isfahan medical sciences university. Med J Hormozgan Univ. 2008;11:267–71. [Google Scholar]
- 19.Taghdisi MH, Madadzadeh N, Shadzi SH, Hassanzadeh A. Effects of education interventions on the coke workers’ immune performances on Baznef model basis at Isfahan melting factory, 2005 Persian. Sci J Ilam Med Univ. 2008;16:24–8. [Google Scholar]
- 20.Ebadi Fard A, Solhi M, Rudbari M. Iran: Guilan University Journal; 2009. Effect of intervention through BASNEF on preventive behaviors among teenage girls in the field of mental health. [Google Scholar]
- 21.Sadeghipour Roudsari HR, Heidari AB, Ghazi Sherbaf P. Study of the rate and causes of Islam shahr urban residents avoiding to refer to the health centers for receiving health services, 2003. J Tehran Fac Med. 2005;63:150–41. [Google Scholar]
- 22.Rahimikian F, Moshrefi M, Mirmohammadali M, Mehran A, Amelvalizadeh M. Effects of emergency contraceptive methods education on the knowledge and attitudes of the health care staff. J Fac Nurs Midwifery. 2007;13:53–9. [Google Scholar]
- 23.Hazavehei SM, Khani Jyhouni A, Hasanzade A, Rashidi M. The effect of educational program based on BASNEF model on diabetic (type Π) eyes care in Kazemi's clinic, (Shiraz) Iran J Endocrinol Metab. 2008;10:145–54. [Google Scholar]
- 24.Bogale B, Wondafrash M, Tilahun T, Girma E. Married women's decision making power on modern contraceptive use in urban and rural southern Ethiopia. BMC Public Health. 2011;11:342. doi: 10.1186/1471-2458-11-342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hazavehei S, Sharifirad G, Kargar M. The comparison of educational intervention effect using BASNEF and classic models on improving assertion skill level. J Res Health Sci. 2008;8:1–11. [PubMed] [Google Scholar]
- 26.Salehi M, Kimiagar SM, Shahbazi M, Mehrabi Y, Kolahi AA. Assessing the impact of nutrition education on growth indices of Iranian nomadic children: An application of a modified beliefs, attitudes, subjective norms and enabling factors model. Br J Nutr. 2004;91:779–87. doi: 10.1079/BJN20041099. [DOI] [PubMed] [Google Scholar]
- 27.Kohzadi K. Tehran: Tehran University of Medical Sciences; 2008. The effect of education through BASNEF model on knowledge, attitude, first year students practice guidance Baneh city about oral health. [Google Scholar]
- 28.Alizadeh R, Heidari MH, Hoseini F. Tehran: Iran University of Medical Sciences; 2006. Review safety culture and the impact of educational intervention model BASNEF on improving its production line employees of the Kimia company Mahshahr Petrochemical Complex in 1384. [Google Scholar]
- 29.Mohamaei F, Nouri Tajer M, Noohi F, Maleki M. Application of BASNEF model in preventing the occurrence of risk factors contributing to myocardial infarction in patients with coronary artery disease. Iran Heart J. 2004;21:29–32. [Google Scholar]
- 30.Taghdisi M, Abdi N, Shahsavari S. Health promotion in cancer patients using the Problem based learning. Journal of Health Systems Research (Persian) 2010;7:434–41. [Google Scholar]
- 31.Jeihuni A, Hazavei M. Impact BASNEF based educational program on glycemic control in patients with type 2 diabetes. Diabete and Lipid Journal (In Persian) 2010;10:67–75. [Google Scholar]
- 32.LaVeist TA, Keith VM, Gutirrez ML. Black/White differences in Prenatal Care Utilization: An assessment of predisposing and enabling factors. Health Serv Res. 1995;30:43–58. [PMC free article] [PubMed] [Google Scholar]
- 33.Pirzadeh A, Hazavei M, Entezari M. Breastfeeding at the end of two years and the factors that affect the structure of thecityBASNEF. Journal of Health Systems Research (Persian) 2010;13:23–29. [Google Scholar]
- 34.Charkazi E, Mir Aeiz Z, Razzagh Nejad A, Shahnazi H, Hasanzadeh A, Badleh T. Breast feeding status during the first two years of infants’ life and its risk factors based on BASNEF model structures in Isfahan. J Health Syst Res. 2010;6:226–234. [Google Scholar]
- 35.Stewart- Knox B, Gardiner K, Wright M. What is the problem with breastfeeding? A qualitative analysis of infant feeding perceptions. J Hun Nut Diet. 2003;16:265–73. doi: 10.1046/j.1365-277x.2003.00446.x. [DOI] [PubMed] [Google Scholar]
- 36.Carmack CC, Lewis-Moss RK. Examining the Theory of Planned Behavior Applied to Condom Use: The Effect-Indicator vs. Causal-Indicator Models. J Prim Prev. 2009;30:659–76. doi: 10.1007/s10935-009-0199-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Amiraliakbari S, Tofighi M. Reasons for not using reliable methods of contraception in women using the withdrawal method. Mazandaran University Journal. 2005;48:92–98. [Google Scholar]
- 38.Agyei WK, Migadde M. Demographic and sociocultural factors influencing contraceptive use in Uganda. J Biosoc Sci. 1995;27:47–60. doi: 10.1017/s0021932000006994. [DOI] [PubMed] [Google Scholar]
- 39.Khalaj M, Mohammadi Zeidi E. Health ducation effects on nutritional behavior odification in primary school students. Shahrekord Univ Med Sci J. 2006;1:41–9. [Google Scholar]
- 40.Little JC, Perry DR, Volpe SL. Effect of nutrition supplement education on nutrition supplement knowledge among high school students from a low income community. J Communit Health. 2002;27:25–35. doi: 10.1023/a:1020653202522. [DOI] [PubMed] [Google Scholar]
- 41.Croyle R. 2nd ed. U.S, Jossey-Bass in San Francisc: Department of health and human services, National Institutes of Health; 2005. Theory at a Glance, A Guide For Health Promotion Practice. [Google Scholar]
- 42.Rafiee far SH. Ministry of Health and Medical Education (Persian) Tehran: Ministry of Health and Medical Education; 2004. Health education and health. Department of Community Health Education. [Google Scholar]
- 43.Begum S, Dwivedi SN, Pandey A, Mittal S. Association between domestic violence and unintended pregnancies in India: Findings from the National Family Health Survey-2 data. Natl Med J India. 2010;23:198–200. [PubMed] [Google Scholar]