

Abstract
Background:
Sexual function is reduced in an infertile woman. This study aimed to determine the effect of a communication skills training program on sexual function in infertile women referring to the medical centers in Isfahan in 2012.
Materials and Methods:
This study is a field trial study using control groups in which 32 infertile couples were selected by convenience sampling, and then, were randomly divided into control and training groups. Data were collected before (T1), 1 week after (T2), and 1 month after (T3) the training. In the intervention group, education was conducted in the form of five 3-h sessions, sequentially held with 1 week interval. Female Sexual Function Index (FISI) scale and Individual Fertility questionnaire were used to collect the data. Data were analyzed by descriptive statistical tests [t-test, analysis of variance (ANOVA), and least significant difference (LSD)].
Results:
Communication skills training increased the sexual function in infertile women. ANOVA showed that women's sexual function was significantly greater in the intervention group compared to the control group, after training. LSD test showed no significant difference in sexual function in T2 and T3.
Conclusions:
Communication skills can have a significant impact on the sexual function of infertile couples, and communication skills training can improve the quality of marital life skills through the counseling sessions conducted with infertile couples.
Keywords: Communication skills training, infertility, sexual function
INTRODUCTION
Infertility refers to failure to achieve pregnancy despite having intercourse for 1 year.[1] It is a great crisis for many individuals and can result in negative mental reactions including depression, stress, sensitivity in personal communication, feeling of loneliness, phobia, and paranoid thoughts.[2] The feeling caused by infertility, in most of the cases, ruins the couples’ mutual understanding and leads to disintegration of marital relationship.[3] One of the issues that are highly influenced by infertility is sexual relationship. In over 40% of infertile women, sexual dysfunction is observed.[4] Sexual relationship is useless and awful among infertile couples and is not a joyful activity as it is for many couples. Fertility and raising a child is an imaginable outcome of sexual function. When the infertile couples do not achieve this goal through sexual relationship, they feel doing a useless action, and a feeling of a stereotyped relationship and indifference is formed between the couples.[3] Infertile couples have lower self-esteem and complain of poor sexual function and marital satisfaction compared to fertile couples.[5] Meanwhile, satisfactory sexual relationship is an important factor to preserve an appropriate marital life, which transforms the couple to a unique unit.
Appropriate sexual relationship also increases the chance of fertility.[6] Sexual problems can occur due to various reasons. One of these problems which highly influences sexual function is the quality of couples’ relationship, as communicational problems are the most common reason for the above-mentioned reduction is sexual desire.[7] High load of mental pressure due to infertility leads to many mood changes in couples, which consequently results in their getting emotionally far from each other and lack of their appropriate relationship.[3] This inappropriate relationship can influence all dimensions of couples’ life, including their sexual function. A clear and efficient relationship among family members leads to growth of emotions and values.
Efficient relationship is essential for a healthy and successful family. In other words, when family members use efficient communicational patterns, they have a clear understanding and transition from the content and intention of each message and fulfill their mutual mental needs.
Therefore, personality communication pattern, learning, and self-confidence influence the power of selection and logical decision making of family members.[8] It can be concluded that communication skills are an important factor that influences almost all dimensions of marital life. In case of couples’ poor skills in this context, they are expected to have numerous problems in various dimensions of life.[9] Communication skills are based on four basics elements: 1) empathy, 2) language and relationship, 3) emotional expression, and 4) acceptance.[10] History of marital relationship investigation dates back to 1960. Since 1971, over 70 studies have been conducted on couples’ communications, including 40 quantitative and 31 qualitative studies. Couples’ communication programs emphasize on the dimensions of attitude and behavior to solve marital conflicts. Communication skills teach the individuals how to start a relationship, continue that and actively listen to the partner, how to express their thoughts and emotions conveniently, and how to understand the emotions of their partner in order to solve the problems constructively.[11] The factors effective in infertile couples’ sexual function have been investigated in various researches. For instance, Bahrami et al. investigated the association between depression and sexual satisfaction.[12] Effect of sexual affairs counseling has been investigated in a number of studies. Pakgohar et al. investigated the effect of sexual counseling on infertile women's sexual satisfaction.[13] Meanwhile, couples’ therapy is more important than sex therapy.[7] With regard to the infertile couples’ emotional needs and the effect of communication skills training on their relationship, and consequently, their sexual function, and due to the shortage of studies conducted in this context, the researcher decided to study this subject. Based on the above-mentioned issues, the goal in the present research is to define if communication skills training can have an effect on infertile couples’ sexual function.
MATERIALS AND METHODS
This is a clinical pre-test–post-test study with a control group. Study population comprised infertile couples who referred to Isfahan Infertility and Fertility Center and Isfahan Shahid Beheshti Infertility Center to treat their infertility in 2012. Sample size was calculated as 16 couples in each group (n = 32 people), with Confidence Interval (CI) = 95%, power = 80%, and approximate standard deviation (SD) = 5 based on previous studies and accuracy = 5.3 for each group of study and control. After consideration of subjects dropping out of the study, a total of 77 couples who met the inclusion criteria were selected through convenient sampling, and then, through random allocation, the subjects referring to the above-mentioned centers in even days were assigned to the study group and those referring in odd days were assigned to the control group. Inclusion criteria were: Iranian infertile couples speaking Persian, Minimum 6 months and maximum of 10 years has elapsed from the diagnosis of infertility, having no mental diseases, no children, no second marriage in either of the partners, no experience of severe stress in the past year, no history of marital problems, and not having to undergo any assisted reproductive techniques and intrauterine insemination (IUI) in the next month. If the treatment programs were changed for the couples and assisted reproductive techniques and IUI were considered for the couples, or if they were absent for more than one session, they were left out of the study. Data were collected by a questionnaire that contained two sections of personal and fertility characteristics and women's sexual function score, which were filled through interviews. The first section of the questionnaire inquired personal and fertility characteristics including age, occupation, education, spouse's education, cause of infertility, length of known infertility, and history of treatment failure. The second section was related to sexual function, which was measured by Female Sexual Function Index (FISI) including five-point Likert's scale type questions. Each question was scored between 1 and 5 based on the questionnaire scoring system. Total obtained score was calculated by summing up the scores. The validity of FISI has been confirmed in the study of Fakhri et al., with a high reliability (r = 0.73-0.86) and an acceptable internal consistency (α =0.72-0.9).[14] The content and number of sections of communication skills training were managed based on text books, articles, and previous research, viewpoints of the academic members of Isfahan University of Medical Sciences and the Psychology Department of Isfahan University, and were confirmed regarding scientific issues and proportion of the study population. Communication skills training courses have been conducted differently in various studies. For instance, in the study of Nazari, it was conducted in seven 1.5-h sessions[10] and in the study of Atari et al., it was conducted in eight 90-min sessions twice a week.[15] In the present study, the classes were held in the form of a workshop for five weekly 3-h sessions with a 1-week interval. Training was given in lecture and group discussion methods by the researcher who was a midwife, with the participation of a counseling psychologist. At the beginning of each session, a feedback from the former session was obtained, and the ending 15 min of each session was devoted to questions and answers. In each session, the related educational pamphlet and CD were given to the participants. During the intervention, the couples who were absent for one session were given private education, but if the couples were absent for more than one session, they were left out of the study.
Data were collected in three pre-test stages, 1 week after and 1 month after the intervention through interviews and taking notes. In the end, to follow ethical considerations, educational pamphlet and CD were also given to the control group after collection of the questionnaires in the third stage. Collected data were analyzed by SPSS version 20. Statistical tests of independent t-test, repeated measure analysis of variance (ANOVA), least significant difference (LSD) test, Chi-square test, Fisher's exact test, and Mann-Whitney test were used.
Ethical considerations
Participation in the study was voluntary and collected data was secretly and in the end of the study results was presented to the infertility centers as well as all of participants and infertility centers was appreciated.
RESULTS
A total of 77 couples entered the study, and finally, 32 couples (16 couples in the study group and 16 couples in the control group) remained and were investigated.
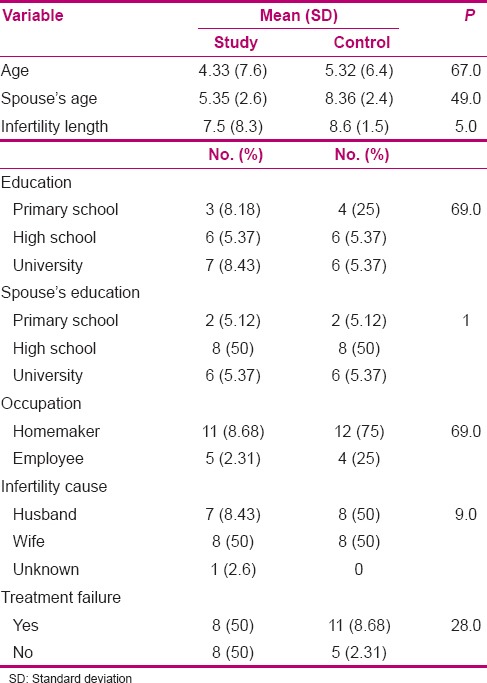
The statistical tests of Chi-square, Mann-Whitney, independent t-test, and Fisher's exact test showed no significant difference in the two groups concerning age, occupation, education, spouse's education, infertility cause, length of known infertility, and history of treatment failure, and the groups were identical (P < 0.005) [Table 1]. Mean scores of women's sexual function before education in the study and control groups were 8.26 (9.4) and 8.26 (1.5), respectively. Independent t-test showed no significant difference in the mean scores of sexual function in the two groups before intervention (P = 0.997, t = 0.001).
Summary of psycho-educational sessions on communication skills with spouses
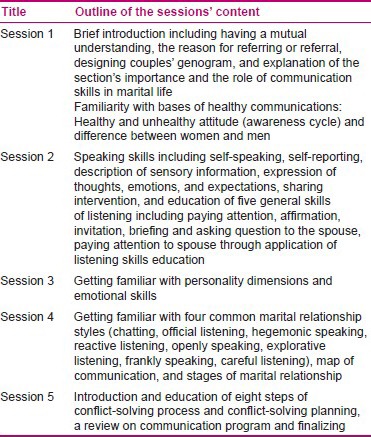
Table 1.
Personal characteristics of women referring to infertility centers of Isfahan in 2012 in the study and control groups
Mean scores of sexual function in the study and control groups changed to 9.29 (1.4) and 6.26 (9.4), respectively, 1 week after intervention and to 8.29 (4.3) and 2.27 (9.4), respectively, 1 month after intervention. Repeated measure ANOVA showed no significant difference in women's sexual function mean scores after and before intervention in the control group (P = 0.86, F = 0.93), while it showed a significant difference in the study group (P = 0.002, F = 6.9).
LSD post-hoc test showed that 1 week and 1 month after intervention, the mean scores of sexual function were similar (P = 0.8), while they increased 1 week after intervention compared to before intervention (P = 0.001) and 1 month after intervention compared to before intervention (P = 0.01).
DISCUSSION
The findings of the present study showed that communication skills training in the form of couples’ relationship program increased the sexual function of infertile women referring to infertility centers in Isfahan. One month after intervention, the findings revealed longevity of educational effect.
The obtained results are in line with those of Nazari who reported that the couples attending a relationship improvement program had higher sexual satisfaction compared to controls.[15] Rezazaheh concluded that there was a significant association between communication skills and sexual problems.[9]
The obtained findings of the present study are consistent with the results of Arnette and Smith, Gordon et al., and Larson and Holman, who showed that a communication improvement educational program increases the quality of marital life.[16,17,18]
Communication skills training teaches couples the appropriate form of relationship and improves couples’ interactions. By teaching the techniques of efficient listening, speaking and giving non-verbal efficient responses and emotional skills to the couples, their perception, recognition, and empathy, as well as their quality of relationship are improved. Objective and behavioral methods of the sessions were focused on those behaviors that occur during couples’ conflicts. Also it should be noted that components of communication skills Can manage crisis and unhappy conditions. As infertility is a great crisis in life and wrong approaches to the crisis lead to loneliness, the couples were taught to have appropriate reaction when faced with problems in life. Teaching the couples the steps of problem-solving process, in addition to helping them solve their own problems not only results in improvement of their natural relationship, their cooperation and empathy, and better recognition of their needs and desires, but also increases their interest in having a better marital relationship and reduction of tensions, and consequently, leads to making them emotionally closer to have a better sexual function.
Gholamzadeh Maryam and Attari Yousefali[19] and Chang[20] also showed that the couples attending a communication improvement program have a more emotional companionship. Another characteristic of these sessions was that this study did not emphasize on treatment of the person, According to Mesters and Johnson model; the problem of sexual relationship is faced by a couple as a two-people combination and the treatment must be related to this two-people unit.[7]
CONCLUSION
Based on the above-mentioned results, it can be concluded that the couples who have no specific sexual disorder can be helped to improve their sexual function through problem solving and communication skills education. As individuals’ beliefs about sexual problems are often negative and they are considered as a taboo, only female subjects were studied in the present study, which is an obstacle for generalization of its results to men. It is suggested to conduct a study on the efficacy of communication skills training on the sexual function of infertile men, as well as on the attitude change of infertile couples toward infertility and on the reduction of depression.
ACKNOWLEDGMENT
The authors appreciate cooperation of the academic members of Isfahan University of Medical Sciences, as well as the authorities of infertility centers and the infertile couples who attended the study. This article was derived from a master thesis of Name of student Mahboobeh Asadi with project number 392305 Isfahan University of Medical Sciences, Isfahan, Iran.
Footnotes
Source of Support: Isfahan University of Medical Sciences, 391246
Conflict of Interest: None declared.
REFERENCES
- 1.Wright K, Johanson J. Infertility. In: Gibbs R, editor. Danforths obstetrics and gynecology. 10th edn. Philadelphia: Lippincott Williams and Wilkins; 2008. p. 705. [Google Scholar]
- 2.Noorbala AA, Ramezanzadeh F, Abedinia N, Naghizadeh MM. Psychiatric disorders among infertile and fertile women. Soc Psychiatry Psychiatr Epidemiol. 2009;44:583–91. doi: 10.1007/s00127-008-0467-1. [DOI] [PubMed] [Google Scholar]
- 3.Khodakarami N, Hashemi S, Seddigh S, Hamdiyyeh M, Taheripanah R. Life Experience with Infertility; A Phenomenological Study. J Reprod Infertil. 2010;4:287–97. [Google Scholar]
- 4.Millheiser LS, Helmer AE, Quintero RB, Westphal LM, Milki AA, Lathi RB, et al. Is infertility a risk factor for female sexual dysfunction? A case-control study. Fertil Steril. 2010;94:2022–5. doi: 10.1016/j.fertnstert.2010.01.037. [DOI] [PubMed] [Google Scholar]
- 5.Pour RE, Banihashemian K. Comparison of sex disorders and couple abuse among fertile and infertile women. J Birjand Univ Med Sci. 2011;18:10–7. [Google Scholar]
- 6.Bahrami N, Sattarzadeh N, Ghojazadeh M, Soleymani MA, Sadeghi T, Kazemi H. Relation between infertility and sexual satisfaction in couples. J Qazvin Univ Med Scis Health Serv. 2010;14:5–11. [Google Scholar]
- 7.Arman S, Hassan Zahrai R. Diagnosis and treatment of sexual disorders. 1st ed. Isfahan: kankash; 2003. Treatment of sexual dysfunction. Arman S; p. 129. [Google Scholar]
- 8.Oliver J, Miller S. Couple communication. J Psychol Christ. 1994;13:151–7. [Google Scholar]
- 9.Rezazadeh SM. The relationship between communication skills and marital adjustment in students. Contemp Psychol. 2009;3:43–50. [Google Scholar]
- 10.Nazari AM. On overview of the impact of relationship enhancement program on aggression and sexual satisfaction of working women. J Women Stud. 2008;2:9–32. [Google Scholar]
- 11.Bahari F, Fatehizadeh MA, Ahmedi SA, Molavi H, Bahrami F. Effectiveness of Couple Communication Skills Training (CCST) on marital conflicts amongst conflicted divorcing couples. Res Clin Psychol Couns. 2011;1:59–70. [Google Scholar]
- 12.Bahrami N, Sattarzadeh N, Ranjbar KF, Ghojazadeh M. Comparing depression and sexual satisfaction in fertile and infertile couples. J Reprod Infertil. 2007;8:52–9. [Google Scholar]
- 13.Pakgohar M, Vizheh M, Babaee GH, Ramezanzadeh F, Abedininia N. Effect of counseling on sexual satisfaction among infertile women referred to Tehran fertility center. J Fac Nurs Midwifery. 2008;14:21–30. [Google Scholar]
- 14.Fakhri A, Mohammadi ZI, Pakpour HA, Morshedi H, Mohammadjafari R, Ghalambor DF. Psychometric properties of Iranian version of female sexual function index. J Ahvaz Jundishapur Univ Med Sci Health Ser. 2011;4:345–54. [Google Scholar]
- 15.Attari YA, Hossein PM, Rahnavard S. Effectiveness of Communication Skills (Couple Communication Program) upon Marital Dissatisfaction. Thought Behav Clin Psychol. 2010;14:25–34. [Google Scholar]
- 16.Gordon CL, Arnette AM, Smith RE. Have you thanked your spouse today? J Pers Individ Dif. 2011;50:339–43. [Google Scholar]
- 17.Yalsin BM, Karahan TF. Effects of a couple communication program on marital adjustment. J Am Board Fam Med. 2007;20:36–44. doi: 10.3122/jabfm.2007.01.060053. [DOI] [PubMed] [Google Scholar]
- 18.Lundblad AM, Hansson K. Couples therapy; effectiveness of treatment and long-term follow-up. J Fam Ther. 2006;28:136–52. [Google Scholar]
- 19.Gholamzadeh Maryam, Attari Yousefali. Study of the effect of communication skills training sessions on family function among self - Referred couples of Ahvaz well-being office in Spring -2008. Knowl Res Appl Psychol. 2009;41:87–110. [Google Scholar]
- 20.Chang YO. The effect of relationship enhancement program among Korean immigrant. J Fam Couns. 2007;13:7–10. [Google Scholar]