

Abstract
Background:
Pain is the common complication after a surgery. The aim of this study was to evaluate the effect of aromatherapy with Rosa damascena Mill. on the postoperative pain in children.
Materials and Methods:
In a double-blind, placebo-controlled clinical trial, we selected 64 children of 3–6 years of age through convenient sampling and divided them randomly into two groups. Patients in group A were given inhalation aromatherapy with R. damascena Mill., and in group B, the patients were given almond oil as a placebo. Inhalation aromatherapy was used at the first time of subjects’ arrival to the ward and then at 3, 6, 9, and 12 h afterward. Common palliative treatments to relieve pain were used in both groups. Thirty minutes after aromatherapy, the postoperative pain in children was evaluated with the Toddler Preschooler Postoperative Pain Scale (TPPPS). Data were statistically analyzed using Chi-square test, one-way analysis of variance (ANOVA), and repeated measures ANOVA.
Results:
There was no significant difference in pain scores at the first time of subjects’ arrival to the ward (before receiving any aromatherapy or palliative care) between the two groups. After each time of aromatherapy and at the end of treatment, the pain score was significantly reduced in the aromatherapy group with R. damascena Mill. compared to the placebo group.
Conclusions:
According to our results, aromatherapy with R. damascena Mill. can be used in postoperative pain in children, together with other common treatments without any significant side effects.
Keywords: Aromatherapy, children, operation, pain intensity, Rosa damascena Mill
INTRODUCTION
Nowadays, despite numerous advancements in pediatric care, many needed interventions to treat the diseases remain traumatic, painful, and disturbing.[1] Millions of people undergo surgery each year. They report that their pain after surgery is not managed.[2] Pain is not often thoroughly treated and the clients often suffer from pain after a disease or due to lack of pain management.[3] The pain caused due to any reason and not managed may lead to long-term physiologic, mental, social, and behavioral consequences. Pain is among the important nursing diagnoses in pediatric nursing for the children undergoing surgery and the health care team should prioritize pain management.[4] Therefore, the level of patients’ pain should be measured and sedatives prescribed to relieve patients’ pain.[2] Narcotics are among the medications that are routinely used in treatment of postoperative pain and can result in general side effects and signs, and are associated with tolerance and cessation-related syndrome in patients. Non-meditational methods are also used as a complementary intervention and not a replacement for meditational methods. There are methods in complementary medicine that can be used by nurses to help the patients.[4] One of the treatments with a notable growth in recent years, compared to other complementary medicine methods, is aromatherapy.[5] Research shows that aromatherapy can reduce anxiety, depression, pain, fatigue, nausea, and vomiting and can heal dermatologic lesions of diseases, although these effects have not been precisely proved.[6] For instance, inhalation aromatherapy with Bergamot in children and adolescents undergoing stem cell transplantation showed that although aromatherapy alone cannot reduce anxiety, nausea, and pain in children, it can be effective, if added to standard supportive treatments.[7] In another study, conducted in England on HIV-positive children on the effect of Lavender and Chamomile on sleep, comfort, and sedation of physical pain, the results showed that all children had a positive response to this combination, had better sleep, and their need to pain relief medications such as acetaminophen or morphine was reduced, although their pain was not thoroughly relieved.[8] Fowler Nancy states in a literature review study that the essence of sweat oranges reduced stress and relaxed the 5–14 year old children who were severely sick and underwent invasive procedures during hospitalization in Harvard University in USA.[9] In another study conducted on the effect of aromatherapy on head and face surgery postoperative distress in 6–36 month old children in three groups receiving M massage with carrier oil, M massage with tangerine oil, and postoperative standard care, the results showed no effect of the interventions.[10] The controversial studies in this context show that the effect of aromatherapy on children's pain needs further studies. With regard to the special condition in children and prohibition of usage of many types of aroma for them, the researcher, through a vast research, selected Rosa damascena Mill. as a harmless aroma for the children, which is consistent with Iranian patients’ culture and beliefs and is also available at a reasonable price in the market. R. damascena Mill. is a refreshing cardiotropic, neurotropic traditional herb, which relieves earache, sore eyes, rectum and uterus pain, and is antipyretic, anti-infective, and anti- inflammatory and edema with wound healing effect.[11,12,13,14,15,16,17,18]
In studies conducted on R. damascena Mill., its suppressing effect on sympathetic system and the reduction of blood adrenaline level have been revealed.[19] It was also observed to induce sleep in rats.[20] The doubt in the efficiency of complementary medicine has slowed down its application in the society and even among the medical society due to lack of evidence-based adequate research conducted among children. This has resulted in prohibition of these interventions in nursing care too. Therefore, the researcher decided to study the effect of aromatherapy on children's post-surgery pain intensity.
We hope these results can act as an efficient step toward recognition of complementary medicine in pediatric nursing society to suggest appropriate strategies based on the findings of this study.
MATERIALS AND METHODS
This is a clinical trial (IRCT 2014030516850N1). The obtained results were collected from two groups and in five stages, during which the effect of independent variable of type of aromatherapy on the pain intensity (dependent variable) was investigated. Baseline variables were children's sex, age, and the diagnosis. The confounding factors such as the type of surgery, history of hospitalization or surgery were controlled by random allocation in the two groups and through statistical tests. Out of control variables (limitations) included existing unpleasant smells in the ward, use of air fresheners by the accompanying persons, and open windows during aromatherapy. The subjects were selected through convenient sampling in such a way that all children hospitalized in the pediatric surgery ward of Imam Hossein and Al-Zahra hospitals and who met the inclusion criteria were selected. Inclusion criteria were: Children of age 3–6 years of both sexes, hospitalized for surgery, not having several surgical incisions, not being tr ansferred to ICU after surgery, having a caretaker, no history of respiratory diseases like asthma, sinus disorders, and rennet allergy, narcotics, tranquilizers, or benzodiazepines not used for the child by the family during 1 week prior to intervention, no respiratory allergy to any essence, perfume, or aroma in the children or in their mothers, no history of dermatologic allergy and dermatitis in the children and their mothers, no chronic pain in the children, and not applying any complementary method of medicine (aromatherapy, etc.) for the child 1 week prior to intervention. Exclusion criteria were: Lack of the child's and his/her family's interest to continue with the researcher at any stage of the study, child's discharge or death before the end of intervention, signs of dermatologic and respiratory allergy during the study, incidence of infection in the subject's surgical incision site during the study, and the subject's critical condition during the disease or the study, which stopped the intervention. Then, the subjects were assigned to aromatherapy with R. damascena Mill. group or sweet almond aroma group through random allocation until the complement of the subject's number. Sample size was calculated by the sample size formula:
Considering Z1 (confidence interval) =95% and Z2 = 80% and S =0.7, the sample size was calculated as 32 in each group (a total of 64 subjects). Immediately after subjects’ arrival to the ward from the operating room, pain intensity assessment checklist was ticked for them for the first time to measure the pain intensity. Then, the aromatherapy intervention was started with one to two drops of R. damascena Mill. extract in the study group and standardized sweet almond oil (due to having no proved respiratory effect and its frequent application in other studies as a placebo) in the other group. The essences were put on an eye pad and at the time of subjects’ arrival to the ward, were laid by the child's head at a distance of 30 cm (after the first pain intensity measurement, and then 3, 6, 9, and 12 h after surgery). Both groups also received routine postoperative care of the related surgery (taking sedation, antipyretics, and intake of fluids, electrolytes, and antibiotics and other interventions).
To investigate pain, 30 min after each aromatherapy, the pain intensity assessment checklist was ticked through 5-min observation of the child by the researcher. Pain checklist was also completed. Data collection tools were a questionnaire and a checklist.
The questionnaire contained six demographic questions including sex, age, diagnosis, type of surgery, and the history of hospitalization or surgery. The checklist for measurement the pain is Toddler Preschooler Postoperative Pain Scale (TPPPS) that was designed by Sali et al. in 1992 to measure pain among the toddlers and children by Massachusetts Medical University surgical department, and its validity and reliability have been already established (Cronbach's alpha = 0.88). This checklist includes seven items. Three items are for verbal expression of pain, three for facial expression of pain, and one for body expression of pain, with the scores being on a scale of 0–7.
All these items should be checked during a 5-min observation.[21] This checklist was ticked immediately after arrival to the ward and then at 3, 6, 9, and 12 h after surgery by the main researcher or her co-researcher. Finally, the data were analyzed by descriptive statistics and analytical tests [Chi-square, repeated measures analysis of variance (ANOVA), one-way ANOVA, and analysis of covariance (ANCOVA)] through SPSS 18.
Ethical considerations
This study has confirmations Ethics Committee (No. 3310). Informed consent was obtained from participants.
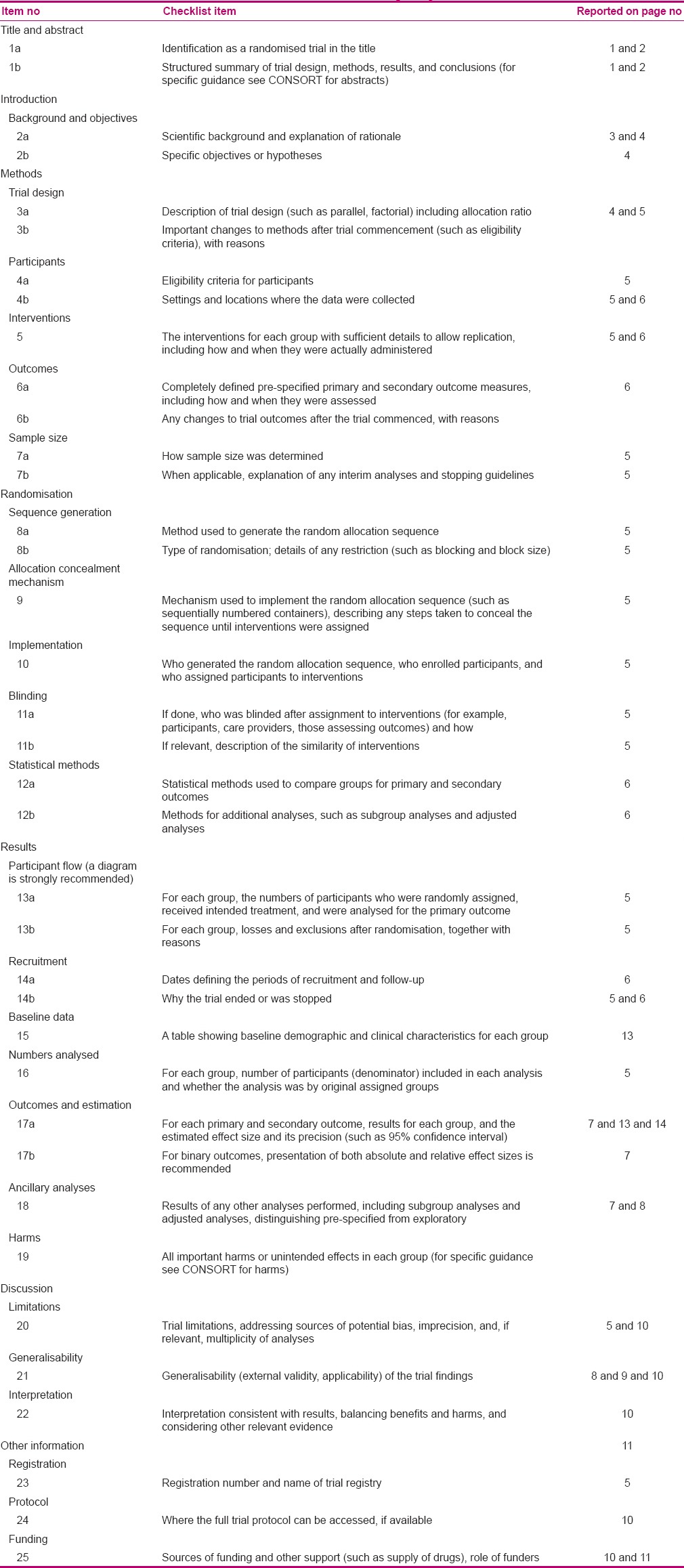
It should be noted that the details of the study are presented in Table 4 (CONSORT Table).
Table 4.
CONSORT 2010 checklist of information to include when reporting a randomized trial
RESULTS
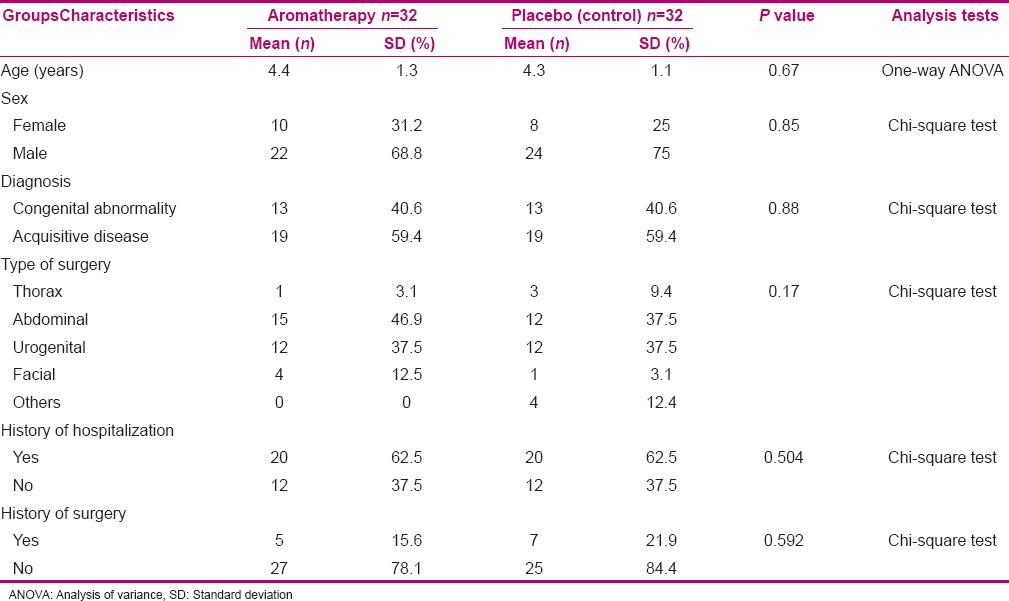
Chi-square test showed no significant difference in subjects’ demographic characteristics including age, sex, diagnosis, type of surgery, history of hospitalization and surgeries between the two groups. These findings have been presented in Table 1.
Table 1.
Demographic characteristics of the subjects in the aromatherapy and control groups
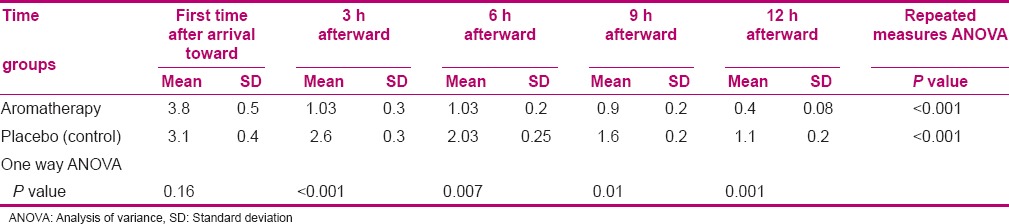
In Table 2, the two groups of study and control have been compared with each other in five time points. Intragroup comparison in the group administered aromatherapy with R. damascena Mill. revealed that the mean score of pain intensity decreased through time and showed a significant difference (P < 0.0001). The intragroup comparison in sweet almond group revealed that the mean score of pain intensity decreased through time and showed a significant difference (P < 0.001). Least significant difference (LSD) post-hoc test showed no significant difference in Rosa and sweet almond groups in the time point of immediately after arrival to the ward (P = 0.16), but in each time point of 3, 6, 9, and 12 h after arrival to the ward, the mean score of pain intensity in the Rosa group was lower than that in the sweet almond group, and the difference in the mean scores of pain intensity was significant between the two groups (P < 0.05).
Table 2.
Mean of pain intensity in different time points in the aromatherapy and control groups
DISCUSSION
The obtained results showed that pain intensity score was higher in the Rosa group at the time of arrival to the ward (before intervention), which seems normal due to disappearance of anesthesia effect and not using any intervention to relieve pain. In this group, pain intensity score showed a significant difference in different time points of 9, 6, 3, and 12 h after the surgery (P < 0.05) in such a way that it decreased after intervention with R. damascena Mill., and this decrease had a significant association with time (P < 0.001). Gharabaghi, in a study on the curing effect of R. damascena Mill. on elective cesarean section post surgery pain, obtained consistent results with the present study. The author showed that pain intensity scores in the Rosa group in time points of 12, 6, 3, and 24 h post surgery decreased and this decrease in pain intensity had a significant association with time.[22] In their study, oral capsules, containing Rosa powder, were used before anesthesia; but in the present study, R. damascena Mill. was used through inhalation. In another study, Hajhashemi et al. investigated the analgesic and anti-inflammatory effect of R. damascena hydro-alcoholic extract in animal models and reported its analgesic response in different phases after intervention in the study group compared to the control group.[23] They used the hydro-alcoholic extract of Rosa through intraperitoneal injections on animal models. Their obtained results concerning the use of Rosa and the positive analgesic effect were in line with the present study.
In the sweet almond group, the mean score of pain intensity was higher at the time of arrival to the ward (before intervention) due to reasons similar to those of Rosa group (no application of any pain relief method before aromatherapy). After aromatherapy with sweet almond oil, the mean scores of pain intensity decreased in different time points after arrival to the ward and undergoing intervention, and this reduction had a significant association with time (P < 0.001). The reduction observed in the mean score of pain intensity through time in this group was associated with the sedative and tranquilizing effect of medications such as acetaminophen, phenobarbital, etc., although both groups had routine pain relief interventions. It can possibly be due to the psychological effects of placebo too. The results of the present study showed a minor difference in the mean scores of pain intensity between the two groups at the time of arrival to the ward, which was not significant (P = 0.16). This insignificant difference between the two groups at the time of arrival and before intervention reveals the homogeneity of the subjects in both groups, as before administration of any routine intervention or aromatherapy, the groups were relatively identical concerning the pain intensity score.
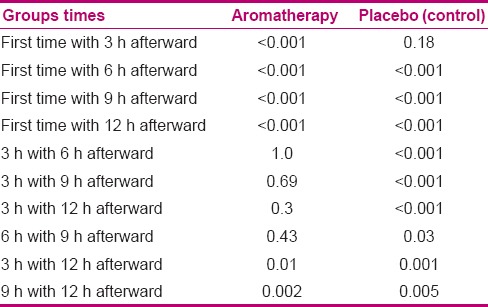
LSD post-hoc test showed a significant difference in the pain intensity scores in the two groups in time points of 3, 6, 9, and 12 h after arrival to the ward (P < 0.05), but the difference in mean pain intensity in different time points after intervention can be due to the different aromatherapy applied in the two groups. As presented in Table 3, LSD post-hoc test (in pair comparison of the time points in the two groups) showed a significant difference in just some of the time points (P < 0.05). It was such that in aromatherapy with sweet almond, the difference was not significant just for 3 h after arrival, but in Rosa group, sedative consumption and the interference of aroma with sedative effects may have influenced the steady trend of pain relief.
Table 3.
Multiple comparison of each two times in each group
Our obtained results are in line with previous studies conducted by Kim et al. with the goal of investigating the self-aromatherapy massage of the abdomen for the reduction of menstrual pain in nurses. They used the essence oil of a mixture of aromas of rose absolute (Rosa centifolia) and rose Otto (R. damascena), clary sage (Salvia sclera), rose geranium (Pelargonium), and ginger (Zingiber officinale) in a base of almond and jojoba oil for abdominal massage. Almond oil alone was used in the second group, and the subjects in the control group took acetaminophen for their pain relief. Their results showed the effect of massage with the above-mentioned mixed aromas on pain relief of menstrual pain 24 h after intervention, compared to the control group. Post-massage pain had a lower intensity compared to pre-massage pain.[24] In the aforementioned study, although a mixture containing R. damascena was used, the effect of each ingredient was not determined. In addition, massage therapy was used instead of inhalation method. In their study, only 24 h after aromatherapy and massage therapy, pain was measured. But both studies are in line with each other concerning the effect of aromatherapy in pain relief. Winter et al. (2005) investigated the effect of Rosa canina powder on relieving the signs of osteoarthritis and in the reduction of consumed medications. They gave a daily dose of 5 g of R. canina to 57 subjects in the study group for three sequential months and placebo under the same conditions to 37 control subjects. All participants were investigated concerning pain, rigidity, disability, and intensity of the disease immediately after entering the study, 3 weeks after and 3 months after starting the treatment. The authors reported a notable reduction in patients’ pain 3 weeks after treatment with Rosa in the study group compared to control. In addition, the amount of sedative consumption was significantly reduced due to intervention.[25] In their study, although a similar sort of Rosa was used for pain relief, the type and method of application, length of use, and length and method of patients’ evaluation were different from the present study. In the study of Willich et al. (2011) on the effect of R. canina on the signs of rheumatoid arthritis (RA), a daily dose of 5 g of Rosa was given to the subjects in the study group and the control group received a similar dosage of placebo. Then, the patients were investigated in an out-patient clinic for a period of 6 months. Evaluation of some parameters in RA patients, including Disease Activity Score (DAS-28) and The Health Assessment Questionnaire Disability Index (HAQ-DI), universal physicians scale, and physical scale, showed that the study group receiving Rosa recovered while the control group had either gone worse or remained in the same condition. In addition, based on some criteria such as pain intensity, the amount of medication, and patients’ mental scale showed no significant difference after this period of time in the two groups. Adding Rosa powder to routine treatments of these patients was found to be beneficial to the patients.[26] They also indicated the positive effect of Rosa in pain relief after treatment, similar to the present study, but had used a different method of intervention and powder of Rosa. The length of intervention with Rosa powder and time length and method of patients’ evaluation were different from the present study.
CONCLUSION
The findings showed the effect of R. damascena Mill. on postoperative pain in the children hospitalized in pediatric surgery wards, compared to the placebo group. Although pain intensity decreased in both groups through time, this reduction was more in the study group, compared to control. It should be noted that despite conducting a vast search for reports on Rosa aromatherapy in children, especially with regard to postoperative acute pain, no other studies were found. Therefore, in some cases, animal studies were discussed in this article. As each study is an introduction for another, this study can open the way for further studies based on its findings. It is suggested to conduct a comparative study on the effects of Rosa and rose geranium on the reduction of post-surgery sedative consumption, the preoperative anxiety in children, length of hospitalization among the children undergoing a surgery, the level of parents’ anxiety and stress before and after their children's surgery, and pain intensity in children hospitalized in other pediatric wards, and also a comparative study on the effect of Rosa and rose geranium with other protocols of children's postoperative pain management.
ACKNOWLEDGEMENT
The present study was derived from a master's dissertation (no. 392187) of the 2nd author. We greatly appreciate the vice-chancellery for research of Isfahan University of Medical Sciences and Clinical Research Development Center of Imam Hossein and Al-Zahra hospitals, Ms Samouee, the head nurse of Pediatric Surgical ward, and Dr. Mohamad Masoud Heidari, the general surgeon, who cooperated with us in this research. And we thank all nursing staff of the pediatric Sergical ward in Imam Hossein and Al-Zahra hospitals, We also thank all the children and their parents for their companionship.
Footnotes
Source of Support: Isfahan University of Medical Sciences.
Conflict of Interest: None declared.
REFERENCES
- 1.Ball JW, Bindler RC, Cowen K. 2nd ed. Pilladelphia: Elsevier Mosby; 2010. Child Health Nursing: Partnering with children and families; p. 490. [Google Scholar]
- 2.8th ed. Philadelphia: Elsevier Mosby; 2007. Phipps. Medical surgical nursing, health and illness perspectives; pp. 33–4. [Google Scholar]
- 3.Bicek E. Nurses attitudes, knowledge, and use of non pharmacological pain management techniques and therapies. 2004. [Last accessed on 2011 Jul 26]. Available from: http://www.digitalcommons.iwu.edu .
- 4.Hockenberry, Marilyn J, Wilson D. 8th ed. Pilladelphia: Lippincott Williams and Wilkins; 2011. Wong, essentials of pediatric nursing; pp. 395–965. [Google Scholar]
- 5.Marline S, Laraine K. Foundation of aromatherapy. [Last accessed on 2010 Dec 25];Lippincott. 2008 22:3–9. Available from: http://www.inlm.org . [Google Scholar]
- 6.Shutes J, Weaver C. Vol. 1. United States: Pearson Prentice Hall; 2008. Aromatherapy for body worker; p. 180. [Google Scholar]
- 7.Ndao DH, Ladas EJ, Cheng B, Sands SA, Snyder KT, Garvin JH, et al. Inhalation aromatherapy in children and adolescents undergoing stem cell infusion: Result of a placebo-controlled double-blind trial. 2010. [Last accessed on 2011 Sep 01]. Available from: http://www.wileyonlinelibrary.com . [DOI] [PubMed]
- 8.Catherin J, Kathi J. Longwood herbal task force. 2001. [Last accessed on 2011 Sep 12]. Available from: http://www.mcp.edu/herbal .
- 9.Fowler NA. Aromatherapy, used as an integrative tool for crisis management by adolescents in a residential treatment center. 2006. [Last accessed on 2011 Sep 12]. Available from: http://www.proquest.com . [DOI] [PubMed]
- 10.Jong MD. Does post operative ‘M’ technique massage with or without mandarin oil reduce infant's distress after major craniofacial surgery. 2011. [Last accessed on 2011 Sep 12]. Available from: http://www.blackwell.com .
- 11.Evans WC. 15th ed. London: WB Saunders Co; 2002. Trease and Evans’ pharmacogenosy; p. 74. [Google Scholar]
- 12.Ansari SA. Tehran: Daroupakhshrazi Co; 1992. Ekhtiaratbadiee; p. 433. [Google Scholar]
- 13.Samsamshareeat H, Moatar F. Vol. 2. Isfahan: Mashaal; 1985. Natural herbal and drag; p. 380. [Google Scholar]
- 14.Sheikh B. Ghanoondarteb. In: Sharafkandi A, editor. Vol. 2. Tehran: Soroush Publication; 1983. pp. 129–31. [Google Scholar]
- 15.Montazer R. Tehran: Culture center of IRI; 2002. Viewpoint of jorjani in headache and treatment; pp. 783–79. [Google Scholar]
- 16.Amin G. Vol. 1. Tehran: Research Center of Health Ministry; 1991. Traditional herbal drag of Iran; pp. 79–80. [Google Scholar]
- 17.Price S, Price L. 3rd ed. Philadelphia: Elsevier Mosby; 2007. Aromatherapy for health professionals; p. 341. [Google Scholar]
- 18.Ody MP. London: Dorling Kindersley; 2000. The Herbs society's complete medicinal herbal; pp. 110–1. [Google Scholar]
- 19.Haze S, Sakai K, Gozu Y. Effect of fragrance inhalation on sympathetic activity in normal adult’. Jpn J Pharmacol. 2002;90:247–53. doi: 10.1254/jjp.90.247. [DOI] [PubMed] [Google Scholar]
- 20.Rakhshandeh H, Hoseini M, Dolati K, Parsaie H. 16th ed. Tehran: Iran Physiologic and pharmacologic congress; 2003. Evaluation sleeping effect of hydro alcoholic essential of Rosa damascene mill in white mice; p. 175. [Google Scholar]
- 21.Tarbell SE, Cohen IT, Marsh JL. The Toddle Preschooler Postoperative Pain Scale for measuring postoperative pain in children aged 1-5.Preliminary report. Pain. 1992;50:273–80. doi: 10.1016/0304-3959(92)90031-6. [DOI] [PubMed] [Google Scholar]
- 22.Gharabaghi PM. Evaluation of the effect of preemptive administration of Rosa damascene extract on post operative pain in elective cesarean sections. Afr J Pharm Pharmacol. 2011;5:1950–5. [Google Scholar]
- 23.Hajhashemi V, Ghannadi A, Hajiloo M. Analgesic and Anti-inflammatory effect of Rosa demascenahydroalcoholic extract and its essential oil in animal models. Iran J Pharm Res. 2010;9:163–8. [PMC free article] [PubMed] [Google Scholar]
- 24.Kim YJ, Lee MS, Yang YS, Hur MH. Self-aromatherapy massage of the abdomen for the reduction of menstrual pain and anxiety during menstruation in nurses: A placebo-controlled. clinical trial. [Last accessed on 2013 Dec 09];European Journal of Integrative Medicine. 2011 3:165–8. Available from: http://www.sciencedirect.com . [Google Scholar]
- 25.Winther K, Apel K, Thamsborg G. A powder made from seeds and shells of a rose hip subspecies (Rosa canina) reduces symptoms of knee and hip osteoarthritis: A randomized, double blind, placebo controlled clinical trial. Scand J Rheumatol. 2005;34:302–8. doi: 10.1080/03009740510018624. [DOI] [PubMed] [Google Scholar]
- 26.Willich SN, Rossnagel K, Roll S, Wagner A, Mune O, Erlendson J, et al. Rose hip herbal remedy in patients with rheumatoid arthritis – a randomised controlled trial. Phytomedicine. 2010;17:87–93. doi: 10.1016/j.phymed.2009.09.003. [DOI] [PubMed] [Google Scholar]