

Abstract
Background:
Breast cancer is the most common cancer among women and 81% of therapeutic surgery performed for breast cancer in Iran is mastectomy. Following mastectomy, the patients suffer from many problems which lead to several disorders and decrease in their quality of life (QOL).
Materials and Methods:
This cross-sectional descriptive study was conducted on 105 breast cancer patients who underwent mastectomy, selected with a convenient sampling method. A questionnaire containing three parts was used to collect data. The data were analyzed by SPSS version 14 using descriptive and analytical statistical methods.
Results:
Spearman test showed that there was a statistically significant relationship between QOL and education level and also fatigue. Moreover, Spearman test indicated a statistically significant correlation between age and the mental dimension of QOL. There was no significant relationship between QOL with marital and employment status.
Conclusions:
Based on the findings, we can suggest that nurses should be educated about the factors affecting QOL. They can receive the necessary knowledge in various areas such as meeting the patients, optimum management of patients’ problems, improvement of their health, and finally help to increase the cancer patients’ QOL.
Keywords: Breast cancer, Iran, mastectomy, nursing, quality of life
INTRODUCTION
Breast cancer is the most common cancer in women.[1,2,3] Statistics show that globally, among every 10 women, 1 person is diagnosed with this disease. According to the American Cancer Society report published in 2007, in every 15 min, five people are diagnosed with breast cancer and one woman dies due to this case.[4] According to the report of the same organization published in 2013, among every eight women in the USA, one is affected by breast cancer and in the year 2013 alone, there were 39,620 deaths from breast cancer in the USA.[5] Breast cancer has been the cause of about 17% of deaths from cancer and it is the second leading cause of death from cancer after lung cancer.[6,7] According to the overall statistics of the country, in Iran, breast cancer has been the most common cancer in women[8,9] and nearly 6160 new cases are reported each year. Of these, 1063 people died due to this disease.[9]
Surgical treatment is the most common treatment of breast cancer.[10] According to the statistics obtained from Iran, mastectomy comprises 81% of breast surgeries in the country.[11,12] The effect of breast cancer and its treatments such as mastectomy on a patient includes psychological discomfort, especially mood disorders, depression, anxiety, anger, fear about the body image, and in general, its influence on the quality of life (QOL) which is greatly reduced after breast surgery.[13,14] Results of several studies showed that the women who had undergone mastectomy compared with women who have had breast conserving surgery had a significantly lower QOL.[15,16] QOL of a person is related to all the factors associated with cancer named as cancer properties.[17] With respect to the components such as the increased incidence of breast cancer, the high degree of impact of this disease on all aspects of people's lives, increase in the average rate of survival seeking medical advances, several complications of mastectomy, and adverse effects on the QOL, and similarly, with regard to the undeniable position of women at home and family and rapid transmission of disease consequences to the other members of the family, evaluation of QOL and related factors would help the community of health workers to organize activities for health promotion and improve the QOL of these patients. Therefore, the researchers decided to design and conduct a study with the aim of investigating the physical, mental, social, and spiritual aspects of QOL and related factors in women with breast cancer who had undergone mastectomy.
MATERIALS AND METHODS
This descriptive, correlational, cross-sectional study was conducted on 105 patients with breast cancer who had undergone mastectomy. They were enrolled in the study during 7 months of 2012 in Sayyed Al-Shohada Hospital affiliated to Isfahan University of Medical Sciences through convenient sampling method.
The inclusion criteria for the studied subjects were: Age more than 18 years, definitive diagnosis of cancer by a specialist physician, having undergone mastectomy surgery (passing of at least 1 year and a maximum of 5 years), and having no known mental problems and not being treated with psychotropic drugs.
In order to gather the required information, a three-part questionnaire was used. The first part was related to demographic variables. The second part of the questionnaire included a checklist that consisted of four items: 1. Did you need to relax? 2. Did you have trouble with sleeping? 3. Did you feel weak? 4. Did you get tired? This section was used to assess fatigue over the past week.
The third part was the National Medical Center and Beckman Research Institute questionnaire (NMCBRI-Q) related to the QOL in women with breast cancer. The NMCBRI-Q contains 44 items and consists of four subscales: Physical, mental, social, and spiritual. Based on the respondent's choice, each item was scored from zero to 10. Score of zero was assigned to the worst case and the best score was 10. The highest possible overall score from this tool was 440 and the lowest score was zero. Test-retest method was used in order to determine the reliability of this questionnaire. Correlation coefficient between the two times of answering the questions was determined as 85%, respectively. The validity of this questionnaire as a measure of QOL is well established. For instance, in the study of Khajeh Aminian et al., the content validity was ascertained and findings revealed good and sufficient validity. Its reliability has been approved by the internal consistency method using Cronbach's alpha of 0.80.[18]
The checklist to assess fatigue was composed of four extracted items from the quality of life questionnaire for Cancer patients (QLQ-C) standard questionnaire and was scored with a 4-point Likert's scale. This checklist was used after confirming the validity content. The reliability of this checklist has been validated in patients with breast cancer and its Pearson's correlation coefficient obtained through test and re-test method with a 2-week interval was 89%.
Considering the ethical considerations and after obtaining the consent of the patients, the researchers began to complete the questionnaires. Literate patients completed the questionnaires by themselves and for the rest of the patients, they were completed through interviewing method. The data were analyzed after collection and coding through software SPSS version 14, SPSS Inc., Chicago, IL, and descriptive (frequency distribution, mean, standard deviation) and analytical statistical methods [analysis of variance (ANOVA) test, Pearson's and Spearman's correlation coefficients] with 95% confidence interval.
RESULTS
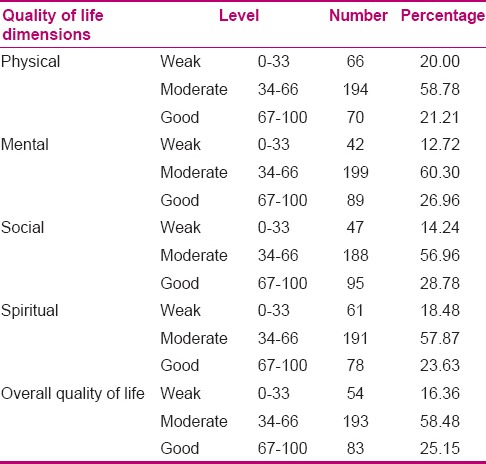
According to the findings of this study, the mean age (SD) of the studied samples was 45.3 (4.6) years with the age ranging from 18 to 66 years. Majority of the study subjects were at stage II of breast cancer (50%). The majority of them (80%) had undergone the surgery of modified radical mastectomy. Relative frequency distributions of the QOL in the studied samples are presented in Table 1. As shown in the table, the QOL for the majority of patients was moderate regarding all aspects. Overall mean QOL was moderate (58.48%) in the studied subjects with regard to the four above-mentioned dimensions.
Table 1.
Absolute and relative frequency distribution of quality of life in women with breast cancer who had undergone mastectomy
The findings of the present study showed that there was no statistically significant relationship between demographic information and features of the disease, such as breast cancer stage, marital and employment status with the QOL. In fact, one-way ANOVA test indicated that there was no statistically significant relationship between the QOL and the marital status (F = 0.32, P = 0.82) and employment status (F = 0.50, P = 0.67). Spearman's test showed that there was a statistically significant relationship between the QOL and the academic status (r = 0.54, P = 0.004).
There was no significant relationship between age and overall score of life quality. However, the findings indicated a significant relationship in terms of the mental dimension of QOL (r = 0.44, P = 0.005). The findings also showed that there was a significant relationship between fatigue and quality of life (QOL) (r = −0.48, P = 0.004). According to the results of the present study, there was no statistically significant relationship between QOL and the type of surgery (modified radical, simple, or partial mastectomy).
DISCUSSION
The findings of the present study show that the QOL of the majority of subjects was moderate. Fazel and colleagues showed that QOL of the majority of women with breast cancer who had undergone mastectomy was moderate at 56%,[19] which was perfectly consistent with the findings of this study.
Nematollahi indicated that the QOL of the majority (66%) of women with breast cancer was moderate.[20] This finding was consistent with the result of the present study. However, in the study of Nemati and colleagues, it was found that QOL for the majority of the studied subjects (87.5%) was lower than moderate level.[21] This difference may be due to the difference in study populations (in the study of Nemati, adolescents with leukemia and in the present study, women with breast cancer who had undergone mastectomy) and also the significant differences in the number of samples (40 patients in the study of Nemati and 105 patients in this study).
In the study of Agha Barari et al., the QOL was found to be moderate in patients with breast cancer in terms of emotional and social dimensions, which is consistent with the findings of the present study.[22] The results of Nematollahi's study also confirmed the findings of the present study.[20]
There was a significant relationship between the education level and the QOL of the patients with breast cancer. An increase in education level of the studied subjects increased the QOL scores and it confirmed the results of the present study. In the study of Shim et al., there was a direct significant relationship between the patient's level of education and their QOL.[23]
There was no significant relationship between age and QOL of women with breast cancer, whereas there was a direct statistically significant relationship between age and the mental aspect of QOL. In the studies of Bakhshi et al.[24] and Nemati et al.,[21] there was no relationship between age and QOL, which was in line with the present study results. In the study of Shim et al., there was no statistically significant relationship between age and QOL.[23] In the context of a meaningful relationship between age and mental aspects of QOL, the findings of Agha Barari et al.'s study were consistent with these results.[22] In justifying the direct observed relationship between age and mental aspects of QOL, it can be said that perhaps in younger women, more aggressive treatments have been used for disease control. This condition has been probably interpreted as a serious illness and the patients are told about the impossibility of a full recovery. This problem has caused more psychological complications in these patients. On the other hand, employment of women at a younger age and accepting more family responsibilities and raising the children are compounded by the lengthy process of treat ment. They cannot assume these responsibilities the same way as in the past. Thus, tensions and stress arise in them and diminish their QOL.[22]
The results showed that there was a significant relationship between fatigue and QOL. The women who had undergone mastectomy with higher levels of fatigue had lower QOL mean scores. The findings of Safaei et al. also confirmed that there was a relationship between the areas of QOL and the intensity of fatigue in patients with cancer.[25] The findings were also consistent with other studies in this regard.[26,27] On the other hand, the results of Holzner's study have shown that there was no significant relationship between fatigue and QOL of the studied patients.[28] Possible reasons for these differences could be due to the difference in sample size, the tools used, sampling method, type of treatment regimen, and different stages of treatment of patients.
According to the results of the present study, there was no statistically significant relationship between the QOL and the type of mastectomy surgery. Dorval et al. showed that there was no statistically significant relationship between the type of mastectomy surgery and the QOL in the long term, which confirms the findings of the present study.[29]
CONCLUSIONS
The results of the present study showed that the QOL was moderate for the majority of subjects in the study. Therefore, the participating patients in this study, more than anything else, needed social, emotional, and spiritual support for completion of their therapies with less stress.
On the other hand, according to the results of the present study, there was a relationship between some features of the disease and demographic information with the QOL of the patients, thus they act as predictive factors of QOL. Therefore, it is suggested that nurses receive the necessary training through academic courses and establishment of workshops to gain knowledge of the factors affecting the QOL. They will be able to benefit from training with a logical approach and have a complete knowledge. They should receive knowledge in areas such as correct management of patients, optimal management of problems, disease complications and treatment, health promotion, and finally, improving the QOL of the patients with cancer.
ACKNOWLEDGMENTS
The authors appreciate all the participating patients of the present study, the nurses for their sincere assistance, and other distinguished personnel of Sayyed Al-Shohada Hospital affiliated to Isfahan University of Medical Sciences for their cooperation in this research.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–917. doi: 10.1002/ijc.25516. [DOI] [PubMed] [Google Scholar]
- 2.Perry SH, Kowalski TH, Chang CH. QOL assessment in women with breast cancer: Benefits, acceptability and utilization. Health Qual Life Outcomes. 2007;2:1–8. doi: 10.1186/1477-7525-5-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Carlan G, Nigard H. 10th ed. Chapter 56. Philadelphia: Lippincott Williams & Wilkins; 2010. Disease of women and obstetrics (Danforth 2008) pp. 1219–67. [Google Scholar]
- 4.Ghazi B, Zonozi A, Bahrami N, editors. 1st Ed. Chapter 6,12,13. Tehran: Avizhe Pubs; 2007. Bereck and Novak. Women Disease; pp. 125–331. 122-398, 330-56. [Google Scholar]
- 5.Atlanta, Ga: American Cancer Society; 2013. [Last accessed on 2013 Aug 11]. American Cancer Society. Cancer Facts and Figures 2013. Available from: http://www.cancer.org/cancer/breastcancer/detailedguide/breast-cancer-key-statistics/ [Google Scholar]
- 6.kistner K. Women disease and health essential. In: Ghazi JB, Nashere G, editors. 3rd ed. Michigan: Mosby Elsevier; 2005. pp. 229–48. [Google Scholar]
- 7.Okobia MN, Bunker CH, Okonofua EF, Osime U. Knowledge, attitude and practice of Nigerian women towards breast cancer and mammography in breast cancer screening. A cross-sectional study. J Surg Oncol. 2006;4:1–9. doi: 10.1186/1477-7819-4-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Khani H, Moslemizade N, Montazeri A, Godazande Gh, Ghorbani A. Knowledge, attitude & performance of health care staff about breast cancer prevention programs in southern border of khazar seal (Caspian sea) Iranian Journal of Breast Disease. 2008;1:28–37. [Google Scholar]
- 9.Akbari ME, Mirzaei HR, Soori H. 5 year survival of breast cancer in Shohada-e-Tajrish and Jorjani hospitals. Hakim Res J. 2006;2:39–44. [Google Scholar]
- 10.Smeltzer SC, Bare BG. 9th ed. Philadelphia: Lippincott; 2000. Bronner and suddarth Text Book of medical surgical nursing; p. 272. 297,301. [Google Scholar]
- 11.Najafi M, Ebrahimi M, Kaviani A, Hashemi E, Montazeri A. Breast conserving surgery versus mastectomy: Cancer practice by general surgeons in Iran. BMD Cancer. 2005;5:35. doi: 10.1186/1471-2407-5-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Weitzner MA, Meyers CA, Stuebing KK, Saleeba AK. Relationship between Mood and QOL in Long- Term survivors of breast cancer treated with Mastectomy. J Psychosoc Oncol. 1997;5:241–8. doi: 10.1007/s005200050067. [DOI] [PubMed] [Google Scholar]
- 13.Kissane DW. Psychological morbidity and QOL in Australian women with early stage of breast cancer: A cross sectional survey. Med J Aust. 1998;169:192–6. doi: 10.5694/j.1326-5377.1998.tb140220.x. [DOI] [PubMed] [Google Scholar]
- 14.Shimozuma K, Ganz PA, Petersen L, Hirji K. QOL in the first year after breast cancer surgery: Rehabilitation needs and patterns of recovery. Breast Cancer Res Treat. 1999;56:45–57. doi: 10.1023/a:1006214830854. [DOI] [PubMed] [Google Scholar]
- 15.Engle J, Kerr J, Schlesinger-Raab A, Sauer H, Holzel D. QOL following breast conserving therapy or mastectomy: Results of a 5- Year prospective study. Breast J. 2004;10:223–31. doi: 10.1111/j.1075-122X.2004.21323.x. [DOI] [PubMed] [Google Scholar]
- 16.Morasso G, Gostantini M, Viterbori P, Bonci F, Del Mastro L, Musso M, et al. Predicting mood disorders in breast cancer patients. Eur J Cancer. 2001;37:216–23. doi: 10.1016/s0959-8049(00)00390-7. [DOI] [PubMed] [Google Scholar]
- 17.Hasanpour Dehkordi A, Shaaban M. Relationship between cancer characteristics and QOL in the cancer patients under chemotherapy referred to selected clinic of Tehran university of medical sciences. Shahrekord Univ Med Sci J Winter. 2005;6:63–71. [Google Scholar]
- 18.Khaje Aminian MR. Iran: Nursing and Midwifery Faculty of Isfahan University of Medical Sciences; 2008. Effect of exercise on QOL in the patients with cancer under chemotherapy referred to Seido Alshohade Hospital of Isfahan University of Medical Sciences 2008. [Google Scholar]
- 19.Fazel B, Tirgari N, Mokhber M, Koushyar H, Esmail y. The effect of mastectomy on mood and QOL in breast cancer patients. J Shahid Sadoughi Univ Med Sci Health Serv. 2008;16:28–36. [Google Scholar]
- 20.Nematollahi A. Iran: Nursing and Midwifery Faculty of Tehran University of Medical Sciences; 2004. QOL in the breast cancer patients referred to selected clinic of Tehran University of Medical Sciences. [Google Scholar]
- 21.Nemati M, Alhani F, Zandshahri R. Iran: The First Congress of QOL in Tarbiat Modares University; 2005. QOL in the adolescence with cancer under chemotherapy referred to selected clinic of Tehran University of Medical Sciences; p. 25. [Google Scholar]
- 22.Aghabarari M, Ahamadi F, Mohammadi E, Hajizadeh E, Farahani AV. Physical, emotional and social dimension of QOL among breast cancer women under chemotherapy. Iran J Nurs Res. 2007;1:55–65. [Google Scholar]
- 23.Shim EJ, Mehnert A, Koyama A, Cho SJ, Inui H, Paik NS, et al. Health related QOL in breast cancer: A cross cultural survey of German, Japanese and South Korean patients. Breast Cancer Res Treat. 2006;99:341–50. doi: 10.1007/s10549-006-9216-x. [DOI] [PubMed] [Google Scholar]
- 24.Bakhshi R, Davachi A, Kamali P. Iran: Nursing and Midwifery Faculty of Iran university of Medical Sciences; 2000. Effect of nurse counseling on QOL among women with breast cancer treated with radiotherapy at the Cancer Institute of Tehran in 2000, master of Sciences Nursing Thesis. [Google Scholar]
- 25.Safaee A, Tabatabaee SH, Moghimi-Dehkordi B, Zeighami B. Cancer-related fatigue in breast cancer patients under chemotherapy. Koomesh J Semnan Univ Med Sci. 2010;11:317–22. [Google Scholar]
- 26.Littlewood TJ, Kallich JD, San Miguel J, Hendricks L, Hedenus M. Efficacy of darbepoetin alfa in alleviating fatigue and the effect of fatigue on QOL in anemic patients with lymphoproliferative malignancies. J Pain Symptom Manage. 2006;31:317–25. doi: 10.1016/j.jpainsymman.2005.08.013. [DOI] [PubMed] [Google Scholar]
- 27.So WK, Dodgson J, Tai JW. Fatigue and QOL among Chinese patients with hematologic malignancy after bone marrow transplantation. Cancer Nurs. 2003;26:211–9. doi: 10.1097/00002820-200306000-00006. [DOI] [PubMed] [Google Scholar]
- 28.Holzner B. QOL in breast cancer patient not enough attention for long-term survivors. J Psychom. 2001;42:117–23. doi: 10.1176/appi.psy.42.2.117. [DOI] [PubMed] [Google Scholar]
- 29.Dorval M, Maunsell E, Desche L, Brisson J. Type of Mastectomy and Quality of Life for Long Term Breast Carcinoma Survivors. Cancer. 1998;83:2130–8. doi: 10.1002/(sici)1097-0142(19981115)83:10<2130::aid-cncr11>3.0.co;2-8. [DOI] [PubMed] [Google Scholar]