

Abstract
Somatostatin (SST) receptors (SSTRs) belong to the typical 7-transmembrane domain family of G-protein-coupled receptors. Five distinct subtypes (termed SSTR1-5) have been identified, with SSTR2 showing the highest affinity for natural SST and synthetic SST analogs. Most neuroendocrine tumors (NETs) have high expression levels of SSTRs, which opens the possibility for tumor imaging and therapy with radiolabeled SST analogs. A number of tracers have been developed for the diagnosis, staging, and treatment of NETs with impressive results, which facilitates the applications of human SSTR subtype 2 (hSSTr2) reporter gene based imaging and therapy in SSTR negative or weakly positive tumors to provide a novel approach for the management of tumors. The hSSTr2 gene can act as not only a reporter gene for in vivo imaging, but also a therapeutic gene for local radionuclide therapy. Even a second therapeutic gene can be transfected into the same tumor cells together with hSSTr2 reporter gene to obtain a synergistic therapeutic effect. However, additional preclinical and especially translational and clinical researches are needed to confirm the value of hSSTr2 reporter gene based imaging and therapy in tumors.
1. Introduction
Somatostatin receptors belong to the typical 7-transmembrane domain family of G-protein-coupled receptors [1]. Five distinct subtypes (termed SSTR1-5) have been identified, with SSTR2 showing the highest affinity for natural SST and synthetic SST analogs [2]. Most NETs, including pituitary adenoma, gastroenteropancreatic tumor (GEP-NET), pheochromocytoma, neuroblastoma, paraganglioma [3, 4], medulloblastoma [5], and medullary thyroid carcinoma [6], have relatively high expression levels of SSTRs, which opens the possibility for tumor imaging and therapy with radiolabeled SST analogs. A number of tracers have been produced due to encouraging initial results from the applications of radiolabeled ligand-receptor systems [7, 8]. The most commonly used radiopharmaceutical for somatostatin receptor scintigraphy (SRS) is [111In-DTPA0]octreotide, which has proven its role in the diagnosis and staging of NETs [9]. Favorable results also have been observed in NET imaging using other γ-emitting tracers like 99mTc-Depreotide and [111In-DOTA]lanreotide [10, 11]. More recently, positron-emitting radiotracers have been developed and seem to be more promising. 68Ga-DOTA-peptides used for positron emission tomography (PET) or positron emission tomography/computed tomography (PET/CT) imaging of NETs have been reported by various research groups with higher sensitivity and specificity compared to SRS and conventional imaging modalities [12–14]. In addition, SST analogs labeled with therapeutic radionuclides, such as 111In, 90Y, 177Lu, and 213Bi, have been applied in peptide receptor radionuclide therapy (PRRT) for patients with inoperable and/or metastatic NETs [15]. The results that were obtained with [90Y-DOTA0-Tyr3]octreotide (90Y-DOTATOC) and [177Lu-DOTA0-Tyr3]octreotate (177Lu-DOTATATE) are particularly promising in terms of tumor regression, overall survival, and quality of life, if adequate renal protection is used [16, 17].
However, SSTR based imaging and therapy are only available in SSTR positive tumors. Many malignant human cancers were poorly or not detected to express SSTR subtypes [18, 19]. Surgery, chemotherapy, and radiotherapy have limited effects on improving survival for patients diagnosed with these cancers [20]. Therefore, some studies [21, 22] have tried to explore the applications of hSSTr2 reporter gene based imaging and therapy in SSTR negative or weakly positive tumors to provide a new strategy for the management of these tumors. To this end, the target gene hSSTr2 should be inserted into gene transfer vectors to induce transfected tumors to express SSTR2 [23–25] and assure that hSSTr2 expression could occur on tumor cell membranes. Optical imaging and biopsy have been taken to identify whether gene transfer succeeds or not. However, poor tissue penetration of light-based reporter systems, such as green fluorescent protein [23, 26] and luciferase [27], hampers a comprehensive assessment of whole organism or targeted tumors [20]. On the other hand, biopsy is an invasive technique and can only evaluate the outcome of gene expression [28]. Nuclear imaging can avoid the unclear images in deep tissues and the need of tissue sampling for histological analysis of gene expression. Tumors transfected with hSSTr2 gene can be monitored by external gamma camera, single photon computed emission tomography (SPECT), or PET imaging techniques with radiolabeled SST analogs [29]. These in vivo hSSTr2 based imaging methods have several advantages: repetitively observing the expression levels of hSSTr2 or other genes within transfected tumors [30], studying the biodistribution of gene transfer vectors [25], predicting the effects of PRRT, and monitoring the time course of tumor growth and the efficacy of antitumor gene therapy [21]. The hSSTr2 gene transfer not only allows for some SSTR negative tumors to be imaged in vivo, but also can be useful for antitumor radionuclide therapy. SST analogs labeled with therapeutic radionuclides can be delivered to the cell receptor targeting site and are able to induce the internalization of ligand-receptor complexes [31–33]. The trapped radiopeptides in transfected tumor cells have been considered to be necessary for internal local irradiation, which offers an alternative approach to conventional therapeutics for SSTR negative tumors [22]. Furthermore, by the simultaneous inclusion of a second therapeutic gene like thymidine kinase (TK) or cytosine deaminase (CD), it is possible to obtain a dual gene vector that includes hSSTr2 working as a reporter gene for in vivo imaging as well as a therapeutic gene for radionuclide therapy. Preliminary studies suggested that a synergistic therapeutic effect could be achieved following dual gene transfer with one vector encoding both hSSTr2 reporter gene and a second therapeutic gene [21, 34].
In this review, we summarize the performances of SSTR based imaging and radionuclide therapy in NETs and introduce the applications of hSSTr2 reporter gene based imaging and therapy with radiolabeled SST analogs in SSTR negative or weakly positive tumors.
2. Somatostatin Receptor Based Imaging
Computed tomography (CT) and magnetic resonance imaging (MRI) are commonly used to detect NETs and have sensitivity between 50 and 80% based on anatomic characteristics [37]. In comparison, functional imaging modalities, that is, PET, SPECT, or scintigraphy, have shown higher sensitivity and specificity in visualizing primary tumors and their metastases. During the past two decades, SRS has been widely used for the diagnosis and staging of NETs. [123I, Tyr3]octreotide was the first radiolabeled SST analog utilized for in vivo imaging [38]. Unfortunately, high nonspecific accumulation was observed in the liver and intestine, which has limited its ability to locate early primary tumors [39]. Soon a new radiotracer consisting of octreotide, the chelator DTPA, and the radionuclide 111In was developed as [111In-DTPA0]octreotide (OctreoScan). It has been approved by the Food and Drug Administration and was commercially available as 111In-pentetreotide [40]. An early study [41] tried to evaluate the potential of [111In-DTPA0]octreotide in the visualization of NETs. Patients (n = 6) with proven tumors (three carcinoids, three insulinomas) were scanned using both [111In-DTPA0]octreotide and [123I, Tyr3]octreotide, obtaining the same results in 4 patients. Nevertheless, [111In-DTPA0]octreotide images showed higher resolution at 21 hours after injection with a more satisfactory tumor-background ratio. Several papers [42–44] reported high sensitivity, varying between 67 and 100%, in NET imaging with [111In-DTPA0]octreotide. In the management of patients with NETs, [111In-DTPA0]octreotide scintigraphy can be used not only to detect primary NETs and their metastases, but also to follow up patients with known tumors, monitor tumor response to therapy, and predict the efficacy of PRRT for patients with inoperable and/or metastatic NETs [41, 45, 46]. These good qualities lay the foundation for [111In-DTPA0]octreotide becoming the gold standard for NET imaging [40]. From 2012, SPECT/CT scanning using [111In-DTPA0]octreotide is an important part of the diagnostic work-up of patients with NETs in the consensus guidelines of European Neuroendocrine Tumor Society [47, 48]. However, some NETs, like primary sympathetic paragangliomas, show low uptake of [111In-DTPA0]octreotide in tumor regions [49] while other NETs may become OctreoScan negative with time due to tumor dedifferentiation [10]. Efforts are therefore spent on developing radiolabeled SST analogs to be capable of imaging SSTR positive tumors with higher sensitivity, specificity, and accuracy. The 99mTc-labeled agent, 99mTc-Depreotide, has received regulatory approval in the United States and Europe for use in the detection of lung cancer [50]. It binds to a wide range of SSTR subtypes (SSTR2, SSTR3, and SSTR5) and has shown promise in diagnosing a variety of tumor types [51–53], including some OctreoScan negative NETs [10]. 111In-DOTA-lanreotide is another γ-emitting tracer with different affinity for SSTR subtypes compared to [111In-DTPA0]octreotide. Tumors expressing mainly SSTR3 and/or SSTR4, for example, intestinal adenocarcinomas, may be well visualized by 111In-DOTA-lanreotide [11, 54].
With the emerging of PET scanning, a variety of positron-emitting tracers have been produced. [18F]fluorodeoxyglucose (18F-FDG) is the most widely used radiotracer for tumor staging and treatment response surveillance in a number of tumor types. The trapped 18F-FDG in cells can reflect glucose metabolism profile of normal tissues and lesions [40]. In general, malignant tumors demonstrate increased uptake of 18F-FDG and can be distinguished from normal tissues. It has been demonstrated in patients affected by NET that 18F-FDG PET has a high accuracy for poorly differentiated tumors [55, 56]. However, 18F-FDG is not indicated primarily for NET imaging since most NETs present low proliferative activity and well differentiation. We attempted to use 18F-FDG imaging to monitor everolimus effect on tumor growth in Bon-1 pancreatic NETs. The results showed that in vivo tumor volumes measured relative to baseline were significantly lower in the everolimus group compared to the control group, whereas the uptake of 18F-FDG was quite low in tumor regions and showed no significant difference between the two groups at any time point after everolimus treatment (Figure 1).
Figure 1.
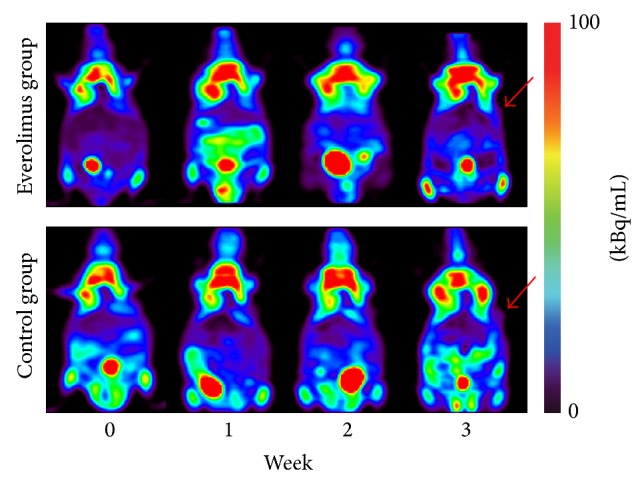
Serial PET images demonstrating glucose metabolism changes before (week 0) and after everolimus treatment (week 1, week 2, and week 3) in nude mice bearing Bon-1 pancreatic tumor xenografts (red arrows). The two groups are presented as the everolimus treatment group and the control group. Images are shown in axial view. No significant difference of the tumor uptake was found between the two groups at each time point after everolimus treatment.
Positron-emitter 68Ga can be produced just depending on 68Ge-68Ga generator, so it is available in departments without a cyclotron. 68Ga-labeled SST analogs with a quite short half-life (68 min) have exhibited great potential for PET imaging of NETs and their metastases [12, 42, 57]. Some [38, 58] predicted that 68Ga-labeled peptides are the most likely candidates for such a universal tracer applied in the diagnosis, staging, and restaging of patients with NETs instead of 111In-DTPA-octreotide. [68Ga-DOTA0-Tyr3]octreotide (68Ga-DOTATOC), [68Ga-DOTA0,1NaI3]octreotide (68Ga-DOTANOC), and [68Ga-DOTA0-Tyr3]octreotate (68Ga-DOTATATE) are three main 68Ga-labeled SST analogs widely utilized to NET imaging and patient selection for PRRT [59]. They demonstrate slightly different affinities for the five SSTR subtypes. 68Ga-DOTATATE is SSTR2 selective, presenting 10-fold higher affinity for SSTR2 in vitro than that of 68Ga-DOTATOC [60], which has high affinity for SSTR2 and SSTR5. In comparison, 68Ga-DOTANOC has a wider receptor binding profile, able to specifically bind to SSTR2, SSTR3, and SSTR5 [61]. These differences may affect their efficiency in the detection of NET lesions. A study [60] explored 40 patients with metastatic NETs, who underwent both 68Ga-DOTATOC and 68Ga-DOTATATE PET/CT. The diagnostic accuracy was almost the same between the two 68Ga-DOTA-conjugated peptides. However, tumor uptake varied considerably both within and between patients. Eighteen patients displayed only lesions with higher uptake of 68Ga-DOTATOC than 68Ga-DOTATATE and the reverse situation was found in 4 patients. The other 18 patients displayed a mixture of lesions with higher uptake of either 68Ga-DOTATATE or 68Ga-DOTATOC. These differences in tumor uptake of the two radiopeptides were also reported by a latest study [35] (Figure 2). The possible reasons for such a variation could be the extensive difference in the SSTR subtype profile and the nonstandardized examination conditions. For tumors expressing broader SSTR subtypes, 68Ga-DOTANOC may be more efficient to detect NET lesions; Wild et al. conducted a study [61] in which 18 patients with clearly diagnostic GEP-NETs were imaged with 68Ga-DOTANOC and 68Ga-DOTATATE. Consequently, the SSTR2, 3, 5 specific radiotracer 68Ga-DOTANOC detected significantly more lesions than the SSTR2 selective radiotracer 68Ga-DOTATATE. Although the diagnostic efficacy varies among the three radiopeptides, PET imaging with 68Ga-DOTA-conjugated peptides offers higher sensitivity and specificity compared with SRS and conventional imaging modalities. In an early study [12], 68Ga-DOTATOC PET was compared with SRS and CT in the visualization of known or suspected NETs (n = 84 patients). As a consequence, 68Ga-DOTATOC PET had a significantly higher diagnostic efficacy than SRS and CT in various clinical situations (initial diagnosis, staging, and follow-up), which have affected clinical management in a considerable number of patients, especially when compared with CT. A latest study [13] aimed to compare NET lesion detectability among SPECT/CT, 68Ga-DOTATATE PET/CT, and whole-body diffusion-weighted MR imaging (WB DWI). The results showed that 68Ga-DOTATATE PET/CT seemed to be more sensitive for detection of NET lesions, especially for bone and unknown primary lesions (Figure 3). Comparison of 68Ga-DOTANOC PET/CT and conventional imaging (mainly CT and MRI) was undertaken in a clinical study [14]. Conventional imaging was available in included patients (n = 111) with 93 patients suspected of NETs; 68Ga-DOTANOC PET/CT was superior for detection of NETs with high sensitivity, specificity, positive predictive value, negative predictive value, and accuracy.
Figure 2.
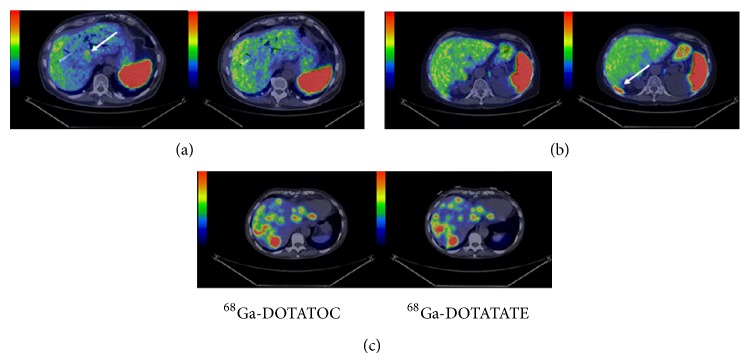
Transaxial images of liver metastases demonstrating cases of higher detection rate for 68Ga-DOTATOC ((a): patient 6, PET/CT fusion); higher detection rate for 68Ga-DOTATATE ((b): patient 8, PET/CT fusion); and equal detection rate ((c): patient 1, PET/CT fusion). Whole-body scans were conducted at 1 hour after injection. Arrows point toward hepatic metastases [35].
Figure 3.
A 49-year-old man with NET of unknown origin for over 4 years. 68Ga-DOTATATE PET/CT (a) identified primary pancreatic lesion (arrow), whereas SPECT/CT (b) and WB DWI (c) did not. This lesion was noted only retrospectively (arrow) on dedicated abdominal CT (d) performed 4 years previously [13].
NETs were formerly described as APUDomas (amine precursor uptake and decarboxylation). Amine precursor such as 5-hydroxy-L-tryptophan (5-HTP) and L-dihydroxyphenylalanine (L-DOPA) may be absorbed into tumor cells and turned into their corresponding amines, dopamine and serotonin. Based on these characteristics of APUD system, 11C-labelled and 18F-labelled L-DOPA (11C-L-DOPA, 18F-L-DOPA) as well as 5-HTP (11C-5-HTP, 18F-5-HTP) have been developed to visualize NETs [62–64]. Their imaging performances are quite good and they can provide additional information for the diagnosis, staging, and management of NETs. One shortage is that nonfunctioning NETs cannot be detected using these tracers. Now they are employed as problem solving tools when other imaging technique results are negative or contradictory [29].
3. Somatostatin Receptor Based Therapy
Surgical treatment suffices for the majority of NETs, but malignant, recurrent, and metastatic tumors need further treatment in order to gain a lengthening of time to progression [65]. Systemic chemotherapy is currently used for patients with poorly differentiated NETs, whereas tumor response is difficult to be assessed as these tumors are not highly chemosensitive and spontaneous standstill or regression is noticed in the time course of tumor growth [66]. A limited number of studies have explored the role for the therapeutic use of external beam radiation therapy in malignant NETs [67]. SST analogs, predominantly octreotide and octreotate, suppressing hormone production, have improved symptoms as well as prognosis in tumors. But the employment of SST analogs must be weighed against the tachyphylaxis and the limited antitumor effects [68]. PRRT using radiolabeled SST analogs has proven to be an effective therapeutic option for NET patients with inoperable and/or metastasized diseases. SST analogs labeled with therapeutic radionuclides, such as 111In, 90Y, 177Lu, and 213Bi, are able to specifically bind to SSTRs on tumor cells and deliver an effective radiation dose to tumors with minimal damage to normal tissues [69].
3.1. Studies with [111In-DTPA0]octreotide
111In not only emits γ-radiation, which penetrates tissues easily and can be imaged by a γ-scanner, but also emits therapeutic Auger and conversion electrons that play an antiproliferative role in malignant tumors with a short to medium tissue penetration [70]. Initial therapeutic studies [71, 72] performed with high radioactivity doses of [111In-DTPA0]octreotide in patients with metastatic NETs resulted in significant symptom relief but relatively few and short-lived objective tumor responses. These results are not unexpected since [111In-DTPA0]octreotide is not an ideal option for PRRT due to their small particle range of Auger electrons [73]. It has been recommended that SST analogs labeled with higher energy β-emitters, which, in reality, have obtained better response rates in various studies [74, 75], should be employed to treat SSTR positive tumors.
3.2. Studies with [90Y-DOTA0, Tyr3]octreotide
90Yttrium (90Y) is a β-particle emitter with a maximum energy of 2.3 MeV and a maximum range of 12 mm in tissue [76]. It is combined with a more stable chelator DOTA instead of DTPA and a modified SST analog octreotide to get a conjunction 90Y-DOTATOC. This tracer has superior therapeutic efficacy since adequate dose of radiation can be delivered to tumors, especially larger tumor masses, to cause cell damage [77]. After 15 years of experience, PRRT with 90Y-DOTATOC is generally well tolerated [78].
Forrer et al. selected 116 patients with metastatic NETs, who underwent PRRT with 90Y-DOTATOC (5994–7400 MBq/m2 body surface). All cases were positive in the scintigraphy. After the last administration, each patient was evaluated with respect to the therapeutic effects on tumor size. The objective response rate was found in 31 patients (26%), including 4% complete remission (CR) and 22% partial remission (PR). 72 patients (62%) showed stabilization of their diseases and the remaining patients (11%) were still progressive (Table 1). No serious side effects occurred and the toxicity was well tolerated [79]. A similar tumor response rate (24%, 2% of which were CR and 22% were PR) was found in a phase II study of 41 patients with GEP-NETs and bronchial tumors who were given intravenously four injections of a total of 6000 MBq 90Y-DOTATOC (Table 1). Grade III pancytopenia was the most severe adverse event occurring in 5% patients [80]. It is not possible to state that 90Y-DOTATOC is of great use for the management of inoperable and/or metastatic NETs when drawing conclusion from a relatively small sample. A study [84] conducted in a larger group of patients with a wide spectrum of NETs supplied more meaningful results. 1109 patients from 29 countries were treated with repeated cycles of 90Y-DOTATOC. Morphologic response was found in 378 patients (34.1%) and stable disease (SD) in 58 patients (5.2%). The median survival from diagnosis was 94.6 months, which was longer than the expected 33-month survival. Longer survival was associated with morphologic, biochemical, and clinical response as well as high tumor uptake in pretherapeutic SRS. Among all the patients, 143 were subjected to severe hematologic toxicities and 102 to permanent renal toxicity.
Table 1.
Tumor responses in patients with various NETs, treated with different radiolabeled SST analogs.
| Ligand | Patient number | Tumor response | References | |||
|---|---|---|---|---|---|---|
| CR | PR | SD | PD | |||
| [111In-DTPA0]octreotide | 26 | 0 | 2 (8%) | 21 (81%) | 3 (11%) | [71] |
| [111In-DTPA0]octreotide | 18 | 0 | 2 (11%) | 16 (89%) | 0 | [72] |
| 90Y-DOTATOC | 116 | 5 (4%) | 26 (22%) | 72 (62%) | 13 (11%) | [79] |
| 90Y-DOTATOC | 41 | 1 (2%) | 9 (22%) | 25 (61%) | 6 (15%) | [80] |
| 177Lu-DOTATATE | 310 | 5 (2%) | 86 (28%) | 158 (51%) | 61 (20%) | [81] |
| 177Lu-DOTATATE | 26 | 3 (12%) | 7 (27%) | 12 (46%) | 4 (15%) | [82] |
| 90Y-DOTATATE and 177Lu-DOTATATE | 26 | 2 (7.7%) | 9 (34.6%) | 11 (42.3%) | 4 (15.4%) | [83] |
| 213Bi-DOTATOC | 7 | 1 (14%) | 2 (28%) | 3 (44%) | n.a. | [36] |
CR: complete remission; PR: partial remission; SD: stable disease; PD: progressive disease; n.a. not available.
Except mentioned studies, there are a large number of reported articles assessing the therapeutic effects of 90Y-DOTATOC. Despite differences in protocols, the objective tumor responses in most of the studies with 90Y-DOTATOC are in the same range, approximately 20–28% in patients with NETs and for patients with GEP-NETs in the range of 28–38% [85].
3.3. Studies with [177Lu-DOTA0-Tyr3]octreotate
177Lutetium (177Lu) is a median energy β-emitter (0.5 MeV) with small particle range [86]. This allows for higher radiation dose delivered to smaller tumors and less damage to surrounding tissues than the radionuclide 90Y [87]. 177Lu also emits γ rays; thus 177Lu-labeled peptides can be used for treatment as well as for dosimetry and monitoring of tumor response. [DOTA0, Tyr3]octreotate (DOTATATE), which presents a ninefold increase in the affinity for SSTR2 compared with [DOTA0, Tyr3]octreotide [88], usually labeled with the radionuclide 177Lu, has been widely used in PRRT. The results that were obtained with 177Lu-DOTATATE are impressive in terms of tumor suppression and patient survival [17, 89].
An early clinical study [75] compared the therapeutic effects of 177Lu-DOTATATE with [111In-DTPA0]octreotide in 6 patients with SSTR positive tumors. After 24 hours, the uptake of 177Lu-DOTATATE was almost equal to that of [111In-DTPA0]octreotide for kidneys but was three- to fourfold higher for 4 of the analyzed tumors. Thus, 177Lu-DOTATATE potentially represents an important improvement since the higher radiation doses can be delivered to tumors with about equal doses to dose-limiting organs, especially kidneys. Latest data illustrated that, even with low radiation doses, 177Lu-DOTATATE could have antitumor effects in advanced pancreatic NETs [82]. Fifty-two patients were assigned to the following two groups: full dosage (FD) group (25.5 GBq, n = 26) and reduced dosage (RD) group (17.8 GBq, n = 26). Both groups showed antitumor activity, with 12% CR, 27% PR, and 46% SD in the FD group (Table 1), while 4% CR, 15% PR, and 58% SD in the RD group. Although response rate was higher in FD, no significant difference was found. However, progression-free survival was significantly longer after injection of a total dose of 25.5 GBq, which is the preferential dosage in tolerated patients.
Since the physical properties of 90Y suggest that this radionuclide will be more effective in larger tumor masses and 177Lu in smaller tumor masses and metastases, the combination treatment of 90Y- and 177Lu-labeled SST analogs seems a reasonable option for managing tumors of varying sizes and SSTR subtypes. As expected, both preclinical and clinical researches have found higher tumor response rate through the combined therapy [83, 86]. Nevertheless, the optimal combination of two radiopharmaceuticals should be determined on a patient-specific basis. As discussed by a recent article [90], the absorbed dose to tumors shows huge interpatient variance, and renal toxicity should be particularly considered since the biologically effective dose to the kidneys of 177Lu was lower compared with 90Y.
3.4. Studies with α-Emitters
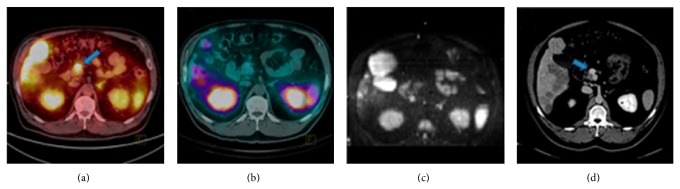
The application of α-emitters such as 213Bi or its mother radionuclide 225Ac is arousing immense interest in PRRT. These radionuclides emit higher energy (8.32 MeV for 213Bi and 27.5 MeV for 225Ac) compared with β-emitters and had a short path-length of only 40–50 μm, which increases the local antitumor effect without affecting untargeted tissues [90]. Alpha radiation can cause double-strand DNA breaks, independent of the cell cycle phase and oxygen concentration [91, 92]. Although PRRT with 90Y- and 177Lu-labeled SST analogs has been promising for NET therapy, some tumors are not radiosensitive to this treatment. SST analogs labeled with α-emitting isotopes may provide an alternative therapy for metastatic, chemoresistant, and hypoxic NETs, which are known to be resistant to PRRT with β-emitting radionuclides. A number of preclinical studies [93–95] have shown the potency and limited toxicity of targeted α therapy in NETs, while clinical trials were seldom studied. Recently, for the first time 213Bi-DOTATOC was used to treat patients with metastatic NETs refractory to therapy with 90Y/177Lu-DOTATOC [36]. Enduring responses were observed in all treated patients during follow-up for more than 2 years (Figure 4; Table 1). The side effects only include moderate chronic kidneys toxicity and favorable acute haematotoxicity. Nevertheless, α radiation with high linear energy transfer may lead to various and less repairable clustered damage, which may further induce secondary neoplasm formation [96]. Also it is unclear whether α-emitting radionuclides are superior to β-emitting radionuclides. Therefore, the therapeutic effects and safety should be further confirmed before α therapy can be well translated to clinical application.
Figure 4.

Patient 5 before therapy ((a)–(c)) and after three cycles of 213Bi-DOTATOC ((d)–(f)) to a dose of 4 GBq. (a) Beta-resistant residuals in the liver (long arrows) and primary tumor (short arrow) are present in the 68Ga-DOTATOC PET maximum intensity projection image. (b) Contrast enhanced CT image with the primary tumor outlined in red. (c) In the MR image with hepatocyte-specific contrast medium, the liver metastases appear as black cavities against the enhancing normal liver parenchyma. ((d)–(f)) After three cycles of 213Bi-DOTATOC to a dose of 4 GBq, the lesions have diminished on the PET image (d) and CT image (e). Also on the MR image (f), the residual lesion has almost disappeared as shown by the growth of normal hepatocytes demonstrated by the uptake of the hepatocyte-specific contrast medium [36].
4. Gene Transfection with hSSTr2
As previously presented, SSTR based imaging and therapy have made a great contribution to the diagnosis and treatment of NETs. However, many SSTR negative or weakly positive tumors, like non-small-cell lung cancer (NSCLC) [20], ovarian cancer [97], malignant glioma [98], and pancreatic cancer [18], are facing a big challenge in therapy. Surgery, chemotherapy, radiotherapy, or the combined therapy modalities have limited effects on improving overall survival. Most patients diagnosed with these tumors will ultimately suffer from recurrent diseases, resist further treatment, and eventually die of their diseases [99].
Over the past two decades, gene therapy has been applied in a number of malignant tumors and appears to be a safe and effective method for treatment. The TK gene, which is a suicide gene from herpes simplex virus (HSV), was widely studied. When HSV-TK is transfected into tumor cells in combination with intravenous ganciclovir, the antitumor efficacy is achieved through converting ganciclovir into a triphosphate configuration, which inhibits DNA synthesis and induces cell apoptosis [100]. Although noninvasive imaging of transferred gene expression has proven available following vector-mediated transfer of the HSV-TK using radiolabeled tracers, some studies [98, 101] found that hSSTr2 reporter based imaging was more sensitive and the uptake of radiolabeled SST analogs well correlated with recombinant vector dose. Moreover, SST analogs labeled with therapeutic radionuclides can be specifically delivered to transfected tumors, which provides an alternative approach to conventional therapeutics for SSTR negative or weakly positive tumors [102]. Since SSTR2 has been known to be most commonly expressed in various NETs and possesses the highest affinity for natural SST and synthetic SST analogs, most experiments utilize hSSTr2 reporter gene to transfect targeted tumor cells alone or together with other therapeutic genes.
In order to improve hSSTr2 gene transfer efficiency, it is critical to choose a vector with powerful infectivity. So far, different vector systems, mainly including adenovirus (Ad), retrovirus, adenoassociated virus, and vaccinia virus, have been employed in various tumor models [98, 109]. Ad remains the most frequently used and most promising virus for gene delivery because it has many advantageous features such as keeping itself stability, acquiring high titers, infecting a wide range of dividing cells as well as nondividing cells, permitting the high level expression of transferred gene, and maintaining a clear separation between viral genome and host chromosomes [103, 111]. Yet, a shortage that Ad depends on the coxsackie Ad receptor (CAR) to enter cells dramatically affects the transfection efficiency because many primary tumors do not express CAR [112]. Various approaches like genetic, chemical, and nonchemical modifications have been taken to retarget Ad vectors to other receptors [104]. The advantages and disadvantages of other main viral vectors used to transfer hSSTr2 are presented in Table 2.
Table 2.
The advantages and disadvantages of main viral vectors used to transfer hSSTr2.
| Vectors | Advantages | Disadvantages | References |
|---|---|---|---|
| Adenovirus | (1) Stability (2) High titers (3) Infecting dividing and nondividing cells (4) High level expression of transgene (5) Not integrating into host chromosome |
(1) Strong immune response (2) Potential replication competence (3) Short-term expression (4) Demanding packaging cell line (5) Small insert size (6) No targeting |
[103–105] |
|
| |||
| Adenoassociated virus | (1) No associated disease (2) Long-term gene expression (3) Integrating into human chromosome 19 |
(1) Extensive antiviral immunity (2) Helper-dependent replication (3) Poor host tropism (4) Small insert size: about 5 kb |
[106] |
|
| |||
| Retrovirus | (1) Integrating into host cell genome (2) Reverse transcription of the RNA genome (3) Infecting dividing cells (4) Long-term expression (5) Fairly high titers |
(1) Immune-related toxicity (2) Infecting dividing cells (3) Potential replication competence (4) Insertion mutation (5) No targeting |
[107, 108] |
|
| |||
| Vaccinia virus | (1) Cytolytic viral vector (2) Preferentially infecting rapid dividing cells (3) Difficult to leak from normal vasculature (4) The vector itself serving as a therapeutic method (5) Large insert size: ≥25 kb DNA |
(1) Live infectious lytic virus (2) Replication competence (3) Short-term gene expression (4) Postvaccinal encephalitis and progressive complications (5) No targeting |
[109, 110] |
5. Somatostatin Receptor Based Reporter Gene Imaging
Although gene therapy in various animal models has acquired encouraging results, many obstacles should be overcome before gene therapy can be well translated to clinical trials [113]. One obstacle is how to make sure that gene transfer occurs in targeted tissues. Some studies have tried to use optical imaging and biopsy to detect the expression levels of transferred genes. However, poor tissue penetration of light-based reporter systems [20] and invasive damage of biopsies [28] hamper a comprehensive assessment of the magnitude and time course of gene expression. Nuclear imaging based on hSSTr2 reporter gene transfer can get rid of these limitations. The hSSTr2 based reporter system has been utilized in a variety of tumor studies both in vitro and in vivo to estimate its ability to image gene transfer. A study [20] hoped to assess whether hSSTr2 is competent to act as a reporter of gene transfer. It used Ad encoding hemagglutinin A and SSTR2 (Ad-CMV-HA-hSSTr2) or control virus to transfect NSCLC cell lines and tumors bearing nude mice. As a result, the radiopeptide [111In-DTPA0]octreotide could specifically bind to tumor cells after Ad-CMV-HA-hSSTr2 transfection and the uptake of tracers in Ad-CMV-HA-hSSTr2 transfected tumors was higher than that of control groups. Similar results were reported by an article [19] which observed the expression of hSSTr2 originating from Ad5-mediated gene transfer to non-small-cell lung tumors with 99mTc- or 88Re-labeled peptides (Figure 5). The article even calculated the approximate number of SSTR2 expressed per Ad5-transfected cell through the uptake of radiolabeled peptides, which provided more accurate information of gene expression. Except NSCLC, hSSTr2 reporter system was adopted to monitor the duration and time course of gene expression in other transfected tumors, including ovarian cancer [24], malignant glioma [98], and fibroblastoma [114], as well as normal tissues like muscle and liver [30]. All these laboratory results were so encouraging that hSSTr2 reporter gene system was applied to clinical trials. Kim et al. conducted a phase I clinical trial of Ad5.SSTR/TK.RGD in patients with recurrent gynecologic cancer [99]. The Ad vector not only contains the therapeutic gene TK but also contains the hSSTr2 reporter gene which allows for noninvasive and repetitive gene transfer imaging with [111In-DTPA0]octreotide. Compared to imaging before Ad-mediated gene therapy, significantly increased uptake of [111In-DTPA0]octreotide was found in patients after the last administration in the highest Ad dose group. All these studies indicate that the hSSTr2 reporter based imaging is a promising method to track gene delivery and expression. The detailed functions of hSSTr2 reporter gene based imaging are demonstrated below: repetitively observing the magnitude, duration, and time variation of gene expression both in vitro and in vivo [30], studying the biodistribution of gene transfer vector in mice or patients [25], optimizing the administration dose of vector encoding hSSTr2 reporter gene and/or other therapeutic genes [24], predicting treatment response of transfected tumor to PRRT [21], and monitoring antitumor effects of various treatments including hSSTr2 gene or another therapeutic gene based therapy [21, 99].
Figure 5.

γ camera imaging of mice injected with 99mTc-labeled SST analogs. Imaging position is shown in (a), with 3 representative images of mice at 3 minutes (b) and 3 hours (c) after intravenous injection. Circles in (c) indicate location of human A427 tumors injected 48 h earlier with Ad5-CMV-hSSTr2, and squares indicate human A427 tumors injected 48 h earlier with Ad5-CMV-LacZ. (d) Results of region of interest analyses [19]. A427 tumors: human non-small-cell lung cancer, hSSTr2 negative Ad5-CMV-LacZ: Ad encoding Escherichia coli β-galactosidase under control of the CMV promoter element.
6. Somatostatin Receptor Based Reporter Gene Therapy
In addition to reporter based imaging, the hSSTr2 can serve as a therapeutic gene to cause tumor regression alone or together with other treatments [115]. As mentioned above, the prognosis of many malignant tumors is poor no matter what therapeutic methods are given. It is badly in need of new therapeutic approaches to treating these tumors. Impressive response of NET leading to improved survival has been observed with PRRT [116], which, however, is only suitable for tumors showing SSTR expression, but not for SSTR negative tumors. Fortunately, it is feasible to induce SSTR negative tumors to express SSTRs by means of gene transfer technology, which provides a novel therapy for some malignant tumors [22, 98, 117].
6.1. Therapy Studies with the Vector Encoding the Single hSSTr2 Gene
In a therapeutic study [22], Zhao et al. evaluated the antitumor effects of 188Re-RC-160 (188Re-labeled SST analog) on A549 tumor, which is one kind of lung adenocarcinomas, transfected with plasmid pcDNA3 encoding hSSTr2 reporter gene. Nude mice bearing pcDNA3-hSSTr2 transfected tumors were divided into five groups according to different therapeutic protocols. Finally, the tumor growth inhibition in the single dose treatment group (7.4 MBq, 188Re-RC-160) was significantly higher than that in 188Re group (2 × 7.4 MBq), RC-160 group, and saline control group. Moreover, two-injection group (2 × 7.4 MBq, 188Re-RC-160) led to significantly increased tumor growth inhibition compared with the single dose treatment group. These results provided a preliminary proof that SSTR negative tumor could be transfected with hSSTr2 reporter gene for radionuclide therapy. One problem observed in the present study was the low transfection efficiency. In fact, viral vectors have become the major vehicle to deliver hSSTr2 reporter gene. Although the drawbacks of viral vectors, especially immune response, are inevitable, transfection rate is fairly higher than that of nonviral vehicles and gene expression within tumors is relatively stable [118].
Reconstructed Ad encoding hSSTr2 gene (Ad-hSSTr2) was utilized in a study [119] to explore the therapeutic effects of [90Y]-SMT 487 ([90Y]-DOTA-D-Phe1-Tyr3-octreotide) on transfected tumors. Mice bearing non-small-cell lung tumors were intratumorally injected two doses of Ad-hSSTr2 (1 week apart) and intravenously administrated four doses of 14.8 MBq [90Y]-SMT 487 or four doses of 18.5 MBq [90Y]-SMT 487 with median tumor quadrupling times of respective 40 and 44 days, while in untreated group and the group that received only four doses of 18.5 MBq [90Y]-SMT 487 without virus, the median tumor quadrupling times were 16 and 25 days, respectively. Significant difference in time to tumor quadrupling between the groups that received Ad-CMV-hSSTr2 plus [90Y]-SMT 487 and the control groups was revealed by the log-rank test. The hSSTr2/[90Y]-SMT 487 system is a potential approach for clinical application, since both Ad vector encoding hSSTr2 gene and [90Y]-SMT 487 have been used for cancer therapy in clinical trials.
6.2. Therapy Studies with the Bicistronic Vector Encoding Both hSSTr2 and CD Genes
Gene therapy vectors containing both hSSTr2 reporter gene and a second therapeutic gene encoding TK or CD have been investigated [21, 99]. The hSSTr2 is available not only for noninvasive imaging of the expression of transferred gene, but also for radionuclide therapy [21]. A synergistic therapeutic effect may be achieved through the combined gene therapy. In view of the toxicity that resulted from the combination treatment of radiolabeled peptide and TK gene [34], the hSSTr2/CD system received considerable attention. Mechanisms of CD gene based therapy are that CD specifically converts the prodrug 5-FC to the highly toxic 5-FU, which disturbs DNA synthesis and induces cell death [120].
NSCLC A549 cells transfected by the bicistronic plasmid pCD-IRES-hSSTR2 (pCIS) were induced to express both SSTR2 and CD. Then 3 × 106 pCIS-A549 cells were injected subcutaneously into each nude mouse on the right axilla and the same number of control A549 cells on the contralateral axillary regions of the same mouse to establish a xenograft tumor model. When tumors grew to an average diameter of 1cm, mice (n = 6) were intravenously injected with 99mTc-RC-160, which specifically bound to pCIS-A549 cell-derived tumors. To study a synergistic inhibitory effect on tumor growth, 131I-RC-160 and 5-FC were injected alone or together into mice bearing tumors via their tail veins. The results showed that the combination treatment of those two agents inhibited pCIS-A549 cell-derived tumor growth significantly more than 131I-RC-160 or 5-FC treatment alone did [21]. These findings suggest that hSSTr2 reporter based therapy can combine with prodrug gene therapy to achieve enhanced antitumor effect and provides a novel treatment for lung cancer.
7. Conclusion
At present there are a number of tracers available for NET imaging. Their uptake is dependent upon different biological mechanisms, predominantly the expressions of SSTRs on tumor cell membranes. SRS with [111In-DTPA0]octreotide has played an important role in the diagnosis and staging of NETs. With the advent of PET technique, positron-emitting tracers were developed and seem to be more encouraging. 68Ga-DOTA-peptides used for PET or PET/CT imaging are hopeful of being routinely utilized to visualize NETs. PRRT is a most promising therapy for patients with inoperable and/or metastasized NETs. Treatment with 90Y-DOTATOC and 177Lu-DOTATATE has been shown to be relatively safe, and most patients had high objective tumor response after the therapy, especially the combined treatment of the two radiopeptides. In addition, hSSTr2 reporter gene based imaging and therapy are feasible in SSTR negative or weakly positive tumors by means of gene transfer technique. Radiolabeled SST analogs can be delivered to transfected tumors, which provides a new specific approach to imaging gene expressions and killing tumor cells. Furthermore, a synergistic therapeutic effect can be achievable by dual gene transfer of hSSTr2 reporter gene and a second therapeutic gene such as TK or CD gene. Though excellent results have been achieved with regard to hSSTr2 reporter gene based imaging and radionuclide therapy in SSTR negative or weakly positive tumors, additional preclinical and especially translational and clinical researches are needed to obtain further proof of value.
Acknowledgments
This work is partly sponsored by National Science Foundation of China (no. 30672396) and Zhejiang Provincial Program for the Cultivation of High-level Innovative Health Talents.
Abbreviations
- SST:
Somatostatin
- SSTR:
Somatostatin receptor
- SSTR2:
Somatostatin receptor subtype 2
- NETs:
Neuroendocrine tumors
- hSSTr2:
Human somatostatin receptor subtype 2
- GEP-NET:
Gastroenteropancreatic neuroendocrine tumor
- SRS:
Somatostatin receptor scintigraphy
- PET:
Positron emission tomography
- PRRT:
Peptide receptor radionuclide therapy
- SPECT:
Single photon computed emission tomography
- TK:
Thymidine kinase
- CD:
Cytosine deaminase
- CT:
Computed tomography
- MRI:
Magnetic resonance imaging
- WB DWI:
Whole-body diffusion-weighted MR imaging
- APUD:
Amine precursor uptake and decarboxylation
- CR:
Complete remission
- PR:
Partial remission
- SD:
Stable disease
- PD:
Progressive disease
- NSCLC:
Non-small-cell lung cancer
- HSV:
Herpes simplex virus
- Ad:
Adenovirus
- CAR:
Coxsackie adenovirus receptor.
Conflict of Interests
The authors declare that they have no conflict of interests.
References
- 1.Cuevas-Ramos D., Fleseriu M. Somatostatin receptor ligands and resistance to treatment in pituitary adenomas. Journal of Molecular Endocrinology. 2014;52(3):R223–R240. doi: 10.1530/JME-14-0011. [DOI] [PubMed] [Google Scholar]
- 2.Sundin A., Garske U., Örlefors H. Nuclear imaging of neuroendocrine tumours. Best Practice and Research: Clinical Endocrinology & Metabolism. 2007;21(1):69–85. doi: 10.1016/j.beem.2006.12.003. [DOI] [PubMed] [Google Scholar]
- 3.Lamberts S. W. J., Krenning E. P., Reubi J.-C. The role of somatostatin and its analogs in the diagnosis and treatment of tumors. Endocrine Reviews. 1991;12(4):450–482. doi: 10.1210/edrv-12-4-450. [DOI] [PubMed] [Google Scholar]
- 4.Sun L. C., Coy D. H. Somatostatin receptor-targeted anti-cancer therapy. Current Drug Delivery. 2011;8(1):2–10. doi: 10.2174/156720111793663633. [DOI] [PubMed] [Google Scholar]
- 5.Frühwald M. C., O'Dorisio M. S., Pietsch T., Reubi J. C. High expression of somatostatin receptor subtype 2 (sst2) in medulloblastoma: implications for diagnosis and therapy. Pediatric Research. 1999;45(5, part 1):697–708. doi: 10.1203/00006450-199905010-00016. [DOI] [PubMed] [Google Scholar]
- 6.Volante M., Rosas R., Allìa E., et al. Somatostatin, cortistatin and their receptors in tumours. Molecular and Cellular Endocrinology. 2008;286(1-2):219–229. doi: 10.1016/j.mce.2007.12.002. [DOI] [PubMed] [Google Scholar]
- 7.Theodoropoulou M., Stalla G. K. Somatostatin receptors: from signaling to clinical practice. Frontiers in Neuroendocrinology. 2013;34(3):228–252. doi: 10.1016/j.yfrne.2013.07.005. [DOI] [PubMed] [Google Scholar]
- 8.Virgolini I., Traub T., Leimer M., et al. New radiopharmaceuticals for receptor scintigraphy and radionuclide therapy. Quarterly Journal of Nuclear Medicine. 2000;44(1):50–58. [PubMed] [Google Scholar]
- 9.Sorschag M., Malle P., Gallowitsch H.-J. Nuclear medicine in NET. Wiener Medizinische Wochenschrift. 2012;162(19-20):416–422. doi: 10.1007/s10354-012-0130-z. [DOI] [PubMed] [Google Scholar]
- 10.Shah T., Kulakiene I., Quigley A.-M., et al. The role of 99mTc-depreotide in the management of neuroendocrine tumours. Nuclear Medicine Communications. 2008;29(5):436–440. doi: 10.1097/MNM.0b013e3282f50747. [DOI] [PubMed] [Google Scholar]
- 11.Virgolini I., Szilvasi I., Kurtaran A., et al. Indium-111-DOTA-lanreotide: biodistribution, safety and radiation absorbed dose in tumor patients. Journal of Nuclear Medicine. 1998;39(11):1928–1936. [PubMed] [Google Scholar]
- 12.Gabriel M., Decristoforo C., Kendler D., et al. 68Ga-DOTA-Tyr3-octreotide PET in neuroendocrine tumors: comparison with somatostatin receptor scintigraphy and CT. Journal of Nuclear Medicine. 2007;48(4):508–518. doi: 10.2967/jnumed.106.035667. [DOI] [PubMed] [Google Scholar]
- 13.Etchebehere E. C., de Oliveira Santos A., Gumz B., et al. 68Ga-DOTATATE PET/CT, 99mTc-HYNIC-octreotide SPECT/CT, and whole-body MR imaging in detection of neuroendocrine tumors: a prospective trial. Journal of Nuclear Medicine. 2014;55(10):1598–1604. doi: 10.2967/jnumed.114.144543. [DOI] [PubMed] [Google Scholar]
- 14.Sharma P., Arora S., Mukherjee A., et al. Predictive value of 68Ga-DOTANOC PET/CT in patients with suspicion of neuroendocrine tumors: is its routine use justified? Clinical Nuclear Medicine. 2014;39(1):37–43. doi: 10.1097/rlu.0000000000000257. [DOI] [PubMed] [Google Scholar]
- 15.Kwekkeboom D. J., de Herder W. W., van Eijck C. H. J., et al. Peptide receptor radionuclide therapy in patients with gastroenteropancreatic neuroendocrine tumors. Seminars in Nuclear Medicine. 2010;40(2):78–88. doi: 10.1053/j.semnuclmed.2009.10.004. [DOI] [PubMed] [Google Scholar]
- 16.Muros M. A., Varsavsky M., Iglesias Rozas P., et al. Outcome of treating advanced neuroendocrine tumours with radiolabelled somatostatin analogues. Clinical and Translational Oncology. 2009;11(1):48–53. doi: 10.1007/s12094-009-0310-5. [DOI] [PubMed] [Google Scholar]
- 17.Khan S., Krenning E. P., Van Essen M., Kam B. L., Teunissen J. J., Kwekkeboom D. J. Quality of life in 265 patients with gastroenteropancreatic or bronchial neuroendocrine tumors treated with [177Lu-DOTA0,Tyr3]octreotate. Journal of Nuclear Medicine. 2011;52(9):1361–1368. doi: 10.2967/jnumed.111.087932. [DOI] [PubMed] [Google Scholar]
- 18.Buscail L., Saint-Laurent N., Chastre E., et al. Loss of sst2 somatostatin receptor gene expression in human pancreatic and colorectal cancer. Cancer Research. 1996;56(8):1823–1827. [PubMed] [Google Scholar]
- 19.Zinn K. R., Buchsbaum D. J., Chaudhuri T. R., Mountz J. M., Grizzle W. E., Rogers B. E. Noninvasive monitoring of gene transfer using a reporter receptor imaged with a high-affinity peptide radiolabeled with 99mTc or 188Re. Journal of Nuclear Medicine. 2000;41(5):887–895. [PubMed] [Google Scholar]
- 20.Singh S. P., Han L., Murali R., et al. SSTR2-based reporters for assessing gene transfer into non-small cell lung cancer: evaluation using an intrathoracic mouse model. Human Gene Therapy. 2011;22(1):55–64. doi: 10.1089/hum.2010.109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yuan M., Wang J., Deng J., et al. Combination therapy in A549 cells. Nuclear Medicine and Biology. 2010;37(3):317–326. doi: 10.1016/j.nucmedbio.2009.11.009. [DOI] [PubMed] [Google Scholar]
- 22.Zhao R., Yang W., Wang Z., Li G., Qin W., Wang J. Treatment of transplanted tumor of lung adenocarcinoma A549 transfected by human somatostatin receptor subtype 2 (hsstr2) gene with 188Re-RC-160. Nuclear Medicine and Biology. 2010;37(8):977–987. doi: 10.1016/j.nucmedbio.2010.05.007. [DOI] [PubMed] [Google Scholar]
- 23.Zhang H., Moroz M. A., Serganova I., et al. Imaging expression of the human somatostatin receptor subtype-2 reporter gene with 68Ga-DOTATOC. Journal of Nuclear Medicine. 2011;52(1):123–131. doi: 10.2967/jnumed.110.079004. [DOI] [PubMed] [Google Scholar]
- 24.Rogers B. E., McLean S. F., Kirkman R. L., et al. In vivo localization of [111In]-DTPA-D-Phe1-octreotide to human ovarian tumor xenografts induced to express the somatostatin receptor subtype 2 using an adenoviral vector. Clinical Cancer Research. 1999;5(2):383–393. [PubMed] [Google Scholar]
- 25.Rogers B. E., Parry J. J., Andrews R., Cordopatis P., Nock B. A., Maina T. MicroPET imaging of gene transfer with a somatostatin receptor-based reporter gene and 94mTc-demotate 1. Journal of Nuclear Medicine. 2005;46(11):1889–1897. [PubMed] [Google Scholar]
- 26.Meyer K., Irminger J.-C., Moss L. G., et al. Sorting human β-cells consequent to targeted expression of green fluorescent protein. Diabetes. 1998;47(12):1974–1977. doi: 10.2337/diabetes.47.12.1974. [DOI] [PubMed] [Google Scholar]
- 27.Bhaumik S., Lewis X. Z., Gambhir S. S. Optical imaging of Renilla luciferase, synthetic Renilla luciferase, and firefly luciferase reporter gene expression in living mice. Journal of Biomedical Optics. 2004;9(3):578–586. doi: 10.1117/1.1647546. [DOI] [PubMed] [Google Scholar]
- 28.Okuwaki K., Kida M., Mikami T., et al. Clinicopathologic characteristics of pancreatic neuroendocrine tumors and relation of somatostatin receptor type 2A to outcomes. Cancer. 2013;119(23):4094–4102. doi: 10.1002/cncr.28341. [DOI] [PubMed] [Google Scholar]
- 29.Sundin A. Radiological and nuclear medicine imaging of gastroenteropancreatic neuroendocrine tumours. Best Practice and Research: Clinical Gastroenterology. 2012;26(6):803–818. doi: 10.1016/j.bpg.2012.12.004. [DOI] [PubMed] [Google Scholar]
- 30.Cotugno G., Aurilio M., Annunziata P., et al. Noninvasive repetitive imaging of somatostatin receptor 2 gene transfer with positron emission tomography. Human Gene Therapy. 2011;22(2):189–196. doi: 10.1089/hum.2010.098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cescato R., Schulz S., Waser B., et al. Internalization of sst2, sst3, and sst5 receptors: effects of Somatostatin agonists and antagonists. Journal of Nuclear Medicine. 2006;47(3):502–511. [PubMed] [Google Scholar]
- 32.Reubi J. C., Waser B., Cescato R., Gloor B., Stettler C., Christ E. Internalized somatostatin receptor subtype 2 in neuroendocrine tumors of octreotide-treated patients. Journal of Clinical Endocrinology and Metabolism. 2010;95(5):2343–2350. doi: 10.1210/jc.2009-2487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Fottner C., Mettler E., Goetz M., et al. In vivo molecular imaging of somatostatin receptors in pancreatic islet cells and neuroendocrine tumors by miniaturized confocal laser-scanning fluorescence microscopy. Endocrinology. 2010;151(5):2179–2188. doi: 10.1210/en.2009-1313. [DOI] [PubMed] [Google Scholar]
- 34.Buchsbaum D. J., Chaudhuri T. R., Zinn K. R. Radiotargeted gene therapy. Journal of Nuclear Medicine. 2005;46(supplement 1):179s–186s. [PubMed] [Google Scholar]
- 35.Velikyan I., Sundin A., Sörensen J., et al. Quantitative and qualitative intrapatient comparison of 68Ga-DOTATOC and 68Ga-DOTATATE: net uptake rate for accurate quantification. Journal of Nuclear Medicine. 2014;55(2):204–210. doi: 10.2967/jnumed.113.126177. [DOI] [PubMed] [Google Scholar]
- 36.Kratochwil C., Giesel F. L., Bruchertseifer F., et al. 213Bi-DOTATOC receptor-targeted alpha-radionuclide therapy induces remission in neuroendocrine tumours refractory to beta radiation: a first-in-human experience. European Journal of Nuclear Medicine and Molecular Imaging. 2014;41(11):2106–2119. doi: 10.1007/s00259-014-2857-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wong K. K., Waterfield R. T., Marzola M. C., et al. Contemporary nuclear medicine imaging of neuroendocrine tumours. Clinical Radiology. 2012;67(11):1035–1050. doi: 10.1016/j.crad.2012.03.019. [DOI] [PubMed] [Google Scholar]
- 38.Kwekkeboom D. J., Kam B. L., van Essen M., et al. Somatostatin receptor-based imaging and therapy of gastroenteropancreatic neuroendocrine tumors. Endocrine-Related Cancer. 2010;17(1):R53–R73. doi: 10.1677/erc-09-0078. [DOI] [PubMed] [Google Scholar]
- 39.Shan L. Molecular Imaging and Contrast Agent Database (MICAD) Bethesda, Md, USA: National Center for Biotechnology Information; 2004. 18F-Fluoroethyl triazole-βAG-[(d)-Phe1-c(Cys2-Tyr3-(d)-Trp4-Lys5-Thr6-Cys7)Thr8] [PubMed] [Google Scholar]
- 40.Bombardieri E., Maccauro M., De Deckere E., Savelli G., Chiti A. Nuclear medicine imaging of neuroendocrine tumours. Annals of Oncology. 2001;12(supplement 2):S51–S61. doi: 10.1093/annonc/12.suppl_2.s51. [DOI] [PubMed] [Google Scholar]
- 41.Ur E., Bomanji J., Mather S. J., et al. Localization of neuroendocrine tumours and insulinomas using radiolabelled somatostatin analogues, 123I-Tyr3-octreotide and 111In-pentatreotide. Clinical Endocrinology. 1993;38(5):501–506. doi: 10.1111/j.1365-2265.1993.tb00346.x. [DOI] [PubMed] [Google Scholar]
- 42.Srirajaskanthan R., Kayani I., Quigley A. M., Soh J., Caplin M. E., Bomanji J. The role of 68Ga-DOTATATE PET in patients with neuroendocrine tumors and negative or equivocal findings on 111In-DTPA-octreotide scintigraphy. Journal of Nuclear Medicine. 2010;51(6):875–882. doi: 10.2967/jnumed.109.066134. [DOI] [PubMed] [Google Scholar]
- 43.Hildebrandt G., Scheidhauer K., Luyken C., et al. High sensitivity of the in vivo detection of somatostatin receptors by111Indium (DTPA-octreotide)-scintigraphy in meningioma patients. Acta Neurochirurgica. 1994;126(2-4):63–71. doi: 10.1007/BF01476412. [DOI] [PubMed] [Google Scholar]
- 44.Lebtahi R., le Cloirec J., Houzard C., et al. Detection of neuroendocrine tumors: 99mTc-P829 scintigraphy compared with 111In-pentetreotide scintigraphy. Journal of Nuclear Medicine. 2002;43(7):889–895. [PubMed] [Google Scholar]
- 45.Bural G. G., Lieberman F., Mountz J. M. Use of 111in-pentetreotide scan in a subject with treatment refractory atypical meningioma. Clinical Nuclear Medicine. 2014;39(4):342–345. doi: 10.1097/rlu.0000000000000326. [DOI] [PubMed] [Google Scholar]
- 46.Bombardieri E., Ambrosini V., Aktolun C., et al. 111In-pentetreotide scintigraphy: procedure guidelines for tumour imaging. European Journal of Nuclear Medicine and Molecular Imaging. 2010;37(7):1441–1448. doi: 10.1007/s00259-010-1473-6. [DOI] [PubMed] [Google Scholar]
- 47.Pavel M., Baudin E., Couvelard A., et al. ENETS consensus guidelines for the management of patients with liver and other distant metastases from neuroendocrine neoplasms of foregut, midgut, hindgut, and unknown primary. Neuroendocrinology. 2012;95(2):157–176. doi: 10.1159/000335597. [DOI] [PubMed] [Google Scholar]
- 48.Pape U.-F., Perren A., Niederle B., et al. ENETS consensus guidelines for the management of patients with neuroendocrine neoplasms from the jejuno-ileum and the appendix including goblet cell carcinomas. Neuroendocrinology. 2012;95(2):135–156. doi: 10.1159/000335629. [DOI] [PubMed] [Google Scholar]
- 49.Blanchet E. M., Martucci V., Pacak K. Pheochromocytoma and paraganglioma: current functional and future molecular imaging. Frontiers in Oncology. 2012;1, article 58 doi: 10.3389/fonc.2011.00058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Xia W., Zhang X., Yu F., et al. Experimental study of 99mTc-depreotide preparation and its affinity with A549 cell. Frontiers in Bioscience. 2011;16(7):2527–2539. doi: 10.2741/3870. [DOI] [PubMed] [Google Scholar]
- 51.Axelsson R., Herlin G., Bth M., Aspelin P., Kölbeck K. G. Role of scintigraphy with technetium-99m depreotide in the diagnosis and management of patients with suspected lung cancer. Acta Radiologica. 2008;49(3):295–302. doi: 10.1080/02841850701793777. [DOI] [PubMed] [Google Scholar]
- 52.Rodrigues M., Li S., Gabriel M., Heute D., Greifeneder M., Virgolini I. 99mTc-depreotide scintigraphy versus 18F-FDG-PET in the diagnosis of radioiodine-negative thyroid cancer. Journal of Clinical Endocrinology and Metabolism. 2006;91(10):3997–4000. doi: 10.1210/jc.2006-0825. [DOI] [PubMed] [Google Scholar]
- 53.van den Bossche B., van Belle S., de Winter F., Signore A., Van De Wiele C. Early prediction of endocrine therapy effect in advanced breast cancer patients using 99mTc-depreotide scintigraphy. Journal of Nuclear Medicine. 2006;47(1):6–13. [PubMed] [Google Scholar]
- 54.Asnacios A., Courbon F., Rochaix P., et al. Indium-111-pentetreotide scintigraphy and somatostatin receptor subtype 2 expression: new prognostic factors for malignant well-differentiated endocrine tumors. Journal of Clinical Oncology. 2008;26(6):963–970. doi: 10.1200/jco.2007.12.7431. [DOI] [PubMed] [Google Scholar]
- 55.Belhocine T., Foidart J., Rigo P., et al. Fluorodeoxyglucose positron emission tomography and somatostatin receptor scintigraphy for diagnosing and staging carcinoid tumours: correlations with the pathological indexes p53 and Ki-67. Nuclear Medicine Communications. 2002;23(8):727–734. doi: 10.1097/00006231-200208000-00005. [DOI] [PubMed] [Google Scholar]
- 56.Kayani I., Bomanji J. B., Groves A., et al. Functional imaging of neuroendocrine tumors with combined PET/CT using 68Ga-DOTATATE (Dota-DPhe1, Tyr3-octreotate) and 18F-FDG. Cancer. 2008;112(11):2447–2455. doi: 10.1002/cncr.23469. [DOI] [PubMed] [Google Scholar]
- 57.Wild D., Mäcke H. R., Waser B., et al. 68Ga-DOTANOC: a first compound for PET imaging with high affinity for somatostatin receptor subtypes 2 and 5. European Journal of Nuclear Medicine and Molecular Imaging. 2005;32(6):p. 724. doi: 10.1007/s00259-004-1697-4. [DOI] [PubMed] [Google Scholar]
- 58.Sharma P., Arora S., Dhull V. S., et al. Evaluation of (68)Ga-DOTANOC PET/CT imaging in a large exclusive population of pancreatic neuroendocrine tumors. Abdominal Imaging. 2015;40(2):299–309. doi: 10.1007/s00261-014-0219-5. [DOI] [PubMed] [Google Scholar]
- 59.Johnbeck C. B., Knigge U., Kjær A. PET tracers for somatostatin receptor imaging of neuroendocrine tumors: current status and review of the literature. Future Oncology. 2014;10(14):2259–2277. doi: 10.2217/fon.14.139. [DOI] [PubMed] [Google Scholar]
- 60.Poeppel T. D., Binse I., Petersenn S., et al. 68Ga-DOTATOC versus 68Ga-DOTATATE PET/CT in functional imaging of neuroendocrine tumors. The Journal of Nuclear Medicine. 2011;52(12):1864–1870. doi: 10.2967/jnumed.111.091165. [DOI] [PubMed] [Google Scholar]
- 61.Wild D., Bomanji J. B., Benkert P., et al. Comparison of 68Ga-DOTANOC and 68Ga-DOTATATE PET/CT within patients with gastroenteropancreatic neuroendocrine tumors. Journal of Nuclear Medicine. 2013;54(3):364–372. doi: 10.2967/jnumed.112.111724. [DOI] [PubMed] [Google Scholar]
- 62.Bombardieri E., Maccauro M., Castellani M. R., et al. Radioisotopic imaging of neuroendocrine tumours. Which radiopharmaceutical and which diagnostic procedure? Minerva Endocrinologica. 2001;26(4):197–213. [PubMed] [Google Scholar]
- 63.Nikolaou A., Thomas D., Kampanellou C., et al. The value of 11C-5-hydroxy-tryptophan positron emission tomography in neuroendocrine tumor diagnosis and management: experience from one center. Journal of Endocrinological Investigation. 2010;33(11):794–799. doi: 10.3275/6936. [DOI] [PubMed] [Google Scholar]
- 64.Junik R., Drobik P., Małkowski B., Kobus-Błachnio K. The role of positron emission tomography (PET) in diagnostics of gastroenteropancreatic neuroendocrine tumours (GEP NET) Advances in Medical Sciences. 2006;51:66–68. [PubMed] [Google Scholar]
- 65.Kaltsas G. A., Papadogias D., Makras P., Grossman A. B. Treatment of advanced neuroendocrine tumours with radiolabelled somatostatin analogues. Endocrine-Related Cancer. 2005;12(4):683–699. doi: 10.1677/erc.1.01116. [DOI] [PubMed] [Google Scholar]
- 66.Kaltsas G., Mukherjee J. J., Plowman P. N., Grossman A. B. The role of chemotherapy in the nonsurgical management of malignant neuroendocrine tumours. Clinical Endocrinology. 2001;55(5):575–587. doi: 10.1046/j.1365-2265.2001.01396.x. [DOI] [PubMed] [Google Scholar]
- 67.Vogel J., Atanacio A. S., Prodanov T., et al. External beam radiation therapy in treatment of malignant pheochromocytoma and paraganglioma. Frontiers in Oncology. 2014;4, article 166 doi: 10.3389/fonc.2014.00166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Mohamed A., Blanchard M. P., Albertelli M., et al. Pasireotide and octreotide antiproliferative effects and sst2 trafficking in human pancreatic neuroendocrine tumor cultures. Endocrine-Related Cancer. 2014;21(5):691–704. doi: 10.1530/ERC-14-0086. [DOI] [PubMed] [Google Scholar]
- 69.Fani M., Maecke H. R., Okarvi S. M. Radiolabeled peptides: valuable tools for the detection and treatment of cancer. Theranostics. 2012;2(5):481–501. doi: 10.7150/thno.4024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Krenning E. P., de Jong M., Kooij P. P. M., et al. Radiolabelled somatostatin analogue(s) for peptide receptor scintigraphy and radionuclide therapy. Annals of Oncology. 1999;10(supplement 2):S23–S29. doi: 10.1093/annonc/10.suppl_2.s23. [DOI] [PubMed] [Google Scholar]
- 71.Anthony L. B., Woltering E. A., Espenan G. D., Cronin M. D., Maloney T. J., McCarthy K. E. Indium-111-pentetreotide prolongs survival in gastroenteropancreatic malignancies. Seminars in Nuclear Medicine. 2002;32(2):123–132. doi: 10.1053/snuc.2002.31769. [DOI] [PubMed] [Google Scholar]
- 72.Delpassand E. S., Sims-Mourtada J., Saso H., et al. Safety and efficacy of radionuclide therapy with high-activity in-111 pentetreotide in patients with progressive neuroendocrine tumors. Cancer Biotherapy and Radiopharmaceuticals. 2008;23(3):292–300. doi: 10.1089/cbr.2007.0448. [DOI] [PubMed] [Google Scholar]
- 73.Capello A., Krenning E. P., Breeman W. A. P., Bernard B. F., de Jong M. Peptide receptor radionuclide therapy in vitro using [111In-DTPA0]octreotide. Journal of Nuclear Medicine. 2003;44(1):98–104. [PubMed] [Google Scholar]
- 74.Davì M. V., Bodei L., Ferdeghini M., et al. Multidisciplinary approach including receptor radionuclide therapy with 90Y-DOTATOC ([90Y-DOTA0,Tyr3]-octreotide) and 177Lu-DOTATATE ([177Lu-DOTA0,Tyr3]-octreotate) in ectopic Cushing syndrome from a metastatic gastrinoma: a promising proposal. Endocrine Practice. 2008;14(2):213–218. doi: 10.4158/ep.14.2.213. [DOI] [PubMed] [Google Scholar]
- 75.Kwekkeboom D. J., Bakker W. H., Kooij P. P., et al. [177Lu-DOTA0,Tyr3]octreotate: comparison with [111In-DTPA0]octreotide in patients. European Journal of Nuclear Medicine. 2001;28(9):1319–1325. doi: 10.1007/s002590100574. [DOI] [PubMed] [Google Scholar]
- 76.Ginj M., Hinni K., Tschumi S., Schulz S., Maecke H. R. Trifunctional somatostatin-based derivatives designed for targeted radiotherapy using auger electron emitters. Journal of Nuclear Medicine. 2005;46(12):2097–2103. [PubMed] [Google Scholar]
- 77.Vinjamuri S., Gilbert T. M., Banks M., et al. Peptide receptor radionuclide therapy with 90 Y-DOTATATE/90 Y-DOTATOC in patients with progressive metastatic neuroendocrine tumours: assessment of response, survival and toxicity. British Journal of Cancer. 2013;108(7):1440–1448. doi: 10.1038/bjc.2013.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Bodei L., Cremonesi M., Grana C. M., et al. Yttrium-labelled peptides for therapy of NET. European Journal of Nuclear Medicine and Molecular Imaging. 2012;39(supplement 1):S93–S102. doi: 10.1007/s00259-011-2002-y. [DOI] [PubMed] [Google Scholar]
- 79.Forrer F., Waldherr C., Maecke H. R., Mueller-Brand J. Targeted radionuclide therapy with 90Y-DOTATOC in patients with neuroendocrine tumors. Anticancer Research. 2006;26(1):703–707. [PubMed] [Google Scholar]
- 80.Waldherr C., Pless M., Maecke H. R., Haldemann A., Mueller-Brand J. The clinical value of [90Y-DOTA]-D-Phe1-Tyr3-octreotide (90Y-DOTATOC) in the treatment of neuroendocrine tumours: a clinical phase II study. Annals of Oncology. 2001;12(7):941–945. doi: 10.1023/a:1011160913619. [DOI] [PubMed] [Google Scholar]
- 81.Kwekkeboom D. J., de Herder W. W., Kam B. L., et al. Treatment with the radiolabeled somatostatin analog [177Lu-DOTA0,Tyr3]octreotate: toxicity, efficacy, and survival. Journal of Clinical Oncology. 2008;26(13):2124–2130. doi: 10.1200/jco.2007.15.2553. [DOI] [PubMed] [Google Scholar]
- 82.Sansovini M., Severi S., Ambrosetti A., et al. Treatment with the radiolabelled somatostatin analog 177Lu-DOTATATE for advanced pancreatic neuroendocrine tumors. Neuroendocrinology. 2013;97(4):347–354. doi: 10.1159/000348394. [DOI] [PubMed] [Google Scholar]
- 83.Seregni E., Maccauro M., Chiesa C., et al. Treatment with tandem [90Y]DOTA-TATE and [177Lu] DOTA-TATE of neuroendocrine tumours refractory to conventional therapy. European Journal of Nuclear Medicine and Molecular Imaging. 2014;41(2):223–230. doi: 10.1007/s00259-013-2578-5. [DOI] [PubMed] [Google Scholar]
- 84.Imhof A., Brunner P., Marincek N., et al. Response, survival, and long-term toxicity after therapy with the radiolabeled somatostatin analogue [90Y-DOTA]-TOC in metastasized neuroendocrine cancers. Journal of Clinical Oncology. 2011;29(17):2416–2423. doi: 10.1200/JCO.2010.33.7873. [DOI] [PubMed] [Google Scholar]
- 85.Nisa L., Savelli G., Giubbini R. Yttrium-90 DOTATOC therapy in GEP-NET and other SST2 expressing tumors: a selected review. Annals of Nuclear Medicine. 2011;25(2):75–85. doi: 10.1007/s12149-010-0444-0. [DOI] [PubMed] [Google Scholar]
- 86.de Jong M., Breeman W. A. P., Valkema R., Bernard B. F., Krenning E. P. Combination radionuclide therapy using 177Lu and 90Y-labeled somatostatin analogs. Journal of Nuclear Medicine. 2005;46(1, supplement):13S–17S. [PubMed] [Google Scholar]
- 87.Romer A., Seiler D., Marincek N., et al. Somatostatin-based radiopeptide therapy with [177Lu-DOTA]-TOC versus [90Y-DOTA]-TOC in neuroendocrine tumours. European Journal of Nuclear Medicine and Molecular Imaging. 2014;41(2):214–222. doi: 10.1007/s00259-013-2559-8. [DOI] [PubMed] [Google Scholar]
- 88.Reubi J. C., Schär J.-C., Waser B., et al. Affinity profiles for human somatostatin receptor subtypes SST1-SST5 of somatostatin radiotracers selected for scintigraphic and radiotherapeutic use. European Journal of Nuclear Medicine. 2000;27(3):273–282. doi: 10.1007/s002590050034. [DOI] [PubMed] [Google Scholar]
- 89.Forrer F., Uusijärvi H., Storch D., Maecke H. R., Mueller-Brand J. Treatment with 177Lu-DOTATOC of patients with relapse of neuroendocrine tumors after treatment with 90Y-DOTATOC. Journal of Nuclear Medicine. 2005;46(8):1310–1316. [PubMed] [Google Scholar]
- 90.Bison S. M., Konijnenberg M. W., Melis M., et al. Peptide receptor radionuclide therapy using radiolabeled somatostatin analogs: focus on future developments. Clinical and Translational Imaging. 2014;2(1):55–66. doi: 10.1007/s40336-014-0054-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Graf F., Fahrer J., Maus S., et al. DNA double strand breaks as predictor of efficacy of the alpha-particle emitter Ac-225 and the electron emitter Lu-177 for somatostatin receptor targeted radiotherapy. PLoS ONE. 2014;9(2) doi: 10.1371/journal.pone.0088239.e88239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Palayoor S. T., Humm J. L., Atcher R. W., Hines J. J., Macklis R. M. G2M arrest and apoptosis in murine T lymphoma cells following exposure to 212Bi alpha particle irradiation. Nuclear Medicine and Biology. 1993;20(6):795–805. doi: 10.1016/0969-8051(93)90166-R. [DOI] [PubMed] [Google Scholar]
- 93.Nayak T. K., Norenberg J. P., Anderson T. L., Prossnitz E. R., Stabin M. G., Atcher R. W. Somatostatin-receptor-targeted α-emitting 213Bi is therapeutically more effective than β—emitting 177Lu in human pancreatic adenocarcinoma cells. Nuclear Medicine and Biology. 2007;34(2):185–193. doi: 10.1016/j.nucmedbio.2006.11.006. [DOI] [PubMed] [Google Scholar]
- 94.Miederer M., Henriksen G., Alke A., et al. Preclinical evaluation of the α-particle generator nuclide 225Ac for somatostatin receptor radiotherapy of neuroendocrine tumors. Clinical Cancer Research. 2008;14(11):3555–3561. doi: 10.1158/1078-0432.CCR-07-4647. [DOI] [PubMed] [Google Scholar]
- 95.Norenberg J. P., Krenning B. J., Konings I. R. H. M., et al. 213Bi-[DOTA0,Tyr3]octreotide peptide receptor radionuclide therapy of pancreatic tumors in a preclinical animal model. Clinical Cancer Research. 2006;12(3, part 1):897–903. doi: 10.1158/1078-0432.ccr-05-1264. [DOI] [PubMed] [Google Scholar]
- 96.Goodhead D. T. Mechanisms for the biological effectiveness of high-LET radiations. Journal of Radiation Research. 1999;40(supplement):1–13. doi: 10.1269/jrr.40.s1. [DOI] [PubMed] [Google Scholar]
- 97.Matthews K., Noker P. E., Tian B., et al. Identifying the safety profile of Ad5.SSTR/TK.RGD, a novel infectivity-enhanced bicistronic adenovirus, in anticipation of a phase I clinical trial in patients with recurrent ovarian cancer. Clinical Cancer Research. 2009;15(12):4131–4137. doi: 10.1158/1078-0432.ccr-08-3354. [DOI] [PubMed] [Google Scholar]
- 98.Verwijnen S. M., Smith P. A. E. S., Hoeben R. C., et al. Molecular imaging and treatment of malignant gliomas following adenoviral transfer of the herpes simplex virus-thymidine kinase gene and the somatostatin receptor subtype 2 gene. Cancer Biotherapy and Radiopharmaceuticals. 2004;19(1):111–120. doi: 10.1089/108497804773391757. [DOI] [PubMed] [Google Scholar]
- 99.Kim K. H., Dmitriev I., O'Malley J. P., et al. A phase I clinical trial of Ad5.SSTR/TK.RGD, a novel infectivity-enhanced bicistronic adenovirus, in patients with recurrent gynecologic cancer. Clinical Cancer Research. 2012;18(12):3440–3451. doi: 10.1158/1078-0432.CCR-11-2852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Higashi K., Hazama S., Araki A., et al. A novel cancer vaccine strategy with combined IL-18 and HSV-TK gene therapy driven by the hTERT promoter in a murine colorectal cancer model. International Journal of Oncology. 2014;45(4):1412–1420. doi: 10.3892/ijo.2014.2557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Zinn K. R., Chaudhuri T. R., Krasnykh V. N., et al. Gamma camera dual imaging with a somatostatin receptor and thymidine kinase after gene transfer with a bicistronic adenovirus in mice. Radiology. 2002;223(2):417–425. doi: 10.1148/radiol.2232010501. [DOI] [PubMed] [Google Scholar]
- 102.ter Horst M., Verwijnen S. M., Brouwer E., et al. Locoregional delivery of adenoviral vectors. Journal of Nuclear Medicine. 2006;47(9):1483–1489. [PubMed] [Google Scholar]
- 103.Akerstrom V., Chen C., Lan M. S., Breslin M. B. Adenoviral insulinoma-associated protein 1 promoter-driven suicide gene therapy with enhanced selectivity for treatment of neuroendocrine cancers. Ochsner Journal. 2013;13(1):91–99. [PMC free article] [PubMed] [Google Scholar]
- 104.Capasso C., Garofalo M., Hirvinen M., Cerullo V. The evolution of adenoviral vectors through genetic and chemical surface modifications. Viruses. 2014;6(2):832–855. doi: 10.3390/v6020832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Castro M. G., Colfi M., Wilson T. J., et al. Adenoviral vector-mediated gene therapy for gliomas: coming of age. Expert Opinion on Biological Therapy. 2014;14(9):1241–1257. doi: 10.1517/14712598.2014.915307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Zinn E., Venberghe L. H. Adeno-associated virus: fit to serve. Current Opinion in Virology. 2014;8:90–97. doi: 10.1016/j.coviro.2014.07.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Ibraheem D., Elaissari A., Fessi H. Gene therapy and DNA delivery systems. International Journal of Pharmaceutics. 2014;459(1-2):70–83. doi: 10.1016/j.ijpharm.2013.11.041. [DOI] [PubMed] [Google Scholar]
- 108.Young L. S., Searle P. F., Onion D., Mautner V. Viral gene therapy strategies: from basic science to clinical application. Journal of Pathology. 2006;208(2):299–318. doi: 10.1002/path.1896. [DOI] [PubMed] [Google Scholar]
- 109.McCart J. A., Mehta N., Scollard D., et al. Oncolytic vaccinia virus expressing the human somatostatin receptor SSTR2: molecular imaging after systemic delivery using 111In-pentetreotide. Molecular Therapy. 2004;10(3):553–561. doi: 10.1016/j.ymthe.2004.06.158. [DOI] [PubMed] [Google Scholar]
- 110.Hruby D. E. Vaccinia virus vectors: new strategies for producing recombinant vaccines. Clinical Microbiology Reviews. 1990;3(2):153–170. doi: 10.1128/cmr.3.2.153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Wang N., Zhang H., Zhang B.-Q., et al. Adenovirus-mediated efficient gene transfer into cultured three-dimensional organoids. PLoS ONE. 2014;9(4) doi: 10.1371/journal.pone.0093608.e93608 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Nair S., Curiel D. T., Rajaratnam V., Thota C., Al-Hendy A. Targeting adenoviral vectors for enhanced gene therapy of uterine leiomyomas. Human Reproduction. 2013;28(9):2398–2406. doi: 10.1093/humrep/det275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.McCormick F. Cancer gene therapy: fringe or cutting edge? Nature Reviews Cancer. 2001;1(2):130–141. doi: 10.1038/35101008. [DOI] [PubMed] [Google Scholar]
- 114.Kundra V., Mannting F., Jones A. G., Kassis A. I. Noninvasive monitoring of somatostatin receptor type 2 chimeric gene transfer. Journal of Nuclear Medicine. 2002;43(3):406–412. [PubMed] [Google Scholar]
- 115.Hemminki A., Belousova N., Zinn K. R., et al. An adenovirus with enhanced infectivity mediates molecular chemotherapy of ovarian cancer cells and allows imaging of gene expression. Molecular Therapy. 2001;4(3):223–231. doi: 10.1006/mthe.2001.0446. [DOI] [PubMed] [Google Scholar]
- 116.van Essen M., Krenning E. P., Kam B. L. R., de Jong M., Valkema R., Kwekkeboom D. J. Peptide-receptor radionuclide therapy for endocrine tumors. Nature Reviews Endocrinology. 2009;5(7):382–393. doi: 10.1038/nrendo.2009.105. [DOI] [PubMed] [Google Scholar]
- 117.Akinlolu O., Ottolino-Perry K., McCart J. A., Reilly R. M. Antiproliferative effects of 111In- or 177Lu-DOTATOC on cells exposed to low multiplicity-of-infection double-deleted vaccinia virus encoding somatostatin subtype-2 receptor. Cancer Biotherapy and Radiopharmaceuticals. 2010;25(3):325–333. doi: 10.1089/cbr.2009.0713. [DOI] [PubMed] [Google Scholar]
- 118.Takahashi M., Sato T., Sagawa T., et al. E1B-55K-deleted adenovirus expressing E1A-13S by AFP-enhancer/promoter is capable of highly specific replication in AFP-producing hepatocellular carcinoma and eradication of established tumor. Molecular Therapy. 2002;5(5):627–634. doi: 10.1006/mthe.2002.0589. [DOI] [PubMed] [Google Scholar]
- 119.Rogers B. E., Zinn K. R., Lin C.-Y., Chaudhuri T. R., Buchsbaum D. J. Targeted radiotherapy with [90Y]-SMT 487 in mice bearing human nonsmall cell lung tumor xenografts induced to express human somatostatin receptor subtype 2 with an adenoviral vector. Cancer. 2002;94(supplement 4):1298–1305. doi: 10.1002/cncr.10300. [DOI] [PubMed] [Google Scholar]
- 120.Chai L.-P., Wang Z.-F., Liang W.-Y., et al. In vitro and in vivo effect of 5-FC combined gene therapy with TNF-alpha and CD suicide gene on human laryngeal carcinoma cell line Hep-2. PLoS ONE. 2013;8(4) doi: 10.1371/journal.pone.0061136.e61136 [DOI] [PMC free article] [PubMed] [Google Scholar]