

Abstract
Background
Posttraumatic stress disorder (PTSD) is associated with abnormal functioning of the hypothalamic-pituitary-adrenal (HPA) axis; however, limited research has examined whether cortisol levels change following successful PTSD treatment. The current study examined the impact of successful PTSD treatment on the cortisol awakening response (CAR).
Method
Twenty-nine adults participating in a treatment trial for chronic PTSD provided saliva samples (upon waking, and 30, 45, and 60-min post-waking) before and after receiving either prolonged exposure therapy or sertraline. PTSD responder status (i.e., loss or retention of a PTSD diagnosis) served as the predictor variable. Outcome measures included area under the curve with respect to ground and increase, reflecting total cortisol output and HPA axis reactivity, respectively.
Results
A series of hierarchical regressions revealed no significant main effects of PTSD responder status for either CAR outcome. However, a significant gender by treatment response interaction for cortisol reactivity revealed that female treatment non-responders displayed higher cortisol reactivity following treatment than female responders, whereas cortisol reactivity did not change pre- to post-treatment for male responders. Findings remained after controlling for age, trauma history, baseline medication status, baseline PTSD, and baseline depressive symptoms.
Conclusion
Loss of a PTSD diagnosis may contribute to decreased cortisol reactivity in females. Neuroendocrine changes following treatment may emerge only for specific subgroups, highlighting the importance of exploring treatment moderators.
Keywords: Stress Disorders, Posttraumatic, Treatment, Prolonged Exposure, Sertraline, Gender, Cortisol
Rates of posttraumatic stress disorder (PTSD) in the general population range from 6.4–6.8%1,2, but vary by gender: females display higher prevalence (8.6%) than males (4.1%2). Co-occurring diagnoses of mood, anxiety, alcohol/substance use disorders2, and impaired physical health3 are the norm, rather than the exception, for individuals with PTSD.
Given consistently observed health correlates/consequences of PTSD, treating the disorder has remained a critical focus for researchers and clinicians. Such efforts have led to the development and refinement of numerous interventions4–8. Evidence-based psychotherapeutic and psychopharmacological PTSD treatments include cognitive behavioral therapies (CBT: prolonged exposure [PE] and cognitive processing therapy) and selective serotonin reuptake inhibitors (SSRIs), respectively. CBT is a first-line treatment for PTSD9–11, with treatment gains lasting up to 5–10 years post-therapy10. The SSRIs sertraline (Zoloft) and paroxetine (Paxil) are the only FDA approved, first-line treatment medications for PTSD12–14.
Though cortisol abnormalities are common in individuals with PTSD (for review, see15), mixed findings have resulted from the few studies that have examined the impact of successful PTSD treatment (via psychotherapeutic16,17, psychopharmacological18, and most recently, virtual reality exposure (VRE) therapies19) on cortisol outcomes. Recently, Rothbaum and colleagues19 conducted a randomized controlled trial examining the efficacy of a 5-session VRE therapy augmented with D-cycloserine, alprazolam, or placebo. Three samples of salivary cortisol (pre-, post-, and 15-minutes post-VRE) were collected at baseline, post-treatment, and 6-months post-treatment assessment. At post-treatment, change scores revealed that cortisol levels decreased the most across samples (from pre-to 15 min. post-exposure) for those who received D-cycloserine compared to alprazolam or placebo. Authors attributed this attenuated cortisol response to the extinction effects of D-cycloserine, such that those who received the latter medication experienced enhanced extinction of fear to trauma-related virtual reality scenes19.
Gerardi and colleagues16 assessed salivary cortisol levels in female rape victims randomly assigned to receive either PE or Eye Movement Desensitization and Reprocessing. Saliva samples were obtained at the end of the first and last exposure session. No differences in cortisol levels between treatments, or changes following treatment emerged. However, treatment responders (defined as 50% reductions in PTSD and depressive symptoms) displayed decreased cortisol levels relative to baseline, and treatment non-responders tended to show increased cortisol levels from initial to last exposure session. Similar to the findings of Rothbaum and colleagues19, the observed cortisol decreases in responders may reflect decreased reactivity to reminders of the stressor.
In contrast, a study testing the efficacy of brief eclectic psychotherapy at normalizing cortisol levels (obtained via one morning blood sample) in 21 individuals with chronic PTSD produced contradictory results17. Cortisol levels increased from pre- to post-treatment in treatment responders (defined as loss of PTSD diagnosis) but decreased in non-responders. However, this effect emerged only when controlling for change in depressive symptoms.
Finally, Tucker and colleagues18 examined pre- and post-treatment levels of cortisol (via saliva samples obtained at 8 am and 4 pm) and immune-related factors in 58 individuals with PTSD randomly assigned to receive citalopram, sertraline, or placebo. Although immune function normalized following significant reduction of PTSD and depressive symptoms, cortisol levels did not change18.
Though this research is suggestive of post-treatment cortisol changes, limitations exist regarding the failure to account for diurnal cortisol variations16,17,19 and to include both genders16. Further, the extant literature has primarily focused upon changes in cortisol levels across time. Given that available research has produced equivocal findings, with some studies finding low cortisol levels in individuals with PTSD20–22 and some finding high cortisol levelsfor a review see 23, measures of overall HPA axis activity should also be considered.
One such measure is the cortisol awakening response (CAR). The CAR provides two outcomes for analysis: a composite variable of total cortisol output/volume, calculated as the area under the curve with respect to the ground (AUCg), and a measure of change or HPA reactivity, calculated as the area under the curve with respect to the increase (AUCi 24,25). The latter is considered to be a more accurate reflection of HPA activation in relation to PTSD than cortisol levels or output24. CAR is assessed by obtaining multiple saliva samples with the first sample reflecting pre-awakening cortisol output, and subsequent samples (15, 30, 45, or 60 min. post-awakening) reflecting the pattern of cortisol increase thereafter, with the peak occurring between 20–45 min post-awakening24,26,27.
The CAR has not been widely studied in relation to PTSD, and the existing literature reveals mixed results. A recent meta-analysis examining the association between the CAR and psychosocial factors included five studies of posttraumatic stress24. Though no significant relationships emerged between posttraumatic stress and CAR increase (defined by the AUCi, and the mean cortisol increase)24, analysis of the highest quality studies (n = 2) revealed a negative relationship. These results suggest that higher PTSD symptoms were associated with smaller increases in cortisol after awakening, perhaps reflecting an overburdened neuroendocrine system (i.e., general hypocortisolism). Conversely, in accordance with literature suggesting that greater HPA responsiveness is present in clinical samples28, Inslicht and colleagues29 found that, in a sample of active duty police officers, larger increases in the CAR assessed prior to critical incident exposure (defined as cumulative critical incidents experienced in the line of duty) predicted higher peritraumatic dissociation and acute stress disorder symptoms post-exposure.
The present study builds upon previous literature by examining the impact of successful PTSD treatment on the CAR in males and females with chronic PTSD. This study is the first to examine CAR differences in treatment responders vs. non-responders. The two most frequently used indices of the CAR, total cortisol output (AUCg) and the post-awakening dynamic increase/change in cortisol (AUCi)26, served as outcome variables. As findings regarding the CAR and PTSD are mixed, we hypothesized differences in CAR among treatment responders vs. non-responders, but did not hypothesize a specific direction.
Method
Participants
The sample (n = 29) was part of a larger clinical treatment trial of individuals with chronic PTSD. Participants were recruited through clinical referrals and community advertising. Inclusion criteria included: adults between the ages of 18 and 65, and DSM-IV primary diagnosis of chronic PTSD. Exclusion criteria included: current diagnosis of schizophrenia or delusional disorder; medically unstable bipolar disorder, depression with psychotic features, or depression severe enough to require immediate psychiatric treatment (e.g., actively suicidal); severe self-injurious behavior or suicide attempt within the past 3-months; no clear trauma memory or trauma before age three; current diagnosis of alcohol or substance dependence within the previous 3-months; ongoing intimate relationship with the perpetrator (in assault cases); unwilling or medically not advisable to stop current CBT or antidepressant medication, based on condition assignment; previous non-response to adequate trial of either PE (eight sessions or more) or sertraline (150 mg/d; eight weeks); or medical contraindication for the initiation of sertraline (e.g., pregnancy/likely to become pregnant).
Overview of Treatment
Treatment consisted of either ten weeks of psychotherapy or pharmacotherapy. All therapists received standardized clinical training, through multiple-day initial training workshops and ongoing clinical supervision.
Psychotherapy
PE consisted of ten weekly, 90–120 min sessions, which included psychoeducation, breathing retraining, approaching avoided situations outside of therapy (i.e., in vivo exposure), and approaching the memory of the trauma repeatedly (i.e., imaginal exposure)30. Patients were assigned weekly homework including listening to their imaginal exposure tapes and practicing in vivo exposure exercises.
Pharmacotherapy
Pharmacotherapy consisted of ten weeks of sertraline, monitored by a board certified psychiatrist. Each session lasted up to 30 min. Sertraline was adjusted based on a standardized titration algorithm31, starting at 25 mg/day and proceeding up to 200 mg/day, if indicated. The mean dosage at the end of treatment was 135.68 mg/day (SD = 66.80). During visits, the psychiatrist monitored side effects, adjusted medication dosage, and provided general encouragement and support.
Supervision and treatment integrity
PE therapists were masters or PhD level and study psychiatrists were board certified and experienced in anxiety disorder treatment. Treatment sessions were video or audiotaped. PE supervision occurred weekly at each site including case discussion and tape review. The administration of sertraline was overseen by Medical Directors, and integrity ratings were based on published protocols 32,33. Trained raters reviewed 10% of videotapes, assessing essential treatment components and protocol violations. For essential components, PE providers completed 90%, and SER providers completed 96%. No protocol violations were observed. PE sessions were also rated for therapist competence (e.g., interactive exchanges with client) on a 3-point scale (1 = Inadequate, 3 = Adequate or Better). Overall PE therapist competence was very good (M = 2.73, SD = .32).
Measures
Independent evaluators who received standardized training on administration of the PTSD Symptom Scale-Interview (PSS-I) and Structured Clinical Interview for DSM-IV (SCID-IV) completed the interviews. Interviewers were trained mental health professionals (i.e., doctoral candidates and Ph.D. level psychologists) who met 80% reliability criterion on training interviews.
Sociodemographics
At baseline, participants reported their age, gender, and race/ethnicity, and completed brief questionnaires regarding trauma history and mental health treatment history.
PSS-I
The PSS-I34, a 17-item interview measure of PTSD symptoms, was administered at baseline and post-intervention. The PSS-I provides a current DSM-IV PTSD diagnosis and severity score. Items are rated on a 0–3 scale combining frequency and severity of symptoms during the past 2-weeks. Higher scores indicate more severe symptoms. Inter-rater reliability was high in the current study (intra-class correlation coefficient = .985; based upon the randomly selected 10% of cases coded for reliability in the larger study).
SCID-IV
The SCID-IV35, a diagnostic interview based upon DSM-IV criteria, was administered at baseline to assess inclusion/exclusion criteria, including current and lifetime history of MDD, substance use, and psychotic disorders. Based on a randomly selected 10% of cases, reliability for the SCID-IV was good36,37 (current MDD κ = .68, ppos = .88, pneg = .80; substance abuse disorders ppos = .00, pneg = 1.00; and other diagnoses ppos =.00, pneg = 1.00).
Beck Depression Inventory (BDI)
The Beck Depression Inventory38 is a 21-item self-report measure assessing depression severity. Each item is scored from 0 to 3, with increasing scores indicating greater severity of depression. The BDI demonstrates good reliability and validity39.
Salivary Cortisol: CAR
Participants were provided with detailed instructions regarding the collection of four salivary cortisol samples. Using Salivette sampling devices (Sarstedt, Newton, NC), participants were instructed to collect the first sample immediately upon waking, and the remaining samples 30-, 45-, and 60-min post-waking. Participants were also instructed not to eat, drink, smoke, or brush their teeth prior to and during the sampling period. We relied on participants’ self-report regarding the timing of each sample to examine protocol adherence. Samples were stored in participants’ freezers until research staff collected them, and were then stored in a −80°C freezer until shipped to the Center for Psychobiology and Psychosomatic Research (Trier, Germany) for assay. Samples were analyzed according to a time-resolved immunoassay with fluorescence detection (DELPIA40).
Procedure
Interested participants were initially screened for eligibility by telephone. If eligible, they were invited for a diagnostic interview. The interviewer obtained informed consent and further determined eligibility. Independent evaluators conducted structured interviews to collect demographic information, and assess PTSD diagnosis and symptom severity and MDD diagnosis. Self-report measures were also completed (BDI). Following this baseline interview, participants began weekly regimens of either pharmacotherapy or psychotherapy. Participants also collected saliva samples for CAR analysis before treatment initiation and at the completion of treatment.
Data Analysis Plan
Analyses were conducted with Statistics Package for the Social Sciences Version 2141, and an alpha level of .05 (two-tailed) was used to determine significance.
Preliminary analyses
Preliminary analyses were conducted to examine bivariate relationships between the variables of interest, and to determine whether, and for which outcomes, moderator analyses were warranted. As such, chi-square analyses were conducted between PTSD treatment response (loss vs. retention of PTSD diagnosis) and gender to test for possible control variables and report upon PTSD outcomes following treatment. One-way ANOVAs were conducted to examine differences in the CAR based upon gender and PTSD treatment response, and Pearson product moment correlations were conducted to test for variables scored continuously.
Primary and moderator analyses
To test the primary hypothesis regarding whether PTSD treatment response predicted CAR outcomes (AUCi and AUCg), separate hierarchical linear regression analyses were conducted. These same analyses were also used to test the moderating effect of gender on the relationship between PTSD and the CAR.
Results
Descriptive Statistics
Twenty-nine adults with chronic PTSD (21 females, 8 males) randomized to receive either PE (n = 18) or sertraline (n = 11) provided complete saliva samples at both the baseline and post-intervention assessments. The majority of the sample was Caucasian (82.8%), with a mean age of 36.2 years (SD = 11.2 years). Participants experienced a wide range of trauma, including non-sexual assault (31.0%), sexual assault (27.6%), motor vehicle or general accident (17.2%), natural disaster or combat (6.8%), the experience of death of a loved one (6.9%), childhood non-sexual assault (6.9%), and childhood sexual assault (3.4%). On average, participants reported experiencing 8.21 (SD = 7.06) types of Criterion A traumatic incidents. In addition to having PTSD, 62.0% of the participants also presented with current comorbid major depression, and 86.2% had been diagnosed with major depression at some point in their lifetime. With the exception of this subsample consisting of fewer minorities (18.8% compared to 35%), current participants did not differ from those in the larger trial.
At the beginning of the study, four participants were stabilized on antidepressant medication, one was on a sleep aid medication, and one additional participant was taking synthroid. As controlling for pre-treatment medication status (or exclusion of this latter participant from analysis) did not impact these results, all participants were included in the final analyses to maintain integrity of the sample.
Preliminary analyses
AUC changes from baseline to post-treatment did not differ based upon treatment type (PE vs. sertraline: AUCi change: F(1, 27) = .15, p = .70; AUCg change: F(1,27) = .51, p = .48). Therefore, treatment type was collapsed for all remaining analyses.
PTSD response
Following treatment, 23 participants were categorized as treatment responders (i.e., loss of PTSD diagnosis), and the remaining 6 participants were considered treatment non-responders (i.e., retention of PTSD diagnosis). Treatment response was differentially impacted by gender (χ2 [1, N = 29] = 5.78, p = .02), such that a higher proportion of females responded to treatment (90.48%; n =19) than males (50.00%; n = 4).
Bivariate associations
Correlations revealed that younger participants had lower AUCg, depressive symptoms, and PTSD symptoms at post-intervention, but not at baseline (see Table 1). Post-intervention PTSD and depressive symptoms were highly multicollinear (r = .87), suggesting that improvement in PTSD symptoms highly overlapped with improvement in depressive symptoms. Regarding the outcome variables, baseline (but not post-intervention) levels of AUCg were positively associated with levels of AUCi, suggesting a moderate correlation among CAR parameters. Higher AUCi at baseline was associated with lower PTSD (trend level) and depressive symptoms post-intervention, and higher AUCg post-intervention was associated with higher post-intervention levels of PTSD at a trend level. Given these associations, baseline levels of AUCi and AUCg were used as covariates in respective analyses.
Table 1.
Bivariate Correlations among Demographic and Key Study Variables
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Age | - | ||||||||
| 2. Baseline Depressive Symptoms | .30 | - | |||||||
| 3. Post-Treatment Depressive Symptoms | .40* | .42* | - | ||||||
| 4. Baseline PTSD Severity | −.20 | .44* | .00 | - | |||||
| 5. Post-Treatment PTSD Severity | .41* | .32+ | .87*** | .13 | - | ||||
| 6. Baseline AUCi | −.07 | −07 | −.45* | .13 | −.36+ | - | |||
| 7. Post-Treatment AUCi | −.03 | −.04 | −.21 | .03 | −.13 | .32+ | - | ||
| 8. Baseline AUCg | −.02 | −.08 | −.26 | −.21 | −.22 | .50** | .51** | - | |
| 9. Post-Treatment AUCg | .37* | .20 | .23 | −.03 | .31+ | .09 | .43* | .45* | - |
Note. Correlations are based upon a sample size of n = 29. PTSD = PTSD Symptoms. AUCi= Area under the curve with respect to increase. AUCg= Area under the curve with respect to the ground.
p<.05.
p<.01.
p<.001.
p ≤ .10.
As seen in Table 2, neither gender nor treatment response differentially impacted AUCg. However, PTSD treatment responders had higher cortisol reactivity (AUCi) at baseline than treatment non-responders (Cohen’s d = 1.12). Further, females displayed higher cortisol reactivity than males at baseline (Cohen’s d = .93) and post-intervention (Cohen’s d = .94). Based upon these differences, gender was examined as a moderator of PTSD treatment response and cortisol reactivity.
Table 2.
Sample Characteristics (N= 29)
| Auci | Aucg | |||
|---|---|---|---|---|
|
| ||||
| Baseline M (SD) |
Post-Treatment M (SD) |
Baseline M (SD) |
Post-Treatment M (SD) |
|
| Gender | ||||
| Males | −79.31 (274.07) | −41.98 (191.86) | 773.51 (457.37) | 907.07 (453.16) |
| Females | 382.24 (374.82) | 221.60 (275.31) | 1034.02 (356.10) | 941.63 (461.69) |
| Total | 254.91 (403.98) | 148.89 (278.78) | 958.09 (390.48) | 914.15 (442.92) |
| F | 10.00** | 6.13* | 2.61 | 0.00 |
| Treatment Response | ||||
| Treatment Non-Responder | −41.28 (239.31) | 69.13 (375.22) | 756.13 (331.85) | 1035.63 (399.16) |
| Treatment Responder | 332.18 (405.62) | 169.69 (254.41) | 1010.67 (393.73) | 882.47 (456.50) |
| Total | 254.91 (403.98) | 148.89 (278.77) | 458.01 (390.49) | 914.15 (442.92) |
| F | 4.56* | .61 | 2.10 | .56 |
Note. AUCi= Area under the curve with respect to increase. AUCg= Area under the curve with respect to the ground.
p<.05.
p<.01.
p<.001.
p ≤ .10.
Primary Analyses
Regression analyses examined the impact of successful PTSD treatment on the CAR. The addition of age, trauma history, pre-treatment medication status, and baseline PTSD and depressive symptoms as covariates in the following analyses did not impact the findings and are therefore not reported below.
Cortisol reactivity (AUCi)
As seen in Table 3, after controlling for baseline levels of AUCi, there were no main effects of gender (β = .09, p > .05) or treatment response (β = −.33, p > .05) on post-intervention levels of AUCi. However, a significant interaction emerged between gender and treatment response in post-treatment levels of AUCi (β = .55, p = .02). Upon decomposition of the interaction, simple slope analyses revealed that female treatment non-responders displayed higher cortisol reactivity than female treatment responders (β = .56, p = .05), whereas cortisol reactivity did not differ for male responders vs. non-responders (β = −.33, p> .05). See Figure 1.
Table 3.
Summary of Hierarchical Regression Moderation Analyses Examining the Impact of Treatment Response on AUCg and AUCi
| Step and Variables | B | SE B | 95% CI | β | ΔR2 |
|---|---|---|---|---|---|
| Outcome: Post-Treatment AUCg | |||||
| Step 1 | |||||
| Baseline AUCg | 0.51 | 0.20 | 0.11, 0.91 | 0.44* | 0.20* |
| Step 2 | |||||
| Baseline AUCg | 0.60 | 0.19 | 0.19, 1.00 | 0.52** | |
|
| |||||
| Outcome: Post-Treatment AUCi | |||||
| Step 1 | |||||
| Baseline AUCi | 0.22 | 0.13 | −0.04, 0.48 | 0.32+ | 0.10+ |
| Step 2 | |||||
| Baseline AUCi | 0.10 | 0.15 | −0.20, 0.40 | 0.15 | |
| Responder Status | 54.90 | 137.66 | −228.61, 338.41 | 0.08 | |
| Gender | 239.53 | 135.01 | −38.53, 517.59 | 0.39+ | 0.10 |
| Step 3 | |||||
| Baseline AUCi | 0.14 | 0.14 | −0.14, 0.42 | 0.20 | |
| Responder Status | −222.96 | 171.14 | −576.17, 130.25 | −0.33 | |
| Gender | 53.09 | 146.04 | −248.33, 354.50 | 0.09 | |
| Responder Status x Gender | 599.05 | 249.34 | 84.43, 1113.67 | 0.55* | 0.16* |
Note. AUCg = Area under the curve with respect to the ground. AUCi = Area under the curve with respect to increase. Treatment Responder Status was coded such that a value of 0 = No PTSD diagnosis and a value of 1 = PTSD diagnosis. Gender was dummy coded such that a value of 0 = male and a value of 1 = female.
p < .05.
p < .01.
p < .001.
Figure 1.
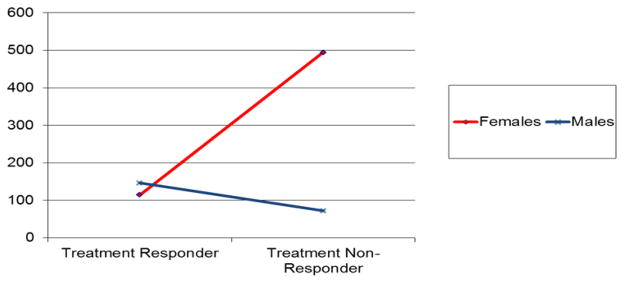
Graph of interaction between gender and PTSD treatment response on post-treatment cortisol reactivity.
Cortisol Output (AUCg)
After controlling for baseline levels of AUCg, there was no main effect of treatment response (β = .28, p > .05), suggesting that cortisol output was not impacted by PTSD treatment response (see Table 3).
Discussion
To our knowledge, the current study was the first to examine the impact of successful PTSD treatment on the CAR in adults with chronic PTSD. Though PTSD treatment responders did not differ from non-responders in total cortisol output or cortisol reactivity, moderation analyses revealed that the cortisol reactivity of female treatment non-responders was higher than that of female treatment responders. No differences emerged for males. Findings remained robust after controlling for age, trauma history, baseline medication status, baseline PTSD, and depressive symptoms.
Results of two prior studies16,19 have suggested that cortisol decreases following successful PTSD treatment may have resulted from either a decreased reactivity to or extinguished fear reaction to reminders/exposures of the index stressor. The present study more directly tests this hypothesis as the CAR can be computed as both an index of cortisol reactivity and output. That changes were evident only for the outcome of cortisol reactivity provides additional support that reactivity measures may be a more sensitive index of neuroendocrine activity than gross output23. However, it is important to consider that no main effects of PTSD responder status emerged for either outcome, highlighting the importance of exploring moderators when dealing with treatment outcomes involving sensitive biological changes42. These results contradict Chida and colleagues’24 meta-analysis, suggesting that individuals with PTSD displayed lower AUCi. However, they included cross-sectional, non-treatment studies that directly compared PTSD to controls, without consideration of gender differences. Given these and sampling differences (Veterans only43), the conflicting findings may be attributable to study design or third variables.
Given that females (vs. males) display elevated rates of PTSD in the face of fewer traumatic exposures44, it seems likely that gender differences would also affect biological outcome. As females displayed higher baseline cortisol reactivity than males, and higher AUCi at baseline was associated with lower post-intervention PTSD (trend level), it is possible that females were able to reap greater benefits of the intervention due to the relative association between elevated baseline reactivity and lower post-intervention PTSD (though statistical regression to the mean cannot be ruled out45).
Furthermore, though gender differences regarding the CAR are oftentimes null/non-robust, a few studies have reported that females display hyper-reactivity, or larger increases in cortisol after awakening (albeit small effects26,46). Should this be the case, females may have greater room for improvement following successful treatment. Traditionally, this difference has been explained by higher rates of depression and general anxiety disorders among women with interpersonal traumatic histories28. However, both genders in the current sample reported similar prior trauma and symptom severity, making them both susceptible to CAR increases. Nonetheless, it is possible that females with extensive interpersonal trauma histories may be more likely to experience reductions in both psychological and biological abnormalities following successful treatment. Given the paucity of gender-based research examining treatment effects on the CAR, these results highlight the need for additional research, including mediators of biological change, on this important topic.
The current findings must be interpreted with caution in light of the following limitations: unequal gender distribution, small sample size and limited power, and the single day sampling protocols to assess the CAR. Replication of the secondary neuroendocrine effects of PTSD treatment is necessary in larger clinical trials involving multiple CAR sampling days at pre-and post-treatment27. The addition of a longer follow-up period would allow for the tracking of CAR changes in the weeks and months following therapy. Further, given established differences in trauma types experienced by males and females47, research into the moderating impact of trauma history characteristics on the relationship between PTSD treatment response and the CAR in a larger sample is also warranted. An additional avenue for research may include the direct comparison of baseline CAR in trauma-exposed individuals with and without PTSD. The additional baseline data from this latter group may allow for a better understanding of underlying HPA disturbances, and interpretation of the changes that occur in treatment regarding CAR levels may be more meaningful when placed in this context.
Further, the present sample consisted of a small sample of treatment-seeking individuals with high rates of prior trauma. However, although the numbers of prior traumatic exposures and the rates of PTSD-MDD comorbidity in our sample were high, they are consistent with the larger literature of treatment-seeking48, 49 and non-treatment seeking samples 50–52, suggesting our sample is representative of the larger PTSD population. Despite these limitations, this study was the first to demonstrate CAR changes following successful PTSD treatment (psychotherapy and pharmacotherapy) in female adult trauma survivors. Neuroendocrine changes following treatment may however emerge only for specific subgroups, highlighting the importance of exploring treatment moderators, and mediators of those changes by gender.
Acknowledgments
Manuscript preparation was supported, in part, by an NRSA postdoctoral training grant T32 MH19985, R01 MH066347 (PI: Zoellner), and R01 MH066348 (PI: Feeny) from the National Institute of Mental Health, and by the William T. Dahms, M.D. Clinical Research Unit, funded under the Cleveland Clinical and Translational Science Award (UL1 RR024989).
References
- 1.Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62:593–602. doi: 10.1001/archpsyc.62.6.593. [DOI] [PubMed] [Google Scholar]
- 2.Pietrzak RH, Goldstein RB, Southwick SM, Grant BF. Prevalence and axis I comorbidity of full and partial posttraumatic stress disorder in the United States: Results from Wave 2 of the National Epidemiologic Survey on Alcohol and Related Conditions. J Anxiety Disord. 2011;25:456–465. doi: 10.1016/j.janxdis.2010.11.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pacella ML, Hruska B, Delahanty DL. The physical health consequences of PTSD and PTSD symptoms: A meta-analytic review. J Anxiety Disord. 2013;27:33–46. doi: 10.1016/j.janxdis.2012.08.004. [DOI] [PubMed] [Google Scholar]
- 4.Bisson J, Brayne M, Ochberg F, Everly G. Early psychosocial intervention following traumatic events. Am J Psychiatry. 2007;164:1016–1019. doi: 10.1176/ajp.2007.164.7.1016. [DOI] [PubMed] [Google Scholar]
- 5.Bradley R, Greene J, Russ E, et al. A multidimensional meta-analysis of psychotherapy for PTSD. Am J Psychiatry. 2005;162:214–227. doi: 10.1176/appi.ajp.162.2.214. [DOI] [PubMed] [Google Scholar]
- 6.Ipser JC, Stein DJ. Evidence-based pharmacotherapy of post-traumatic stress disorder (PTSD) The International Journal of Neuropsychopharmacology. 2012;15:825–840. doi: 10.1017/S1461145711001209. [DOI] [PubMed] [Google Scholar]
- 7.Powers MB, Halpern JM, Ferenschak MP, et al. A meta- analytic review of prolonged exposure for posttraumatic stress disorder. Clin Psychol Rev. 2010;30:635–641. doi: 10.1016/j.cpr.2010.04.007. [DOI] [PubMed] [Google Scholar]
- 8.Steckler T, Risbrough V. Pharmacological treatment of PTSD–established and new approaches. Neuropharmacology. 2012;62:617–627. doi: 10.1016/j.neuropharm.2011.06.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Foa EB, Keane T, Friedman M, Cohen J, editors. Effective treatments for PTSD: Practice guidelines from the International Society for Traumatic Stress Studies. New York: Guilford Press; 2009. [Google Scholar]
- 10.Resick PA, Williams LF, Suvak MK, et al. Long-term outcomes of cognitive–behavioral treatments for posttraumatic stress disorder among female rape survivors. J Counsult Clin Psychol. 2012;80:201–210. doi: 10.1037/a0026602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.VA/DoD Guideline Working Group. VA/DoD clinical practice guideline for management of post-traumatic stress. 2010 Retrieved from http://www.healthquality.va.gov/ptsd/ptsd-sum_2010a.pdf.
- 12.Jeffreys M. Clinican’s guide to medications for PTSD. National center for PTSD; 2009. Retrieved from http://www.ptsd.va.gov/professional/pages/clinicians-guide-to-medications-for-ptsd.asp. [Google Scholar]
- 13.Stein DJ, Ipser J, McAnda N. Pharmacotherapy of posttraumatic stress disorder: a review of meta-analyses and treatment guidelines. CNS Spectr. 2009;14:25–31. [PubMed] [Google Scholar]
- 14.Mushtaq D, Ali A, Margoob MA, et al. Association between serotonin transporter gene promoter-region polymorphism and 4-and 12-week treatment response to sertraline in posttraumatic stress disorder. J Affect Disord. 2012;136:955–962. doi: 10.1016/j.jad.2011.08.033. [DOI] [PubMed] [Google Scholar]
- 15.De Kloet CS, Vermetten E, Geuze E, Kavelaars AMAA, Heijnen CJ, Westenberg HGM. Assessment of HPA-axis function in posttraumatic stress disorder: pharmacological and non-pharmacological challenge tests, a review. J Psychiatr Res. 2006;40(6):550–567. doi: 10.1016/j.jpsychires.2005.08.002. [DOI] [PubMed] [Google Scholar]
- 16.Gerardi M, Rothbaum BO, Astin M, Kelley M. Cortisol response following exposure treatment for PTSD in rape victims. Journal of Aggression, Maltreatment, and Trauma. 2010;19:349–356. doi: 10.1080/10926771003781297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Olff M, de Vries G-J, Guzelcan Y, et al. Changes in cortisol and DHEA plasma levels after psychotherapy for PTSD. Psychoneuroendocrinology. 2007;32:619–626. doi: 10.1016/j.psyneuen.2007.04.001. [DOI] [PubMed] [Google Scholar]
- 18.Tucker P, Ruwe WD, Masters B, et al. Nueroimmune and cortisol changes in selective serotonin reuptake inhibitor and placebo treatment of chronic posttraumatic stress disorder. Biol Psychiatr. 2004;56:121–128. doi: 10.1016/j.biopsych.2004.03.009. [DOI] [PubMed] [Google Scholar]
- 19.Rothbaum BO, Price M, Jovanovic T, Norrholm S, Gerardi M, Dunlop B, Davis M, Bradley B, Duncan EJ, Rizzo A, Ressler K. A randomized, double-blind evaluation of D-Cycloserine or Alprazolam combined with virtual reality exposure therapy for posttraumatic stress disorder (PTSD) in OEF/OIF war. Veterans Am J Psychiatry. 2014;171(6):640–648. doi: 10.1176/appi.ajp.2014.13121625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Heim C, Nemeroff CB. Neurobiology of posttraumatic stress disorder. CNS Spectr. 2009;14(1 Suppl 1):13–24. [PubMed] [Google Scholar]
- 21.Pace TWW, Heim CH. A short review on the psychoneuroimmunology of posttraumatic stress disorder: From risk factors to medical comorbidities. Brain Behav Immun. 2011;25:6–13. doi: 10.1016/j.bbi.2010.10.003. [DOI] [PubMed] [Google Scholar]
- 22.Wessa M, Rohleder N. Endocrine and inflammatory alterations in post-traumatic stress disorder. Expert Review of Endocrinology & Metabolism. 2007;2:91–122. doi: 10.1586/17446651.2.1.91. [DOI] [PubMed] [Google Scholar]
- 23.Meewisse ML, Reitsma JB, De Vries GJ, et al. Cortisol and post-traumatic stress disorder in adults Systematic review and meta-analysis. BR J Psychiatry. 2007;191:387–392. doi: 10.1192/bjp.bp.106.024877. [DOI] [PubMed] [Google Scholar]
- 24.Chida Y, Steptoe A. Cortisol awakening response and psychosocial factors: a systematic review and meta-analysis. Biol psychol. 2009;80:265–278. doi: 10.1016/j.biopsycho.2008.10.004. [DOI] [PubMed] [Google Scholar]
- 25.Pruessner JC, Kirschbaum C, Meinlschmid G, Hellhammer DH. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology. 2003;28:916–931. doi: 10.1016/s0306-4530(02)00108-7. [DOI] [PubMed] [Google Scholar]
- 26.Clow A, Hucklebridge F, Stalder T, et al. The cortisol awakening response: more than a measure of HPA axis function. Neuroscience Biobehav Rev. 2010;35:97–103. doi: 10.1016/j.neubiorev.2009.12.011. [DOI] [PubMed] [Google Scholar]
- 27.Hellhammer J, Fries E, Schweisthal OW, et al. Several daily measurements are necessary to reliably assess the cortisol rise after awakening: state-and trait components. Psychoneuroendocrinology. 2007;32:80–86. doi: 10.1016/j.psyneuen.2006.10.005. [DOI] [PubMed] [Google Scholar]
- 28.Kudielka BM, Kirschbaum C. Sex differences in HPA axis responses to stress: a review. Biol Psychol. 2005;69:113–132. doi: 10.1016/j.biopsycho.2004.11.009. [DOI] [PubMed] [Google Scholar]
- 29.Inslicht SS, Otte C, McCaslin SE, et al. Cortisol awakening response prospectively predicts peritraumatic and acute stress reactions in police officers. Biol Psychiatr. 2011;70:1055–1062. doi: 10.1016/j.biopsych.2011.06.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Foa E, Hembree E, Rothbaum BO. Prolonged exposure therapy for PTSD: Emotional processing of traumatic experiences therapist guide. Oxford University Press; 2007. [Google Scholar]
- 31.Brady K, Pearlstein T, Asnis GM, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder. JAMA. 2000;283:1837–1844. doi: 10.1001/jama.283.14.1837. [DOI] [PubMed] [Google Scholar]
- 32.Foa EB, Rothbaum BO, editors. Treating the Trauma of Rape. 9. New York, NY: Guilford Press; 1998. [Google Scholar]
- 33.Marshall RD, Beebe KL, Oldham M, Zaninelli R. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry. 2001;158:1982–1988. doi: 10.1176/appi.ajp.158.12.1982. [DOI] [PubMed] [Google Scholar]
- 34.Foa EB, Riggs DS, Dancu CV, Rothbaum BO. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J Trauma Stress. 1993;6:459–473. [Google Scholar]
- 35.First MB, Gibbon M, Spitzer RL, Williams JBW. Structured Clinical Interview for DSM-IV Personality Disorders, (SCID-II) Washington, D.C: American Psychiatric Press, Inc; 1997. [Google Scholar]
- 36.Regier DA, Narrow WE, Clarke DE, Kraemer HC, Kuramoto SJ, Kuhl EA, Kupfer DJ. DSM-5 field trials in the United States and Canada, part II: test-retest reliability of selected categorical diagnoses. Am J Psychiatry. 2003;170(1):59–70. doi: 10.1176/appi.ajp.2012.12070999. [DOI] [PubMed] [Google Scholar]
- 37.Kraemer HC, Kupfer DJ, Clarke DE, Narrow WE, Regier DA. DSM-5: how reliable is reliable enough? Am J Psychiatry. 2012;169(1):13–15. doi: 10.1176/appi.ajp.2011.11010050. [DOI] [PubMed] [Google Scholar]
- 38.Beck AT, Ward C, Mendelson M. Beck depression inventory (BDI) Arch Gen Psychiatry. 1961;4:561–571. doi: 10.1001/archpsyc.1961.01710120031004. [DOI] [PubMed] [Google Scholar]
- 39.Beck AT, Steer RA, Carbin MG. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin Psychol Rev. 1988;8:77–100. [Google Scholar]
- 40.Dressendorfer RA, Kirschbaum C, Rohede W, et al. Synthesis of a cortisol-biotin conjugate and evaluation as tracer in an immunoassay for salivary cortisol measurement. J Steroid Biochem Mol Biol. 1992;43:683–692. doi: 10.1016/0960-0760(92)90294-s. [DOI] [PubMed] [Google Scholar]
- 41.SPSS Inc. SPSS Statistics Version 21 [Computer software] Chicago, IL: SPSS, Inc; 2012. [Google Scholar]
- 42.Kraemer HC, Wilson GT, Fairburn CG, Agras WS. Mediators and moderators of treatment effects in randomized clinical trials. Arch Gen Psychiatry. 2002;59:877–883. doi: 10.1001/archpsyc.59.10.877. [DOI] [PubMed] [Google Scholar]
- 43.De Kloet CS, Vermetten E, Heijnen CJ, Geuze E, Lentjes EGWM, Westenberg HGM. Enhanced cortisol suppression in response to dexamethasone administration in traumatized veterans with and without posttraumatic stress disorder. Psychoneuroendocrinology. 2007;32(3):215–226. doi: 10.1016/j.psyneuen.2006.12.009. [DOI] [PubMed] [Google Scholar]
- 44.Blain LM, Galovski TE, Robinson T. Gender differences in recovery from posttraumatic stress disorder: A critical review. Aggress Violent Behav. 2010;15(6):463–474. [Google Scholar]
- 45.Carlson LE, Speca M, Patel KD, Goodey E. Mindfulness-based stress reduction in relation to quality of life, mood, symptoms of stress and levels of cortisol, dehydroepiandrosterone sulfate (DHEAS) and melatonin in breast and prostate cancer outpatients. Psychoneuroendocrinology. 2004;29(4):448–474. doi: 10.1016/s0306-4530(03)00054-4. [DOI] [PubMed] [Google Scholar]
- 46.Fries E, Dettenborn L, Kirschbaum C. The cortisol awakening response (CAR): facts and future directions. Int J Psychophysiol. 2009;72:67–73. doi: 10.1016/j.ijpsycho.2008.03.014. [DOI] [PubMed] [Google Scholar]
- 47.Tolin DF, Foa EB. Sex differences in trauma and posttraumatic stress disorder: A quantitative review of 25 years of research. Psychol Bull. 2006;132:959–992. doi: 10.1037/0033-2909.132.6.959. [DOI] [PubMed] [Google Scholar]
- 48.Mills KL, Teesson M, Back SE, Brady KT, Baker AL, Hopwood S, Ewer PL, et al. Integrated exposure-based therapy for co-occurring posttraumatic stress disorder and substance dependence: a randomized controlled trial. JAMA. 2012;308(7):690–699. doi: 10.1001/jama.2012.9071. [DOI] [PubMed] [Google Scholar]
- 49.Rytwinski NK, Scur MD, Feeny NC, Youngstrom EA. The co-occurrence of major depressive disorder among individuals with posttraumatic stress disorder: A meta-analysis. J Trauma Stress. 2013;26(3):299–309. doi: 10.1002/jts.21814. [DOI] [PubMed] [Google Scholar]
- 50.Araújo AX, Berger W, Coutinho ESF, Marques-Portella C, Luz MP, Cabizuca M, Mendlowicz M, et al. Comorbid depressive symptoms in treatment-seeking PTSD outpatients affect multiple domains of quality of life. Compr Psychiatry. 2014;55(1):56–63. doi: 10.1016/j.comppsych.2013.09.004. [DOI] [PubMed] [Google Scholar]
- 51.Gola H, Engler H, Schauer M, Adenauer H, Riether C, Kolassa S, Kolassa IT, et al. Victims of rape show increased cortisol responses to trauma reminders: A study in individuals with war-and torture-related PTSD. Psychoneuroendocrinology. 2012;37(2):213–220. doi: 10.1016/j.psyneuen.2011.06.005. [DOI] [PubMed] [Google Scholar]
- 52.Irish LA, Gabert-Quillen CA, Ciesla JA, Pacella ML, Sledjeski EM, Delahanty DL. An examination of PTSD symptoms as a mediator of the relationship between trauma history characteristics and physical health following a motor vehicle accident. Depress Anxiety. 2013;30(5):475–482. doi: 10.1002/da.22034. [DOI] [PMC free article] [PubMed] [Google Scholar]