

Abstract
Introduction:
Atherosclerosis leading to ischemic heart disease (IHD) is the most common cause of cardiac deaths worldwide. To evaluate the prevalence of atherosclerosis, an autopsy-based study conducted on subjects who died of noncardiac causes can be a valuable tool. With this hypothesis, we conducted this study on the hearts of subjects who died of noncardiac causes.
Materials and Methods:
This study was conducted from August 2012 to February 2013 at Department of Pathology, BJ Medical College, Ahmedabad, Gujarat. The deceased patients who died of noncardiac causes and underwent autopsy at our hospital, their hearts were sent to our department for histopathological analysis. The hearts were fixed in 10% formalin, weighed, measured, and the three main coronary arteries were dissected out and carefully examined for any histological evidence of atherosclerotic plaques and associated pathological lesions and graded according to the classification given by American Heart Association.
Results:
A total of 250 autopsy cases were evaluated. Amongst them 113 were deaths due to noncardiac causes, of which 83 (73.45%) subjects had evidence of atherosclerosis. In the study, 68 (82%) were males and 15 (18%) were females. Left anterior descending artery (LADA; 69%) was the most commonly involved coronary artery. Triple vessel disease was found in 22% of subjects.
Conclusion:
The study showed alarmingly high prevalence of atherosclerosis. The pathogenesis of coronary atherosclerosis begins at a younger age in Indian population. Though the incidence of atherosclerosis is more common in males compared to females; coronary atherosclerosis is an important risk factor for IHDs in both sexes and screening for the same should begin at an early age.
Keywords: Atherosclerosis, autopsy, coronary vessels, left anterior descending artery, triple vessel disease
INTRODUCTION
Coronary artery disease due to atherosclerosis has emerged as a major social epidemic in India. The incidence of coronary artery disease has touched alarming proportions. It has almost doubled during past 3-4 decades. It will soon emerge as the single largest disease accounting for nearly one-third of all deaths in India. According to estimates, about 6.4 crore cases of coronary vascular disease are likely in the year 2015. About 1.3 million Indians died from this in 2000. It is projected that by the year 2015, coronary artery disease would cause around 2.95 million deaths, of which 14% of the mortality will be in population under 30 years of age and 31% deaths will occur in subjects below the age of 40 years.[1]
Atherosclerosis is a chronic degenerative condition of arteries responsible for significant cardiovascular morbidity and mortality worldwide. In the Indian subcontinent, it is reported to be responsible for more than 25% of deaths.[2] Atherosclerotic lesions start developing at an earlier age and are found to be in more advanced stages in Indian population as compared to the patients in western countries. Atherosclerosis can lead to various complications like myocardial infarction (MI), stroke, embolization, ulceration, thrombosis, and aneurysm which cause considerable morbidity and mortality, thus affecting the lifespan and the quality of life of a large segment of population.
Assessment of atherosclerotic lesions in living subjects is difficult and almost nonexistent due to its invasive nature and can be an expensive enterprise. Hence, autopsy-based study of coronary vessels and aorta, has emerged as an invaluable tool for studying these atherosclerotic lesions in deceased subjects. It will be a true representation of distribution and prevalence of atherosclerotic lesions present in the population if an autopsy study is conducted on deceased patients without any prior history of coronary artery disease and who expired due to noncardiac causes (as compared to the deaths caused by cardiac causes). With this hypothesis we conducted this study in 113 noncardiac death patients. The age group ranged from 6 to 89 years.
MATERIALS AND METHODS
This study was conducted from August 2012 to February 2013 at Department of Pathology, BJ Medical College, Ahmedabad, Gujarat. The deceased patients who underwent autopsy at our hospital and their prior/past medical history were recorded and their hearts were sent to our department for histopathological analysis. Written informed consent was taken from the relative/guardian of the deceased patient. The study was ethically approved by the institute's ethical committee.
The hearts of 250 successive autopsies were received in the department. Amongst these 113 deceased individuals had no prior history of cardiac disease, that is, deaths due to noncardiac causes. The hearts were dissected following standard autopsy protocol. The hearts were fixed in 10% formalin, weighed, measured, and the three main coronary arteries were dissected out. A 5 cm section of the right coronary artery (RCA) in the atrioventricular groove from its origin, a 5 cm segment of the left anterior descending artery (LADA) distal to the origin of the circumflex artery, but including the region of origin of the circumflex branch and left coronary artery (LCA) from its origin till the circumflex branch were excised and dissected out. Each coronary artery was then sectioned longitudinally with a scalpel. The exposed artery was carefully examined for any thickening, yellow streaks, frank plaque, or calcification. Multiple sections were taken from areas thus found and proper identification number was given. After routine processing and paraffin embedding, 4 μm sections were taken and stained with hematoxylin and eosin (H and E). All the histological sections were examined microscopically for the presence of atheroma and MI. American Heart Association typing of atherosclerotic plaque was done.
Grade 0
Sections showing normal histology or adaptive thickening without macrophages or foam cells.
Grade 1
Presence of isolated macrophages and foam cells.
Grade 2
Mainly intracellular lipid accumulation.
Grade 3
Grade 2 lesions along with small extracellular lipid pools.
Grade 4
Grade 2 changes along with a core of extracellular lipid.
Grade 5
Lipid core and fibrotic layer or multiple lipid cores and fibrotic lipid layers; mainly calcific or fibrotic.
Grade 6
Surface defect, hematoma, hemorrhages, or thrombus formation.
The degree of atherosclerosis was classified as unremarkable (Grade 0), mild (Grade 1-2), moderate (Grade 3-4), and severe (Grade 5-6).
RESULTS
During the study period from August 2012 to February 2013;250 consecutive autopsied hearts were submitted to the Department of Pathology, of which 113 deceased subjects had no prior history of coronary vessel disease and had a history of noncardiac cause of death. The age group ranged from 6 to 89 years. Out of these 113 subjects, 83 (73.45%) subjects had some histopathological evidence of coronary atherosclerosis. Amongst the 83 subjects with atherosclerosis, 68 (82%) were males and 15 (18%) were females [Table 1]. The average heart weight for all 113 noncardiac death subjects in males and females was found to be 276.19 and 235.2 g, respectively. The average heart weight of 83 subjects found to have evidence of atherosclerosis in males and females was found to be 287.21 and 246 g, respectively.
Table 1.
Age and sex distribution of atherosclerosis cases
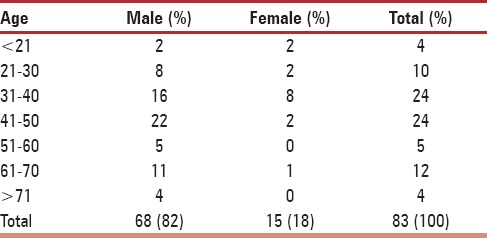
All the subjects were grouped into specific age groups based on the age at the time of death. The age and sex distribution of all 83 cases showing evidence of atherosclerosis are given in Table 1. The involvement of individual coronary arteries and severity of involvement is shown in Table 2.
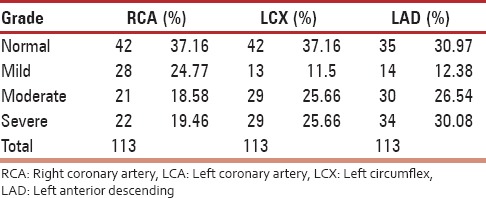
Table 2.
Degree/severity of atherosclerosis in the coronary vessels
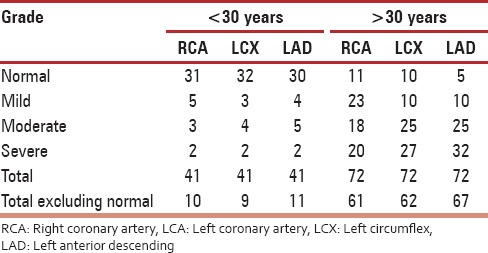
The 3rd decade of life appears to be a watershed line in the pathogenesis of coronary vascular atherosclerosis, as we observed a steady increase in overall frequency, the number of coronary vessels involved, and severity of atherosclerosis from the 3rd decade onwards [Table 3].
Table 3.
Frequency and severity/degree of atherosclerosis in different coronary vessels before and after 3rd decade of life
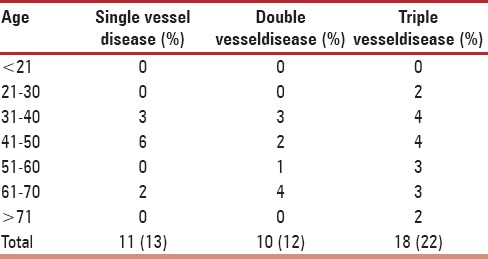
Amongst the 83 cases, all the three coronary arteries were severely involved (triple vessel disease) in 18 cases (22%). Double vessel and single vessel disease were seen in 10 (12%) and 11 (13%) cases, respectively [Table 4].
Table 4.
Correlation of age with number of coronary vessels involved
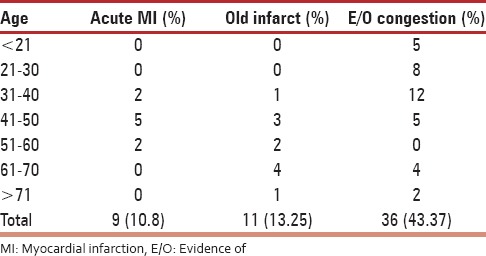
Evidence of acute MI was found in nine (10.8%) cases, old healed scars were found in 11 (13.25%) cases, and evidence of congestion was found in 36 (43.37%) cases [Table 5].
Table 5.
Associated histopathological findings
DISCUSSION
Morbidity and mortality due to coronary atherosclerosis in India has reached alarming proportions and these numbers are expected to maintain the upward trend in the next decade. Atherosclerosis is a commonly observed pathological finding in almost all ethnicities and societies worldwide, but with variable prevalence in different races. The onset of atherosclerosis starts early in life from childhood and gradually progresses through young adulthood to form the lesions that causes coronary heart disease later in life.
In the present study, the overall incidence of atherosclerosis was found to be 73.45%, which is higher than what has been found in earlier studies by Dhruva et al., (23.3%);[3] Golshahi et al., (28.9%);[4] Garg et al., (46.4%);[5] and Yazdi et al., (40%).[6]
Ischemic heart disease (IHD) due to coronary vascular disease is mainly caused due to atherosclerosis. The Indian population is otherwise also vulnerable to coronary vascular disease and the disease also has an earlier onset in our population. In our study we found that there is a progressive steady increase in atherosclerosis of coronary vessels in individuals from the 3rd decade of life onwards. Our findings corroborates well with findings of earlier studies in India. Yazdi et al.,[6] Wig et al.,[7] and Singh et al.,[8] found that significant atherosclerotic lesions start developing from 2nd decade of life and onwards. Tandon et al.,[9] also reported that there was a progressive increase in the number and severity of atherosclerotic lesions from the 2nd and 3rd decade of life onwards. Dhruva et al.,[3] also reported similar findings with increasing frequency of atherosclerosis from 3rd decade onwards and with a peak of 76.6% in 6th decade, followed by a decline to 66.7% in the 8th decade. Garg et al.,[5] also noted a progressive increase in atherosclerotic lesions from 3rd decade onwards. In this modern globalized era, where human life style has become more and more complex and challenging. Various life stressors (anxiety, depression, etc.) along with a sedentary lifestyle and lack of exercise and poor dietary habits like intake of junk food and increased use of refined and processed food items in place of whole grains and fresh fruits and vegetables can be important factors for earlier initiation of development and progressive increase in atherosclerotic lesions in this young Indian population.
Males have a relative preponderance of coronary heart disease as is evident from multitude of national and international studies conducted in the past. In the study conducted by Garg et al.,[5] they found coronary atherosclerotic lesions in 80.9% (93) males as compared to 19.1% (22) females. Bhargava and Bhargava[10] reported coronary atherosclerotic lesions were more prevalent in 74.8% males in comparison to 24.2% females in their study. Murthy et al.,[11] studied 150 cases of coronary atherosclerotic lesions, out of which 123 (82%) were males and 27(18%) were females. Singh et al.,[8] also reported coronary atherosclerotic lesions in 200 cases and found that these lesions were more frequently found in 85% males as compared to 15% in females. Padmavati and Sandhu[12] found that 66.5% males and 33.5% females were affected by coronary atherosclerotic lesions. In the present study too, we found a male (82%) preponderance of coronary atherosclerosis as compared to 18% in females. The findings of our study corroborates well with the findings of previous studies. There may be a protective role of female hormones like estrogen against atherosclerosis. Moreover, there is greater indulgence of males in smoking and alcoholism as compared to females, which may possibly explain the male preponderance towards development of more severe and progressive atherosclerosis.
In the 83 individuals with coronary atherosclerosis, the average weight of the heart was greater as compared to nonatherosclerotic cases. This may be due to increased cardiac work load and compensatory hypertrophy. As atherosclerosis was found to be more in frequency and degree of severity in males as compared to females, it was also evident as the average hearts of males were heavier than those of age group-matched female patients. Our findings are comparable to the similar findings of Dhruva et al.,[3] and Garg et al.,[5] who too found that the average heart weight in males was higher as compared to females.
Triple, double, and single vessel disease was found in 22, 12, and 13% of cases, respectively, with severe atherosclerotic lesions in our study. Dhruva et al.,[3] found that single vessel was involved in 31%, while two and three vessel involvements was seen in 17 and 36% cases, respectively. In their study, Garg et al.,[5] reported that triple vessel involvement (44.4%) was the most common, followed by double and single vessel involvement seen in 42.2 and 13.3% cases, respectively.
Incidence of coronary involvement in LADA was 40%, RCA 32%, and left circumflex artery 30%. This was in concordance with the data given by Sudha et al.,[13] who showed LADA as the most common site for plaque (47%) and Yazdi et al.,[6] who showed LAD as the most commonly involved artery (60%), followed by RCA (50%) and left circumflex artery (42.5%). Garg et al.,[5] too found that LADA (38.1%) was the commonest involved vessel followed by right coronary (35.1%) and left circumflex artery (34%).
Acute MI was seen in 10.8% cases as compared to observations of 9.72, 6.5, and 3% acute MI cases observed by Dhruva et al.,[3] Maru,[14] and Garg et al.,[5] respectively. It is a bit surprising and unexpected finding that the percentage of acute MI in our study was slightly on the higher side as our subjects did not have any prior history of a coronary vascular event or history of cardiac cause of death.
CONCLUSION
The study showed unexpectedly high prevalence of atherosclerosis in Ahmedabad, India; especially in the relatively young population with no prior history of cardiovascular disease and where the diagnosis of coronary vascular disease is least suspected. However, there is a male preponderance of coronary atherosclerosis, but there is a progressive increase in the proportion of females who present with coronary atherosclerosis. The study of human atherosclerotic lesion is an extremely difficult task in a living subject and autopsy study is the best possible way to work on it. Though our study involved only a small number of cases, it highlights the early onset and increasing prevalence and severity of atherosclerotic lesions in Indian population. It also calls for institution of screening programs and preventive and control measures against atherosclerosis from an early age.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Indrayan A. Forecasting vascular disease cases and associated mortality in India. NCMH Background Papers: Burden of Disease in India. National Commission on Macroeconomics and Health, Government of India. 2005:197–215. [Google Scholar]
- 2.Gupta R, Joshi P, Mohan V, Reddy KS, Yusuf S. Epidemiology and causation of coronary heart disease and stroke in India. Heart. 2008;94:16–26. doi: 10.1136/hrt.2007.132951. [DOI] [PubMed] [Google Scholar]
- 3.Dhruva GA, Agravat AH, Sanghvi HK. Atherosclerosis of coronary arteries as predisposing factor in myocardial infarction: An autopsy study. [Last accessed on 2013 Dec 13];Online J Health Allied Scs. 2012 11:1. Available from: http://www.ojhas.org/issue43/2012-3-1.htm . [Google Scholar]
- 4.Golshahi J, Rojabi P, Golshahi F. Frequency of atherosclerotic lesions in coronary arteries of autopsy specimens in Isfahan forensic medicine center. J Res Med. 2005;1:16–9. [Google Scholar]
- 5.Garg M, Agarwal AD, Kataria SP. Coronary atherosclerosis and myocardial infarction: An autopsy study. [Last accessed on 2013 Dec 13];J Indian Acad Forensic Med. 2011 33:39–42. Available from: http://medind.nic.in/jal/t11/i1/jalt11i1p39.pdf . [Google Scholar]
- 6.Yazdi SA, Rezaei A, Azari JB, Hejazi A, Shakeri MT, Shahri MK. Prevalence of atherosclerotic plaques in autopsy cases with noncardiac death. Iran J Pathol. 2009;4:101–4. [Google Scholar]
- 7.Wig KL, Malhotra RP, Chitkara NL, Gupta SP. Prevalence of coronary atherosclerosis in northern India. Br Med J. 1962;1:510–3. doi: 10.1136/bmj.1.5277.510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Singh H, Oberoi SS, Gorea RK, Bal MS. Atherosclerosis in coronaries in malwa region of Punjab. J Indian Acad Forensic Med. 2005;27:32–5. [Google Scholar]
- 9.Tandon OP, Aggarwal VC, Katiyar BC. Coronary and aortic atherosclerosis (A study on 300 medicolegal postmortems) Indian Heart J. 1969;21:5–10. [PubMed] [Google Scholar]
- 10.Bhargava MK, Bhargava SK. Coronary atherosclerosis in North Karnataka. Indian J Pathol Microbiol. 1975;18:65–79. [PubMed] [Google Scholar]
- 11.Murthy MS, Dutta BN, Ramalingaswami V. Coronary atherosclerosis in North India (Delhi Area) J Pathol Bacteriol. 1963;85:93–101. doi: 10.1002/path.1700850109. [DOI] [PubMed] [Google Scholar]
- 12.Padmavati S, Sandhu I. Incidence of coronary artery disease in Delhi from medico-legal autopsies. Indian J Med Res. 1969;57:465–76. [PubMed] [Google Scholar]
- 13.Sudha ML, Sundaram S, Purushothaman KR, Kumar PS, Prathiba D. Coronary atherosclerosis in sudden cardiac death: An autopsy study. Indian J Pathol Microbiol. 2009;52:486–9. doi: 10.4103/0377-4929.56130. [DOI] [PubMed] [Google Scholar]
- 14.Maru M. Coronary atherosclerosis and myocardial infarction in autopsied patients in Gondar, Ethiopia. J R Soc Med. 1989;82:399–401. doi: 10.1177/014107688908200710. [DOI] [PMC free article] [PubMed] [Google Scholar]