

Abstract
Objective
The purpose of the present study was to examine gender differences in the frequency of high-risk drinking situations and to investigate the extent to which depressive symptoms mediate the relationship.
Method
Participants were 143 outpatient alcohol treatment seekers. Each participant completed the Beck Depression Inventory-II and Inventory of Drug-Taking Situations (IDTS) at baseline prior to treatment.
Results
Multivariate analysis of variance was used to examine gender differences in drinking across eight categories of situations assessed on the IDTS. Mediational analyses tested whether gender differences on these IDTS subscales may be mediated by depressive symptoms. We found support for the hypothesis that women report drinking more than men in response to unpleasant emotions and conflict with others, and that these associations are significantly mediated by depression severity.
Conclusions
The current findings have important implications for appropriate treatment for alcohol-dependent women. In particular, such treatment should include training in affect regulation and interpersonal skills, as well as treatment for depression, when appropriate.
Keywords: Alcohol, depression, high-risk, gender, relapse
1. Introduction
A core feature of cognitive-behavioral approaches to treating alcohol dependence is the identification of specific high-risk situations associated with drinking. Specifically, in models of relapse prevention treatment, understanding common antecedents to use or high-risk situations for using is critical in preventing relapses (Marlatt & Gordon, 1985). Marlatt and Gordon (1980) developed an eight-category taxonomy of high-risk situations that may trigger relapse derived from interviews with alcohol treatment patients. These determinants include: negative emotional states, negative physical states, positive emotional states, testing personal control, urges and temptations, interpersonal conflict, social pressures, and positive emotional states in interpersonal situations. According to this model, a primary goal of treatment is to teach patients to effectively anticipate and cope with the high-risk situations as to prevent relapse episodes (Marlatt & Gordon, 1985; Irvin, Bowers, Dunn, & Wang, 1999).
Some studies examining high-risk situations for heavy drinking have revealed gender differences. Building on the work of Marlatt & Gordon, Annis (1982) developed the Inventory of Drinking Situations (IDS) to assess situational antecedents to heavy drinking. The subscales of the IDS reflect Marlatt and Gordon’s taxonomy of heavy drinking situations. Annis et al. (1987) found that in a sample of alcohol-dependent treatment seekers, men reported drinking heavily more often than women in response to pleasant emotions, pleasant times with others, and social pressure to drink (Annis, Graham, & Davis, 1987). Women, however, reported drinking heavily more frequently when experiencing unpleasant emotions. Another study examined four different profiles of precipitants of alcohol use as assessed with the IDS. Findings revealed that alcohol-dependent individuals with a negative profile, as compared to those with a positive profile, were more likely to be women and exhibit heavy drinking in response to negative emotions and conflict with others (Annis & Graham, 1995). Other researchers specifically examining precipitants of relapse episodes have also discovered gender differences. Women have been found to be more likely to drink in response to negative emotional states and interpersonal influences (Connors, Maisto, & Zywiak, 1998; Olenick & Chalmers, 1991; Zywiak et al., 2006). Men, on the contrary, are more likely to relapse as a result of positive affect (Connors et al., 1998) and social pressure (Zywiak, Stout, Trefry, et al.., 2006; Zywiak, Stout, Longabaugh, et al., 2006).
Notwithstanding, other studies have found no differences between men and women on high-risk drinking situations. For example, Rubin et al. (1996) found no gender differences across the eight categories of Marlatt’s taxonomy in the situation preceding the most recent relapse, or in frequency of drinking across the categories of the IDS. It is possible that comparability of drinking patterns in the immediate relapse episode (e.g., amount consumed, hours of drinking) and the slightly more impaired users in this sample may partially account for the lack of gender difference in the study. In another study, alcohol-dependent men and women did not significantly differ in the nature of the relapse situation following treatment across the eight categories (Annis, Sklar, & Moser, 1998). However, there was a trend in which women were at greater risk for relapse in situations involving negative emotional states, whereas men were more likely to relapse due to social pressure to use. Thus, while research on high-risk situations for alcohol use provides some support for differences between men and women, inconsistencies in the literature remain. Additional research is warranted to further clarify the situations under which each gender is most likely to engage in heavy alcohol consumption and the underlying factors that may account for these differences.
In addition to the research examining gender differences in drinking in risky situations, gender differences have also been examined in the prevalence of depressive disorders and in the association between depression and alcohol use disorders. Compared to men, women are twice as likely as men to be diagnosed with any affective disorder (Brady, Grice, Dustan, & Randall, 1993) and have a higher estimated lifetime occurrence of major depression (Hasin, Goodwin, Stinson, & Grant, 2005; Kessler, Zhao, Blazer, & Swartz, 1997). The risk of alcohol abuse is greater among women with major depression than men with major depression (Grant & Harford, 1995). Further, women with alcohol dependence present with greater depressive symptomology before treatment than men with alcohol dependence (Glenn & Parsons, 1991; Pettinati, Pierce, Wolf, Rukstalis, & O’Brien, 1997). Overall, these findings suggest that negative affect, and specifically depression, may be a stronger contributor to women’s alcohol use than men’s. Then, it is possible that depressive symptoms may be one mechanism through which gender differences in high-risk drinking situations occur.
The present research had two primary objectives. First, we sought to address mixed findings in previous studies regarding gender differences in the frequency of heavy drinking in various high-risk situations. Second, we offer one explanation that may account for the observed gender difference on risky situations by testing the extent to which depressive symptoms mediate the relationship between gender and drinking in high-risk situations. It was hypothesized that men and women will differ in high-risk situations for heavy drinking. Specifically, it was expected that women will report heavy drinking more frequently in response to situations involving negative affect or unpleasant emotions and interpersonal conflict, whereas men will report heavy drinking more frequently in response to pleasant emotions, social pressure, and pleasant times with others. Furthermore, it was expected that any associations between gender and high-risk drinking situations are mediated by depressive symptomatology.
2. Materials and methods
2.1. Participants and procedure
The sample was 143 (91 men) outpatient treatment-seekers meeting DSM-IV diagnostic criteria for alcohol dependence. Participants completed questionnaires for the present study as part of a comprehensive substance use assessment battery prior to behavioral treatment for substance use. The mean age of the sample was 38.93 years (SD = 10.71). Participants were predominately White (75.5%), but ethnic minorities were represented (19.6% African American, 3.5% Hispanic, 0.7% Asian, and 0.7% Native American). Participants included those who were single (45.5%), married (28%), divorced or separated (21.7%), and cohabitating (4.2%). Most participants were employed either full-time (41.3%) or part-time (15.4%), but unemployed (33.6%) and disabled or retired participants were also represented (8.4%). Participants reported consuming an average of 7.5 (SD = 5.19) drinks per drinking day. (a drink was defined as 12 ounces of beer, 5 ounces of wine, or 1.5 ounces of spirits). Sixty-five percent of the sample reported prior treatment for alcohol problems. Participants consented to have their data used for research purposes, and the study was approved by the Institutional Review Board at the University at Buffalo.
2.2. Measures
2.2.1. Beck Depression Inventory, 2nd Edition (BDI-II; Beck, Steer, & Brown, 1996)
The BDI-II, a 21-item self-report measure, assesses the severity of depressive symptoms during the past 2 weeks. Items are rated from 0 to 3 (range = 0–63). Responses are summed to derive a total score, with higher scores indicating greater severity. The BDI-II has excellent psychometric properties and is internally consistent (α = .88).
2.2.2. Inventory of Drug-Taking Situations (IDTS; Annis & Martin, 1985)
The IDTS, a 50-item self-report instrument, assesses a client’s substance use across eight categories of situations. The IDTS has two versions, one for illicit drugs and one for alcohol. The alcohol version was used in this study. The measure provides eight subscale scores, corresponding to eight categories of high-risk situations: Unpleasant Emotions, Physical Discomfort, Pleasant Emotions, Testing Personal Control, Urges and Temptations to Use, Conflict with Others, Social Pressure to Use, and Pleasant Times with Others. Participants are presented with high-risk situations and are instructed to indicate how frequently they drink heavily in each situation. The definition of heavy consumption was based on the discretion of the participant. Responses range from 1 (“never”) to 4 (“almost always”), with higher scores indicating greater frequency of drinking in that situation (range = 50–200). The IDTS has been validated for use in alcohol-dependent populations and has excellent internal consistency (α = .96).
2.2.3. Timeline Follow-back (TLFB; Sobell & Sobell, 1992)
The TLFB is a calendar-based method of estimating the number of standard drinks one has consumed in a given time period. The TLFB has been extensively evaluated, has good psychometric properties, and is considered a gold standard for assessing changes in alcohol consumption (Sobell & Sobell, 1992). The TLFB variable of interest for the purpose of this study was the mean number of standard drinks the participants consumed per drinking day.
3. Results
3.1. Participant characteristics by gender
A comparison of participant characteristics by gender is shown in Table 1. Findings revealed that alcohol-dependent women scored significantly higher than men on the BDI-II, t(79) = −2.32, p < .05, supporting previous research asserting that women experience more depressive symptoms than men. Alcohol-dependent men were more likely to have a history of prior treatment for alcohol problems, χ2 (1) = 4.50, p < .05. No statistically significant gender differences were found in age, employment, ethnicity, martial status, or average number of drinks per drinking day.
Table 1.
Participant Characteristics by Gender
| Variable | Men (n = 91) | Women (n = 52) |
|---|---|---|
| Age | 38.90 (10.94) | 38.98 (10.39) |
| Employed (%) | 59.3 | 52.9 |
| Ethnicity (%, Caucasian) | 73.6 | 78.8 |
| Marital Status (%, married/cohabitating) | 35.2 | 26.9 |
| Prior alcohol treatment (%)* | 71.4 | 53.8 |
| Weekly alcohol use (standard drinks) | 21.30 (19.73) | 15.90 (13.87) |
| Average # of drinks per drinking day | 7.56 (5.04) | 7.29 (5.54) |
| BDI-II scores* | 12.11 (7.80) | 16.21 (11.33) |
p < .05
3.2. Multivariate analysis of variance
Multivariate analysis of variance (MANOVA) was conducted to examine gender differences in heavy drinking situations across the eight subscales of the IDTS (see Table 2). Results revealed significant differences between men and women on some subscales of the IDTS, F(8, 134) = 4.15, p < .001. Univariate F tests yielded significant differences for two of the eight IDTS subscales. As shown in Table 2, relative to men, women reported a higher frequency of heavy drinking in response to Unpleasant Emotions, F(1,141) = 6.95, p < .01, and Conflict with Others, F(1,141) = 4.32, p < .05. There were no gender differences in drinking heavily in response to positive affect or social pressure. Because of the multivariate results, only the subscales of the IDTS that demonstrated gender differences were subjected to the mediational analyses described below.
Table 2.
Means, Standard Deviations, and Univariate Analyses of Variance for IDTS Subscales
| Variable | Men
|
Women
|
Univariate
|
||
|---|---|---|---|---|---|
| M | SD | M | SD | F(1,141) | |
| Unpleasant Emotions | 49.89 | 22.94 | 60.58 | 23.99 | 6.95** |
| Conflict with Others | 35.46 | 23.09 | 43.91 | 23.91 | 4.32* |
| Physical Discomfort | 21.10 | 18.76 | 25.13 | 22.74 | 1.31 |
| Pleasant Emotions | 42.93 | 23.77 | 42.18 | 26.16 | 0.03 |
| Testing Personal Control | 30.70 | 22.62 | 22.59 | 26.82 | 0.47 |
| Urges/Temptations | 41.47 | 21.31 | 34.74 | 19.99 | 3.44 |
| Social Pressure to Use | 46.01 | 25.99 | 41.15 | 26.33 | 1.14 |
| Pleasant Times with Others | 52.82 | 25.22 | 44.23 | 28.53 | 3.49 |
p < .05,
p < .01.
3.3. Mediational analysis
Hierarchical multiple regression analyses were performed to examine whether the gender differences found on the IDTS subscales are mediated by depressive symptoms as measured by the BDI-II. Mediation was determined using the guidelines set forth by Baron and Kenny (1986). Evidence of mediation is present if the following conditions are met: (a) there is a significant predictor to outcome association (path c in Figs. 1 and 2); (b) there is a significant predictor to mediator association (path a in Figs. 1 and 2); (c) there is a significant mediator to outcome association (path b in Figs. 1 and 2); and (d) there is a reduction in the predictor to outcome relationship after controlling for the mediator (path c’ in Figs. 1 and 2). The significance of the indirect effect was tested using the Sobel (1982) test. In the present study, we tested the mediating effect of depressive symptoms on the relationship between gender and the Unpleasant Emotions subscale, and then between gender and Conflict with Others subscale. Depression severity would be considered a mediator if it accounted for all or some of the relationship between gender and Unpleasant Emotions or Conflict with Others. The present sample of 143 is sufficient to detect medium size mediational effects with .8 statistical power in single-mediator models using indirect effects test (i.e., Sobel test; Fritz and MacKinnon, 2007). Table 3 displays Pearson’s product moment correlations for the variables under study.
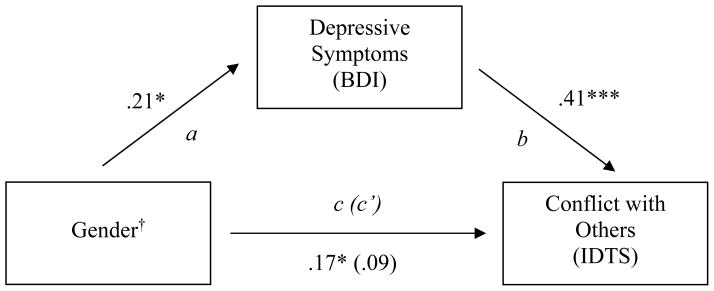
Figure 1.
Depressive symptoms as a mediating variable between gender and drinking in response to Conflict with Others. Values on paths are standardized β’s. †1 = men; 2 = women. *p < .05, ** p < .01, *** p < .001.
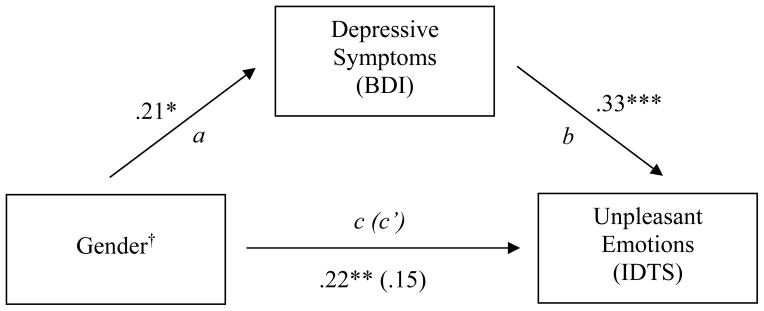
Figure 2.
Depressive symptoms as a mediating variable between gender and drinking in response to Unpleasant Emotions. Values on paths are standardized β’s. †1 = men; 2 = women. *p < .05, ** p < .01, *** p < .001.
Table 3.
Variable Correlations
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 Sex | -- | |||||||||
| 2. BDI | .21* | -- | ||||||||
| 3. IDTS - Conflict with Others | .17* | .43** | -- | |||||||
| 4. IDTS - Unpleasant Emotions | .22** | .37** | .79** | -- | ||||||
| 5. IDTS - Physical Discomfort | .10 | .24** | .65** | .63** | -- | |||||
| 6. IDTS - Pleasant Emotions | −.02 | .17* | .48** | .43** | .48** | -- | ||||
| 7. IDTS - Testing Personal Control | .06 | .15 | .52** | .49** | .52** | .50** | -- | |||
| 8. IDTS - Temptation to Use | −.15 | .16 | .56** | .56** | .52** | .55** | .61** | -- | ||
| 9. IDTS - Social Pressure to Use | −.09 | .13 | .50** | .39** | .37** | .44** | .53** | .64** | -- | |
| 10. IDTS - Pleasant Times with Others | −.16 | .17* | .50** | .42** | .33** | .60** | .46** | .65** | .80** | -- |
Note. Sex (1=male, 2=female);
p<.05,
p<.01
3.3.1. BDI-II mediating gender and Unpleasant Emotions subscale
Results showed that gender was significantly associated with scores on the Unpleasant Emotions subscale (see Figure 1; β = .22, p < .01) and was significantly positively associated with the BDI-II scores (β = .21, p < .05). BDI-II scores were, in turn, significantly positively associated with the Unpleasant Emotions subscale (β = .33, p < .001). The previously significant relationship between gender and Unpleasant Emotions was not significant after BDI-II scores were controlled (β = .15, p = ns). The test of the indirect effect revealed that BDI-II scores served as a significant mediating variable between gender and Unpleasant Emotions (z = 2.24, p < .05). Fifty-four percent of the variance was accounted for by mediation.
3.3.2. BDI-II mediating gender and Conflict with Others subscale
Analyses revealed a significant relationship between gender and Conflict with Others subscale scores (see Figure 2; β = .17, p < .05). Gender was significantly positively associated with the Conflict with Others subscale and with BDI-II scores (β = .21, p < .05). BDI-II scores were significantly positively associated with the Conflict with Others subscale (β = .41, p < .001). The previously significant relationship between gender and Conflict with Others was nonsignificant after controlling for BDI-II scores (β = .09, p = ns). The Sobel (1982) test revealed that BDI-II scores significantly mediated the relationship between gender and the Conflict with Others subscale (z = 2.32, p < .05). Sixty-two percent of the variance was accounted for by mediation.
4. Discussion
The present study found differences between alcohol-dependent men and women in high-risk situations for heavy drinking. Multivariate analysis showed that women were more likely than men to engage in heavy drinking when experiencing Unpleasant Emotions and Conflict with Others. These findings are consistent with the body of literature supporting a gender difference in high-risk drinking situations and relapse precipitants, whereby showing that women are more likely to drink in response to negative emotional states and interpersonal influences (e.g., Annis et al., 1987; Annis & Graham, 1995; Connors et al., 1998). With respect to men, we predicted a greater frequency of drinking in response to Pleasant Emotions, Social Pressure, and Pleasant Times with Others. Our findings did not support this hypothesis. Although men did have higher mean scores than women on the Social Pressure and Pleasant Times with Others subscales, these differences were not significant. One possibility that may partially account for the lack of support could be related to the measure of drinking situations. Previous gender differences noted in heavy drinking situations utilized the 100-item IDS (Annis et al., 1987; Annis & Graham, 1995), which is the predecessor to the 50-item IDTS. It is possible that the differences between these measures may have contributed to the null findings with men in our study. Future work may focus on the consistency of these findings in other studies and across different samples.
Mediational analyses demonstrated that depressive symptoms as measured by the BDI-II served as a significant intervening variable between gender and alcohol consumption in particular high-risk drinking situations. Specifically, the relationships between gender and drinking in response to Unpleasant Emotions and in response to Conflict with Others were explained by depressive symptoms. These results suggest that greater endorsement by women of drinking heavily when experiencing negative affect and interpersonal conflict may be explained by the level of depressive symptoms they reported. Our findings are consistent with the existing literature on women and alcohol use in showing a stronger association between drinking and depressive symptoms for women as compared with men. This relationship emerged despite the fact that the women in our sample scored within the “minimal” range of depressive severity on the BDI-II.
The current findings could have important implications for the treatment of women with alcohol dependence. If the high-risk situations for heavy drinking as assessed by the IDTS are believed to reflect relapse precipitants, then gender differences found in this study warrant attention in treatment with women. Relapse prevention-based treatment programs may specifically address unpleasant emotions and conflict with others as salient triggers to alcohol use and to help clients learn to anticipate and effectively cope with these situations without drinking. In addition, treatment programs for alcohol dependent women should integrate components to target potential deficits in these particular domains. For example, programs may emphasize interpersonal or social skills training to help clients enhance personal relationships (O’Leary & Monti, 2002). By gaining training in domains such as basic communication skills and conflict resolution skills, clients may be better able to manage problematic social interactions, and thereby lessen the occurrence of interpersonal conflict as a precipitant for heavy drinking.
Another implication that our findings suggest is the importance of assessing and treating depressive symptoms in alcohol-dependent women. Our sample of women presented with significantly higher BDI-II scores than men at baseline for outpatient treatment. Additionally, depressive symptoms significantly explained gender differences in high-risk drinking situations. These findings, combined with the literature indicating a higher prevalence of mood disorders in women and that depression may contribute to a more rapid progression of substance use (Grant & Harford, 1995; Brown, Inaba, Gillin, Schuckit, Stewart, & Irwin, 1995), point to the importance of attending to affective issues in alcohol-dependent women seeking treatment.
One approach to address drinking in response to unpleasant emotions is to incorporate treatment content that focuses on associations between negative emotional states and substance use. One goal of such an approach would be to improve the client’s ability to regulate negative emotional states without the use of alcohol and/or other drugs of abuse (e.g., Bradizza & Stasiewicz, in press). This, and other innovative treatment modalities, have the potential to improve the effectiveness of treatment programs for alcohol abusing men and women, but may be especially useful for women given the current findings. In addition, pharmacological treatment, such as antidepressant medications, may be warranted for patients presenting with co-morbid depression and alcohol dependence (Torrens, Fonseca, Mateu, & Farre, 2005). The use of other pharmacological treatments for alcohol dependence (i.e., naltrexone) also has shown benefit when used in conjunction with psychosocial treatment (Anton et al., 2005; Anton, Moak, Waid, Latham, Malcolm, & Dias, 1999).
Despite the potential contribution of the present study, there are several limitations that should be addressed. The higher level of depressive symptoms observed in the present study among women may reflect differential responding or a self-report bias. Research has shown that women are more willing than men to self-report affective symptoms (Sigmon et al., 2005; Kessler, 2000). However, evidence does support a higher prevalence of depression in women (Hasin et al., 2005) even when using informant reports (Kendler, Davis, & Kessler, 1997), suggesting that self-report bias cannot account entirely for the gender difference observed. Another limitation involves generalizing the present findings to individuals meeting diagnostic criteria for a mood disorder as opposed to those endorsing depressive symptoms measured on the BDI-II. In addition, the participants in this study met DSM-IV criteria for alcohol dependence, and were seeking treatment. These results may not generalize to problem drinkers who are not-seeking treatment, or to individuals who are mandated to treatment by the legal system. With regard to the latter, the majority of individuals arrested for driving under the influence do not meet diagnostic criteria for a current alcohol use disorder as determined by a structured clinical interview (Lapham, Smith, C’de Baca et al., 2001; Stasiewicz, Nochajski, & Homish, 2007). Therefore, when mandated to an alcohol treatment program, these individuals may remain unconvinced about the necessity of formal treatment.
Another limitation of the present study is the use of a cross-sectional design that limits inferences of causality or direction of effect. Instead of a model in which depressive symptoms result in drinking to Unpleasant Emotions and Conflict with Others, it may be that drinking in response to Unpleasant Emotions and Conflict with Others results in greater depressive symptomatology. It is possible that other models could fit the data equally well as the mediational model posited currently. However, our model is empirically grounded and supported by previous research findings in the areas of alcohol use, affect, and risky drinking situations. To fully understand the casual precedence of the current study variables, however, it would be beneficial to replicate this study using a longitudinal design. Furthermore, a future study may evaluate prospectively the extent to which the situations of heavy drinking as reported on the IDTS are consistent with specific precipitators of relapses (Zywiak, Stout, Longabaugh, Dyck, Connors, & Maisto, 2006).
The present study contributes to the literature by demonstrating differences between men and women in heavy drinking situations and sheds light on an underlying factor that may explain these differences. We found support for depressive symptoms serving as a mediator of the relationship between gender and drinking in response to negative emotions and interpersonal conflict. In general, the present study sought to gain a deeper understanding of the gender differences in antecedents to alcohol use and the role of depressive symptomatology in that relationship. Although future research should seek to replicate the current findings, this investigation constituted an important contribution toward understanding gender differences in drinking that may impact treatment efficacy in general and alcohol relapse in specific.
Acknowledgments
Preparation of this manuscript was supported by National Institute of Alcohol Abuse and Alcoholism grant T32-AA007583.
References
- Annis HM. Inventory of drinking situations. Toronto: Addiction Research Foundation of Ontario; 1982. [Google Scholar]
- Annis HM, Graham JM. Profile types on the Inventory of Drinking Situations: Implications for Relapse Prevention Counseling. Psychology of Addictive Behaviors. 1995;9:176–182. [Google Scholar]
- Annis HM, Graham JM, Davis CS. Inventory of Drinking Situations (IDS): User’s guide. Toronto: Addiction Research Foundation of Ontario; 1987. [Google Scholar]
- Annis H, Martin G. Inventory of Drug-Taking Situations (IDTS-50) Toronto, Ontario, Canada: Addiction Research Foundation of Ontario; 1985. [Google Scholar]
- Annis HM, Sklar SM, Moser AE. Gender in relation to relapse crisis situations, coping, and outcome among treated alcoholics. Addictive Behaviors. 1998;23:127–131. doi: 10.1016/s0306-4603(97)00024-5. [DOI] [PubMed] [Google Scholar]
- Anton RF, Moak DH, Latham P, Waid LR, Myrick H, Voronin K, Thevos A, Wang W, Woolson R. Naltrexone combined with either cognitive behavioral or motivational enhancement therapy for alcohol dependence. Journal of Clinical Psychopharmacology. 2005;25:349–357. doi: 10.1097/01.jcp.0000172071.81258.04. [DOI] [PubMed] [Google Scholar]
- Anton RF, Moak DH, Waid LR, Latham PK, Malcolm RJ, Dias JK. Naltrexone and cognitive behavioral therapy for the treatment of outpatient alcoholics: Results of a placebo-controlled trial. American Journal of Psychiatry. 1999;156:1758–1764. doi: 10.1176/ajp.156.11.1758. [DOI] [PubMed] [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality & Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory. 2. San Antonio, TX: The Psychological Corporation; 1996. [Google Scholar]
- Bradizza CM, Stasiewicz PR. Alcohol and drug use disorders. In: Salzinger K, Serper M, editors. Behavioral mechanisms: Behavioral disorders and their treatment. American Psychological Association; Washington, D.C: in press. [Google Scholar]
- Brady KT, Grice DE, Dustan L, Randall C. Gender differences in substance use disorders. American Journal of Psychiatry. 1993;150:1707–1711. doi: 10.1176/ajp.150.11.1707. [DOI] [PubMed] [Google Scholar]
- Brown SA, Inaba RK, Gillin JC, Schuckit MA, Stewart MA, Irwin MR. Alcoholism and affective disorder: Clinical course of depressive symptoms. American Journal of Psychiatry. 1995;152:45–52. doi: 10.1176/ajp.152.1.45. [DOI] [PubMed] [Google Scholar]
- Connors GJ, Maisto SA, Zywiak WH. Male and female alcoholics’ attributions regarding the onset and termination of relapses and the maintenance of abstinence. Journal of Substance Abuse. 1998;10:27–42. doi: 10.1016/s0899-3289(99)80138-2. [DOI] [PubMed] [Google Scholar]
- Fritz MS, MacKinnon DP. Required sample size to detect the mediated effect. Psychological Science. 2007;18:233–239. doi: 10.1111/j.1467-9280.2007.01882.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glenn SW, Parsons OA. Prediction of resumption of drinking in posttreatment alcoholics. International Journal of the Addictions. 1991;26:237–254. doi: 10.3109/10826089109053186. [DOI] [PubMed] [Google Scholar]
- Grant BF, Harford TC. Comorbidity between DSM-IV alcohol use disorders and major depression: results of a national survey. Drug & Alcohol Dependence. 1995;39:197–206. doi: 10.1016/0376-8716(95)01160-4. [DOI] [PubMed] [Google Scholar]
- Hasin DS, Goodwin RD, Stinson FS, Grant BF. Epidemiology of major depressive disorder: Results from the National Epidemiologic Survey on Alcoholism and Related Conditions. Archives of General Psychiatry. 2005;62:1097–1106. doi: 10.1001/archpsyc.62.10.1097. [DOI] [PubMed] [Google Scholar]
- Irvin JE, Bowers CA, Dunn ME, Wang MC. Efficacy of relapse prevention: A meta-analytic review. Journal of Consulting & Clinical Psychology. 1999;67:563–570. doi: 10.1037//0022-006x.67.4.563. [DOI] [PubMed] [Google Scholar]
- Kendler KS, Davis CG, Kessler RC. The familial aggregation of common psychiatric and substance abuse disorders in the National Comorbidity Survey: A family history study. British Journal Psychiatry. 1997;170:541–548. doi: 10.1192/bjp.170.6.541. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Zhao S, Blazer DG, Swartz M. Prevalence, correlates, and course of minor depression and major depression in the national comorbidity survey. Journal of Affective Disorders. 1997;45:19–30. doi: 10.1016/s0165-0327(97)00056-6. [DOI] [PubMed] [Google Scholar]
- Kessler RC. Gender differences in major depression: Epidemiological findings. In: Frank E, editor. Gender and its effects on psychopathology. Washington, DC: American Psychiatric Publishing, Inc; 2000. pp. 61–84. [Google Scholar]
- Lapham SC, Smith E, C’de Baca J, Chang I, Skipper BJ, Baum G, Hunt WC. Prevalence of psychiatric disorders among persons convicted of driving while impaired. Archives of General Psychiatry. 2001;58:943–949. doi: 10.1001/archpsyc.58.10.943. [DOI] [PubMed] [Google Scholar]
- Marlatt GA, Gordon JR. Determinants of relapse: Implications for the maintenance of behavior change. In: Davidson PO, Davidson SM, editors. Behavioral medicine: Changing health lifestyles. New York: Runner/Mazel; 1980. pp. 410–452. [Google Scholar]
- Marlatt GA, Gordon JR. Relapse Prevention. New York, NY: Guildford Press; 1985. [Google Scholar]
- O’Leary TA, Monti PM. Cognitive-behavioral therapy for alcohol addiction. In: Hofmann SG, Tompson MC, editors. Treating chronic and severe mental disorders: A handbook of empirically supported interventions. New York, NY: Guildford Press; 2002. pp. 234–257. [Google Scholar]
- Olenick NL, Chalmers DK. Gender-specific drinking styles in alcoholics and nonalcoholics. Journal of Studies on Alcohol. 1991;52:325–330. doi: 10.15288/jsa.1991.52.325. [DOI] [PubMed] [Google Scholar]
- Pettinati HM, Pierce JD, Wolf AL, Rukstalis MR, O’Brien CP. Gender differences in comorbidly depressed alcohol-dependent outpatients. Alcoholism: Clinical & Experimental Research. 1997;21:1742–1746. [PubMed] [Google Scholar]
- Rubin A, Stout RL, Longabaugh R. Gender differences in relapse situations. Addiction. 1996;91(Supplement):111–120. [PubMed] [Google Scholar]
- Sigmon ST, Pells JJ, Boulard NE, Whitcomb-Smith S, Edenfield TM, Hermann BA, LaMattina SM, Shartel JG, Kubik E. Gender differences in self-reports of depression: The response bias revisited. Sex Roles. 2005;53:401–411. [Google Scholar]
- Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. In: Leinhart S, editor. Sociological Methodology. San Francisco: Jossey-Bass; 1982. pp. 290–312. [Google Scholar]
- Sobell LC, Sobell MB. Timeline Follow-back: A technique for assessing self-reported ethanol consumption. In: Allen J, Litten RZ, editors. Measuring Alcohol Consumption: Psychosocial and Biological Methods. Totowa, NJ: Humana Press; 1992. pp. 41–72. [Google Scholar]
- Stasiewicz PR, Nochajski TH, Homish DL. Assessment of alcohol use disorders among court-mandated DWI offenders. Journal of Addictions & Offender Counseling. 2007;27:102–112. [Google Scholar]
- Torrens M, Fonseca F, Mateu G, Farre M. Efficancy of antidepressants in substance use disorders with and without comorbid depression: A systematic review and meta-analysis. Drug and Alcohol Dependence. 2005;78:1–22. doi: 10.1016/j.drugalcdep.2004.09.004. [DOI] [PubMed] [Google Scholar]
- Zywiak WH, Stout RL, Longabaugh R, Dyck I, Connors GJ, Maisto SA. Relapse-onset factors in Project Match: The Relapse Questionnaire. Journal of Substance Abuse Treatment. 2006;31:341–345. doi: 10.1016/j.jsat.2006.05.007. [DOI] [PubMed] [Google Scholar]
- Zywiak WH, Stout RL, Trefry WB, Glasser I, Connors GJ, Maisto SA, Westerberg VS. Alcohol relapse repetition, gender, and predictive validity. Journal of Substance Abuse Treatment. 2006;30:349–353. doi: 10.1016/j.jsat.2006.03.004. [DOI] [PubMed] [Google Scholar]