

Abstract
Objective
To implement an Employee Total Health Management (ETHM) model-based questionnaire and provide estimates of model program elements among a statewide sample of Iowa employers.
Methods
Survey a stratified random sample of Iowa employers, characterize and estimate employer participation in ETHM program elements
Results
Iowa employers are implementing under 30% of all 12 components of ETHM, with the exception of occupational safety and health (46.6%) and worker compensation insurance coverage (89.2%), but intend modest expansion of all components in the coming year.
Conclusions
The Employee Total Health Management questionnaire-based survey provides estimates of progress Iowa employers are making toward implementing components of total worker health programs.
The case for change for transforming employee health programs into integrated employee well-being programs has been articulated by three inter-related reports.1, 2, 3 The 2004 NIOSH Steps to a Healthier U.S. Workforce Conference influenced the foundation of the NIOSH WorkLife Initiative, since transitioned to the NIOSH Total Worker Health™ Program (TWH)(www.cdc.gov/niosh/TWH) which supports The University of Iowa Healthier Workforce Center for Excellence4. The concept of worker well-being, which underpins TWH, has gained recognition globally over the last decade and was the subject of the 2010 Towards Better Work and Well-being Conference in Helsinki, drawing 190 participants from 30 countries.5 Despite this widening recognition, the concept of TWH is not well understood by the vast majority of employers. In the US, this is particularly so among small employers (< 50 employees), which constitute over 97% of Iowa employers. While small employers are still primarily motivated by workplace regulations, incentives offered via by the public health and prevention provisions of the Patient Protection and Accountable Care Act (ACA) will likely influence future behavior.
The University of Iowa Healthier Workforce Center for Excellence has sought, through its outreach conferences, surveys, technical reports and electronic bulletins, to make Iowa employment stakeholders more aware of the benefits of fully integrated employee health protection and promotion, or TWH, programs. We have partnered with David P. Lind Benchmark (DPLB), an Iowa health benefit evaluation company, which has conducted 14 annual Iowa Employer Benefit Studies (www.dplindbenchmark.com); first to enhance the DPLB Health and Wellness Initiatives module, and for his 2012 study to develop and implement an expanded Health and Wellness Initiatives module based on elements of the Employee Total Health Management (ETHM) model, as articulated by the IOM (Figure 1)1. This model seeks to describe the components of an integrated and sustainable approach to total employee health management, while the IOM also makes the case that such programs must be integrated and measurable to be effective and sustainable. Hence, TWH programs must include health protection and health promotion program components, which together include several modifiable risk factors that have been linked to increased sickness absenteeism, increased presenteeism and reductions in preventable health care costs.6, 7, 8 However, these findings are based on studies of large employers that include many if not all of these program components, but which also organize their employee health programs to ensure integration of health protection and health promotion programs. While available evidence makes clear that integration of employee health programs is important, the methodology for defining and measuring integration is still developing and is not the focus of this study.9, 10
Figure 1.
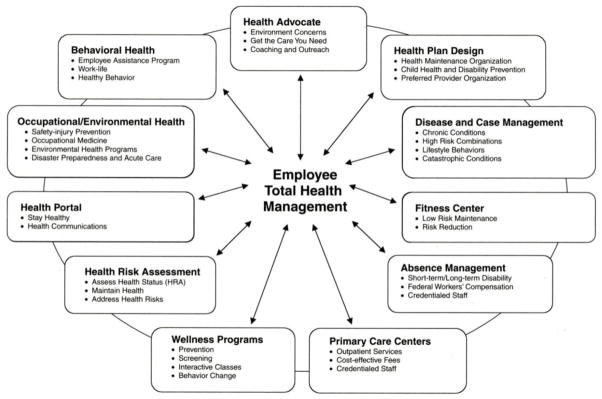
IOM Employee Total Health Management Model
Reprinted with the permission of the National Academies of Sciences
To fully describe employer adoption of TWH would require assessment of both ETHM program components and measures of program organization and integration. The goal of this 2012 survey of a sample of Iowa employers is to translate the ETHM into a 12 item questionnaire suitable for use for a statewide survey of employers of all sizes, and to provide estimates of the ETHM model component adoption among these employers.
Methods
A total of 107,940 eligible employers were identified from the Iowa Dun & Bradstreet database for employers with two or more employees (2012). Organizations were stratified by number of employees (2–9, 10–19, 20–49, 50–249, 250–999, 1000+), using proprietary randomization software developed by Data Point Research under contract with DPLB. A stratified random sample of 5,606 employers was selected for the 2012 survey. Data was collected from a total of 1,206 organizations through web-based questionnaires and with telephone follow-up.
The Employee Total Health Management questionnaire is an elaboration of eight previous DPLB Health and Wellness Initiatives modules included in Iowa Employer Benefit surveys of over 7400 employers. Items used in previous surveys included medical information (website, newsletter, etc.), blood pressure/cholesterol screening, chronic disease management, smoking cessation/weight control wellness programs, health risk assessment, and health club discount or other incentives. The HWCE provided collaboration on the design of the previous questionnaire and contracted with DPLB to administer the current ETHM-based questionnaire, which used the same format and many of the same items included in previous DPLB surveys (see Table 3 for the full questionnaire). Survey data included employment sector, organization size, rural or urban location as defined by USDA Rural-Urban Continuum Codes11, insurance coverage, and health and wellness module responses. All analyses were conducted at the HWCE using SAS, version 9.2 (SAS Institute, Inc., Cary, NC).
Table 3.
Employers Offering or Considering Health and Wellness Programs
| Employer Total Health Management Questionnaire Items | Currently Offers | Plans to offer in the next 12 months |
|---|---|---|
| Does your organization currently offer health or medical information, such as a website or newsletter? | 28.4% (340/1199) | 7.0% (84/1199) |
| Does your organization currently offer Health Advocacy, such as health counseling or coaching? | 16.3% (195/1199) | 3.3% (40/1199) |
| Does your organization currently offer a Health Risk Assessment program either on paper or computer? | 16.8% (201/1199) | 3.5% (42/1199) |
| Does your organization currently offer a Health Screening program such as one that would include screenings for blood pressure, obesity, blood sugar, cholesterol, lung function, vision, or hearing? | 19.0% (228/1199) | 2.8% (33/1199) |
| Does your organization currently offer a Chronic Disease Management program, such as one that addresses heart disease, diabetes, hypertension, or COPD? | 13.3% (159/1199) | 2.1% (25/1199) |
| Does your organization currently offer a Wellness program such as one that addresses smoking cessation, weight control, or exercise and fitness routines? | 18.3% (219/1199) | 3.5% (42/1199) |
| Does your organization currently provide or sell healthy food options to employees? | 16.6% (199/1199) | 1.4% (17/1199) |
| Does your organization currently offer a Health Incentive program such as health club membership, cash bonuses for participation, or insurance premium discounts? | 14.8% (178/1199) | 2.9% (35/1199) |
| Does your organization currently retain or contract with a health care provider such as a physician, physician assistant, or nurse practitioner? | 7.4% (89/1199) | 1.1% (13/1199) |
| Does your organization currently offer an Occupational Safety and Health program such as programs on worksite safety, industrial hygiene, ergonomics, environmental exposure control, or disaster preparedness? | 46.6% (559/1199) | 1.8% (21/1199) |
| Does your organization currently offer a Behavioral Health program to provide employees with counseling for alcohol, drugs, depression, or work-life assistance? | 21.4% (257/1199) | 1.2% (15/1199) |
| Does your organization currently provide Workers’ Compensation Insurance? | 89.2% (1069/1199) | 1.2% (15/1199) |
| Does your organization currently have a Credentialed Disability Management Specialist? | 3.2% (38/1199) | 0.6% (7/1199) |
Results
A total of 888 organizations of fewer than 50 employees, 232 of 50–249 employees and 91 of 250 or more employees participated in the survey. The response rate was 21.5%. The margin of error for all organizations employing fewer than 250 was 2.9 percent, and for all employers with 250 or more employees, the margin of error was 9.3 percent.
Employers by organization size and SIC code, which distributes the population over eight employment sectors, are summarized in Table 1. Seven employers did not fall within any of these SIC codes and were eliminated from further analysis. As is evident within all employment sectors, this sample provides employee distributions which are predominantly small, nearly a third employing nine or fewer employees and nearly three quarters employing fewer than 50 employees. The largest employment sectors are Services, Retail Trade and Manufacturing which together constituted two thirds of the sample.
Table 1.
Employers by Employment Sector and Organization Size
| Major Employment Sectors | Organization Size | ||||||
|---|---|---|---|---|---|---|---|
| Frequency Percent | 2–9 | 10–19 | 20–49 | 50–249 | 250–999 | 1000 + | Total |
| Construction | 4 | 10 | 10 | 5 | 0 | 1 | 30 |
| 0.33 | 0.83 | 0.83 | 0.42 | 0.00 | 0.08 | 2.50 | |
| Manufacturing | 66 | 50 | 43 | 38 | 10 | 2 | 209 |
| 5.50 | 4.17 | 3.59 | 3.17 | 0.83 | 0.17 | 17.43 | |
| Transportation and Pub. Utilities | 8 | 8 | 11 | 12 | 1 | 0 | 40 |
| 0.67 | 0.67 | 0.92 | 1.00 | 0.08 | 0.00 | 3.34 | |
| Wholesale Trade | 3 | 13 | 15 | 8 | 6 | 0 | 45 |
| 0.25 | 1.08 | 1.25 | 0.67 | 0.50 | 0.00 | 3.75 | |
| Retail Trade | 104 | 68 | 32 | 11 | 2 | 1 | 218 |
| 8.67 | 5.67 | 2.67 | 0.92 | 0.17 | 0.08 | 18.18 | |
| Finance, Insurance and Real Estate | 40 | 46 | 25 | 19 | 10 | 6 | 146 |
| 3.34 | 3.84 | 2.09 | 1.58 | 0.83 | 0.50 | 12.18 | |
| Services | 76 | 88 | 71 | 95 | 30 | 13 | 373 |
| 6.34 | 7.34 | 5.92 | 7.92 | 2.50 | 1.08 | 31.11 | |
| Public Administration | 48 | 19 | 25 | 38 | 7 | 1 | 138 |
| 4.00 | 1.58 | 2.09 | 3.17 | 0.58 | 0.08 | 11.51 | |
| Total | 349 | 302 | 232 | 226 | 66 | 24 | 1199 |
| 29.11 | 25.19 | 19.35 | 18.85 | 5.50 | 2.00 | 100.00 | |
Over half of organizations participating in this survey are located in rural counties, which include 55% of companies with 9 or fewer employees (Table 2), while organizations employing at least 250 employees are located primarily in urban counties. Only 51% of the smallest organizations offer health insurance, while organizations employing at least 50 employees reported nearly universal health care coverage (96%). Organizations employing at least 250 employees were frequently self-insured, while organizations under 50 (of those which offer health insurance), offered fully insured policies over 85% of the time.
Table 2.
Location and Insurance Coverage by Organization Size
| Organization Size | |||||||
|---|---|---|---|---|---|---|---|
| 2–9 | 10–19 | 20–49 | 50–249 | 250–999 | 1000+ | Total | |
| Rural | 55.0% (191/347) | 14.1% (168/301) | 53.2% (123/231) | 55.8% (126/226) | 38.5% (25/65) | 20.9% (5/24) | 53.4% (638/1194) |
| Offers health insurance | 51.3% (179/349) | 77.2% (233/302) | 87.5% (203/232) | 96.5% (218/226) | 96.7% (64/66) | 91.7% (22/24) | 46.6% (556/1194) |
| Offers a self-insured health insurance policy* | 11.8% (20/169) | 10.7% (24/224) | 16.9% (32/189) | 36.0% (71/197) | 66.7% (40/60) | 90.0% (18/20) | 23.9% (205/859) |
| Offers a fully-insured health insurance policy** | 88.2% (149/169) | 89.3% (200/224) | 84.1% (159/189) | 66.0% (130/197) | 33.3% (20/60) | 10.0% (2/20) | 76.8% (660/859) |
A self-funded plan in which employer assumes financial risk for health care benefits
Employee health insurance plan provided through a health insurance carrier
The prevalence of organizations offing ETHM program components are summarized in Table 3. The most frequent response (89%) was provision of worker’s compensation insurance, required by law for most Iowa employers. Nearly 47% of employers reported having an occupational safety and health program, an essential element of TWH programs. Other program elements were much less prevalent, led by programs on health or medical information, behavioral health, wellness, having a health risk assessment, and health advocacy. Employers collectively indicated they intended to increase offering all ETHM program components in the next 12 months, most frequently planning to offer new health information programs (7%). Larger employers (>50 employees) planned to offer new program components more frequently than did small employers; organization responses by SIC code found inconsistent participation across industrial sectors, led by Public Administration (see www.hwce.org for these additional results).
The distribution of program participation by company size found only organizations employing 9 or fewer to have less than 90% worker’s compensation insurance coverage (Table 4). Only a third of 2–9 employee organizations reported having occupational health and safety programs, a prevalence that increased to nearly 80% among organization employing 1000 or more. Similar progressions in prevalence by organization size were observed for all other ETHM program components.
Table 4.
Employee Total Health Management Element Adoption by Organization Size
| Program | 2 to 10 Employees (n=349) | 11 to 19 Employees (n=302) | 20 to 49 Employees (n=232 | 50 to 249 Employees (n=226) | 250–990 Employees (n=66) | 1000+ Employees (n=24) |
|---|---|---|---|---|---|---|
| Health or Medical Information | 12.3% | 18.5% | 29.3% | 47.4% | 68.2% | 87.5% |
| Health Advocacy | 6.6% | 11.6% | 14.2% | 25.2% | 42.4% | 79.2% |
| Health Risk Assessment | 4.6% | 10.3% | 12.5% | 31.0% | 56.1% | 75.0% |
| Health Screening | 4.6% | 11.6% | 15.1% | 36.7% | 62.1% | 75.0% |
| Chronic Disease Management | 3.2% | 6.3% | 9.9% | 23.0% | 54.6% | 75.0% |
| Wellness Program | 4.6% | 8.9% | 18.1% | 31.4% | 65.2% | 83.3% |
| Healthy Food Options | 8.0% | 10.6% | 12.1% | 25.2% | 56.1-% | 70.8% |
| Health Incentive Program | 3.2% | 7.6% | 12.9% | 26.6% | 59.1% | 62.5% |
| Health Care Provider on Retainer | 4.0% | 3.6% | 6.5% | 12.4% | 16.7% | 41.7% |
| Occupational Health and Safety Program | 33.5% | 44.0% | 52.2% | 53.5% | 72.7% | 79.2% |
| Behavioral Health | 5.7% | 9.6% | 19.1% | 33.5% | 77.3% | 91.7% |
| Workers’ Compensation Insurance | 82.8% | 91.4% | 91.8% | 91.6% | 92.4% | 95.8% |
| Credentialed Disability Specialist | 2.0% | 2.0% | 2.6% | 3.5% | 9.1% | 20.8% |
DISCUSSION
Development of the Employee Total Health Management questionnaire, based on a model described by the IOM1, provides a framework to describe and quantify employer participation in providing individual components of this model. As Iowa begins to implement the prevention provisions of ACA, this questionnaire will provide a TWH tool to assess statewide progress as employers provide the building blocks for a TWH approach to safer and healthier workplaces
Very few population-based data are available for small employers, especially for companies employing 2–9 employees; yet 90% of workplaces are of this size in Iowa and many other more rural states. As has been documented by all previous Iowa Employer Benefit Studies, these smaller employers are usually not able to offer health insurance, so the modest number of small employers offering health and wellness program components is not surprising. The ETHM questionnaire contained several Health and Wellness Initiative questions included in previous DPLB surveys, and the results from annual survey-to-annual survey results on these large samples of Iowa employers, are remarkably consistent--in general finding increasing participation with time. Consistent with previous results, employers intend, for all ETHM program elements, to extend their offerings in the coming year.
The current survey estimates only employer participation in offering the 12 ETHM program components, but did not seek to measure integration of these employee health programs. However, several of these program components are essential for measurement of modifiable risk factors known to be important predictors of preventable health care costs, sickness absenteeism and presenteeism.6, 7, 8 Among large employers participating in the cited studies, risk has been found to decrease as employees actively engage in more complete prevention programs, the most successful of which include individual coaching to optimize individual employee behavior8 Exactly how even large employers organize and administer their integrated employee health programs, while known to be important and advocated by the IOM, is less clear.1 The first organizational priority recommended by the IOM was transformational leadership, which has recently been shown to have a positive effect on employee well-being.12 Development of valid and reliable methods to assess organizational measures of integrated employee health programs continues to be an important research priority.9 Another research priority necessary to fully realize the benefits of TWH programs is go beyond measurement of risk factors to base program impact based on measures of employee well- being, absenteeism and presenteeism.
Limitations
The generalizability of the results of this study is limited by the response rate of this survey. However, this health and wellness survey is a further iteration of eight previous annual surveys of large, random samples of predominantly small Iowa employers for which there is an acceptable margin of error of 2.9%. For the six items common to the previous DPLB survey module and ETHM questionnaire, the year-to-year results are remarkably consistent suggesting this instrument is providing reliable and valid results for these items. The study has a number of strengths including assessment of a large random statewide sample of predominantly small Iowa employers for which little research is available, and population-based employer estimates of adoption of components of an IOM-endorsed Employee Total Health Management model.
Conclusions
This statewide survey of health and wellness program activities provides useful estimates from a random statewide sample of employers. This is important as it provides unique data about small employers, the employment segment which faces the greatest challenge in both providing employees with health insurance and health and wellness benefits. These data build on previous annual DPLB surveys and provide a benchmark for future adoption of TWH program components in Iowa. As the US shifts to a more health based model of health care, this survey instrument may be useful for other population-based assessments of employer participation in building employee health programs.
Acknowledgments
This study was funded by funding from NIOSH grant: 5U19OH008868
Footnotes
None of the authors had any conflict of interest related to the manuscript.
Contributor Information
James A. Merchant, Director, University of Iowa, Healthier Workforce Center for Excellence, 118 IREH, University Research Park, Iowa City, IA 52242.
David P. Lind, President, David P. Lind Benchmark, 13375 University, Suite 202, Clive, IA 50325.
Kevin M. Kelly, Senior Scientist, University of Iowa, Healthier Workforce Center for Excellence, 102 IREH, University Research Park, Iowa City, IA 52242.
Jennifer L. Hall, Outreach Director, University of Iowa, Healthier Workforce Center for Excellence, 102 IREH, University Research Park, Iowa City, IA 52242.
References
- 1.Institute of Medicine Committee to Assess Worksite Preventive Health Program Needs for NASA Employees. Integrating Employee Health—A Model Program for NASA. Washington, DC: The National Academies Press; 2005. [Google Scholar]
- 2.Sorenson G, Barbeau E. NIOSH 2012. Research Compendium: The NIOSH Total Worker Health Program: Seminal research papers 2012. Washington, DC: Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health; 2012. May, [Accessed May, 2013.]. Steps to a healthier JS Workforce: Integrating occupational health and safety and worksite health promotion. State of the science; p. 10214. DHHS (NIOSH) Publication No. 2012-146. Available at: http://www.cdc.gove/niosh/docs/2012-146/ [Google Scholar]
- 3.Goetzel RZ. NIOSH 2012. Research compendium: The NIOSH Total Worker Health Program: Seminal research papers 2012. Washington, DC: Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH); 2012. May, [Accessed May, 2013.]. Examining the value of integrating occupational health and safety and health promotion programs n the workplace; p. 10214. Publication No. 2012-146. Available at: http://www.cde.gove/niosh/docs/2012-146/ [Google Scholar]
- 4.Cherniack M, Henning R, Merchant JA, Punnett L, Sorensen GR, Wagner G. Statement on National Worklife Priorities. American Journal of Industrial Medicine. 2011 Jan;54(1):10–20. doi: 10.1002/ajim.20900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Schulte P, Vainio H. Well-being at work—overview and perspective. Scand J Work Environ Health. 2010;36(5):422–429. doi: 10.5271/sjweh.3076. [DOI] [PubMed] [Google Scholar]
- 6.Sorenson G, et al. Integration of health protection and health promotion: innovative approaches to worksite health. JOEM. In press this issue, 2013. [Google Scholar]
- 7.Pronk N. Integrated worker health protection and promotion programs: overview and perspectives on health and economics outcomes. JOEM. doi: 10.1097/JOM.0000000000000031. In press this issue, 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.USDA Economic Research Service. [Accessed July 17, 2013.];Rural-Urban Continuum Codes. 2003 Available at: http://www.ers.usda.gov/data-products/rural-urban-continuum-codes.aspx.
- 9.Burton WN, Coni DJ, Chen CY, Schultz AB, Edington DW. The role of health risk factors and diseases on worker productivity. JOEM. 1999;41(10):863–877. doi: 10.1097/00043764-199910000-00007. [DOI] [PubMed] [Google Scholar]
- 10.Goetzel RZ, Pei S, Tabrizi MJ, Henke RM, Kowlessar N, Nelson CF, Metz DR. Ten modifiable health risk factors are linked to more than one-fifth of employer-employee health care spending. Health Affairs. 2012;31(11):2474–2484. doi: 10.1377/hlthaff.2011.0819. [DOI] [PubMed] [Google Scholar]
- 11.Loeppke R, Edington D, Bender J, Reynolds A. The association of technology in a workplace wellness program with health risk factor reduction. JOEM. 2013;55(3):259–264. doi: 10.1097/JOM.0b013e3182898639. [DOI] [PubMed] [Google Scholar]
- 12.Jacobs C, Holger P, Lehner B, Driller E, Nitzsche A, Stieler-Lorenz B, Wasem J, Jung J. The influence of transformational leadership on employee well-being. JOEM. 2013;55(7):772–778. doi: 10.1097/JOM.0b013e3182972ee5. [DOI] [PubMed] [Google Scholar]