

Highlights
-
•
Eventration of diaphragm is an abnormal elevation of an intact diaphragm characterized by a developmental abnormality of the diaphragm musculature.
-
•
Eventration may be complicated by acute gastric volvulus, chronic gastric volvulus, or chronic recurrent volvulus of the splenic flexure of the colon.
-
•
Symptomatic gastric volvulus associated with diaphragmatic eventration is a surgical emergency.
Keywords: Diaphragmatic eventration, Gastric volvulus, Gastropexy
Abstract
Background
Eventration of diaphragm associated with gastric volvulus is an uncommon condition.
Case presentation
We reporting a case of a 16-year-old male having left sided diaphragmatic eventration associated with acute mesenteroaxial gastric volvulus. The patient presented with acute pain abdomen and upper abdomen fullness. Plication of left hemidiaphragm with anterior gastropexy was performed through an abdominal approach. Postoperatively the patient’s recover uneventfully.
Conclusion
Symptomatic gastric volvulus associated with diaphragmatic eventration is a surgical emergency and always requires surgical repair.
1. Introduction
Eventration of diaphragm is an abnormal elevation of an intact diaphragm and most often is characterized by a developmental abnormality of the diaphragm musculature. Permanent elevation of either right or left hemi diaphragm in diaphragmatic eventration causes abnormal placement of organs. It may be either congenital or acquired owing to abnormalities in phrenic nerve function. Eventration may be further complicated by acute gastric volvulus, chronic gastric volvulus, or chronic recurrent volvulus of the splenic flexure of the colon [1].
We are reporting a case of a 14-year-old male having left sided diaphragmatic eventration associated with acute mesenteroaxial gastric volvulus Fig. 1.
Fig. 1.
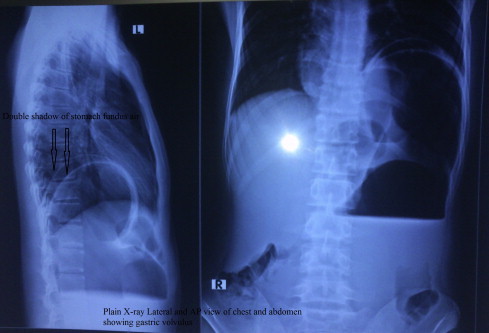
Plain X- ray film of abdomen and chest lateral and antero–posterior view.
2. Case presentation
16 years old male patient presented to our casualty department of PBM hospital with complain of pain and fullness in upper abdomen from last 2 days. Patient also had complaint of retching after admission in hospital. On examination slight distention was present in upper abdomen with rest whole abdomen non-distended and soft. Ultrasound abdomen shows distended stomach. X-ray FPA done in erect position shows elevated left hemi-diaphragm, two large air fluid level in left hypo-chondrium. Barium study indicates the diagnosis of gastric volvulus with eventration of diaphragm. Diagnosis was confirmed by contrast enhanced CT scan. Nasogastric tube decompression was done. Patient was taken for emergency laparotomy. On exploration spleen comes anteriorly in midline and stomach is fully distended, rotated along axis of its mesentry, occupy whole of left hypochondrium. Diaphragm was high up in chest and eventration present. Plication of left hemidiaphragm with anterior gastropexy was done Fig. 2.
Fig. 2.
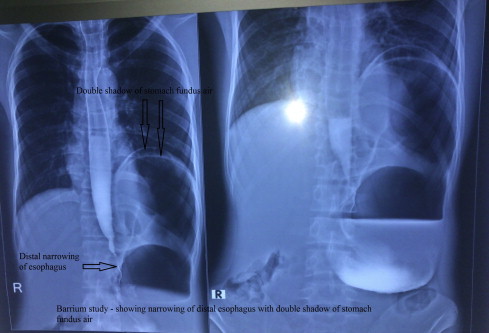
Barium study of abdomen and chest shows diaphragmatic eventration with gastric volvulus.
3. Discussion
Eventration is a congenital anomaly of the diaphragm characterized by muscular aplasia and subsequent abnormal elevation of an intact hemidiaphragm Fig. 3. Gastric volvulus was first described by Berti in 1866 in a female autopsied patient, and the first operation was performed by Berg in 1897 [2]. Since then, over 400 cases have been reported in literature; at least 2/3rd are of chronic or recurring type [3]. Based on etiology, both primary and secondary forms of gastric volvulus have been recognized. The primary (idiopathic) subtype occurs as a result of neoplasia, adhesions or an abnormality in the attachment of the stomach. Alternatively, a secondary gastric volvulus may arise because of disorders of gastric anatomy or gastric function or abnormalities of adjacent organs such as the diaphragm or spleen. In adults, the most common association is with a paraesophageal hernia however traumatic defects, diaphragmatic eventration and phrenic nerve paralysis have also been reported [4]. The three remaining categories of gastric volvulus that exist are defined according to their axes of rotation. Organo-axial volvulus is the most common. Occurring in 60% of cases, this subtype is associated with para-esophageal hernias and diaphragmatic eventration. It is characterized by rotation around an axis adjoining the gastro esophageal junction and the pylorus and therefore causes the greater curvature of the stomach to rest superior to the lesser curvature, resulting in an ‘inverted’ stomach. The second type of gastric volvulus is mesenteroaxial. This less commonly encountered variant is not usually associated with diaphragmatic anomalies and is characterized by rotation of the stomach along an axis perpendicular to its longitudinal axis. In this position the stomach lies in the vertical plane with the antrum and pylorus rotated anterior and superior to the gastro esophageal junction. The third and rarest form of gastric volvulus is when the stomach rotates about both the organo-axial and mesenteroaxial axes resulting in a combined volvulus [5]. The classic triad of retching, severe and constant epigastric pain, and difficulty in passing a nasogastric tube should suggest the presence of acute gastric volvulus [6]. Few case reports have shown that delayed onset of secondary gastric volvulus associated with congenital diaphragmatic eventration is also possible [7]. The diagnosis of diaphragmatic eventration associated with gastric volvulus is usually straight forward and can be established by history and, in most cases, by routine chest X-rays and either upper GI series or CT scan. Management of diaphragmatic eventration varies greatly depending on whether the diagnosis is made in infants or adults. Simple cases of diaphragmatic eventration may not require surgical intervention if it is not intruding significantly into the thoracic cavity and is not associated with adverse symptoms [1]. Symptomatic gastric volvulus associated with diaphragmatic eventration is a surgical emergency and always requires surgical repair [8]. The most widely accepted approach is repair via an abdominal (subcostal) incision because this allows ready access to both diaphragms for plication, permits anterior gastric fixation via a gastropexy or gastrostomy, and allows abdominal exploration for associated gastrointestinal anomalies [8].
Fig. 3.
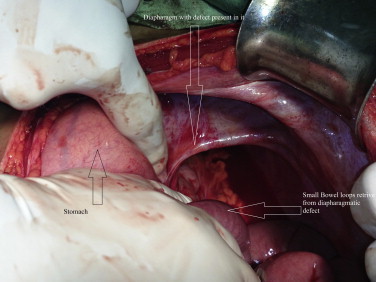
Intraoperative picture showing eventration defect of left hemidiapharagm.
4. Conclusion
In order to prevent the very high morbidity and mortality due to complications of gastric volvulus in a case of eventration of diaphragm, we recommend early diagnosis of the condition, early surgical referral, and urgent surgical intervention.
Conflicts of interest
No conflict of interest.
Funding
No source of funding.
Consent
Consent of patient not required.
Author contribution
All work done by corresponding author Prabhu Dayal Sinwar.
Acknowledgment
I heartily thankful to Monika Kuri for help in typing the material of case report.
References
- 1.Wayne E.R., Campbell J.B., Burrington J.D., Davis W.S. Eventration of the diaphragm. J. Pediatr. Surg. 1974;9(5):643–651. doi: 10.1016/0022-3468(74)90101-8. [DOI] [PubMed] [Google Scholar]
- 2.Matsuzaki Y., Asai M., Okura T., Tamura R. Ultrasonography of gastric volvulus; peanut sign. Intern. Med. 2001;40(1):23–27. doi: 10.2169/internalmedicine.40.23. [DOI] [PubMed] [Google Scholar]
- 3.Camblos J.F.B. Acute volvulus of stomach. Am. Surg. 1969;35(7):505–509. [PubMed] [Google Scholar]
- 4.McElreath D.P., Olden K.W., Hiccups Aduli F. A subtle sign in the clinical diagnosis of gastric volvulus and a review of the literature. Dig. Dis. Sci. 2008;53:3033–3036. doi: 10.1007/s10620-008-0258-2. [DOI] [PubMed] [Google Scholar]
- 5.Cribbs R.K., Gow K.W., Wulkan M.L. Gastric volvulus in infants and children. Pediatrics. 2008;122:752–762. doi: 10.1542/peds.2007-3111. [DOI] [PubMed] [Google Scholar]
- 6.Llaneza P.P., Salt 2nd W.B. Gastric volvulus-More common than previously thought? Postgrad. Med. 1986;80(5):279–283. doi: 10.1080/00325481.1986.11699576. [DOI] [PubMed] [Google Scholar]
- 7.Cancrini A., Bellotti C., Santoro A., Stanzani G.L., Ascenzi P., Cancrini G. Diaphragmatic eventration in the adult: repair with Gore- Tex surgical mesh. G Chir. 1998;19(1–2):35–39. [PubMed] [Google Scholar]
- 8.Par W., Choi S., Suh S. Pediatric gastric volvulus–experience with 7 cases. J. Korean Med. Sci. 1992;7(3):258–263. doi: 10.3346/jkms.1992.7.3.258. [DOI] [PMC free article] [PubMed] [Google Scholar]