

Highlights
-
•
Our goal in presenting this case was to emphasize the importance of taking an accurate medical history in patients with clear cell carcinoma, a rarely seen gallbladder cancer.
Keywords: Gallbladder, Clear cell carcinoma, Cholecystectomy
Abstract
Introduction
Gallbladder cancer is a rare tumor in the gastrointestinal tract has poor prognosis, low survival and is difficult to diagnose. The most common type of gallbladder cancer is adenocarcinoma, and the incidence of clear cell carcinoma is low. Mostly, it is difficult to determine whether the isolated tumor is a primary tumor in the gallbladder or a metastatic tumor from another region. Before accepting a clear cell carcinoma as a primary gallbladder tumor, the kidneys and other possible secondary focuses are clinically considered in terms of metastases.
Presentation of case
Here, we present a rarely seen case of gallbladder clear cell carcinoma, which was diagnosed by pathological examination after the surgery.
Discussion
Prior to establishing that clear cell carcinoma is a primary gallbladder cancer, it is appropriate to clinically investigate possible secondary focuses, in particular the kidneys in terms of metastasis.
Conclusion
Our goal in presenting this case was to emphasize the importance of taking an accurate medical history in patients with clear cell carcinoma, a rarely seen gallbladder cancer.
1. Introduction
Gallbladder cancers are rare tumors with a poor prognosis [1]. They are the fifth most common malignant tumor of the gastrointestinal tract [2]. Only 10–50% of the patients can be diagnosed in the preoperative period [1]. While the most common type of gallbladder cancer is adenocarcinoma, clear cell carcinoma is seen less frequently. Prior to establishing clear cell carcinoma as a primary gallbladder cancer, it is appropriate to clinically investigate possible secondary focuses, in particular the kidneys in terms of metastasis. Metastases have been reported in approximately one-third of patients with renal cell cancer at the time of the diagnosis, while in 11% of the patients metastases have been detected 10 or more years later after nephrectomy [3].
2. Case
A 56-year-old female patient presented to our general surgery outpatient clinic with abdominal pain and bloating that occurred after a meal. The physical examination revealed tenderness on deep palpation in the right upper quadrant and an incision scar due to previous left nephrectomy. The patient’s medical history showed that approximately 10 years ago she had undergone nephrectomy for a renal stone and had no other diseases except for hypertension. The patient did not have additional information about the previous operation and did not know the outcome of the pathology. The abdominal computed tomography (CT) with contrast revealed a slightly hyperdense contrast retaining mass lesion in the lumen of the gallbladder that could not be distinguished from the wall (Figs. 1 and 2). The magnetic resonance western (MRI) was performed with a preliminary diagnosis of gallbladder. The axial and coronal sections showed a heterogeneous solid mass protruding towards the associated lumen of the gallbladder which contained hypointense and hyperintense areas (Figs. 3 and 4). Positron emission tomography (PET) scanning was performed in order to screen for other metastatic foci. Axial-coronal-thoracoabdominal PET-CT imaging revealed involvement that was compatible with significant metabolic activity in the mass lesions of the gallbladder (Figs. 5–7 ). Considering that the tumor was limited to the gallbladder, the patient underwent laparoscopic cholecystectomy with resection part of liver tissue of gallbladder bed (Fig. 8). The pathology was reported as clear cell carcinoma, histological grade III, subserosa-invasive, negative for lymphovascular invasion and with safe surgical margins (Figs. 9 and 10).
Figs. 1 and 2.
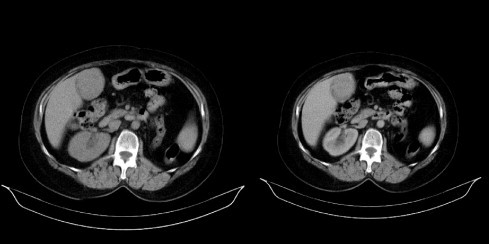
The abdominal computed tomography (CT) with contrast revealed a slightly hyperdense contrast retaining mass lesion in the lumen of the gallbladder that could not be distinguished from the wall.
Figs. 3 and 4.
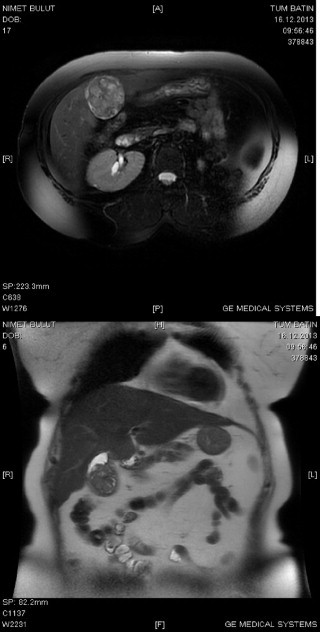
The axial and coronal sections showing a heterogeneous solid mass protruded towards the associated lumen of gallbladder.
Figs. 4–6.
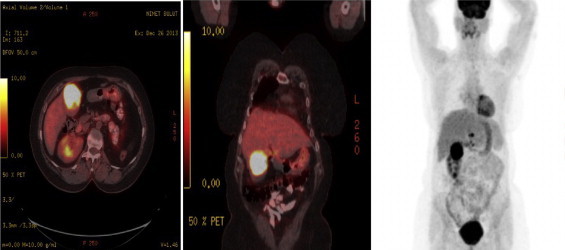
Axial, coronal, thoracoabdominal PET images showing diffuse radioactive involvement in the mass lesion in the gallbladder.
Figs. 7 and 8.

Macroscopic image.
Figs. 9 and 10.
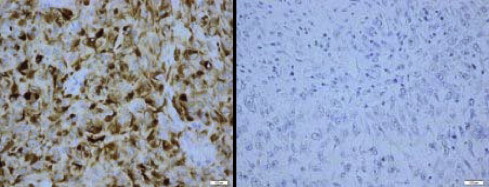
Tumor infiltration composed of small cord structures, showing diffuse pattern and atypical cells with clear nucleus and atypical mitotic figures in desmoplastic stroma.
3. Discussion
Although gallbladder cancer is a rare, it ranks 5th worldwide in digestive system related cancers. Gallbladder cancer is more frequently seen in women, while biliary tract cancers are more frequently seen in men [1]. The risk factors for gallbladder cancer are the presence of a stone larger than 2 cm in diameter inside the gallbladder, polyps larger than 1 cm in diameter inside the gallbladder, choledochal cysts, typhoid and Opisthorchis viverr disease, primary sclerosing cholangitis, porcelain gallbladder, and excessive consumption of red meat and tobacco.
The most common histologic type of gallbladder cancer is adenocarcinoma [2]. In situ carcinoma, papillary carcinoma, mucinous carcinoma, clear cell adenocarcinoma, signet ring cell carcinoma, adeno-squamous carcinoma, squamous cell carcinoma, small cell carcinoma, undifferentiated carcinoma, and carcinosarcoma are other types of gallbladder cancers. Clear cell carcinoma is rarely seen. In the TNM classification of malignant tumors system the tumor's gallbladder wall or liver tissue invasion degree is classified as T1-4, lymph node involvement of nodes along the cystic duct, common bile duct, hepatic artery or portal vein is classified as N1, and metastases to periaortic, pericaval, superior mesenteric artery or celiac artery lymph node is classified as N2 and whether distant metastasis was present or not is classified as M0, M1 [4,5].
Surgical treatment of gallbladder cancer varies by case. Stage of the disease, tumor localization and whether it was the first identified tumor or recurred tumor are important factors that will decide surgical method. While in some appropriate patients, cholecystectomy is sufficient, some cases may require major operations such as hepatectomy, resection of the bile duct and pancreaticoduodenectomy.
In stage I (T1, N0) gallbladder cancer cases have reported a 100% 5-year survival with only cholecystectomy [2]. Prior to establishing that clear cell carcinoma is a primary gallbladder cancer, it is appropriate to clinically investigate possible secondary focuses, in particular the kidneys in terms of metastasis. McNichols et al., have reported seeing metastasis in 11% of renal cell carcinoma patients after 10 or more years after nephrectomy [3]. In our study, we classified our patient as stage I and performed a laparoscopic cholecystectomy. Our goal in presenting this case was to emphasize the importance of taking an accurate medical history in patients with clear cell carcinoma, a rarely seen gallbladder cancer.
Conflicts of interest
There is no conflict of interest.
Sources of funding
There is no funding.
Ethical approval
Hospital approval was taken.
Consent
Patients approval was taken.
Author contribution
HE, MGB, SB, AI, DF, OC : study concept or design, data collection, data analysis or interpretation, writing the paper.
Guarantor
HE, MGB, SB, AI, DF, OC.
Reference:
- 1.Mehmet Y., Nazif E., Kemal A. Safra kesesi kanserinde tanı ve tedavi: kötü prognoz. Ege Tıp Dergisi. 2005;44(2):107–110. [Google Scholar]
- 2.Bartlett D.L., Fong Y. Gallbladder Cancer. In Hepatobiliary Cancer. In: Blumgart L.H., Fong Y., Jarnagin W.R., editors. B.C. Decker Inc Hamilton; London: 2001. pp. 211–224. [Google Scholar]
- 3.McNichols D.W., Segura J.W., DeWeerd J.H. Renal cell carcinoma: long-term survival and late recurrence. J. Urol. 1981;126:17–23. doi: 10.1016/s0022-5347(17)54359-1. [DOI] [PubMed] [Google Scholar]
- 4.Cem Ç., Ümit S., Gülüm A., Banu B. Safra kesesinin primer karsinoid tümörü. Haseki Tıp Bülteni. 2012;50:107–109. [Google Scholar]
- 5.Edge S.E., Byrd D.R., Compton C.C., Fritz A.G., Greene F.L., Trotti A.I.I.I. 7th ed. NY: Springer; New York: 2010. AJCC Cancer Staging Manual. [Google Scholar]