

Abstract
Background
Blood pressure (BP) trajectories derived from measurements repeated over years have low measurement error and may improve cardiovascular disease prediction compared to single, average, and usual BP (single BP adjusted for regression dilution). We characterized 10‐year BP trajectories and examined their association with cardiovascular mortality, all‐cause mortality, and life years lost.
Methods and Results
Data from 2 prospective and nearly extinct cohorts of middle‐aged men—the Minnesota Business and Professional Men Study (n=261) and the Zutphen Study (n=632)—were used. BP was measured annually during 1947–1957 in Minnesota and 1960–1970 in Zutphen. BP trajectories were identified by latent mixture modeling. Cox proportional hazards and linear regression models examined BP trajectories with cardiovascular mortality, all‐cause mortality, and life years lost. Associations were adjusted for age, serum cholesterol, smoking, and diabetes mellitus. Mean initial age was about 50 years in both cohorts. After 10 years of BP measurements, men were followed until death on average 20 years later. All Minnesota men and 98% of Zutphen men died. Four BP trajectories were identified, in which mean systolic BP increased by 5 to 49 mm Hg in Minnesota and 5 to 20 mm Hg in Zutphen between age 50 and 60. The third systolic BP trajectories were associated with 2 to 4 times higher cardiovascular mortality risk, 2 times higher all‐cause mortality risk, and 4 to 8 life years lost, compared to the first trajectory.
Conclusions
Ten‐year BP trajectories were the strongest predictors, among different BP measures, of cardiovascular mortality, all‐cause mortality, and life years lost in Minnesota. However, average BP was the strongest predictor in Zutphen.
Keywords: blood pressure, cardiovascular disease, epidemiology, prospective cohort study
Introduction
The relation between arterial blood pressure (BP) and cardiovascular disease (CVD) has been investigated in many cohorts. The Prospective Studies Collaboration reported a 1.5 to 2 times higher coronary heart disease mortality risk per 20 mm Hg difference in systolic BP level.1 A previous report from the Seven Countries Study indicated a 1.7 times higher coronary heart disease mortality risk per 20 mm Hg difference in systolic BP level.2 In both studies, BP was based on resting BP obtained on a single occasion in midlife and relative risks were adjusted for regression dilution.3
Compared to single BP assessment adjusted for regression dilution, patterns of BP over time (ie, BP trajectories) may have greater power in predicting CVD.4 In the Minnesota Business and Professional Men Study and the Zutphen Study, BP was recorded annually over a 10‐year period.5–6 The Minnesota Study started in 1947 and the Zutphen Study in 1960, a time in which only exceptionally high levels of BP were treated.7–8 In 2002, the last Minnesota man died and by 2010, 98% of the Zutphen cohort had died. These “extinction” cohorts provide a unique opportunity to study not only the predictive value of BP trajectories in relation to CVD mortality and all‐cause mortality, but also in relation to life years lost.
The aim of the present study was to characterize trajectories of systolic and diastolic BP based on annual resting BP measurements over a 10‐year period and to investigate the association of these BP trajectories with CVD mortality, all‐cause mortality, and life years lost in 2 cohorts of middle‐aged men followed to “extinction.” Moreover, we compared these associations with those of single BP (defined as BP measured at baseline), average BP (defined as the average of all available BP levels during the 10‐year period), and usual BP (defined as single BP adjusted for regression dilution) with CVD mortality, all‐cause mortality, and life years lost.
Methods
Design and Study Populations
An overview of the study design is given in Figure 1. We aimed to replicate the results of the Minnesota cohort in those of the Zutphen cohort. BP was measured annually in the periods 1947–1971 in Minnesota and 1960–1970 in Zutphen. Therefore, a 10‐year period was chosen to model BP trajectories in both cohorts.
Figure 1.
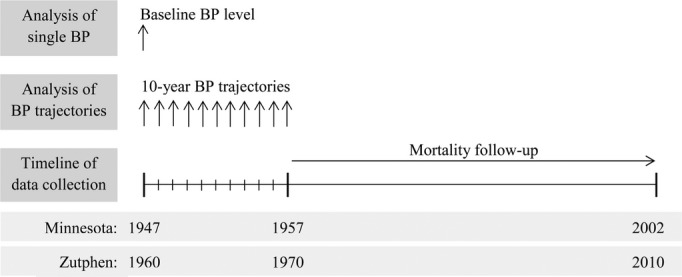
Overview of the study design. The age range at baseline is 45 to 55 years in 1947 in Minnesota and 40 to 60 years in Zutphen. BP indicates blood pressure.
Minnesota Study
In 1947, business and professional men from the upper socioeconomic class who resided in Minneapolis and St. Paul, MN, were recruited for an epidemiologic program to cover 300 men. Detailed information about the study design is described elsewhere.5 In total, 285 clinically healthy men, aged 45 to 55 years, participated in the Minnesota Business and Professional Men Study, subsequently referred to as the Minnesota Study. In the first decade, 15 men died and 4 men had had myocardial infarction; we excluded these men from analysis. No one had a medical history of stroke. In addition, 5 men were excluded for having <5 BP recordings during 1947–1957, leaving 261 men for analysis.
Zutphen Study
In 1960, a longitudinal investigation on coronary heart disease risk factors was begun among middle‐aged men in the town of Zutphen, The Netherlands. Out of 1088 randomly selected men, aged 40 to 60 years, 878 men participated. In the first decade, 118 men died and 55 men had had myocardial infarction or stroke; we excluded these men from analysis. In addition, 73 men were excluded for having <5 BP recordings during 1960–1970, leaving 632 men for analysis.
Oral informed consent was obtained, as was appropriate at baseline in both cohorts, before the Helsinki Declaration was developed.
Data Collection
Minnesota Study
Every year from 1947 through 1957, men were physically examined at the Laboratory of Physiological Hygiene at the University of Minnesota, Minneapolis, MN.5 Men came to the Laboratory in the morning without breakfast and had avoided strenuous activity after waking. BP was recorded with men in the supine position with a mercury sphygmomanometer at the beginning of the examination after at least 10 minutes of rest. BP was recorded 3 times about 5 minutes apart. The mean of these 3 recordings in systole and in the fifth phase of diastole was used for analysis. In total, 2738 recordings from 261 men were available.
Height and weight were measured annually. Serum cholesterol levels were determined with the Bloor method from 1947 through 1953 and then converted to Abell–Kendall values.5,9 Thereafter, Abell–Kendall values were used. Smoking was assessed in 1954 by a questionnaire that included questions that made it possible to reconstruct smoking habits from 1947 onwards. Men were categorized into current former or never smokers. Prevalence of diabetes mellitus was determined by self‐reported physician diagnosis (annually) or fasting glucose with a cutoff point of 7 mmol/L (in 1949 and 1952). A 12‐lead ECG was taken every year and evaluated according to the Minnesota Code.10
Zutphen Study
Every year from 1960 through 1970, men were physically examined according to the protocol of the Seven Countries Study.11 With men in the supine position, BP was recorded with a mercury sphygmomanometer at the end of the examination after at least 5 minutes of rest. Two successive BP recordings were made. The mean of these 2 recordings in systole and in the fifth phase of diastole was used. In total, 6616 recordings from 632 men were available.
Height and weight were measured annually. In 1960 and 1965, serum cholesterol levels were determined with the Abell–Kendall method and in 1970 with the Zlatkis method12 that were converted to Abell–Kendall values.13 Smoking was assessed by the Seven Countries Study questionnaire.11 Men were categorized into current former or nonsmokers. Prevalence of diabetes mellitus was determined by self‐reported physician diagnosis in 1960, 1965, and 1970. A 12‐lead ECG was taken every year and evaluated according to the Minnesota Code.10
Outcome Ascertainment
In both cohorts, men were followed to “extinction.” In Minnesota, mortality follow‐up continued until the last man died in 2002. Mortality information was obtained from death certificates, hospital records, the Minnesota Department of Health, and the National Death Index. In Zutphen, mortality follow‐up continued until July 1, 2010, when 12 men aged 90 to 95 years were still alive. Mortality information was obtained from the municipal population registry, hospital disease registry, general practitioners, and Statistics Netherlands.
Causes of death were adjudicated by an expert in cardiovascular epidemiology (A.M.), according to the International Classification of Diseases (ICD). In Minnesota, CVD mortality included ICD‐9 codes 401‐459 and 798. In Zutphen, CVD mortality included ICD‐8 codes 400‐458 and 795. In the present analysis, mortality follow‐up started 10 years after baseline in both cohorts (Figure 1).
Statistical Analysis
Analyses were done separately for each cohort. Over a 10‐year period, systolic and diastolic BP trajectories were identified by using latent mixture modeling within the PROC TRAJ procedure in SAS.14 This procedure identifies groups of individuals with similar trajectories. We started with a 1‐trajectory model and then fitted those up to the optimal number of trajectories by comparing the Bayesian Information Criterion for each number of trajectories14 and by comparing the number of men per trajectory. Each man was assigned to a trajectory based on the likelihood of correctly classifying men in trajectories (range of mean likelihood across trajectories: 91% to 95%). Linear and quadratic terms were considered and evaluated based on their significance level, starting with the highest polynomial. Age was used as timescale for the trajectories. Because a small fraction of men (<5% in both cohorts) was assigned to the fourth systolic BP trajectories (SBP4), the present study focused on the comparison of the third trajectories (SBP3) with the first trajectories (SBP1).
Cox proportional hazards analysis was used to investigate the association of BP trajectories with risk of CVD and all‐cause mortality. Systolic or diastolic BP trajectories were included as dummy variables in the model using the first BP trajectories (SBP1 and DBP1) as reference.
For all men who had died during follow‐up, age at death was calculated. Linear regression analysis was used to investigate the association between BP trajectories and age at death (which was normally distributed), resulting in the estimated number of life years lost per trajectory compared to mean age at death of the reference trajectory. BP trajectories were included as dummy variables in the model using the first BP trajectories as reference. For the 12 men who were still alive in Zutphen on July 1, 2010, their age in 2010 was used as age at death. Using age plus 3 years (the life expectancy for an average 90‐to‐95‐year‐old man in 2011) instead did not change the results.
In addition to BP trajectories, Cox proportional hazards analysis was used to investigate the association of single BP (BP measured at baseline), average BP (average of all available BP levels during the 10‐year period), and usual BP (single BP adjusted for regression dilution) with risk of CVD and all‐cause mortality. Linear regression analysis was used to investigate the association of single, average, and usual BP with the number of life years lost. Estimates were obtained for each unit difference of 10, 25, and 50 mm Hg systolic BP and 10, 15, and 30 mm Hg diastolic BP. These units were selected because they are similar to the differences in BP level between the reference trajectory and other BP trajectories at age 50 (the mean age at baseline). Average BP level was defined as the mean of all available BP levels during the 10‐year period. We calculated the regression dilution ratio3 from 11 annual BP measurements over the 10‐year period to approximate the underestimate of the strength of the association between usual BP and risk of CVD mortality, all‐cause mortality, and number of life years lost. The Akaike Information Criterion of proportional hazards models (single BP, average BP, and BP trajectories) were compared to investigate the best model fit.
Prediction of CVD mortality, all‐cause mortality, and the number of life years lost by BP trajectories was compared between the 2 cohorts by calculating Z‐scores and corresponding P values. All associations were adjusted for age, serum cholesterol, smoking status, and diabetes mellitus at baseline. Analyses were performed for both cohorts using SAS version 9.2 (SAS Institute, Inc). A 2‐sided P value of <0.05 was considered statistically significant.
Results
Initial mean age was 49.4 years in both cohorts (Table 1). Mean BP level at baseline was 17/16 mm Hg lower in Minnesota than in Zutphen. During 10 years, mean BP level increased by 11/9 mm Hg in Minnesota and 5/0 mm Hg in Zutphen. Mean body mass index was about 25 kg/m2 in both cohorts at baseline and 10 years later. At baseline, mean serum cholesterol level was 23 mg/dL higher in Zutphen, compared to Minnesota, but levels were similar after 10 years. In Minnesota, fewer men were smokers than in Zutphen. In both cohorts, few men were diabetic (<2%).
Table 1.
Characteristics of Men Participating in the Minnesota Study and the Zutphen Study at the First and Last Year of the BP Trajectory
| Minnesota Study | Zutphen Study | |||
|---|---|---|---|---|
| 1947 | 1957 | 1960 | 1970 | |
| N | 261 | 231 | 632 | 568 |
| Age, y | 49.4 (2.8) | 59.4 (2.8) | 49.4 (5.4) | 59.5 (5.4) |
| Height, cm | 176.0 (6.2) | 175.8 (6.3) | 173.7 (6.6) | 173.8 (6.6) |
| Weight, kg | 76.3 (12.1) | 78.1 (11.5)* | 72.6 (9.5) | 76.0 (9.5)† |
| BMI, kg/m2 | 24.6 (3.6) | 25.3 (3.4)* | 24.0 (2.7) | 25.1 (2.7)† |
| Systolic BP, mm Hg | 124.1 (15.4)‡ | 134.8 (22.2) | 141.4 (18.5)§ | 146.1 (20.2)‖ |
| Diastolic BP, mm Hg | 73.0 (10.9)‡ | 81.6 (11.6) | 89.0 (11.8)¶ | 88.9 (11.5)‖ |
| Serum cholesterol, mg/dL | 209.4 (33.6)‡ | 234.4 (38.5)* | 232.7 (43.6)** | 237.6 (42.4) |
| Current smoking, N (%) | 147 (56.3%)* | 103 (44.6%)* | 499 (74.3%) | 304 (54.3%)†† |
| Diabetes mellitus, N (%) | 0 (0.0%) | 4 (1.7%) | 6 (0.9%) | 10 (1.8%) |
Values are means (SD) unless stated otherwise. BMI indicates body mass index; BP, blood pressure.
Data are available for *229 men, †565 men, ‡259 men, §629 men, ‖567 men, ¶628 men, **599 men, and ††560 men.
Smoking was assessed in 1954 by an extensive questionnaire that included questions about smoking history that made it possible to reconstruct the smoking habits in 1947. Smoking habits in 1954 were used as a proxy for those in 1957.
Four trajectories of systolic BP (SBP1 to SBP4) and diastolic BP (DBP1 to DBP4) were identified in both cohorts (Figure 2). Trajectories consisted of increasing BP levels fanning out with age, that is, BP increased more rapidly in men with higher initial BP levels. Mean systolic BP of the 4 trajectories increased by 5 to 49 mm Hg in Minnesota and 5 to 20 in Zutphen from age 50 to 60. For diastolic BP, these 10‐year increases were 6 to 26 mm Hg in Minnesota and 2 to 12 mm Hg in Zutphen.
Figure 2.
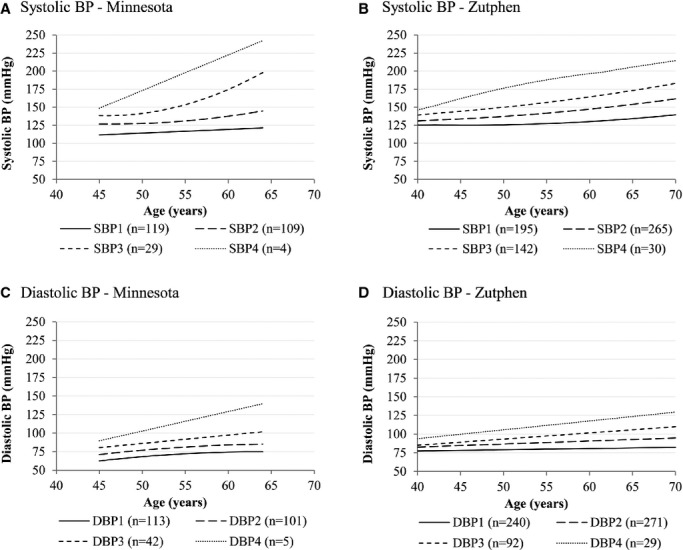
Trajectories of systolic (A, B) and diastolic (C, D) BP in 261 American men participating in the Minnesota Study and 632 Dutch men participating in the Zutphen Study. DBP indicates diastolic blood pressure; SBP, systolic blood pressure.
During a mean (±SD) follow‐up of 20.9±10.0 years, all Minnesota men had died, of whom 137 (52.5%) died from CVD. During a mean follow‐up of 18.8±9.6 years, 623 Zutphen men had died (98.1%), of whom 282 (44.6%) died from CVD. In both cohorts, CVD mortality rate was ≈25 per 1000 person‐years and all‐cause mortality rate was ≈50 per 1000 person‐years. Mean age at death was 79.7±9.5 years in Minnesota and 78.3±8.8 years in Zutphen.
Systolic BP was directly associated with CVD mortality (Tables 2 and 3). This association was more pronounced in Minnesota than in Zutphen. After adjustment, the third systolic BP trajectory, SBP3, was associated with a CVD mortality risk ratio of 3.8 (95% CI: 2.2 to 6.6) in Minnesota and 2.1 (95% CI: 1.5 to 2.9) in Zutphen, compared to the first trajectory (Table 2). For SBP3, hazard ratios were significantly higher in Minnesota than in Zutphen (P=0.03) (Table 4). Each unit difference of 25 mm Hg systolic BP was associated with a CVD mortality risk ranging from 1.5 for single BP to 1.6 for usual BP in Minnesota and from 1.3 for single BP to 1.7 for average BP in Zutphen (Table 3). Similar patterns were found for diastolic BP. In addition to CVD mortality, systolic BP was directly associated with all‐cause mortality (Tables 5 and 6). BP trajectories were the strongest predictors of CVD and all‐cause mortality in Minnesota, whereas in Zutphen, average BP was the strongest predictor (Table 7).
Table 2.
Hazard Ratios (95% CI) for Risk of CVD Mortality Per Trajectory of Systolic and Diastolic BP in the Minnesota Study and the Zutphen Study
| Minnesota Study (n=261) | Zutphen Study (n=632) | |||||||
|---|---|---|---|---|---|---|---|---|
| N | Unadjusted | Age‐adjusted* | Fully adjusted** | N | Unadjusted | Age‐adjusted* | Fully adjusted** | |
| N cases CVD mortality (%) | 137 (52.5%) | 282 (44.6%) | ||||||
| Sum of person‐years | 5448 | 11912 | ||||||
| N cases/1000 person‐years | 25.1 | 23.7 | ||||||
| Systolic BP trajectories | ||||||||
| SBP1 | 119 | Reference | Reference | Reference | 195 | Reference | Reference | Reference |
| SBP2 | 109 | 1.68 (1.16 to 2.43) | 1.87 (1.28 to 2.72) | 1.82 (1.25 to 2.66) | 265 | 1.15 (0.86 to 1.54) | 1.38 (1.03 to 1.86) | 1.34 (1.00 to 1.81) |
| SBP3 | 29 | 3.11 (1.82 to 5.30) | 3.91 (2.26 to 6.74) | 3.80 (2.18 to 6.64) | 142 | 1.56 (1.13 to 2.15) | 2.13 (1.53 to 2.97) | 2.05 (1.47 to 2.87) |
| SBP4 | 4 | 4.35 (1.35 to 14.04) | 2.99 (0.92 to 9.75) | 3.95 (1.17 to 13.38) | 30 | 1.97 (1.15 to 3.39) | 3.06 (1.76 to 5.33) | 3.05 (1.74 to 5.33) |
| Diastolic BP trajectories | ||||||||
| DBP1 | 113 | Reference | Reference | Reference | 240 | Reference | Reference | Reference |
| DBP2 | 101 | 1.13 (0.78 to 1.65) | 1.33 (0.90 to 1.95) | 1.34 (0.90 to 1.98) | 271 | 1.19 (0.91 to 1.56) | 1.39 (1.06 to 1.82) | 1.35 (1.02 to 1.78) |
| DBP3 | 42 | 1.63 (1.01 to 2.64) | 2.09 (1.27 to 3.43) | 2.10 (1.26 to 3.49) | 92 | 1.16 (0.80 to 1.66) | 1.69 (1.16 to 2.46) | 1.66 (1.14 to 2.43) |
| DBP4 | 5 | 3.67 (1.32 to 10.17) | 3.10 (1.11 to 8.65) | 4.07 (1.42 to 11.63) | 29 | 2.17 (1.31 to 3.61) | 3.61 (2.13 to 6.10) | 3.68 (2.16 to 6.26) |
CVD indicates cardiovascular disease; DBP, diastolic blood pressure; SBP, systolic blood pressure.
Adjusted for age.
Adjusted for age, serum cholesterol, smoking status, and diabetes mellitus.
Missing values for serum cholesterol at baseline were replaced by serum cholesterol levels measured at the consecutive year.
Table 3.
Hazard Ratios* (95% CI) for CVD Mortality Risk Per Single BP Unit Difference* in the Minnesota Study and Zutphen Study
| Minnesota Study (n=261) | Zutphen Study (n=632) | |||||
|---|---|---|---|---|---|---|
| Single BP* | Average BP* | Usual BP* | Single BP* | Average BP* | Usual BP* | |
| Baseline systolic BP | ||||||
| Per 10 mm Hg | 1.17 (1.06 to 1.28) | 1.17 (1.08 to 1.27) | 1.22 | 1.12 (1.06 to 1.19) | 1.24 (1.15 to 1.34) | 1.17 |
| Per 25 mm Hg | 1.47 (1.16 to 1.86) | 1.49 (1.22 to 1.82) | 1.62 | 1.34 (1.16 to 1.54) | 1.72 (1.43 to 2.08) | 1.50 |
| Per 50 mm Hg | 2.16 (1.35 to 3.45) | 2.22 (1.49 to 3.33) | 2.64 | 1.78 (1.34 to 2.38) | 2.96 (2.03 to 4.32) | 2.23 |
| Baseline diastolic BP | ||||||
| Per 10 mm Hg | 1.18 (1.02 to 1.37) | 1.29 (1.10 to 1.50) | 1.28 | 1.14 (1.03 to 1.26) | 1.40 (1.20 to 1.62) | 1.24 |
| Per 15 mm Hg | 1.28 (1.03 to 1.60) | 1.46 (1.16 to 1.83) | 1.44 | 1.21 (1.04 to 1.41) | 1.65 (1.32 to 2.07) | 1.37 |
| Per 30 mm Hg | 1.64 (1.06 to 2.55) | 2.12 (2.12 to 3.37) | 2.08 | 1.47 (1.08 to 1.99) | 2.73 (1.74 to 4.27) | 1.89 |
BP indicates blood pressure; CVD, cardiovascular disease.
Adjusted for age, serum cholesterol, smoking status, and diabetes mellitus. Missing values for serum cholesterol at baseline were replaced by serum cholesterol levels measured at the consecutive year.
Differences in single BP level are similar to the differences in BP level between the reference trajectory (SBP1) and other BP trajectories at age 50, which is the mean age at baseline.
Defined as BP level measured at baseline.
Defined as the average of all available BP levels during the 10‐year period.
Defined as single BP adjusted for regression dilution. Adjustment factors were 1.26 for systolic and 1.48 for diastolic BP in the Minnesota Study and 1.39 for systolic and 1.65 for diastolic BP in the Zutphen Study.
Table 4.
Comparison of Associations of Systolic BP Trajectories With CVD Mortality, All‐Cause Mortality, and Life Years Lost Between Minnesota and Zutphen
| Minnesota Study | Zutphen Study | Z Score | P Value | |
|---|---|---|---|---|
| CVD mortality, HR (95% CI) | ||||
| SBP2 | 1.82 (1.25 to 2.66) | 1.34 (1.00 to 1.81) | −1.27 | 0.10 |
| SBP3 | 3.80 (2.18 to 6.64) | 2.05 (1.47 to 2.87) | −1.87 | 0.03 |
| SBP4 | 3.95 (1.17 to 13.38) | 3.05 (1.74 to 5.33) | −0.40 | 0.34 |
| All‐cause mortality, HR (95% CI) | ||||
| SBP2 | 1.44 (1.10 to 1.88) | 1.12 (0.93 to 1.36) | −1.47 | 0.07 |
| SBP3 | 2.48 (1.62 to 3.79) | 1.54 (1.23 to 1.93) | −1.93 | 0.03 |
| SBP4 | 2.45 (0.88 to 6.86) | 2.44 (1.64 to 3.62) | −0.01 | 0.50 |
| Number of life years lost, years (95% CI) | ||||
| SBP2 | 3.06 (0.68 to 5.43) | 1.07 (−0.53 to 2.67) | −1.62 | 0.05 |
| SBP3 | 8.10 (4.39 to 11.82) | 3.68 (1.80 to 5.56) | −2.32 | 0.01 |
| SBP4 | 12.75 (3.74 to 21.77) | 6.42 (3.11 to 9.74) | −1.38 | 0.08 |
CVD indicates cardiovascular disease; HR, hazard ratio; SBP, systolic blood pressure.
Table 5.
Hazard Ratios (95% CI) for Risk of All‐Cause Mortality Per Trajectory of Systolic and Diastolic BP in the Minnesota Study and the Zutphen Study
| Minnesota Study (n=261) | Zutphen Study (n=632) | |||||||
|---|---|---|---|---|---|---|---|---|
| N | Unadjusted | Age‐adjusted* | Fully adjusted** | N | Unadjusted | Age‐adjusted* | Fully adjusted** | |
| N cases all‐cause mortality (%) | 261 (100%) | 620 (98.1%) | ||||||
| Sum of person‐years | 5448 | 11912 | ||||||
| N cases/1000 person‐years | 47.9 | 52.0 | ||||||
| Systolic BP trajectories | ||||||||
| SBP1 | 119 | Reference | Reference | Reference | 195 | Reference | Reference | Reference |
| SBP2 | 109 | 1.34 (1.03 to 1.74) | 1.48 (1.14 to 1.93) | 1.44 (1.10 to 1.88) | 265 | 0.93 (0.77 to 1.12) | 1.12 (0.93 to 1.36) | 1.12 (0.93 to 1.36) |
| SBP3 | 29 | 2.14 (1.42 to 3.23) | 3.91 (1.73 to 4.01) | 2.48 (1.62 to 3.79) | 142 | 1.15 (0.92 to 1.43) | 1.57 (1.25 to 1.96) | 1.54 (1.23 to 1.93) |
| SBP4 | 4 | 2.71 (1.00 to 7.36) | 1.91 (0.70 to 5.24) | 2.45 (0.88 to 6.86) | 30 | 1.47 (1.00 to 2.17) | 2.32 (1.56 to 3.43) | 2.44 (1.64 to 3.62) |
| Diastolic BP trajectories | ||||||||
| DBP1 | 113 | Reference | Reference | Reference | 240 | Reference | Reference | Reference |
| DBP2 | 101 | 1.08 (0.83 to 1.42) | 1.26 (0.96 to 1.66) | 1.24 (0.94 to 1.64) | 271 | 0.91 (0.77 to 1.09) | 1.05 (0.88 to 1.26) | 1.04 (0.87 to 1.25) |
| DBP3 | 42 | 1.44 (1.01 to 2.06) | 1.83 (1.27 to 2.64) | 1.75 (1.21 to 2.55) | 92 | 0.85 (0.67 to 1.09) | 1.24 (0.96 to 1.60) | 1.22 (0.95 to 1.58) |
| DBP4 | 5 | 2.42 (0.99 to 5.95) | 2.05 (0.83 to 5.05) | 2.55 (1.02 to 6.38) | 29 | 1.36 (0.93 to 2.01) | 2.24 (1.51 to 3.33) | 2.38 (1.59 to 3.54) |
DBP indicates diastolic blood pressure; SBP, systolic blood pressure.
Adjusted for age.
Adjusted for age, serum cholesterol, smoking status, and diabetes mellitus.
Missing values for serum cholesterol at baseline were replaced by serum cholesterol levels measured at the consecutive year.
Table 6.
Hazard Ratios* (95% CI) for All‐Cause Mortality Risk Per Single BP Unit Difference* in the Minnesota Study and Zutphen Study
| Minnesota Study (n=261) | Zutphen Study (n=632) | |||||
|---|---|---|---|---|---|---|
| Single BP* | Average BP* | Usual BP* | Single BP* | Average BP* | Usual BP* | |
| Baseline systolic BP | ||||||
| Per 10 mm Hg | 1.10 (1.02 to 1.18) | 1.13 (1.06 to 1.20) | 1.13 | 1.08 (1.04 to 1.13) | 1.16 (1.10 to 1.23) | 1.11 |
| Per 25 mm Hg | 1.26 (1.05 to 1.52) | 1.34 (1.14 to 1.58) | 1.34 | 1.21 (1.09 to 1.35) | 1.46 (1.27 to 1.68) | 1.30 |
| Per 50 mm Hg | 1.60 (1.11 to 2.30) | 1.80 (1.31 to 2.48) | 1.81 | 1.47 (1.19 to 1.82) | 1.71 (1.24 to 2.37) | 1.71 |
| Baseline diastolic BP | ||||||
| Per 10 mm Hg | 1.14 (1.02 to 1.27) | 1.23 (1.09 to 1.38) | 1.21 | 1.08 (1.01 to 1.16) | 1.20 (1.08 to 1.33) | 1.14 |
| Per 15 mm Hg | 1.21 (1.03 to 1.42) | 1.36 (1.14 to 1.62) | 1.33 | 1.12 (1.01 to 1.24) | 1.31 (1.11 to 1.54) | 1.21 |
| Per 30 mm Hg | 1.47 (1.06 to 2.03) | 1.86 (1.31 to 2.64) | 1.77 | 1.25 (1.01 to 1.55) | 1.71 (1.24 to 2.37) | 1.45 |
BP indicates blood pressure; CI, confidence interval; CVD, cardiovascular disease; SBP, systolic blood pressure.
Adjusted for age, serum cholesterol, smoking status, and diabetes mellitus. Missing values for serum cholesterol at baseline were replaced by serum cholesterol levels measured at the consecutive year.
Differences in single BP level are similar to the differences in BP level between the reference trajectory (SBP1) and other BP trajectories at age 50, which is the mean age at baseline.
Defined as BP level measured at baseline.
Defined as the average of all available BP levels during the 10‐year period.
Defined as single BP adjusted for regression dilution. Adjustment factors were 1.26 for systolic and 1.48 for diastolic BP in the Minnesota Study and 1.39 for systolic and 1.65 for diastolic BP in the Zutphen Study.
Table 7.
Comparison of the Akaike Information Criterion*, a Measure of the Model Fit, for Each Proportional Hazards Model of Systolic BP*
| Minnesota Study | Zutphen Study | |
|---|---|---|
| CVD mortality | ||
| Single systolic BP | 1251 | 3126 |
| Average systolic BP | 1248 | 3111 |
| Systolic BP trajectories | 1239 | 3119 |
| All‐cause mortality | ||
| Single systolic BP | 2379 | 6761 |
| Average systolic BP | 2374 | 6747 |
| Systolic BP trajectories | 2370 | 6750 |
The lower the Akaike Information Criterion (AIC), the better the model fit.
The AIC was not obtained for usual blood pressure (BP), because for usual BP single BP was adjusted for regression dilution.
Systolic BP was directly associated with life years lost (Tables 8 and 9). This association was more pronounced in Minnesota than in Zutphen. After adjustment, the number of life years lost associated with SBP3 was 8.1 (95% CI: 4.4 to 11.8) years in Minnesota and 3.7 (95% CI: 1.8 to 5.6) years in Zutphen (Table 8). For SBP3, the number of life years lost were significantly higher in Minnesota than in Zutphen (P=0.01) (Table 3). The number of life years lost associated with each 25 mm Hg difference in systolic BP ranged from 2.9 for single BP to 3.9 for average BP in Minnesota and from 1.7 for single BP to 2.9 for average BP in Zutphen (Table 9). Similar patterns were found for diastolic BP.
Table 8.
Life Years Lost (Years)* (95% CI) per Trajectory of Systolic and Diastolic BP in the Minnesota Study and the Zutphen Study
| Minnesota Study (n=261) | Zutphen Study (n=632) | |||||||
|---|---|---|---|---|---|---|---|---|
| N | Unadjusted | Age‐adjusted* | Fully adjusted** | N | Unadjusted | Age‐adjusted* | Fully adjusted** | |
| Age at death, y | 79.6±9.6 | 78.3±8.8 | ||||||
| Systolic BP trajectories | ||||||||
| SBP1 | 119 | Reference | Reference | Reference | 195 | Reference | Reference | Reference |
| SBP2 | 109 | 3.29 (0.89 to 5.69) | 3.35 (0.92 to 5.77) | 3.06 (0.68 to 5.43) | 265 | 1.32 (−0.27 to 2.91) | 0.97 (−0.63 to 2.57) | 1.07 (−0.53 to 2.67) |
| SBP3 | 29 | 8.54 (4.79 to 12.29) | 8.61 (4.84 to 12.39) | 8.10 (4.39 to 11.82) | 142 | 4.15 (2.29 to 6.01) | 3.69 (1.82 to 5.56) | 3.68 (1.80 to 5.56) |
| SBP4 | 4 | 11.88 (2.67 to 21.08) | 11.96 (2.72 to 21.19) | 12.75 (3.74 to 21.77) | 30 | 6.69 (3.39 to 10.00) | 6.07 (2.75 to 9.38) | 6.42 (3.11 to 9.74) |
| Diastolic BP trajectories | ||||||||
| DBP1 | 113 | Reference | Reference | Reference | 240 | Reference | Reference | Reference |
| DBP2 | 101 | 2.28 (−0.24 to 4.79) | 2.45 (−0.11 to 5.02) | 2.28 (−0.25 to 4.82) | 271 | 0.84 (−0.67 to 2.35) | 0.48 (−1.04 to 2.00) | 0.55 (−0.97 to 2.07) |
| DBP3 | 42 | 6.01 (2.69 to 9.34) | 6.25 (2.86 to 9.65) | 5.80 (2.46 to 9.14) | 92 | 2.37 (−0.28 to 4.45) | 1.67 (−0.45 to 3.79) | 1.77 (−0.35 to 3.89) |
| DBP4 | 5 | 11.08 (2.68 to 19.49) | 11.40 (2.94 to 19.86) | 11.61 (3.36 to 19.86) | 29 | 6.68 (3.33 to 10.02) | 5.84 (2.48 to 9.21) | 6.37 (3.00 to 9.75) |
DBP indicates diastolic blood pressure; SBP, systolic blood pressure.
The number of life years lost is based on the age at death.
Adjusted for age.
Adjusted for age, serum cholesterol, smoking status, and diabetes mellitus.
Missing values for serum cholesterol at baseline were replaced by serum cholesterol levels measured at the consecutive year.
Table 9.
Life Years Lost (Years)** (95% CI) Per Single BP Unit Difference* in the Minnesota Study and Zutphen Study
| Cohort | ||||||
|---|---|---|---|---|---|---|
| Minnesota Study (n=261) | Zutphen Study (n=632) | |||||
| Single BP* | Average BP* | Usual BP* | Single BP* | Average BP* | Usual BP* | |
| Age at death, y | 79.7±9.5 | 78.3±8.8 | ||||
| Baseline systolic BP | ||||||
| Per 10 mm Hg | 1.16 (0.42 to 1.89) | 1.54 (0.84 to 2.25) | 1.46 | 0.66 (0.29 to 1.03) | 1.16 (0.71 to 1.62) | 0.92 |
| Per 25 mm Hg | 2.89 (1.05 to 4.73) | 3.86 (2.10 to 5.62) | 3.64 | 1.65 (0.73 to 2.57) | 2.91 (1.78 to 4.04) | 2.29 |
| Per 50 mm Hg | 5.79 (2.11 to 9.47) | 7.71 (4.19 to 11.23) | 7.30 | 3.30 (1.47 to 5.13) | 5.82 (3.56 to 8.08) | 4.59 |
| Baseline diastolic BP | ||||||
| Per 10 mm Hg | 1.58 (0.54 to 2.62) | 2.64 (1.39 to 3.88) | 2.34 | 0.68 (0.10 to 1.27) | 1.51 (0.67 to 2.35) | 1.12 |
| Per 15 mm Hg | 2.37 (0.80 to 3.93) | 3.95 (2.09 to 5.82) | 3.51 | 1.03 (0.15 to 1.90) | 2.26 (1.01 to 3.52) | 1.70 |
| Per 30 mm Hg | 4.73 (1.61 to 7.86) | 7.91 (4.18 to 11.63) | 7.00 | 2.05 (0.30 to 3.80) | 4.53 (2.02 to 7.04) | 3.38 |
BP indicates blood pressure; SBP, systolic blood pressure.
The number of life years lost are based on the age at death.
Adjusted for age, serum cholesterol, smoking status, and diabetes mellitus. Missing values for serum cholesterol at baseline were replaced by serum cholesterol levels measured at the consecutive year.
Differences in single BP level are similar to the differences in BP level between the reference trajectory (SBP1) and other BP trajectories at age 50, which is the mean age at baseline.
Defined as BP level measured at baseline.
Defined as the average of all available BP levels during the 10‐year period.
Defined as single BP adjusted for regression dilution. Adjustment factors were 1.26 for systolic and 1.48 for diastolic BP in the Minnesota Study and 1.39 for systolic and 1.65 for diastolic BP in the Zutphen Study.
Discussion
In 1 extinct cohort of American middle‐aged men and 1 nearly extinct cohort of Dutch middle‐aged men, 10‐year BP trajectories were identified that were strong predictors of CVD mortality, all‐cause mortality, and life years. Compared to other BP measures, 10‐year BP trajectories were the strongest predictors of mortality in Minnesota. In Zutphen, however, average BP was the strongest predictor of mortality. The third systolic BP trajectory was associated with 4 times greater CVD mortality risk in Minnesota and 2 times greater risk in Zutphen, compared to the first trajectory. In both cohorts, these trajectories were associated with a 2 times greater risk of all‐cause mortality. The number of life years lost between these trajectories was 8 years in Minnesota and 4 years in Zutphen.
In this study, mean initial BP level in Minnesota was lower than in Zutphen. This finding was confirmed by a study in which BP levels in the Minnesota Study were compared to those in other American cohorts.15 An explanation for these lower BP levels may be that measured BP in Minnesota was closer to basal BP levels because 3 consecutive measurements of BP separated by 5 minutes each were taken after a long period of rest. Moreover, the Minnesota Study involved highly educated men who were selected for health, whereas the Zutphen Study involved a random population sample of Zutphen inhabitants.
Although BP levels were lower in Minnesota than in Zutphen, we observed relatively similar BP trajectories in both cohorts. In all 4 trajectories, BP levels increased more rapidly in men with higher initial levels. In Minnesota, these increases were more rapid than in Zutphen. For example, from age 50 through 60, mean systolic BP of the 4 trajectories increased by 5 to 49 mm Hg in Minnesota and 5 to 20 mm Hg in Zutphen. In the Framingham Heart Study, 4 trajectories were identified in 890 men aged 30 to 84 years with a maximum of 15 BP measurements per person. Systolic BP rose linearly by 5 to 23 mm Hg per 10 years within all 4 trajectories.16 These findings were similar to those observed in Zutphen, but the associations between trajectories and cardiovascular outcomes were not investigated.
The CARDIA study recently demonstrated that higher BP trajectories from young adulthood through middle age were associated with an increased risk of coronary artery calcification, a marker of subclinical atherosclerosis.4 In our study, higher BP trajectories from middle age through old age were associated with a higher risk of CVD mortality. Since the present study focuses on middle through old age, these findings complement those of the younger CARDIA population. Moreover, the association of BP trajectories with a mortality end point, rather than a marker of CVD, was investigated in the present study.
Our findings regarding life years lost are in line with those of the Framingham Heart Study. In that study, normotensive men were expected to live 1.7 years longer than prehypertensive men and 5.1 years longer than hypertensive men.17 The second trajectory in our study, which is comparable to the prehypertensive group in the Framingham Heart Study, was associated with 1.1 (Zutphen) to 3.1 (Minnesota) life years lost compared with the first trajectories. The third trajectory, which is comparable to the hypertensive group, was associated with 3.7 (Zutphen) to 8.1 (Minnesota) life years lost. Although similar results were observed, it should be noted that life expectancy was the outcome of the Framingham Heart Study, whereas life years lost that are based on the actual age at death was the outcome of the present study.
Due to random‐within person variation in BP, the strength of the association between BP obtained on a single occasion and mortality will be underestimated. By taking the average BP or adjusting for regression dilution (usual BP), associations with CVD mortality, all‐cause mortality and life years lost became stronger compared to single BP. Associations regarding BP trajectories were about twice as strong as compared to single BP. The number of life years lost according to BP trajectories was twice as high in Minnesota than in Zutphen. Moreover, we observed that BP trajectories were stronger predictors of mortality than single, average, and usual BP in Minnesota. In Zutphen, however, average BP was the strongest predictor of mortality. BP was based on 3 recordings with longer time intervals in Minnesota and on 2 recordings with shorter time intervals in Zutphen. Therefore, BP may be measured less accurately in Zutphen than in Minnesota, which has led to less valid BP trajectories in Zutphen. Another explanation could be that BP trajectories in Zutphen are quite linear, which is also captured by average BP. Therefore, the model with a long‐term continuous BP variable (average BP) was superior to the model with categorical BP variables (BP trajectories) in terms of model fit. These findings indicate that measuring BP accurately is crucial for estimating the association between BP and mortality.
Cumulative BP levels over time (eg, patterns of BP) are not taken into account in recommendations for management of hypertension. In individuals younger than 60 years, the current recommendation is to start pharmacologic treatment at BP levels of ≥140 mm Hg systolic or ≥90 mm Hg diastolic.18 An individual's BP pattern before reaching this BP cut‐off level is not included in these recommendations. Our findings emphasize the importance of taking BP increases during time into account. Increases in BP seem especially important in the group that does not yet reach the treatment cut‐off level of 140/90 mm Hg. We observed that the first trajectories, in which systolic BP increased from 114 to 121 mm Hg in Minnesota and 125 to 130 mm Hg in Zutphen from age 50 through 60, were the most favorable in terms of life years lost and risk of CVD and all‐cause mortality. Trajectories starting at a systolic BP level of 127 mm Hg in Minnesota and 137 mm Hg in Zutphen at age 50 and increasing with 10 mm Hg until age 60 were associated with a 30% to 80% greater risk of CVD mortality, a 10% to 40% greater risk of all‐cause mortality and 1.1 to 3.1 life years lost, compared with the first trajectories. These findings suggest that regularly monitoring BP of middle‐aged men who have a BP level between 130 to 140 mm Hg is important, as these men are usually not treated but already have an increased risk of CVD mortality. Monitoring BP in this group provides the opportunity to detect hypertension and prevent CVD earlier in life. Moreover, our findings show that average BP is superior to single BP in terms of mortality prediction. For clinical settings, this implies that a BP level based on multiple annual BP recordings is a stronger predictor than a BP level based on a few recordings at a single moment in time.
A major strength of the present study is that detailed data on BP during a long follow‐up period were collected in both cohorts. Almost everyone had died at the end of follow‐up, which enabled us to investigate the association of BP trajectories with life years lost. A mean of 10 (out of 11) BP measurements per person was included to characterize 10‐year BP trajectories, which indicates that the majority of men had complete BP data. Because cohorts were initiated in a time when only very high levels of BP were treated, it is unlikely that the observed associations are confounded by antihypertensive medication. A drawback of the present study is that the characterization of BP trajectories is complex. It is too time‐consuming to use BP trajectories as a predictive tool in clinical settings. However, our findings on average BP and mortality emphasize the importance of repeated BP measurements from middle into old age, which is relevant for clinicians. Another drawback is the small number of participants. Few men were assigned to the fourth BP trajectories, which warrants cautious interpretation for these specific findings. It should be noted that the Minnesota men were all from the upper socioeconomic class in the metropolitan area of Minneapolis, St. Paul, which could limit the generalizability of these findings. However, we observed similar findings in the population‐based Zutphen Study, which included more men with large differences in socioeconomic class.
Perspectives
In 2 cohorts of American and Dutch middle‐aged men, 4 10‐year BP trajectories were characterized. BP trajectories were stronger predictors of CVD mortality, all‐cause mortality, and life years lost than single, average, and usual BP in Minnesota, but not in Zutphen. In general, we observed similar associations within these cohorts, emphasizing the replication of the results of 1 cohort in the other. To our knowledge, this is the first study that investigated the association of BP trajectories with CVD mortality, all‐cause mortality, and life years lost. The novel approach of using data from cohorts in which participants were physically examined and followed to “extinction” provided a unique opportunity to study the association of risk factors in relation to cardiovascular health and life years lost.
Sources of Funding
The contribution to this work of Susanne M. A. J. Tielemans, Sabita S. Soedamah‐Muthu, and Daan Kromhout was funded by the Royal Netherlands Academy of Arts and Sciences.
Disclosures
None.
References
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins RProspective Studies Collaboration. Age‐specific relevance of usual blood pressure to vascular mortality: a meta‐analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002; 360:1903-1913. [DOI] [PubMed] [Google Scholar]
- van den Hoogen PC, Feskens EJ, Nagelkerke NJ, Menotti A, Nissinen A, Kromhout D. The relation between blood pressure and mortality due to coronary heart disease among men in different parts of the world. Seven countries study research group. N Engl J Med. 2000; 342:1-8. [DOI] [PubMed] [Google Scholar]
- Clarke R, Shipley M, Lewington S, Youngman L, Collins R, Marmot M, Peto R. Underestimation of risk associations due to regression dilution in long‐term follow‐up of prospective studies. Am J Epidemiol. 1999; 150:341-353. [DOI] [PubMed] [Google Scholar]
- Allen NB, Siddique J, Wilkins JT, Shay C, Lewis CE, Goff DC, Jacobs DR, Jr, Liu K, Lloyd‐Jones D. Blood pressure trajectories in early adulthood and subclinical atherosclerosis in middle age. JAMA. 2014; 311:490-497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keys A, Taylor HL, Blackburn H, Brozek J, Anderson JT, Simonson E. Coronary heart disease among Minnesota business and professional men followed fifteen years. Circulation. 1963; 28:381-395. [DOI] [PubMed] [Google Scholar]
- Keli S, Bloemberg B, Kromhout D. Predictive value of repeated systolic blood pressure measurements for stroke risk: The Zutphen study. Stroke. 1992; 23:347-351. [DOI] [PubMed] [Google Scholar]
- Law MR, Watt HC, Wald NJ. The underlying risk of death after myocardial infarction in the absence of treatment. Arch Intern Med. 2002; 162:2405-2410. [DOI] [PubMed] [Google Scholar]
- Mahmood SS, Levy D, Vasan RS, Wang TJ. The Framingham Heart Study and the epidemiology of cardiovascular disease: a historical perspective. Lancet. 2014; 383:999-1008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abel LL, Levy BB, Brodie BB, Kendall FE. A simplified method for the estimation of total cholesterol in serum and demonstration of its specificity. J Biol Chem. 1952; 195:357-366. [PubMed] [Google Scholar]
- Rose GA, Blackburn H. Cardiovascular Survey Methods1968. 137-154. [PubMed] [Google Scholar]
- Keys A, Aravanis C, Blackburn HW, Van Buchem FS, Buzina R, Djordjevic BD, Dontas AS, Fidanza F, Karvonen MJ, Kimura N, Lekos D, Monti M, Puddu V, Taylor HL. Epidemiological studies related to coronary heart disease: characteristics of men aged 40‐59 in seven countries. Acta Med Scand. 1966; 460suppl:1-392. [PubMed] [Google Scholar]
- Zlatkis A, Zak B, Boyle AJ. A new method for the direct determination of serum cholesterol. J Lab Clin Med. 1953; 41:486-492. [PubMed] [Google Scholar]
- Kromhout D. Body weight, diet, and serum cholesterol in 871 middle‐aged men during 10 years of follow‐up (the Zutphen study). Am J Clin Nutr. 1983; 38:591-598. [DOI] [PubMed] [Google Scholar]
- Jones BL, Nagin DS, Roeder K. A SAS procedure based on mixture models for estimating developmental trajectories. Soc Methods Res. 2001; 29:374-393. [Google Scholar]
- The Pooling Project Research Group. Relationship of blood pressure, serum cholesterol, smoking habit, relative weight and ECG abnormalities to incidence of major coronary events: final report of the pooling project. J Chronic Dis. 1978; 31:201-306. [DOI] [PubMed] [Google Scholar]
- Franklin SS, Gustin WT, Wong ND, Larson MG, Weber MA, Kannel WB, Levy D. Hemodynamic patterns of age‐related changes in blood pressure. The Framingham Heart Study. Circulation. 1997; 96:308-315. [DOI] [PubMed] [Google Scholar]
- Franco OH, Peeters A, Bonneux L, de Laet C. Blood pressure in adulthood and life expectancy with cardiovascular disease in men and women: life course analysis. Hypertension. 2005; 46:280-286. [DOI] [PubMed] [Google Scholar]
- James PA, Oparil S, Carter BL, Cushman WC, Dennison‐Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC, Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT, Jr, Narva AS, Ortiz E. 2014 evidence‐based guideline for the management of high blood pressure in adults: report from the panel members appointed to the eighth joint national committee (JNC 8). JAMA. 2014; 311:507-520. [DOI] [PubMed] [Google Scholar]