

Abstract
Objective:
This study was conducted to investigate the relationship between the intake of different food groups by pregnant mothers and neonatal low birth weight and premature births.
Materials and Methods:
In this cohort, the target population was 225 pregnant women, randomly selected from different geographical areas of the city of Isfahan, Iran (from April to September, 2012). The main variables in the study were weight and gestational age of the neonates and the type and amount of different food groups used by the mothers. All nutritional variables were compared according to different groups of infants (normal, premature, and low birth weight). In the multivariate analysis, multiple linear and logistic regression models were used to identify those different food frequency questionnaire (FFQ) variables independently associated with the newborn's weight and gestational age, adjusted by maternal consumption of calcium supplementation, folic acid, and omega-3, during pregnancy.
Results:
A total of 214 (47.7% boys) infants with complete information were included. They had a mean gestational age of 38.72 ± 1.2 weeks. The mean birth weight was 3.11 ± 0.384 kg. The percentages of premature and low birth weight (LBW) infants were 7 and 5%, respectively. At multiple logistic regression controlling for potentially confounding factors that were significantly associated with prematurity and LBW at univariate analysis (maternal consumption of calcium supplementation, folic acid, and omega-3, during pregnancy), type of nutritional groups containing dairy products, proteins, fish, and shrimp group, as well as fruits and vegetables, had a significant positive association with increasing the gestational age (P < 0.05). The group that consumed proteins, fish, and shrimp, as well as fruits and vegetables had a significant positive association with the newborn's weight (P < 0.05).
Conclusion:
This study indicated the importance of proper nutrition on reducing the rates of LBW and premature births. Comprehensive educational programs at individual and public levels are warranted in this regard.
Keywords: Education, fetal growth, health promotion, maternal nutrition, pregnancy
INTRODUCTION
Pregnancy is the most important and most risky stage in the lives of the mother and fetus, with long-term impacts on their social well-being and health of individuals, families, and communities. The mother's ill-health or disease during this period not only affects the quality of her life, but also the health of the fetus and that of the future generations. Many factors are effective in determining the proper course of pregnancy and its outcome. Proper nutrition at this time is one of the most important factors.[1] Studies have shown that improved maternal nutrition before and during pregnancy, compared to the quantity and quality of feeding during the neonatal period, is a more important factor in the reduction of neonatal mortality and health promotion.[2] A growing body of evidence supports the fetal programming of chronic non-communicable diseases.[3] In addition to adequate nutrition, a balance of nutrients like the balance between protein and energy in the diet of the mother in late pregnancy has important implications for the baby's birth weight and subsequent diseases.[4] One of the main criteria of the healthiness of the infant is the measurement of the anthropometric indices of the newborn, which includes the measurement of weight, height, head, and chest circumference. Anthropometric indices along with the primary examination of the newborn can, to a great extent, reveal the newborn's health. Weight is the most important indicator of the infant's health. Birth weight is not only associated with the nutritional quality, health, prenatal care, and social environment of the mother, but is also associated with growth and normal development of the child. Newborns weighting less than 2500 g at birth are considered to have a low birth weight (LBW).[5] The significant quality of LBW infants is not only the mortality rate, but this is also followed by other effects such as reduced life expectancy, infectious disease, respiratory problems, hypothermia, anemia, retinopathy, blindness, hearing loss, mental retardation, cerebral palsy, chronic pulmonary insufficiency, chromosome abnormalities, disproportionate body organs, and caring and feeding problems.
This longitudinal study was conducted to investigate the effect of the intake of different food groups by pregnant mothers on neonatal LBW and premature births.
MATERIALS AND METHODS
This cohort study was conducted from April to September 2012, in Isfahan, Iran.
This study was approved by the Ethical Committee of the Faculty of Medicine, Isfahan University of Medical Sciences. Written informed consent was obtained from all participants.
The target population was 225 pregnant women living in different geographical areas of the city, at least for the last one year. The samples were randomly selected from various areas of the city.
The main variables in the study were weight and gestational age of the neonates and the type and amount of food consumption of the mother, based on different food groups.[6] Data collection was conducted by a face-to-face interview with the mothers. A food frequency questionnaire was completed. After birth, the neonatal anthropometric parameters were measured according to the standard protocols, by using calibrated instruments. All the study subjects were matched in terms of variables such as maternal diseases (diabetes, hypothyroidism, and blood pressure) during pregnancy or influencing variables (non-smoking, drug use by the baby's father, and maternal age).
Statistical analysis
Data normality was verified using the Kolgomorov–Smirnov test corrected by Lilliefors and the variance homogeneity was verified using the Leven's test. Descriptive analyses were performed for all variables. Continuous variables were reported by using mean standard deviations.
All nutritional variables were compared according to different groups of infants (Normal, premature, and underweight). The comparison of means in the different study groups was conducted using the Student's t test, as appropriate. In the multivariate analysis, multiple linear and logistic regression models were used to identify the different FFQ variables independently associated with infant born status, adjusted by maternal consumption of calcium supplementation, folic acid, and omega-3, during pregnancy. Two-sided tests will be used, and P values < 0.05 will be considered as statistically significant. Statistical analyses will be performed using the SPSS for Windows (version 19.0, SPSS Inc., Chicago, Illinois)
RESULTS
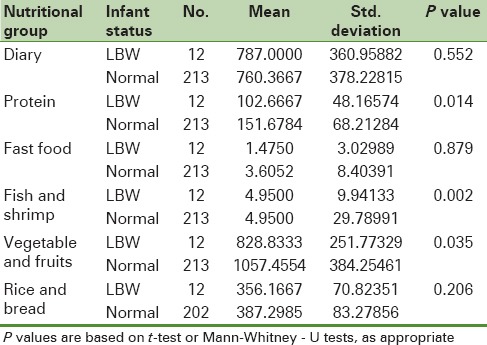
A total of 214 infants with complete information (225 pregnant women) were included. Our cases had a mean gestational age of 38.72 ± 1.2 (range 33.28 – 41) weeks. The mean birth weight was 3.11 ± 0.384 (range 1.43 – 4.28) kg. One hundred and two (47.7%) infants were male. The percentage of premature and low birth weight infants were 7 and 5%, respectively. For comparison of nutritional items between the LBW and normal groups, the following items were compared: Consumption of dairy products, fruits and vegetables, fast foods, shrimp and fish, protein groups, as well as bread and cereals. As presented in Table 1, the mothers of both groups of LBW and normal weight infants had statistically significant differences (P < 0.05) for the consumption of protein, fish and shrimp, fruits and vegetables. Consumption of all the above foods was significantly higher in mothers with normal-weight newborns.
Table 1.
Descriptive statistics for consumption of various nutritional factors in the two groups of low birth weight infants and normal weight
A comparison of the dietary intake of mothers of premature newborns with that of mothers of full-term newborns having a normal weight is presented in Table 2. It shows that mothers of premature newborns consumed lower amounts of dairy products and fruits and vegetables.
Table 2.
Consumption of various nutritional factors of premature and normal weight infants
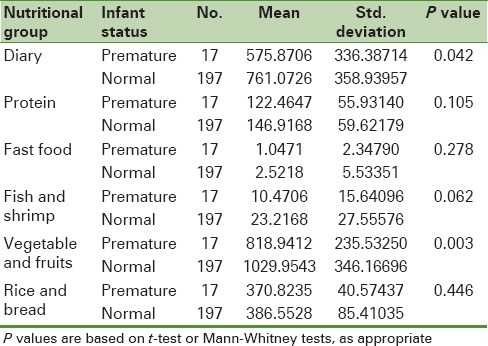
Mothers with normal-weight newborns had a significantly higher consumption of dairy products, fish and shrimp, as well as fruits and vegetables, regardless of receiving prenatal supplements. Consumption of bread and cereals was also higher in mothers of neonates with normal weight than in mothers of the low birth weight and premature infants. However, the statistical analysis of the results showed that based on the mean comparison tests for two independent groups, in the LBW group (P value = 0.206) and in the premature group (P value = 0.446), there was no statistically significant difference between these groups.
At multiple logistic regression controlling for potentially confounding factors that were significantly associated to prematurity and low birth weight at univariate analysis (maternal consumption of calcium supplementation, folic acid and omega-3 during pregnancy), type of nutritional groups containing dairy products, proteins, fish and shrimp group, as well as fruits and vegetables, had a significantly positive association with increasing gestational age (P < 0.05). The frequency of intake of protein, fish, and shrimp group, as well as fruits and vegetables was significantly associated with the newborn's weight (P < 0.05).
DISCUSSION
Our study serves as confirmatory evidence for the effects of dietary intake of pregnant mothers on fetal growth. Pregnant mothers need various kinds of foods with adequate calories. Lack of adequate nutrition with good quality and quantity, before and during pregnancy can cause health problems for the both mother and her fetus. It increases the risk of preterm delivery and intrauterine growth retardation to a considerable extent. Studies on pregnant women in the Second World War, who were undernourished, have highlighted this issue.[7] In the Netherlands, those women with good nutrition before pregnancy, who received less than 1000 calories per day during pregnancy, gave birth to stunted and LBW infants, however, the rate of stillbirths and preterm births was not increased in this group. However, in Leningrad, those women who faced severe malnutrition before and during pregnancy experienced high rates of stillbirths, premature birth, and infectious diseases.[7]
On the basis of the findings of the current study, consumption of fruits and vegetables is associated with decreased rates of preterm birth and LBW. Given that fruits and vegetables are rich sources of antioxidants[8] the importance of the consumption of this food group is completely clear. The results of this study are consistent with the results of some previous studies in showing the relationship between consumption of fruits and vegetables and reducing the risk of preterm delivery.[9] In addition, it is known that oxidative stress, by decreasing the cellular defense and damage to the existing collagens, in the amniotic membrane of embryonic cells can trigger preterm labor.[10,11] The underlying cause of oxidative stress is an imbalance in free radicals and the antioxidant defense system.[10,12] Mercola et al., reviewed the details of different foods before and during the second trimester of pregnancy. They demonstrated that in those women who consumed less than 10% of foods containing vitamin C and less than 21 mg per day of this vitamin before pregnancy, the risk of premature rupture of the fetal membranes and preterm delivery were two times higher than in other women. In pregnant women who consumed less than 65 mg of vitamin C per day, this percentage during the second trimester and increased risk of these complications was 70%.[13]
One of the important reasons of preterm deliveries is pre-eclampsia and eclampsia. It is suggested that higher consumption of fruits and vegetables containing vitamin C and other antioxidants may reduce the incidence of pre-eclampsia.[14] The insufficient dietary intake of protein, calcium, sodium, magnesium, as well as, vitamins A, E, and C may be among the predisposing factors of pre-eclampsia.[15] With reviewing a large number of controlled clinical trials, Villar and colleagues concluded that lack of antioxidants including vitamins A, E, and C in pregnant women can increase the incidence of pre-eclampsia. They suggested special attention to the dietary antioxidants.[16] Researchers are focusing on providing the vitamin and minerals through foods, especially fruits and vegetables, and limiting the consumption of vitamin supplements and minerals to certain conditions, such as, malnutrition in pregnancy. In this regard, the results of a study that was performed on the vegetarians in Tennessee from 1977 to 1982, indicated that out of 755 pregnant women who were vegetarian, only one case was diagnosed with pre-eclampsia.[17] Another study showed that consuming less than the minimum allowable ratio of fruits and vegetables (less than five servings per day) increased the risk of pre-eclampsia 1.2 times.[18] One other study showed that consumption of more than the allowed amount of the required fruits and vegetables reduced the risk of high blood pressure by 45%.[14] Another study found that the risk of pre-eclampsia was 1.7 fold higher in pregnant women who had used fruits as apple, orange, grapefruit, peach than in those who had not used these fruit[19] These studies indicate the controlling effect of fruit and vegetable consumption on pre-eclampsia, and consequently, this may reduce the number of preterm deliveries and LBW neonates.
Another notable point of the current study is the significant difference in the weight of infants according the consumption of fish and shrimp by their mothers. These results are consistent with the studies, which show that in the fish-consuming populations, such as in islands, pregnancy is longer and the infants have more weight.[20] A study in Denmark and ]Ireland documented that lower consumption of fish by pregnant mothers was associated with a higher incidence of preterm labor.[20] Fish and seafood contain long chain unsaturated fatty acids, such as, linolenic acid (6 n) and alpha-linolenic acid from the omega-3 family, which are among the group of essential fatty acids. On the basis of the previous studies, an inverse relationship exists between the increased blood levels of omega-3 and preterm delivery[21] As omega-3 produces α2F and 2E prostaglandin, some researchers suggest that fish oil capsules be consumed. However, due to the high amount of vitamin A and E to protect fatty acids, the possibility of hypervitaminosis should be taken into account. The United States Food and Drug Administration (FDA) does not recommend its supplement use for pregnant women.[22] Thus, following a proper diet with at least 5 g of essential fatty acids, during pregnancy, can increase the uterine myometrium muscle relaxation, continuation of the pregnancy, and better fetal weight.[23]
The current study also indicated that dairy product consumption during pregnancy has a significant relationship with weight gain and reduction of premature deliveries. Dairy products are considered as the major sources of calcium and protein. Researchers believe that calcium intake during pregnancy affects the birth weight, prolonging pregnancy and increasing fetal growth.[24] Lack of calcium will be a barrier to the expansion of blood vessels and will finally result in premature and low birth weight infants.[25] On the basis of the new findings on the role of calcium in changing the weight and prevention of chronic diseases,[26] some experts even recommend entering it in the dietary guidelines. It is documented that limiting milk intake during pregnancy could reduce the absorption of protein, calcium, and vitamin D, which could threaten the infant's health through reducing the birth weight. Calcium is an essential nutrient, which is responsible for the construction, metabolic, and regulating roles in the body. Shortage in the consumption of milk and dairy products threatens the health of pregnant women and their children. Milk and dairy products play an essential role in providing the protein and calcium requirements of pregnancy, prevention of osteoporosis, and dental caries.[27] The blood pressure lowering effects of calcium are documented, as well.[28] This attenuation effect could reduce the risk of elevated blood pressure during pregnancy, which is one of the main causes of preterm deliveries. The mechanism of this action of calcium remains to be determined. The proposed mechanisms include the effects of calcium on the serum parathyroid hormone and plasma rennin activity.[28]
In the current study, a significant correlation exists between the consumption of fast foods, infant weight gain and loss, and prematurity. The study shows that consumption of fast foods can have an effect on the increase of weight and decrease the rate of preterm birth. There has been no research in this field, but we are aware that unsaturated fats, which are the integral components in preparing fast foods, can increase the cholesterol and triglyceride levels of pregnant women. According to the previous studies, triglyceride and cholesterol levels are higher in patients with pre-eclampsia.[29] Triglycerides can damage the endothelium and have a direct relationship with hypertension and proteinuria, and play a role in the pathophysiology of pre-eclampsia.[30]
In a cross-sectional study in pregnant women with pre-eclampsia, triglycerides, LDL cholesterol, and phospholipid levels were higher and the HDL cholesterol level was lower.[31] In another study in 2009, increasing the lipid level in pregnancy was significantly correlated with pre-eclampsia.[32] In addition, in pregnant women, obesity has been recognized as an important factor in increasing the risk of diabetes. Researches have shown that abnormal weight gain is significant in carbohydrate intolerance and it is associated with a higher risk of gestational diabetes mellitus. Although, increasing the weight by ‘10–20’ kg will increase the risk 2.5 times, the risk with an increase of more than 20 kg will be 3.5 times higher.[33] Accordingly, it can be predicted that continuous and excessive consumption of fast foods during pregnancy can increase the risk of premature deliveries, with abnormal blood lipid levels and increased risk of gestational diabetes mellitus. Perhaps the lack of consistency with the previous conducted studies is because, in the present study, a small number of pregnant mothers consumed fast foods. Also, due to the potential risk of fast foods, a low and rare use of these foods was seen among the mothers. In fact, even in this study, all the mothers who had fast food consumption, had not had enough to cause complications resulting from its use. Excessive consumption of fast foods, in addition to the mentioned risks, can cause lack in the mother's nutrition of the needed common nutrients in pregnancy, such as, fruits and vegetables. Therefore, it can lead to malnutrition in pregnancy, underweight, and preterm birth.
In addition to their protein content, meat and its substitutes may supply the needed iron to a pregnant mother. In the present study, the consumption of proteins, including meat, eggs, and beans was related to a gain in weight of the infant, at the time of birth. Moreover, meat and eggs are rich sources of iron. Iron-deficiency anemia in pregnancy can cause several complications, including weakness of mother, increased risk of mortality at the time of delivery, increased risk of premature birth, low birth weight, and abortion.[34] Consumption of meat and its substitutes for the provision of essential proteins for the synthesis of fetal and maternal tissues has been emphasized at different stages of pregnancy. In a study conducted on women in Guatemala, it has been reported that giving calories alone to protein-deficient women does not have the same effect on birth weight as the combined administration of protein and calories.[35] Zlatnick and colleagues reported that the birth weight of the infant is associated with maternal protein intake during pregnancy.[36] The results of the current study are consistent with the above-mentioned studies.
In the present study, consumption of bread and cereals did not differ among the groups studied. Bread and cereals play an essential role in the supplying calories for women and are rich in vitamin B, iron, zinc, and fiber. Low consumption of cereals, especially in women with normal or low body mass index, will cause depletion of maternal stores during pregnancy.[27] These mothers face excessive fatigue. In Kramer's study, high rates of LBW births and intrauterine growth restriction occurred because of small weight gain during pregnancy, on account of low energy intake.[37] A study in Maryland was conducted on 300 pregnant mothers and indicated a significant relationship between energy intake and birth weight of infants.[38]
The results of the current study are in line with some previous studies[25,39] in showing a direct correlation between maternal nutrition (including dairy, proteins, fast foods, fish and shrimp, and fruits and vegetables) and LBW and premature births.
In this study, the mothers of underweight and normal infants have significant differences in the case of consumption of all the measured food groups. The consumption of all mentioned items (other than bread and cereals) was higher in mothers who had given birth to infants with normal weight. These findings highlight the importance of maternal nutrition during pregnancy, which is an important factor in the reduction of underweight and premature infants. Therefore, more attention to nutrition education during pregnancy will lead to improved maternal nutritional status for newborns, which is one of the important issues in public health. Maybe this is the reason that primary health care has been adopted for all by the World Health Organization, as a basic strategy to achieve health goals. Policy makers have underscored the importance of such issues as components of primary health care. It should be kept in mind that improving neonatal health in a community can improve the health of the society and the future generations.
CONCLUSION
This study indicated the importance of proper nutrition in reducing the rates of LBW and premature births. Reducing infant mortality and adverse health effects of underweight and immature infants requires comprehensive studies and implementation of a defined educational program at individual and public levels. Therefore, designing of educational interventions and proper nutritional interventions, such as, allocating special food baskets to women with poor nutritional status, with control and follow-up, can have a significant impact on the reduction of premature infants and LBW newborns.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Szawajcer EM, Hiddink GJ, Koelen MA, Van Woerkum CM. Nutrition awareness and Pregnancy: Implication for the life course perspective. Eur Jobstet Gynecol Reprod Biol. 2007;135:5864. doi: 10.1016/j.ejogrb.2006.11.012. [DOI] [PubMed] [Google Scholar]
- 2.Hosseini MS, Nastaran J. Relationship between pregnancy outcome and maternal BMI and wight gain. Int Congr Ser. 2004;1271:380–3. [Google Scholar]
- 3.Rasmussen MK. The “fetal origins” hypothesis: Challenges and opportunities for maternal and child nutrition. Annual Rew Nut. 2001;21:73–95. doi: 10.1146/annurev.nutr.21.1.73. [DOI] [PubMed] [Google Scholar]
- 4.Fagen C. Nutrition During pregnancy and Laction. In: Mahan KL, Escott-stumps, editors. Krause's food nutrition and diet therapy. 11th ed. USA: W. B. Saunders; 2004. pp. 168–46. [Google Scholar]
- 5.Garmaroudi GR, Eftekhar H, Batebi A. Low birth weight frequency and risk factors in Tehran. Payesh. 2002;1:13–8. [Google Scholar]
- 6.Wong JE, Parnell WR, Black KE, Skidmore PM. Reliability and relative validity of a food frequency questionnaire to assess food group intakes in New Zealand adolescents. Nutr J. 2012;11:65. doi: 10.1186/1475-2891-11-65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gilbert ES, Harmon JS. 3rd ed. London: Saunders; 2003. Manual of high risk pregnancy and delivery; pp. 522–5. [Google Scholar]
- 8.Wall PD, Pressman EK, Woods JR., Jr Preterm premature rapture of the membrance and antioxydants: The free radical connection. J Perinat Med. 2002;30:447–57. doi: 10.1515/JPM.2002.071. [DOI] [PubMed] [Google Scholar]
- 9.Roozbahani N, Torkestani N, Gazerani N. Study of the relationship between preterm labor and consuming fruit and vegetable before and during pregnancy. J Arak Univ Med Scis. 2004;7:13–9. [Google Scholar]
- 10.Halliwell B. The antioxidant paradox. Lancet. 2000;355:1179–84. doi: 10.1016/S0140-6736(00)02075-4. [DOI] [PubMed] [Google Scholar]
- 11.Woods JR., Jr Reactive oxygen species and preterm premature rupture of membranes-a review. Placenta. 2001;(Suppl A):S38–44. doi: 10.1053/plac.2001.0638. [DOI] [PubMed] [Google Scholar]
- 12.Eberherdt M. 1st ed. USA: CRC Press; 2001. Reactive oxygen metabolits; pp. 272–9. [Google Scholar]
- 13.Mercola J. Lack of vitamin C may trigger premature delivery. [Last accessed on 2013]; Optimal wellness center/mercola.com. [Google Scholar]
- 14.Conlin PR, Chow D, Miller ER, 3 rd, Svetkey LP, Lin PH, Harsha DW, et al. The effect of dietary patterns on blood pressure control in hypertensive pations: Results from the dietary approaches to stop hypertension (Dash) trial. Am J Hypertens. 2000;13:949–55. doi: 10.1016/s0895-7061(99)00284-8. [DOI] [PubMed] [Google Scholar]
- 15.Gilbert E, Harman J. 2nd ed. St Louis: Mosby; 2003. Manual of high risk pregnancy and delivery; pp. 445–62. [Google Scholar]
- 16.Villar J, Merialdi M, Gülmezoglu AM, Abalos E, Carroli G, Kulier R, et al. Nutritional interventions during pregnancy for the prevention of treatment of maternal morbidity and preterm delivery: An overview of randomized controlled trials. J Nutr. 2003;133:1606s–25. doi: 10.1093/jn/133.5.1606S. [DOI] [PubMed] [Google Scholar]
- 17.Mangels R. Vegetaration diet during pregnancy. Human Society of United State. 2004. [Last accessed on July10,2012]. pp. 1–8. Available from: http://www.googel.com .
- 18.Zhang C, Williams MA, King IB, Dashow EF, Sorensen TK, Frederio IO, et al. Vitamin C and the risk of preeclampsia-resaits from dietary questionnaire and plasma assay. Epidemiology. 2002;13:382–3. doi: 10.1097/00001648-200207000-00008. [DOI] [PubMed] [Google Scholar]
- 19.Atkinson JO, Mahomed K, Williams SM, Woelk GB, Mudzamiris WN. Dietary risk factors for preeclampsia among women attending Harare Maternity Hospital, Zimbewe. Cont Afr J Med. 1999;44:86–92. [PubMed] [Google Scholar]
- 20.Olsen SF, Secher NJ. LOW consumption of seafood in early pregnancy as a risk factor for preterm delivery: Prospective cohort study. BMJ. 2002;324:447. doi: 10.1136/bmj.324.7335.447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jafarian M. Long life without disease with omega-3. Miracle of the new century. Row Publishers. 2004:61–52. [Google Scholar]
- 22.Kohen Dara. London: Rout Leadge; 2002. Woman and mental Health. [Google Scholar]
- 23.Louis ST. Philadelphia: Wolters Kluwer Company CEO; 2001. Facts and comparisons. [Google Scholar]
- 24.Merialdi M, Carroli G, Villar J, Abalos E, Gulmezoglu AM, Kulier R, et al. Nutritional interventions during pregnancy for the prevention or treatment of impaired fetal growth: An overview of randomized controlled trials. J Nutr. 2003;133:S1626–31. doi: 10.1093/jn/133.5.1626S. [DOI] [PubMed] [Google Scholar]
- 25.Burris HH, Mitchell A, Werler MM. Periconceptional Multivitamin Use and Infant Birth Weight disparities. Ann Epidemiol. 2010;20:233–40. doi: 10.1016/j.annepidem.2009.12.003. [DOI] [PubMed] [Google Scholar]
- 26.Miller GD, Anderson JJ. The role of calcium in prevention of chronic diseases. J Am Coll Nutr. 1999;18:S371–2. doi: 10.1080/07315724.1999.10718900. [DOI] [PubMed] [Google Scholar]
- 27.Foruzani M. 1st ed. Tehran: Chehr Publications; 2003. Nutrition during pregnancy. [Google Scholar]
- 28.Repke J, Villar J. Pregnancy induced hypertension and low-birth-weight: The role of calcium. Am J Clin Nutr. 1991;54:237–41. doi: 10.1093/ajcn/54.1.237S. [DOI] [PubMed] [Google Scholar]
- 29.Enquobahrie DA, Williams MA, Butler CL, Frederick IO, Miller RS, Luthy DA. Maternal plasma lipid concentrations in early pregnancy and risk of preeclampsia. Am J Hypertens. 2004;17:574–81. doi: 10.1016/j.amjhyper.2004.03.666. [DOI] [PubMed] [Google Scholar]
- 30.Winkler K, Wetzka B, Hoffmann MM, Friedrich I, Kinner M, Baumstark MW, et al. Triglyceride-rich lipoproteins are associated with hypertension in preeclampsia. J Clin Endocrinol Metab. 2003;88:1162–6. doi: 10.1210/jc.2002-021160. [DOI] [PubMed] [Google Scholar]
- 31.Khaliq F, Singhal U, Arshad Z, Hossain MM. Study of serum lipid and lipoprotein in preeclampsia with special reference to parity. Indian J Physiol Pharmacol. 2000;44:192–6. [PubMed] [Google Scholar]
- 32.Wiznitzer A, Mayer A, Novack V, Sheiner E, Gilutz H, Malhotra A, et al. Association of lipid levels during gestation with preeclampsia and gestational diabetes mellitus: A population based study. Am J Obstet Gynecol. 2009;201:482.el. doi: 10.1016/j.ajog.2009.05.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Baeten JM, Bukusi EA, Lambe M. Pregnancy complications and outcomes among overweight and obese nulliparous women. Am J Public Health. 2001;91:436–40. doi: 10.2105/ajph.91.3.436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Salvaggro A, Periti M, Quaglia G, Marzorati D. Iron and ferritin in Italian Subyects Eur. J Epidemiol. 1991;7:621–7. doi: 10.1007/BF00218672. [DOI] [PubMed] [Google Scholar]
- 35.Foroozani M. Tehran: Chehreh Publications; 1381. Nutrition in pregnancy; p. 4. 5,37,38. [Google Scholar]
- 36.Zlatnick FJ, Burmeister LF. Dietary in pregnancy: Effect on anthropometric indices of the new born infant. Am J Obstet Gynecol ; 1983;146:199. doi: 10.1016/0002-9378(83)91054-2. [DOI] [PubMed] [Google Scholar]
- 37.Kramer SM. The epidemiology of adverse pregnancy outcomes: An overview. J Nutr. 2003;133:1284–42. doi: 10.1093/jn/133.5.1592S. [DOI] [PubMed] [Google Scholar]
- 38.Langley Evans JL, Langley Evans CS. Relationship between maternal nutrient intake in early and late pregnancy and infants weight and proportions at birth. Prospective cohort study. J R Soc Promot Health. 2004;123:210–6. doi: 10.1177/146642400312300409. [DOI] [PubMed] [Google Scholar]
- 39.Khoushabi F, Saraswathi G. Association between maternal nutrition status and birth weight of neonates in selected hospitals in Mysore City, India. Pak J Nutr. 2010;9:1124–30. [Google Scholar]