

Abstract
Background:
Neurological complications following lightning are rare and occur in form of temporary neurological deficits of central origin. Involvement of peripheral nervous system is extremely rare and only a few cases have been described in the literature. Isolated unilateral pan-brachial plexus neuropraxia has never been reported in the literature. Steroids have long been used for treatment of neuropraxia. However, their use in lightning neural injury is unique and requires special mention.
Case Description:
We report a rare case of lightning-induced unilateral complete flaccid paralysis along with sensory loss in a young patient. Lightning typically causes central nervous involvement in various types of motor and sensory deficit. Surprisingly, the nerve conduction study showed the involvement of peripheral nervous system involvement. Steroids were administered and there was significant improvement in neurological functions within a short span of days. Patients’ functions in the affected limb were normal in one month.
Conclusion:
Our case was interesting since it is the first such case in the literature where lightning has caused such a rare instance of unilateral pan-brachial plexus lesion. Such cases when seen, raises the possibility of more common central nervous system pathology rather than peripheral involvement. However, such lesions can be purely benign forms of peripheral nerve neuropraxia, which can be managed by steroid treatment without leaving any long-term neurological deficits.
Keywords: Good recovery, lightning injury, neuropraxia, pan-brachial plexus
INTRODUCTION
Brachial plexus injury is usually of traumatic origin due to road traffic accidents, fall from height, etc. The neurological deficits arising out of this injury can involve all the trunks and cords resulting in pan-brachial palsy or may involve selective trunks with characteristic motor and sensory deficit pattern. Depending upon the severity of neural involvement, it can be simple, reversible functional dysfunction of neuropraxia to severe complete loss of structural integrity in form of neurotmesis. However, practically complete or pan-brachial plexus neuropraxia of traumatic origin is not possible. But sudden, reversible loss of all modalities of sensation or motor power can occur following exposure to a very high electric current or voltage such as lightning. This is due to the electroporatic effect of high electric current, which de-stabilises the membrane potential across any biological cell membranes such as that of neurons.[1,8] Steroids have a membrane stabilizing effect, thereby facilitate the early restoration of membrane potential across the neuronal membrane.
CASE REPORT
A 25-year-old male patient presented with complete flaccid paralysis and numbness of right upper limb. One day earlier, he had been electrocuted while holding a telephone pole with his right hand during the lightning. Immediately, following this he developed complete paralysis of right side upper limb with loss of sensation. There was no loss of consciousness, disturbance of speech, or seizure. The right side upper limb was normal on general examination with no entry burn points, bluish coloration, and all the peripheral pulses were normal. On neurologic examination, there was complete loss of all movements with power around all joints being grade 0 in right upper limb [Figure 1]. All modalities of sensation were absent in the same limb, excepting a very small patch in the uppermost part of right arm where it was reduced to 20% of that on left side. Nerve conduction study done on 5th day after the lightning injury, showed grossly diminished conduction velocity and increased distal latencies in all the major nerves of right upper limb without any decrease in amplitude. Electromyography showed no fibrillations. Magnetic resonance imaging (MRI) neck showed normal brachial plexus with no avulsion or pseudomeningocele formation [Figure 2]. Patient was put on steroid therapy (20 mg prednisolone thrice daily for 2 weeks) followed by tapering doses for a total of 6 weeks. An arm sling was given to support the paralysed limb. On follow-up, 1 week after starting the steroid therapy, power in right hand had improved; he could open and close his fist, write with bad hand writing (with support from left hand). However, there was no recovery of muscle function in forearm and arm muscles. There was restoration of sensations in right side upper limb to 30% of normal. On completion of 2nd follow-up week, power in right hand grossly improved with ability to write properly and do routine activities. Patient was able to raise his forearm against gravity (Grade 3 power). Abduction at shoulder joint was possible to only 30° [Figure 3]. Sensation improved to 75% of normal. Twenty days after starting the steroid therapy, power in forearm muscles improved to grade 5, abduction at shoulder increased to 70–80°. There was complete recovery of sensation in right upper limb. At the end of 4th week course of steroid therapy, patient had regained complete power of muscles and sensations in right upper limbs. Now he could raise his right arm to full extent, do normal routine activities with his hand, forearm, and arm [Figure 4]. Nerve conduction study done at the end of 5th week showed 80% recovery in conduction velocity and distal latencies.
Figure 1.

Complete flaccid paralysis of right upper limb at day 1 of lightning injury
Figure 2.
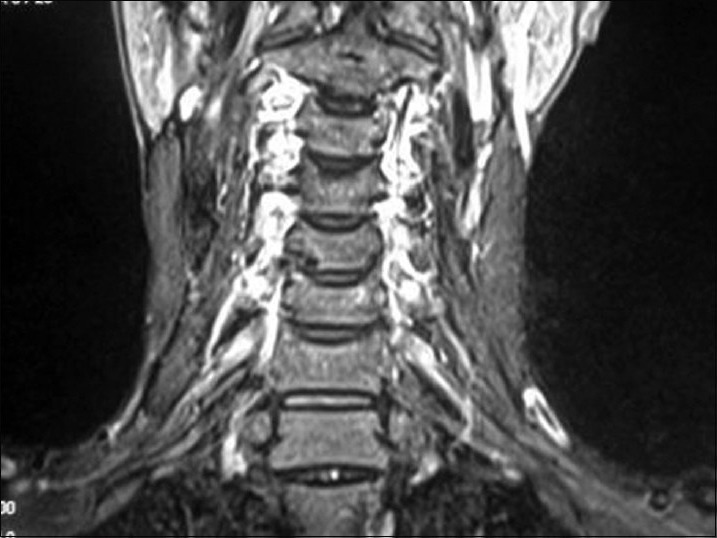
MRI Neck showing normal brachial plexus on both sides
Figure 3.

Post 2nd week following injury and on steroid therapy – Gross improvement in right hand and forearm muscle power
Figure 4.

Post 4th week – Complete restoration of muscle power in all groups of muscles in right upper limb
DISCUSSION
Brachial palsy including neuropraxia is commonly caused by traumatic events, and that caused by lightning injury have been rarely described in the literature.[5] Neurological complications due to lightning mainly relate to the central nervous system like loss of consciousness, paraplegia, tetraplegia, aphasia, seizures, memory disorder, headache, movement disorders like dystonia or tremor and are mostly temporary.[8] Pathology is usually in form of encephalopathy, hemorrhagic or ischemic stroke, and cerebellar damage.[1] Spinal cord involvement is less frequent than the cranial component and usually in the form of myelopathy affecting the anterior horn cells.[1] Damage to the peripheral nervous system is rare.[1] Nerve conduction studies should be done in every case of brachial plexus injury due to electrical injury so as to differentiate peripheral from central location of pathology. In our case, the nerve conduction study and the electromyography were suggestive of neuropraxia rather than axonal injury. Again the pattern of motor and sensory recovery was from distal to proximal, which also establishes the neuropraxic nature of the injury. In more serious axonal injury, there would have diminished amplitude of the conduction with fibrillations in electromyography, which were not seen in our case. There is a special kind of injury in up to two-thirds of the seriously injured lightning patients, called kerauno-paralysis, which is a unique temporary paralysis secondary to lightning strike. It is characterized by lower and sometimes upper extremities paralysis and the limbs are bluish, mottled, cold, and pulseless. This kerauno-paralysis is secondary to vascular spasm and sympathetic nervous system instability.[2,3] The paralysis usually improves within a few hours, but rarely there may be permanent paralysis or paresthesias. Our patient did not have any features of cutaneous or vascular findings suggestive of this type of pathology. Literature describes a syndrome of delayed muscle atrophy due to peripheral nerve injury by lightning.[4]
Electroporation, or electro-permeabilization, is a gross increase in the electrical conductivity and permeability of the plasma membrane caused by an externally applied electrical field. Neuropraxia can be caused by the effect of electroporation, which results in disturbed threshold of membrane excitability due to the electric current. Electric injury either direct or in form of lightning can cause temporary suspension of nerve conduction due to their membrane destabilizing effect. Steroids can speed up the recovery by their membrane stabilizing effect. This is mediated through prevention of lipid peroxidation of cell membranes and restoration of membrane sodium pumps. Steroids also reduce the peri-neuronal edema, which may have a role in the pathogenesis of brachial plexus neuropraxia caused by lightning or other electrical energy.
Our case was exclusive in that the brachial plexus involvement was caused by lightning injury and there was pan-brachial involvement. Although, the literature mentions that peripheral nerve damage caused by lightning injury has poor outcome,[6,7] our patient had complete recovery within a short span of days. Patient presented with complete loss of sensation and paralysis and the electrophysiological tests were confirmatory of pan-brachial neuropraxia. We started the steroid therapy and recovery occurred within a short span of 20–30 days. So we conclude that such rare case of pan-brachial plexus neuropraxia caused by lightning injury can be managed successfully only with the steroid therapy. Serial follow-up and steroid therapy are the only treatment required in such types of brachial plexus neuropraxia.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2015/6/3/110/153650
Contributor Information
Ashis Patnaik, Email: dr_ash007@yahoo.co.in.
Ashok Kumar Mahapatra, Email: akmahapatra22000@gmail.com.
Menka Jha, Email: drmenkajha@gmail.com.
REFERENCES
- 1.Cherington M. Neurologic manifestations of lightning strikes. Neurology. 2003;60:182–5. doi: 10.1212/01.wnl.0000033801.15204.b5. [DOI] [PubMed] [Google Scholar]
- 2.Cooper MA. Lightning injuries: Prognostic signs for death. Ann Emerg Med. 1980;9:134–8. doi: 10.1016/s0196-0644(80)80268-x. [DOI] [PubMed] [Google Scholar]
- 3.ten Duis HJ, Klasen HJ, Reenalda PE. Keraunoparalysis, a “specific” lightning injury. Burns Incl Them Inj. 1985;12:54–7. doi: 10.1016/0305-4179(85)90183-4. [DOI] [PubMed] [Google Scholar]
- 4.Francis DA, Heron JR. Progressive muscular atrophy and posterior dislocation of the humerus following electrical shock. Postgrad Med J. 1984;60:143–4. doi: 10.1136/pgmj.60.700.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Guiraud V, Touzé E, Cabane JP, Zuber M. Bilateral plexopathy following lightning injury. Rev Neurol. 2004;160:1078–80. doi: 10.1016/s0035-3787(04)71146-7. [DOI] [PubMed] [Google Scholar]
- 6.Mankani MH, Abramov GS, Boddie A, Lee RC. Detection of peripheral nerve injury in electrical shock patients. Ann N Y Acad Sci. 1994;720:206–12. doi: 10.1111/j.1749-6632.1994.tb30448.x. [DOI] [PubMed] [Google Scholar]
- 7.Shantha TR. Causalgia induced by telephone-mediated lightning electrical injury and treated by interpleural block. Anesth Analg. 1991;73:507–8. [PubMed] [Google Scholar]
- 8.Tan HH, Goh SH. Lightning injury: Changi Hospital experience. Hong Kong J Emerg Med. 2003;10:223–32. [Google Scholar]