

Abstract
The residual consciousness of unconscious patients can be detected by studying the P300, a wave among event-related potentials. Previous studies have applied tones, the subject's name and other names as stimuli. However, the results were not satisfactory. In this study, we changed the constituent order of subjects’ two-character names to create derived names. The subject's derived names, together with tones and their own names, were used as auditory stimuli in event-related potential experiments. Healthy controls and unconscious patients were included in this study and made to listen to these auditory stimuli. In the two paradigms, a sine tone followed by the subject's own name and the subject's derived name followed by the subject's own name were used as standard and deviant stimuli, respectively. The results showed that all healthy controls had the P300 using both paradigms, and that the P300 in the second paradigm had a longer latency and two peaks. All minimally conscious state patients had the P300 in the first paradigm and the majority of them had the P300 in the second paradigm. Most vegetative state patients had no P300. Patients who showed the P300 in the two paradigms had more residual consciousness, and patients with the two-peak P300 had a higher probability of awakening within a short time. Our experimental findings suggest that the P300 event-related potential could reflect the conscious state of unconscious patients.
Keywords: nerve regeneration, brain injury, cognitive neuroscience, event-related potential, P300, electrophysiology, nutritional state, minimally conscious state, consciousness, disorders of consciousness, unconsciousness, evaluation, prognosis, NSFC grants, neural regeneration
Introduction
Definitions for the vegetative state and minimally conscious state have been proposed for more than 10 years (Ashwal et al., 1994; Giacino et al., 2002). However, the rate of misdiagnosis is very high (Majerus et al., 2005; Schnakers et al., 2009). What's more, could an unconscious patient come to be aware? When would he come to be aware? What will he be when wakes up? There is much uncertainty around these questions.
Measurement of event-related potentials (ERPs) is an objective and easy method for evaluating the residual cognitive function of patients with disorders of consciousness (DOC) (Faugeras et al., 2011), and is more and more popular. The P300 is the most appropriate cognition-related wave with which to evaluate consciousness (Kotchoubey et al., 2005).
As auditory stimuli, sine tones were widely used at first. However, the number of patients showing the P300 in response to these stimuli was limited (Cavinato et al., 2011). Even some healthy persons presented a small tone-evoked P300 (Holeckova et al., 2006; Fischer et al., 2008). In subsequent work, the subject's own name (SON) was used (Holeckova et al., 2006; Perrin et al., 2006; Schnakers et al., 2008; Cavinato et al., 2011). However, both vegetative state and minimally conscious state patients showed the P300, which made it difficult to differentiate between them (Perrin et al., 2006). Thus, another first name was used as a deviant stimulus to overcome the above shortcomings. However, using these stimuli, different authors generated different results (Perrin et al., 2006; Schnakers et al., 2008). Cavinato's study (2011) made some improvements. He used another first name as the deviant stimulus, but he also used two other paradigms with different difficulties. He thought the modulation of P300 latency according to the different tasks might predict the recovery of vegetative state to minimally conscious state. However, they could not identify differences between minimally conscious state patients and healthy controls because they both showed P300 modulation (Cavinato et al., 2011). This might be explained by salient differences between another first name and SON, which lead to a ceiling effect, with a similar effect being seen in minimally conscious state and control subjects. What's more, the difficulty in generating another first name limits its use (Perrin et al., 2006; Eichenlaub et al., 2012; Ruby et al., 2013). It is necessary to find a stimulus that is familiar to subjects, but which has small differences from SON such that the differentiation of it and SON is more difficult, thereby eliminating the ceiling effect.
According to the concept of derived pseudo-words (changing the constituent order of the two-character real words) (Wang et al., 2009), SON is a real word and a subject's derived name (SDN) is a derived pseudo-word. For example, if “xiao ming” is the SON, then “ming xiao” is the SDN. The same constituents in SDN and SON verify the familiarity of the SDN, while the similarity of SON and SDN increases the difficulty in differentiating them. What's more, the SDN is easy to generate and has a similar duration to the SON.
In the present study, we used three kinds of stimuli: a 1,000 Hz tone, the SON and the SDN. SON could elicit a larger response when uttered by a familiar voice (Holeckova et al., 2006); therefore, SON and SDN were both called by a familiar voice. These stimuli were arranged into two paradigms: (1) a 1,000 Hz tone as a standard stimulus and SON as a deviant stimulus; and (2) SDN as a standard stimulus and SON as a deviant stimulus. The expectation was that the first paradigm would produce similar results to previous studies. The creative second paradigm would potentially allow identification of a higher consciousness level, and so could further select patients that might be able to regain consciousness.
Subjects and Methods
Subjects
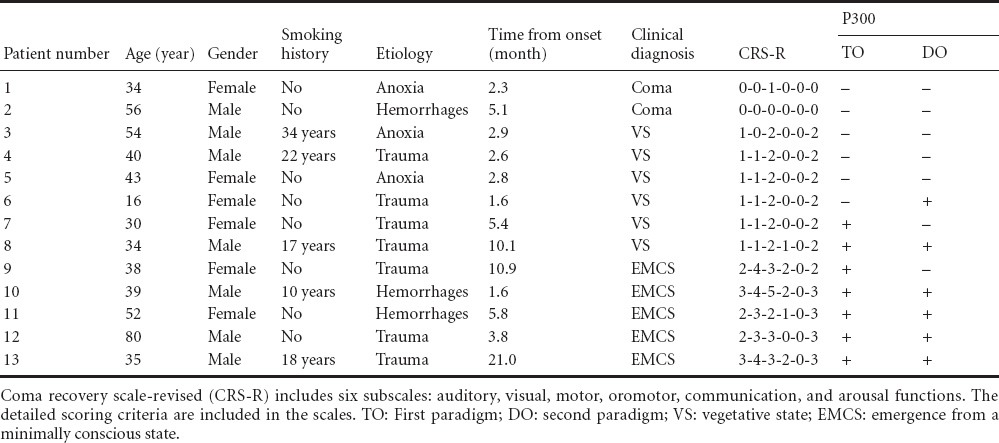
Seventeen healthy controls aged 24–56 years (8 males and 9 females, mean age 32.0 ± 8.5 years) were recruited through advertisements at Xuanwu Hospital, Capital Medical University (Beijing, China). Thirteen DOC patients (two in a coma, six in a vegetative state and five minimally conscious state patients) aged 16–80 years (7 males and 6 females, mean age 42 ± 16 years) were recruited from the Department of Rehabilitation Medicine of Xuanwu Hospital, China between June 2013 and August 2014.
In patients, clinical examination was performed using the Coma Recovery Scale-Revised (CRS-R). This scale includes six subscales: auditory, visual, motor, oromotor, communication, and arousal functions, and these subscales comprise 29 items. Apart from the arousal subscale, items marked “□” denote emergence from minimally conscious state and those marked “*” denote minimally conscious state. Items with no mark denote a vegetative state.
According to the arousal subscale, patients in a coma are unarousable. Among them, two healthy controls and five DOC patients had a smoking history of 10–34 years. The general conditions of the included patients are shown in Table 1. Informed consent was given by the healthy controls themselves or the patients’ family members. Ethical approval was provided by the ethics committee of the hospital.
Table 1.
The general conditions of patients with disorders of consciousness
Vegetative state patients
According to the CRS-R scale (Kalmar and Giacino, 2005), patients who showed no behaviors marked “□” or “*” were diagnosed as being in a vegetative state. They had to be in a vegetative state for > 1 month to exclude natural recovery. Patients should show normal or slightly delayed brain stem auditory-evoked responses. Patients with unstable clinical conditions or a previous history of hearing disorders, neurological, psychiatric disorders were excluded.
Minimally conscious state patients
According to the CRS-R scale (Kalmar and Giacino, 2005), patients who showed one or more behaviors marked “*” were diagnosed as being in a minimally conscious state. They had to be in a minimally conscious state for > 1 month to exclude natural recovery. Patients should show normal or slightly delayed brain stem auditory-evoked responses. Patients with unstable clinical conditions or a previous history of hearing disorders, neurological, psychiatric disorders were excluded.
Coma patients
According to the CRS-R scale (Kalmar and Giacino, 2005), patients who were unarousable were deemed to be in a coma. These patients had to be in a coma for > 1 month to exclude natural recovery. Patients should show normal or slightly delayed brain stem auditory-evoked responses. Patients with unstable clinical conditions or a previous history of hearing disorders, neurological, psychiatric disorders were excluded.
Healthy controls
Persons with no history of hearing disorders were included. Persons with a previous history of neurological or psychiatric disorders were excluded.
Clinical assessment
After admission, patients were allowed to familiarize themselves to the ward environment for 3–4 days and for their clinical conditions to stabilize. At the same time, DOC patients were repeatedly assessed with the CRS-R scale, daily. According to the CRS-R scale, patients were divided into three groups, including coma patients (n = 2), vegetative state patients (n = 6) and minimally conscious state patients (n = 5).
To examine the prognostic value of the ERP study, longitudinal behavioral assessments were performed at 1, 2, 3, 6, 9, and 12 months using the CRS-R scale if patients left the hospital after the ERP test. If patients were in the hospital, besides the time point above, their state of consciousness could be known at any time.
Procedure
There were three stimuli: a 1,000 Hz tone, the SON and the SDN. The 1,000 Hz tone lasted for 100 ms and was generated using Adobe Audition software (Adobe, Beijing Fistar Technology Limited Company, Beijing, China). The two-character SON was uttered by a first-degree family member. For the unmarried subjects, the SON was called by their best friend. The SON provider was told to speak the SON within a time of approximately 600 ms. The SDN was similar to the SON, but was formed by reversing the constituent order of the SON. The mean durations of SON and SDN were 504 ms and 519 ms for healthy controls. The mean durations of SON and SDN were 591 ms and 596 ms for DOC patients. The intensity of all three stimuli was 90 dB. The stimuli were delivered binaurally through earphones with a pseudorandom inter-stimulus interval of 0.8–1.2 seconds including 100 ms as a pre-stimulus baseline. A paradigm consisted of 800 stimuli, of which 120 were the deviant stimuli. Standard stimuli and deviant stimuli were given pseudo-randomly.
The three stimuli were arranged into two paradigms. In the first paradigm, also called the TO paradigm, participants were presented a 1,000 Hz tone as standard stimuli and SON as deviant stimuli. The second paradigm, also called the DO paradigm, included SDN as a standard stimulus and SON as a deviant stimulus. The probability of being presented with the deviant stimuli was 0.15. The program was presented using E-prime 2.0 software (Carnegie-Mei Long University and University of Pittsburgh, Pittsburgh, PA, USA). The order of presentation of these two paradigms was counterbalanced across all subjects.
ERPs of healthy controls were collected in the ERP experiment room. Subjects were told to clean their hair 1 day before test to decrease the electric resistance of the scalp. All subjects were asked to eat so as not to be too full or hungry. Because the P300 needed to be obtained without participants’ special attention, the healthy controls were asked to watch a silent movie to divert their attention (Holeckova et al., 2006, 2008; Muller-Gass et al., 2007). In the present study, the healthy controls were instructed to watch the nature documentary series ‘Wild China’ and to ignore the auditory stimuli. ERPs were collected at the patients’ bedsides. As for healthy controls, clean hair and appropriate energy were still necessary to assure the experiment could proceed smoothly. Because their attention resources were deficient, they did not need to watch the silent movie.
ERP recording
The healthy controls performed the experiment while sitting in a comfortable chair. ERP recording from DOC patients was completed with them lying in bed. ERPs were recorded from central line electrodes Fz, Cz and Pz with 64-channel electrode caps (Neuroscan Inc., Charlotte, NC, USA) according to the extended international 10–20 system. The reference electrode was placed on the nose. The ground electrode was near the FPz. Vertical electrooculogram and horizontal electrooculogram were recorded using two pairs of electrodes. For the vertical electrooculogram, the two electrodes were placed above and below the left eye. For the horizontal electrooculogram, the two electrodes were placed 10 mm from the lateral canthi of the eyes. The electrode impedance was below 5 kΩ throughout the experiment. The bandpass was 0.1–100 Hz and the sampling rate was 1,000 Hz.
Data analysis
EOG artifacts were corrected using the method proposed by Semlitsch et al. (1986). The EEG was segmented into the epochs from 100 ms pre-stimulus to 600 ms post-stimulus. Then, baseline adjustment was done to ensure that all ERP segments had the same origin. The EEG segment contaminated by amplifier clipping, bursts of electromyography activity, or peak-to-peak deflection exceeding ± 100 μV were excluded from averaging. The EEG segments were averaged separately for deviant and standard stimuli. At least 50 responses to deviant and standard stimuli were needed.
Peak detection was used to get the amplitudes and latencies of the P300. The latency and amplitude of the peak was assessed inside a time-window around the latency of the peak in the grand average graph. The P300 component was defined as the largest visible positive peak between 250 ms and 500 ms in the TO paradigm for healthy controls. With the DO paradigm, the P300 was a complex wave with two peaks. The first and second peaks were called DO1 and DO2, respectively. The DO1 and DO2 waves were defined as the largest visible positive peak between 380 ms and 500 ms and between 500 ms and 600 ms, respectively, in the DO paradigm for healthy controls. The P300 amplitude and latency in DOC patients were calculated manually one by one.
Statistical analysis
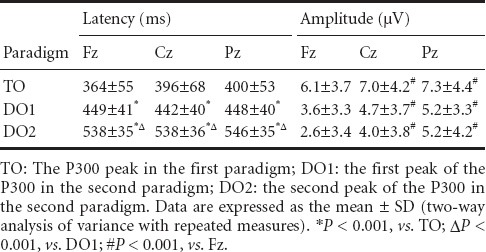
All data showed a normal distribution and are presented as the mean ± SD. Comparisons between the P300 latencies and amplitudes of healthy controls were performed. Two-way analysis of variance with repeated measures was conducted with condition (TO, DO paradigms) and scalp distribution (Fz, Cz, Pz) as factors, using SPSS 16.0 software (SPSS, Chicago, IL, USA). A Bonferroni test for post-hoc comparisons was adopted when results reached significance at P < 0.05. When appropriate, Greenhouse-Geisser corrections were made.
Results
P300 of healthy controls
Figure 1 shows that SON induced a positive component in both the TO and DO paradigms between 300 ms and 600 ms. The positive component in the TO paradigm had one peak, which was called the P300. However, in the DO paradigm, there were two peaks, which were called a P300 complex wave. The first and second peaks were called DO1 and DO2, respectively. The average amplitudes of TO, DO1 and DO2 were 6.79, 4.51, 3.90 μV, respectively. There was no significant difference between the amplitudes of DO1 and DO2. The amplitude tended to be higher in the TO paradigm than in the DO paradigm. There was a significant difference in amplitudes between scalp locations (P < 0.001, with LSD correction). Post-hoc analysis revealed that the P300 amplitude was slightly higher at Cz and Pz compared with Fz (P = 0.001 for Fz and Cz, P = 0.001 for Fz and Pz).
Figure 1.
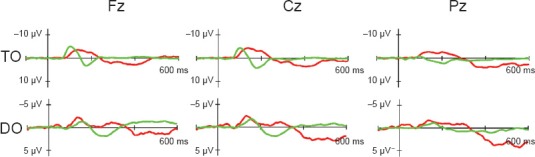
Grand averages of P300 in healthy controls at Fz, Cz, Pz in the TO and DO paradigms.
The green line represents standard stimuli and the red line represents deviant stimuli. In the first row, the green line is the tone, and the red line is the SON. In the second row, the green line is the SDN, and the red line is the SON. SDN: Subject's derived name; SON: subject's own name; TO: first paradigm; DO: second paradigm.
The average latencies of TO, DO1 and DO2 were 386.49, 446.49, and 540.39 ms, respectively. Analysis of variability showed that the latencies of P300 were prolonged in response to different levels of stimuli complexity (P < 0.001, with least significant difference correction). The DO paradigm had two specific P300 waves, and the latencies of both were significantly longer than that in the TO paradigm (P < 0.001 for TO and DO1, P < 0.001 for TO and DO2, with the least significant difference correction). In the DO paradigm, the latency of the second peak was significantly longer than that for the first peak (P < 0.001 for DO1 and DO2, with LSD correction). The latency did not differ among Fz, Cz and Pz. Table 2 shows the exact values of the amplitudes and latencies of Fz, Cz, Pz in the TO and DO paradigms.
Table 2.
The average latencies and amplitudes of P300 at Fz, Cz, Pz in healthy controls
P300 in DOC patients
The responses of 13 DOC patients are shown in Figure 2. According to the ERP results, the patients were classified into four groups: the first group is those who showed no P300 in either the TO or the DO paradigm; the second group is those who had no P300 in the TO paradigm but showed a P300 in the DO paradigm; the third group is those who had a P300 in the TO paradigm but no P300 in the DO paradigm; and the fourth group is those who showed the P300 in both TO and DO paradigms.
Figure 2.
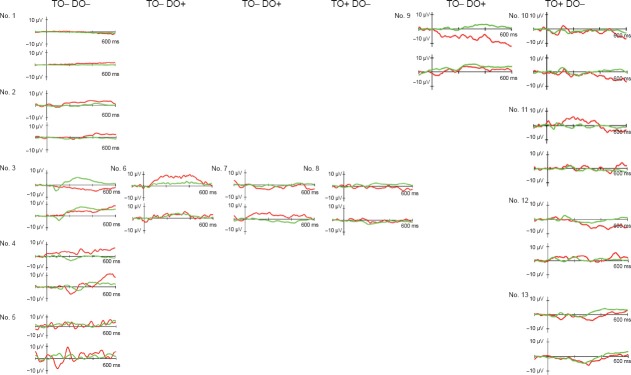
The P300 at Cz in 13 patients (No. 1–13) with disorders of consciousness.
The upper graph shows the results with the TO paradigm, while the lower one shows the results with the DO paradigm in each patient. Among all graphs, the green line represents the standard stimuli (tone/SDN) and the red line represents deviant stimuli (SON). SDN: Subject's derived name; SON: subject's own name; TO: first paradigm; DO: second paradigm.
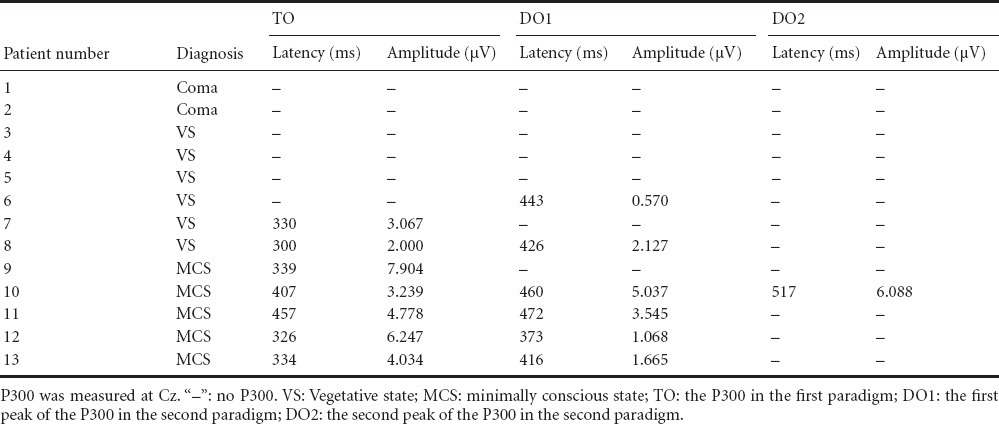
Apparently, the EEG of the two coma patients was flat. The vegetative state patients were scattered among the four groups. Four of six vegetative state patients belonged to the first two groups. They showed no P300 in the classical TO paradigm, regardless of whether they showed a P300 in the DO paradigm. Only two of the six vegetative state patients belonged to the latter two groups. They showed a P300 in the classical TO paradigm firstly, and then in the DO paradigm. The P300 of the two vegetative state patients (No. 7, No. 8) in the TO paradigm had a relatively shorter latency and lower amplitude. The P300 of vegetative state patient No. 6 in the DO paradigm, who had no P300 in the TO paradigm, had a very low amplitude. The P300 of vegetative state patient No. 8 in the DO paradigm, who had a P300 in the TO paradigm, had an appropriate latency and slightly lower amplitude. All minimally conscious state patients were in the latter two groups. They all showed a P300 between 300 ms and 600 ms in the TO paradigm, and the P300 had a latency and amplitude similar to the average values in healthy controls. Four of five minimally conscious state patients also showed a P300 in the DO paradigm with relatively suitable latency, but lower amplitude apart from patient No. 10. Minimally conscious state patient No. 10 not only had a P300 in the DO paradigm, but the P300 was a two-peak one. The latencies and amplitudes of these two peaks were both close to the normal values.
Patients No. 7 and No. 9 both belonged to the third group, but had different clinical diagnoses. Although the P300 latencies were similar, the P300 amplitude of minimally conscious state patient No. 9 in the TO paradigm was obviously larger than that in vegetative state patient No. 7. Vegetative state patient No. 8 and minimally conscious state patients No. 10–13 all belonged to the fourth group, but the P300 values of the minimally conscious state patients were closer to the normal values. The P300 latencies and amplitudes of individual patients are given in Table 3.
Table 3.
The P300 latencies and amplitudes in patients with disorders of consciousness
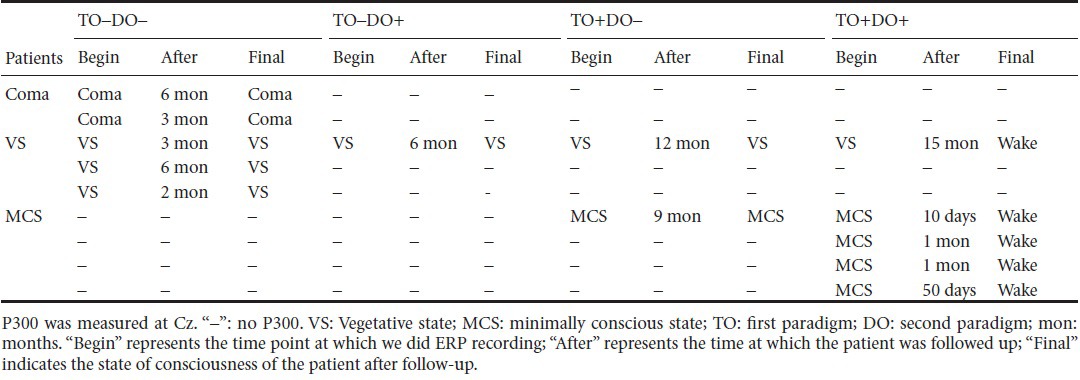
The prognosis of DOC patients
As shown in Table 4, patients without a P300 in the TO paradigm had a poor prognosis regardless of the result in the DO paradigm. The prognosis of patients with a P300 in the TO paradigm was varied. Patients in the third group could be vegetative state or minimally conscious state. However, these patients could still be discriminated easily based on the amplitude and latency of P300. Patients with a lower amplitude and/or longer latency tended to be vegetative state patients; otherwise, they were minimally conscious state patients. The remaining four minimally conscious state patients in the fourth group had a P300 in both the TO and DO paradigms, and had a good prognosis. All of the patients in this group eventually awoke. The minimally conscious state patient who had a two-peak P300 wave similar to the healthy controls awoke after 10 days. Thus, the P300 in the DO paradigm might be critical to the conscious level.
Table 4.
The prognosis of patients with disorders of consciousness
Discussion
The results of this study verified that all healthy controls showed reactions to SON, but that there was a one-peak P300 in the TO paradigm and a two-peak P300 with a longer latency and a smaller amplitude in the DO paradigm. The two coma patients showed no response to SON. Some vegetative state patients but almost all minimally conscious state patients showed reactions to SON. Patients who had the P300 in both the TO and DO paradigms seemingly had the opportunity to regain consciousness, especially the ones with a two-peak P300 in the DO paradigm.
The responses to SON in the TO paradigm were induced in all of the healthy controls, consistent with the results of previous studies (Perrin et al., 2006; Schnakers et al., 2008; Cavinato et al., 2011; Faugeras et al., 2011). SON is used in everyday life, and is thought to be familiar to subjects. Functional MRI and ERP test results also showed that SON called by a familiar voice could induce stronger cognitive activity (Holeckova et al., 2006, 2008). SON in the present study was called by the subject's first-degree family member or best friend. Therefore, the P300 was robustly induced in the TO paradigm. Then, the reactions of DOC patients to SON were observed. The results showed that all minimally conscious state patients and some vegetative state patients had the P300. Previous studies have been controversial around this point. Cavinato thought that all minimally conscious state patients and some vegetative state patients (6/11) showed the P300 to SON, consistent with the results of the present study (Cavinato et al., 2011). Resetti et al. (2013) found that the novelty P300 was found in all minimally conscious state patients and a large proportion of vegetative state patients. However, Fisher et al. (2010) thought the novelty P300 was not different between minimally conscious state patients and vegetative state patients, but that it had a close relationship with their etiology (being less frequent in cases of anoxia than in other etiologies). As the stimuli were similar, these controversial results might be a result of the different levels of consciousness of the DOC patients, although they were all classified as minimally conscious state or vegetative state. However, the results also showed that evaluating the consciousness level with only the TO paradigm is far from sufficient. Because most studies found that all minimally conscious state patients had the P300, it is possible that this task was used because it is somewhat easy to do. However, a more difficult paradigm is badly needed.
A previous study demonstrated that transparently derived pseudo-words, which still resemble real words, are processed similar to real words unlike opaque pseudo-words which are apparently different from real words (Raettig and Kotz, 2008). Coch et al. (2012) did their research with a real word (dark), a pronounceable pseudo-word (darl), a non-pronounceable nonword (rdka), and the letter-in-xs stimuli (dxxx) and found that the real word and pronounceable pseudo-word (which resembled the real word) both elicited a larger N400 than did the nonword and letter-in-xs stimuli. They both elicited a larger N400 than the nonword and letter-in-xs stimuli (Coch et al., 2012). In the present study, SDN was chosen as the standard stimulus. It resembled the SON, so we supposed SDN might had a similar quality with SON based on the studies of Raettig and Coch, which made it difficult to discriminate from SON. Because there have been no prior studies using SDN, the DO paradigm was used with healthy controls first. All healthy controls had a P300 in the DO paradigm, which verified its utility. The P300 latency in the DO paradigm was longer than that in the TO paradigm. Because complex stimuli require more time to process and the information-processing speed would be slower (Hong et al., 2013; van Dinteren et al., 2014), the DO paradigm was really a more complex paradigm. The similarity of SON and SDN decreased the difference between standard and deviant stimuli and increased the difficulty of this group. The surprising result was that there were two peaks in the DO paradigm between 300 ms and 600 ms. It is possible that this reflects cognitive activity. Subjects might have identified the SDN as the SON by automatically changing the order of the constituent letters. This might indicate a higher function of the brain, as suggested by the present results in DOC patients. The P300 amplitude and latency were close to the normal values in minimally conscious state patients, while those in vegetative state patients were greatly different from normal values. This finding is also similar to those of Cavinato et al. (2011).
Previous studies all failed to evaluate minimally conscious state or vegetative state at length. Perrin et al. (2006) studied the response to SON with another's first name as the background. He found that all minimally conscious state patients and three of five vegetative state patients had the P300, but he still could not differentiate vegetative state from minimally conscious state patients if they all showed a P300 (Perrin et al., 2006). Faugeras's experiment used five tones as standard and deviant stimulus; these stimuli also changed. He found that only two of 22 vegetative state patients had P300-like responses, and these patients showed signs of consciousness within 3 to 4 days following ERP recording. However, he did not observe minimally conscious state patients (Faugeras et al., 2011). In the present study, with the help of the DO paradigm, vegetative state patients were classified into four groups and minimally conscious state patients were classified into two groups. Thus, the consciousness level of DOC patients could be evaluated further on the basis of minimally conscious state or vegetative state. Even if patients were all evaluated as minimally conscious state according to their clinical behavior and scales, they all had different consciousness levels in reality. If the evaluation was done better, the prognosis prediction might be more accurate.
As to the prognosis, some studies used a tone and SON as a research tool. Fischer et al. (2008) showed that, in coma patients who had been in a coma for < 3 months, a P300 was highly correlated with awakening. Cavinato suggested et al. (2009) that vegetative state patients with the P300 tended to have more chance of waking but there were no minimally conscious state patients in that study. Therefore, the present results could not provide any consolidated evidence for prognosis prediction. The present results are in accordance with Fischer's results. Only the SON result could not accurately reflect the prognosis. Vegetative state or minimally conscious state patients with a P300 in the TO paradigm could remain in a DOC, but could also awaken. However, with the DO paradigm, it was easy to tell which patient would regain consciousness. Only those patients with a P300 in both the TO and DO paradigms would regain consciousness. Patients with a two-peak P300 in the DO paradigm would regain consciousness soon, while those with a one-peak P300 would take a longer time to regain consciousness. During this procedure, there might be a two-peak P300 that was not detected.
With the help of the TO and DO paradigms, vegetative state and minimally conscious state patients were divided into many subgroups. That is to say, disorders of consciousness were classified into more levels instead of just vegetative state and minimally conscious state. Thus, the evaluation of consciousness level was clearer. Accurate evaluation was a precondition of prognosis prediction. Therefore, the present results are beneficial for prognosis predicting.
Although these results are exciting, there are some limitations. The number of patients could be further expanded. Due to the number of beds and available research time, there was no time to recruit more subjects. If possible, subjects should include locked-in patients or patients with brain injury but no disorders of consciousness. These kinds of subjects would be helpful to give a more detailed explanation of the results and find out more about how the P300 response is regulated differently among these subjects.
In the present study, vegetative state patients could be differentiated from minimally conscious state patients using auditory ERPs. Long-term follow-ups verified that the present design could provide a way to predict consciousness recovery. In future clinical work, patients prone to being aware will receive direct and timely treatment, while seriously injured patients will be admitted to nursing homes rather than receiving endless treatments. This will reduce the waste of medical resources. Future work using functional MRI is needed to observe whether SON and SDN activate similar brain areas to verify the utility of SDN and disclose the mechanisms underlying the DO paradigm.
Acknowledgments:
We gratefully acknowledge the cooperation of the subjects included in this study and we are grateful to Lun Zhao from Beijing Yiran Sunny Electronic Technology Co., Ltd., Beijing, China for his contribution to the statistic analysis.
Footnotes
Funding: This work was supported by grants from the National Natural Science Foundation of China, No. 81371194.
Conflicts of interest: None declared.
Copyedited by McGowan D, Norman C, Wang J, Yang Y, Li CH, Song LP, Zhao M
References
- Ashwal S, Cranford R, Bernat J, Celesia G, Coulter D, Eisenberg H, Myer E, Plum F, Walker M, Watts C. Medical aspects of the persistent vegetative state. N Engl J Med. 1994;330:1499–1508. [Google Scholar]
- Cavinato M, Freo U, Ori C, Zorzi M, Tonin P, Piccione F, Merico A. Post-acute P300 predicts recovery of consciousness from traumatic vegetative state. Brain Inj. 2009;23:973–980. doi: 10.3109/02699050903373493. [DOI] [PubMed] [Google Scholar]
- Cavinato M, Volpato C, Silvoni S, Sacchetto M, Merico A, Piccione F. Event-related brain potential modulation in patients with severe brain damage. Clin Neurophysiol. 2011;122:719–724. doi: 10.1016/j.clinph.2010.08.024. [DOI] [PubMed] [Google Scholar]
- Coch D, Mitra P, George E. Behavioral and ERP evidence of word and pseudoword superiority effects in 7- and 11-year-olds. Brain Res. 2012;1486:68–81. doi: 10.1016/j.brainres.2012.09.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eichenlaub JB, Ruby P, Morlet D. What is the specificity of the response to the own first-name when presented as a novel in a passive oddball paradigm? An ERP study. Brain Res. 2012;1447:65–78. doi: 10.1016/j.brainres.2012.01.072. [DOI] [PubMed] [Google Scholar]
- Faugeras F, Rohaut B, Weiss N, Bekinschtein T, Galanaud D, Puybasset L, Bolgert F, Sergent C, Cohen L, Dehaene S. Probing consciousness with event-related potentials in the vegetative state. Neurology. 2011;77:264–268. doi: 10.1212/WNL.0b013e3182217ee8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fischer C, Dailler F, Morlet D. Novelty P3 elicited by the subject's own name in comatose patients. Clin Neurophysiol. 2008;119:2224–2230. doi: 10.1016/j.clinph.2008.03.035. [DOI] [PubMed] [Google Scholar]
- Fischer C, Luaute J, Morlet D. Event-related potentials (MMN and novelty P3) in permanent vegetative or minimally conscious states. Clin Neurophysiol. 2010;121:1032–1042. doi: 10.1016/j.clinph.2010.02.005. [DOI] [PubMed] [Google Scholar]
- Giacino JT, Ashwal S, Childs N, Cranford R, Jennett B, Katz DI, Kelly JP, Rosenberg JH, Whyte J, Zafonte R. The minimally conscious state definition and diagnostic criteria. Neurology. 2002;58:349–353. doi: 10.1212/wnl.58.3.349. [DOI] [PubMed] [Google Scholar]
- Holeckova I, Fischer C, Giard MH, Delpuech C, Morlet D. Brain responses to a subject's own name uttered by a familiar voice. Brain Res. 2006;1082:142–152. doi: 10.1016/j.brainres.2006.01.089. [DOI] [PubMed] [Google Scholar]
- Holeckova I, Fischer C, Morlet D, Delpuech C, Costes N, Mauguière F. Subject's own name as a novel in a MMN design: a combined ERP and PET study. Brain Res. 2008;1189:152–165. doi: 10.1016/j.brainres.2007.10.091. [DOI] [PubMed] [Google Scholar]
- Hong JS, Lee JH, Yoon YH, Choi JH, Shin JE, Kim SM, Park YG. The assessment of reliability of cognitive evoked potential in normal person. Ann Rehabil Med. 2013;37:263–268. doi: 10.5535/arm.2013.37.2.263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kalmar K, Giacino JT. The JFK coma recovery scale-revised. Neuropsychol Rehabil. 2005;15:454–460. doi: 10.1080/09602010443000425. [DOI] [PubMed] [Google Scholar]
- Kotchoubey B, Lang S, Mezger G, Schmalohr D, Schneck M, Semmler A, Bostanov V, Birbaumer N. Information processing in severe disorders of consciousness: vegetative state and minimally conscious state. Clin Neurophysiol. 2005;116:2441–2453. doi: 10.1016/j.clinph.2005.03.028. [DOI] [PubMed] [Google Scholar]
- Majerus S, Gill-Thwaites H, Andrews K, Laureys S. Behavioral evaluation of consciousness in severe brain damage. Prog Brain Res. 2005;150:397–413. doi: 10.1016/S0079-6123(05)50028-1. [DOI] [PubMed] [Google Scholar]
- Muller-Gass A, Macdonald M, Schröger E, Sculthorpe L, Campbell K. Evidence for the auditory P3a reflecting an automatic process: elicitation during highly-focused continuous visual attention. Brain Res. 2007;1170:71–78. doi: 10.1016/j.brainres.2007.07.023. [DOI] [PubMed] [Google Scholar]
- Perrin F, Schnakers C, Schabus M, Degueldre C, Goldman S, Brédart S, Faymonville M-E, Lamy M, Moonen G, Luxen A. Brain response to one's own name in vegetative state, minimally conscious state, and locked-in syndrome. Arch Neurol. 2006;63:562–569. doi: 10.1001/archneur.63.4.562. [DOI] [PubMed] [Google Scholar]
- Raettig T, Kotz SA. Auditory processing of different types of pseudo-words: an event-related fMRI study. Neuroimage. 2008;39:1420–1428. doi: 10.1016/j.neuroimage.2007.09.030. [DOI] [PubMed] [Google Scholar]
- Risetti M, Formisano R, Toppi J, Quitadamo LR, Bianchi L, Astolfi L, Cincotti F, Mattia D. On ERPs detection in disorders of consciousness rehabilitation. Front Hum Neurosci. 2013;7:775. doi: 10.3389/fnhum.2013.00775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruby P, Blochet C, Eichenlaub JB, Bertrand O, Morlet D, Bidet-Caulet A. Alpha reactivity to complex sounds differs during REM sleep and wakefulness. PLoS One. 2013;8:e79989. doi: 10.1371/journal.pone.0079989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schnakers C, Perrin F, Schabus M, Majerus S, Ledoux D, Damas P, Boly M, Vanhaudenhuyse A, Bruno MA, Moonen G. Voluntary brain processing in disorders of consciousness. Neurology. 2008;71:1614–1620. doi: 10.1212/01.wnl.0000334754.15330.69. [DOI] [PubMed] [Google Scholar]
- Schnakers C, Vanhaudenhuyse A, Giacino J, Ventura M, Boly M, Majerus S, Moonen G, Laureys S. Diagnostic accuracy of the vegetative and minimally conscious state: clinical consensus versus standardized neurobehavioral assessment. BMC Neurol. 2009;9:35. doi: 10.1186/1471-2377-9-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Semlitsch HV, Anderer P, Schuster P, Presslich O. A solution for reliable and valid reduction of ocular artifacts, applied to the P300 ERP. Psychophysiology. 1986;23:695–703. doi: 10.1111/j.1469-8986.1986.tb00696.x. [DOI] [PubMed] [Google Scholar]
- van Dinteren R, Arns M, Jongsma ML, Kessels RP. P300 development across the lifespan: a systematic review and meta-analysis. PLoS One. 2014;9:e87347. doi: 10.1371/journal.pone.0087347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang Q, Huang H, Mao L. N400 repetition effect in unidentifiable Chinese characters: evidence for automatic process. Neuroreport. 2009;20:723–728. doi: 10.1097/WNR.0b013e32832ad310. [DOI] [PubMed] [Google Scholar]