

Abstract
Extra-adrenal myelolipoma is an uncommon entity. But myelolipoma located in the bone is extremely rare. We report a case of myelolipoma occurring in an unusual site: the Costa. It was demonstrated by Computed tomography (CT) scan that an expansive bony mass with heterogeneous low density contents adhered to the 6th ribs. The mass was successful resected and which was yielded to a bony lump through grossly inspection. Histological, the mass was confirmed as an intraosseous myelolipoma, with mature adipocytes mixed with hemopoietic cells. To the authors’ knowledge, it is the first reported that myelolipoma located in the rib in human beings.
Keywords: Extra-adrenal myelolipoma, intraosseous myelolipoma, costa
Introduction
Myelolipoma is an uncommon benign tumor, which consisting of mature adipose tissue and hematopoietic elements [1]. This lesion was first described by Gierke in 1905 and was named myelolipoma by Oberling in 1929 [2]. Myelolipomas most commonly occur in the adrenal glands, but extra-adrenal myelolipomas are rare with a few cases of kidney, perirenal part, presacral region, retroperitoneum, pelvis, spleen, and chest in the literature [2-4]. And fewer cases had been reported in the bone [5-7]. Herein, we present a case of primary myelolipoma occurring in the Costa of an 18-year-old Chinese man.
Case presentation
An 18-year-old man, who was a student, was admitted to the Guizhou Provincial People’s Hospital due to by chance found a mass in the left anterior chest during a routine physical exam. No other complaints or previous disease were noted. Physical examination did not reveal any other abnormalities, such as hepatosplenomegaly, lymphadenopathy or adrenal mass. Laboratory studies revealed no abnormal findings on blood and urine routine examination, renal and liver function tests. Only chest CT scan showed that a mass was derived from the anterior 6th rib, well-circumscribed osseous mass with heterogeneous low density contents, and irregularly sclerosis at the rim of lesions (Figure 1).
Figure 1.
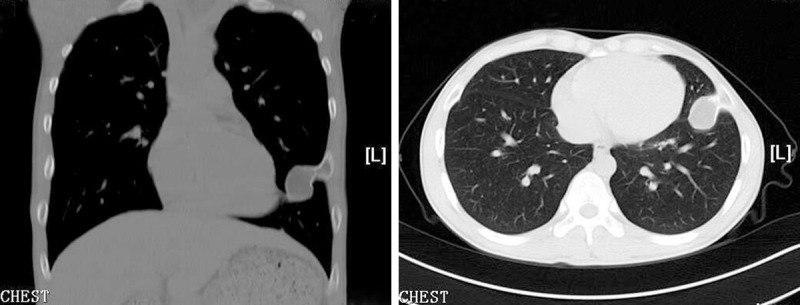
Chest CT scan shows an expanding bony mass adhering to the left anterior 6th rib.
Under the C-arm positioning, the patient was performed with a surgical procedure. After that, the mass and part of costal pleura and ribs were radically excised, which was extrinsic and adherent to the 6th ribs. The wall of mass had thin, crisp and fragile characters. There were some reddish and yellowish soft tissues in the middle of the mass. The excised specimen was measured 2.0 cm × 2.0 cm × 1.5 cm and was described as a bony mass, and this lesion destroyed cortical bone and without any trabeculae bone in the middle of the mass.
Histological examination revealed that this lesion was a bony shell around soft tissues. The soft tissues composed of fewer atrophy trabeculae bone and more tissue, which was mature adipocytes mixed with hemopoietic cells. Hemopoietic cells consisting of trilineage elements: myeloid, erythroid and megakaryocytic cells, and local reticular fibers (Figure 2).
Figure 2.
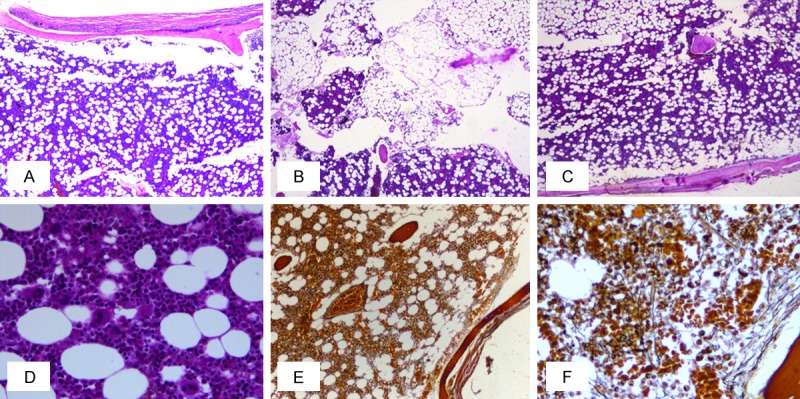
Photomicrograph from the obtained surgical specimen using hematoxylin and eosin (H&E) staining (images A-D) and reticulin staining (images E and F). Images A-C (× 40) showed mature adipose tissue with prominent cellular stroma. Images D was a higher magnification (× 400) views which showed that the stroma consisted of all three hematopoietic cell lineages: myeloid, erythroid, and megakaryocytic forming cell lines. A few plasma cells and lymphocytes were also scattered within the marrow. Images E (× 100) and F (× 400) showed that local reticular fibers were increased.
The patient recovered well from the surgery without any complications, and was discharged on the 8th postoperative day. There were not any complications or tumor recurrences during 2 years of follow-up.
Discussion
Myelolipoma is a benign tumor. It mostly occurs in the adrenal glands, and extra-adrenal myelolipoma is infrequent. The etiology of myelolipoma is still unclear and they are considered a type of extramedullary myeloid proliferation.
Our review of the literature demonstrates there have been about 60 reported cases of extra-adrenal myelolipomas, some with multiple lesions and locations including: nasal cavity, Pulmonary-bronchus, pleural, liver, hepatic falciform ligament, mediastinum, renal, perirenal, paravertebral, intraperitoneal, retroperitoneal, presacral, and even in the bone [2-7]. Based on this review, we know that intraosseous myelolipomas are much less, and our case is the 5th case of intraosseous myelolipomas reported in literature. But in the rib, it is the first time to be described.
And costal myelolipoma has been pathomorphologically diagnosed. The imaging shows that trabeculae bone are atrophy and even disappeared, and which are replaced by more tissue with mature adipocytes mixed with hemopoietic cells. Hemopoietic cells are made up of trilineage elements: myeloid, erythroid and megakaryocytic cells. A few mature plasma cells and lymphocytes are also scattered within the marrow. The normal cellular maturation sequence is maintained and there are no abnormalities in the morphology of the cells. In the local areas, reticular fibers are increased. These images like as those cases which were referred ahead [5-7].
The imaging of differential diagnosis is mainly hyperplasia of the hematopoietic marrow in this site [8-10]. Hyperplasia of the hematopoietic marrow is a deviation from the accepted adult pattern of red-yellow marrow distribution, with an augmentation of the red components. A benign form of hematopoietic hyperplasia is associated with heavy smoking, long distance running, and obesity. A more significant form of hematopoietic hyperplasia is observed in association with malignancies and chronic anemia, while intraosseous myelolipomas are not associated with an underlying systemic disease [10].
In conclusion, the tumor location has not been reported up to now, and costal myelolipoma should be known and mentioned in case of adipose-containing tumor. Furthermore, intraosseous myelolipomas are rare, till now, only 5 cases have been reported, and these locations include humerus, acetabulum [5], femur [5,7], mandible [6]. And the differential diagnosis mainly includes focal hematopoietic hyperplasia and hyperplasia of the hematopoietic marrow in this location.
Management options for intraosseous myelolipoma include conservative and surgical approaches depending upon the certainty of the diagnosis and the progression of the patient’s symptoms. It is generally impossible to distinguish this entity from other bone tumors by radiographic differentiation. So the final diagnosis should depend on pathological features of the surgically removed sample.
Disclosure of conflict of interest
None.
References
- 1.Damjanov I, Katz SM, Catalano E, Mason D, Schwartz AB. Myelolipoma in a heterotopic adrenal gland: light and electron microscopic findings. Cancer. 1979;44:1350–1356. doi: 10.1002/1097-0142(197910)44:4<1350::aid-cncr2820440428>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 2.Wood WG, Restivo TE, Axelsson KL, Svahn JD. Myelolipoma in the spleen: a rare discovery of extra-adrenal hematopoietic tissue. J Surg Case Rep. 2013;2013:rjt007. doi: 10.1093/jscr/rjt007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shen C, Han Z, Che G. A bilateral neoplasm in chest: a case report and literature review. BMC Surg. 2014;14:42. doi: 10.1186/1471-2482-14-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sagan D, Zdunek M, Korobowicz E. Primary myelolipoma of the chest wall. Ann Thorac Surg. 2009;88:e39–41. doi: 10.1016/j.athoracsur.2009.06.085. [DOI] [PubMed] [Google Scholar]
- 5.Sundaram M, Bauer T, von Hochstetter A, Ilaslan H, Joyce M. Intraosseous myelolipoma. Skeletal Radiol. 2007;36:1181–1184. doi: 10.1007/s00256-007-0347-x. [DOI] [PubMed] [Google Scholar]
- 6.Chiarini L, Bertoldi C, Criscuolo M, Ferronato G. Myelolipomatosis. A report of a case located in the mandible. Minerva Stomatol. 1992;41:165–172. [PubMed] [Google Scholar]
- 7.Papapietro N, Martinelli N, Ippolito M, Amato C, Denaro V. Intraosseous myelolipoma within proximal femoral metaphysis in a patient with previous prostate cancer: a case report. Hip Int. 2009;19:283–286. doi: 10.1177/112070000901900317. [DOI] [PubMed] [Google Scholar]
- 8.Edelstein G, Kyriakos M. Focal hematopoietic hyperplasia of the rib--a form of pseudotumor. Skeletal Radiol. 1984;11:108–118. doi: 10.1007/BF00348798. [DOI] [PubMed] [Google Scholar]
- 9.Galindo LM, Soans S, Chiaramonte C, Garcia FU. Focal hematopoietic hyperplasia of the rib. Report of a case diagnosed by fine needle aspiration. Acta Cytol. 1998;42:987–990. doi: 10.1159/000331982. [DOI] [PubMed] [Google Scholar]
- 10.Lee KB, Kim BS, Cho JH. Focal hematopoietic hyperplasia of the rib. Skeletal Radiol. 2002;31:175–178. doi: 10.1007/s00256-001-0457-9. [DOI] [PubMed] [Google Scholar]