

Summary
Estimation of the total body surface area burned (%TBSA) following a burn injury is used in determining whether to transfer the patient to a burn center and the required fluid resuscitation volumes. Unfortunately, the commonly applied methods of estimation have revealed inaccuracies, which are mostly related to human error. To calculate the %TBSA (quotient), it is necessary to divide the burned surface area (Burned BSA) (numerator in cm2) by the total body surface area (Total BSA) (denominator in cm2). By using everyday objects (eg. credit cards, smartphones) with well-defined surface areas as reference for estimations of Burned BSA on the one hand and established formulas for Total BSA calculation on the other (eg. Mosteller), we propose an approximation method to assess %TBSA more accurately than the established methods. To facilitate distribution, and respective user feedback, we have developed a smartphone app integrating all of the above parameters, available on popular mobile device platforms. This method represents a simple and ready-to-use clinical decision support system which addresses common errors associated with estimations of Burned BSA (=numerator). Following validation and respective user feedback, it could be deployed for testing in future clinical trials. This study has a level of evidence of IV and is a brief report based on clinical observation, which points to further study.
Keywords: burns, decision support systems, clinical, fluid therapy, burn surface area estimation
Abstract
L’estimation de la totale de la surface corporelle brûlée (% de la SCT) à la suite d’une brûlure est importante en déterminant le transfert du patient vers un centre de brûlés et les volumes nécessaires des fluides de réanimation. Malheureusement, les méthodes d’estimation couramment appliquées ont révélé des inexactitudes, qui sont principalement liés à l’erreur humaine. Pour calculer le % de la SCT il faut diviser la surface brûlée (numérateur en cm2) de la surface corporelle totale (dénominateur en cm2). En utilisant des objets du quotidien (par exemple cartes de crédit et smartphones) avec des surfaces bien définies comme référence pour les estimations de la SC brûlée d’une part, et des formules établies pour le calcul de la SC totale sur l’autre (par exemple Mosteller), nous proposons une méthode d’approximation d’évaluer le % de la SCT brûlée plus de précision que les méthodes établies. Pour faciliter la distribution, et les commentaires des utilisateurs, nous avons développé une application intégrant tous les paramètres ci-dessus, disponibles sur les plates-formes d’appareils mobiles populaires. Cette méthode représente un système simple et prêt à l’emploi aide à la décision clinique qui traite les erreurs courantes associées aux estimations de BSA brûlé (= numérateur). Après la validation et la rétroaction des utilisateurs, il pourrait être déployé pour les tests dans les futurs essais cliniques. Cette étude a un niveau de preuve IV et elle présente un bref rapport basé sur l’observation clinique, qui pointe vers une étude plus approfondie.
Introduction
It is important that the assessment of burn size be performed accurately and adequately as the outcome can impact on the decision whether or not to transfer the patient to a burn center and on the initial volume requirement for fluid resuscitation, among other things.
The majority of assessments of percentages of total burn surface area (%TBSA) to-date have revealed inaccuracies, mostly related to human error, with overestimations of more than 100% identified in emergency departments.1-4
Three predominantly used and established methods of burn size estimation are:
In adults, the "Rule of Nines" is used to determine the total percentage of burned regions per body segment.6 In some cases, burn injuries only partially affect a region or even extend beyond it, and thus such burns are measured using the palm of the injured person as a reference representative of 1% of body surface area ("Rule of Palm").5 According to previous reports, the Rule of Palm (Fig. 1) can lead to overestimations of about 10–20%8,9 because, in adults, the surface area of the palm, including the fingers, represents only 0.8 %TBSA in men and 0.7 %TBSA in women. Excluding the fingers, the averages are as low as 0.5 and 0.4 %TBSA in men and women respectively. In children, the palm approximates 0.92 and 0.52 %TBSA with and without the fingers, respectively. According to Wallace, and cited by Knaysi,6 the Rule of Nines (Fig. 1) is quite accurate in persons weighing about 10–80kg. However, overestimations of %TBSA by use of the Rule of Nines occur,10 especially in persons with higher body-mass indices.11 To overcome this, a proportionate adaptation previewed a "Rule of Five" for persons >80 kg, and a "Rule of Eight" for those <10 kg of body weight.12
Fig. 1. "Rule of Nines" and "Rule of Palm".

The Lund-Browder charts7 take into account body proportions associated with different ages and are more precise than the Rule of Nines. Even so, overestimations have still been reported: Alm13 reported an average overestimation of 17.8% in 90% of cases, Nichter4 reported 12.4% and Berry11 identified overestimations of 154% in 25 out of 60 cases.
Furthermore, we have previously demonstrated that, regardless of the chosen methodology for estimating surface areas, notably small, scattered burn areas pose a problem when estimating total burn surface area.1
In order to optimize clinical decision-making following a burn or scald injury, objectivation of TBSA assessments is well warranted and new methods predominantly based on computer-aided technologies have emerged.14-17 Smartphones based on different mobile platforms (eg. iOS, Android, Blackberry, Windows Mobile etc.) are not just very popular among the general population, but also among medical staff. These mobile devices are able to perform automated calculations and to transmit data securely.
This report is based on the idea that everyday objects (eg. credit cards, smartphones) have a distinct well-defined surface area, and that these objects can serve as reference for surface area estimations.
Methods
For calculation of the %TBSA, it is necessary to divide the burned surface area (Burned BSA) (numerator, in cm2) by the total body surface area (Total BSA) (denominator, in cm2).
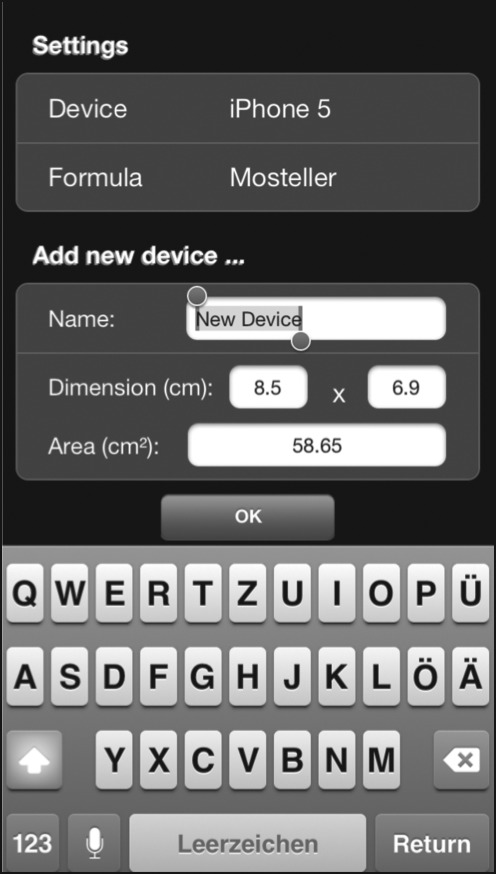
In a mobile application, we incorporated well-defined surface areas (in cm2) of everyday objects like credit cards or smartphones as a reference tool for burn surface area estimations. For known objects, these surface areas have been predefined, but a free input option for other dimensions of known surface areas of other squared or rectangular devices is available (Fig. 2).
Fig. 2. Graphical user interface (GUI) A. The user can choose between different preinstalled references of known surface area (= "Device", eg. smartphones). Optionally, new devices for burn size estimation (eg. credit card) can be added by defining its surface area dimensions and saving it under a new device name (e.g. credit card).
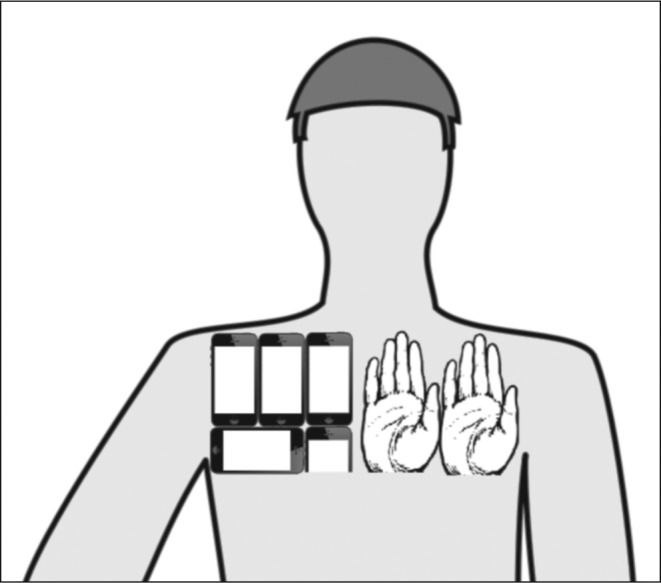
In our proposed scenario, the user estimates how often a predefined known surface area object (as mentioned above) fits into a burn surface area (Fig. 3), which will render the burned surface area as calculated by the app in cm2.
Fig. 3. Graphical user interface (GUI) B. Comparable to the "Rule of Palm", the user estimates how often the surface area of a predefined device (e.g. iPhone) fits into the burn surface area.
The other parameters to be entered in the app are weight and height of the patient, which will calculate the total body surface area by use of the selected predefined formula in cm2 (eg. Mosteller, DuBois DuBois). The final result of the entered parameters is the then calculated % TBSA by the app (Fig. 4).
Fig. 4. Graphical user interface (GUI) C. Having selected the height and weight of the patient, the app calculates the total burn surface area (Total BSA). After the user has selected the number of times the predefined device fits into the burn surface area, the app then calculates the burn surface area (Burned BSA) and reveals the calculated %TBSA.

Verification
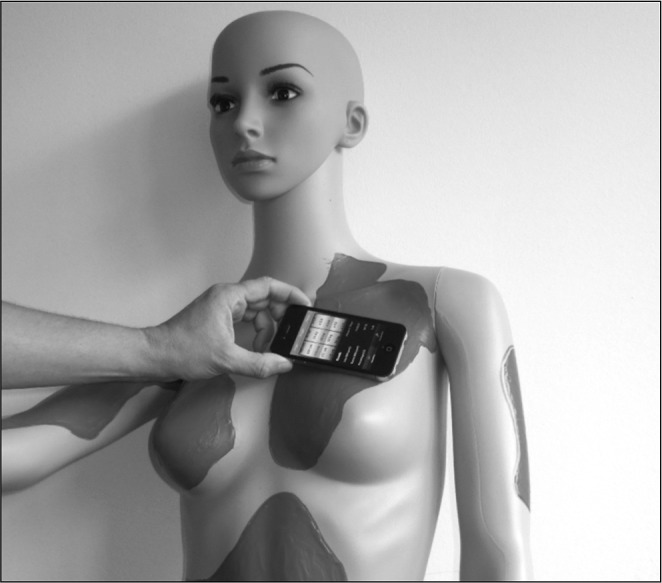
For verification of the app, 30 burnt areas (test areas) have been designed using a special liquid on three mannequins (one male, one female and one child - burn sizes ranging from 1% to 15% TBSA, 10 burnt areas on each mannequin) (Fig. 5).
Fig. 5. Example: Test area (# F5) left shoulder and breast: - Total body surface area of the mannequinn = 15335 cm2. - The iPhone 4 fits 3.5 times into the test area: 3.5 times iPhone 4 = 236 cm2 236/15335= 1.54 % of the TBSA (estimated by the Rapid Burn Assessor). - Real size of the test area= 251.3 cm2 251/15335= 1.63% (measured by the scanner).
After completion of test size estimations, these test areas have been pulled off and transferred onto a flat-bed scanner (Brother MFC-9420CN) and the area (in cm2) was measured by use of ImageJ™ for computer based planimetric measurements. For calculation of the %TBSA, the test areas (in cm2) were divided by the total body surface areas (TBSA in cm2).
In order to evaluate the total body surface areas of the mannequinns, all 3 mannequins have been scanned by use of the TOF-3D-Scanner and by use of the Software ReconstructMe ™ (Profactor) and the total body surface area in % was calculated.
Results
To put to use this simple method of %TBSA estimations, we have developed a free mobile application called the "Rapid Burn Assessor" for Apple iOSTM and Google AndroidTM, which has integrated the above-mentioned formulas and calculation methods. In order to validate the results, we took 30 test areas in the range from 62.7cm2 to 966.3cm2 on 3 mannequins. The differnce (in %) between the test areas (in cm²) assessed with the RBA-Tool and the measured areas was 6.16%. The difference concerning TBSA burned (in %) was 0.1% TBSA.
Discussion
To optimize resources for transfers to burn centers and initial fluid resuscitation volumes, we have developed a simple and cost-efficient tool for health-care professionals (eg. first-responders, GPs, nursing staff, medical/surgical specialists etc.) for improving %TBSA estimations. Estimation errors related to and/or based on incorrect %TBSA assessments may affect clinical decision-making and, in the extreme, can result in either hypovolemic shock and cardiac failure (under-estimation) or abdominal/extremity compartment syndrome, pulmonary edema and electrolyte imbalance (over-estimation).1
Although our proposed method of estimation is subject to some inaccuracies (resulting from human error, variations of body weight/height), it does at least represent a simplified approximation that reduces the common errors associated with burn surface area estimations by using an everyday reference of known size. Even though the idea of a reference tool (eg. Rule of Palms) is not new, to the best of our knowledge, this is the first published attempt in over 30 years to improve one side of the mathematical formula, namely the burn surface area.
This approach can be useful for small-scattered burn surface areas, which are the most common kind of burn injury encountered in daily clinical practice and have been demonstrated to result in the most inaccurate assessments by the above-cited methods.1,17
In order to improve %TBSA estimations, further objectivity is required, which could include, for example, full body scans with mobile scanners used to assess total body surface area burned.
In this context, the "Rapid Burn Assessor" is a very simple and cost-efficient support system for clinical decision- making related to burn/scald injuries, applicable and ready to use, even in an emergency setting. This brief report encourages active user feedback to facilitate deployment and improvement of the mobile application for future validation and testing in clinical trials.
Acknowledgments
Conflict of interest. None
Funding. None
References
- 1.Giretzlehner M, Dirnberger J, Owen R, Haller HL, Lumenta DB, Kamolz LP. The determination of total burn surface area: How much difference? Burns. 2013 doi: 10.1016/j.burns.2013.01.021. Epub. [DOI] [PubMed] [Google Scholar]
- 2.Chan QE, Barzi F, Cheney L, Harvey JG, Holland AJA. Burn size estimation in children: Still a problem. Emerg Med Australas. 2012;24:181–6. doi: 10.1111/j.1742-6723.2011.01511.x. [DOI] [PubMed] [Google Scholar]
- 3.Jose RM, Roy DK, Vidyadharan R, Erdmann M. Burns area estimation – an error perpetuated. Burns. 2004;30:481–2. doi: 10.1016/j.burns.2004.01.019. [DOI] [PubMed] [Google Scholar]
- Nichter LS, Bryant CA, Edlich RF. Efficacy of burned surface area estimation calculated from charts – the need for a computerbased model. J Trauma. 1985;25:477–81. doi: 10.1097/00005373-198506000-00001. [DOI] [PubMed] [Google Scholar]
- 5.Rossiter ND, Chapman P, Haywood IA. How big is a hand? Burns. 1996;22:230–1. doi: 10.1016/0305-4179(95)00118-2. [DOI] [PubMed] [Google Scholar]
- 6.Knaysi GA, Crikelair GF, Cosman B. The rule of nines: Its history and accuracy. Plast Reconstr Surg. 1968;41:560–3. [PubMed] [Google Scholar]
- 7.Lund CC, Browder NC. The estimation of area of burns. Surg Gynaecol Obstet. 1944;79:352–8. [Google Scholar]
- 8.Amirsheybani HR, Crecelius GM, Timothy NH, Peiffer M, Saggers GC, Manders EK. The natural history of the growth of the hand: I. Hand area as a percentage of body surface area. Plast Reconstr Surg. 2001;107:726–33. doi: 10.1097/00006534-200103000-00012. [DOI] [PubMed] [Google Scholar]
- 9.Nagl TR, Schunk JE. Using the hand to estimate the surface area of a burn children. Pedatr Emerg Care. 1997;13:254–5. doi: 10.1097/00006565-199708000-00003. [DOI] [PubMed] [Google Scholar]
- 10.Wachtl Tl, Berry CC, Wachtel EE, Frank HA. The inter-rater reliability of estimating the size of burns from various burn area chart drawings. Burns. 2000;26:155–70. doi: 10.1016/s0305-4179(99)00047-9. [DOI] [PubMed] [Google Scholar]
- 11.Berry MG, Evison D, Roberts AH. The influence of body mass index on burn surface estimated from the area of the hand. Burns. 2001;27:591–4. doi: 10.1016/s0305-4179(00)00145-5. [DOI] [PubMed] [Google Scholar]
- 12.Livingston EH, Lee S. Percentage of burned body surface area determination in obese and non-obese patients. J Surg Res. 2000;91:106–10. doi: 10.1006/jsre.2000.5909. [DOI] [PubMed] [Google Scholar]
- 13.Alm J. A retrospective Study of TBSA-B Calculating; Manual estimated burnchart versus computerized burncharts. Final Programme and abstracts. 10th Congress European Burns Association Bergen; Norway. 2003. [Google Scholar]
- 14.Haller H. Data collection in burn injuries – Rationale for Burn-Case 3D. Osteo Trauma Care. 2007;15:34–41. [Google Scholar]
- 15.Haller H, Dirnberger J, Giretzlehner M, et al. "Understanding burns": Research project BurnCase 3D – overcome the limits of existing methods in burns documentation. Burns. 2009;35:311–7. doi: 10.1016/j.burns.2008.07.010. [DOI] [PubMed] [Google Scholar]
- 16.Neuwalder JM, Sampson C, Breuing KH, Orgill DP. A review of computer-aided body surface area determination: SAGE II and EPRI´s 3D Burn Vision. J Burn Care Rehabil. 2002;23:55–9. doi: 10.1097/00004630-200201000-00011. [DOI] [PubMed] [Google Scholar]
- 17.Jeschke MG, Kamolz LP, Sjöberg F, Wolf SE, editors. Handbook of Burns – Volume 1: Acute Burn Care. New York: Springer Wien; 2013. Medical documentation of burn injuries; pp. 117–29. [Google Scholar]