

Abstract
Objectives
The predictive capabilities of skinfold regression equations are limited across populations and current equations may not be well suited for the prediction of body fat in older adults or obese Americans. The goal of this study was to compare percent body fat (%BF) predicted by several skinfold regression equations to %BF determined by Dual-Energy X-ray Absorptiometry (DXA) in obese and non-obese Caucasian men and women in the United states over the age of 65 years.
Design
A block design was used with two blocks: obesity (non-obese/obese) and gender (male/female). All subjects underwent the same testing procedures in one visit.
Setting
University of Pittsburgh Clinical and Translation Research Center.
Participants
Seventy-eight older healthy adults were recruited for participation.
Measurements
Actual percent body fat was determined from a whole body DXA scan. Estimated percent body fat (%BF) was calculated using skinfold measurements and established regression equations. The predictive accuracy of the regression equations was evaluated by comparing the estimated %BF to the actual %BF measured with DXA using a within subject ANOVA (α=0.05). This was done within subgroups: obese males, obese females, non-obese males and non-obese females.
Results
Durnin and Womersly and Jackson and Pollock had reasonably good agreement with DXA in older Caucasian American females and males, respectively. The remaining equations significantly overestimated %BF in older Caucasian American males. Mixed results were found in females with Gause-Nilsson and Jackson and Pollock significantly underestimating %BF, while Visser and Kwok overestimated %BF.
Conclusion
Numerous factors of a population including age, race, ethnicity, gender and obesity should be considered when selecting a skinfold regression equation to estimate %BF. While Durnin and Womersly and Jackson and Pollock are recommended for predicting %BF in older Caucasian American females and males, respectively, there exists a need to develop accurate regression models that consider obesity, gender, race or ethnicity when predicting %BF in a diverse geriatric American population.
Keywords: Aging, obesity, anthropometry, body fat, skinfold
Introduction
Obesity is a growing concern among older adults in the United states. In 2009-2010 nearly three quarters of American adults aged 60 and older were either overweight (25.0 ≤ BMI ≤ 29.9) or obese (BMI ≥ 30.0) (1, 2). Additionally, older adults are more likely to be obese than young adults (2). Obesity has been linked to serious health risks with overweight older adults having a greater risk of impaired physical function and higher risk of injury (3, 4). In 2008, an estimated $147 billion in medical costs were associated with obesity (5). Current trends, specifically an aging population in combination with older adults having the highest rate of obesity increase, suggest that the scope of this problem will likely be steadily increasing as well (1, 2, 6). estimating body fat percentage (%BF) is important in health care and obesity management. With growing obesity rates, accurate and affordable techniques for the estimation %BF in older or obese Americans are necessary.
Dual-Energy X-ray Absorptiometry (DXA) is a well-established method to provide an accurate measure of %BF (7). However, due to cost and other limitations, DXA is not always practical for determining %BF (7-10). Alternative techniques, such anthropometric prediction equations using skinfold thickness, are commonly used to estimate %BF (11-13). The American College of Sports Medicine currently recommends the use of Jackson and Pollock (JP) body density equations combined with an equation to convert to %BF (14-17). These equations were developed from non-obese middle-aged Americans and are based on the assumption that fat is distributed subcutaneously and internally in a similar manner for all individuals (18). It has been shown that fat distribution varies across gender, ethnicity, body type, and age (19, 20). Thus, the predictive capabilities of these skinfold regression equations are limited across populations. As such, these equations, and others, may not be well suited for the prediction of %BF in older or obese Caucasian Americans.
Skinfold-based regression equations used to predict %BF specifically in older adults have been published, including Visser (V), Durnin and Womersly (DW), Gause-Nilsson (GN) and Kwok (K) (21-24). Due to their inherent bias towards the populations used for development, attempts at validation of these equations have yielded mixed results in various populations of older adults. Two studies found DW to accurately predict %BF in non-obese (25, 26), while other studies found that DW overestimated %BF in males and underestimated %BF in females (23, 27) or underestimated %BF in middle-aged obese Americans (28, 29). Previous research has found that JP significantly underestimate %BF in older non-obese and middle-aged obese Americans (18, 28, 30). Additionally, previous studies have suggested that V overestimates %BF in non-obese older Portuguese and Swedish populations (23, 31). To our knowledge, no studies have examined DW, JP, V or K in an obese older Caucasian American population. As previously mentioned, %BF and fat distribution vary across age, ethnicity, race and obesity, as such, the aforementioned regression equations may not be well suited for an older obese Caucasian population in the United States.
It has yet to be established which %BF prediction equations, if any, are best suited for an older obese Caucasian population in the United States. In order to understand the effects of age and obesity on the accuracy of %BF predictive equations, the aim of this study was to compare %BF predicted by several skinfold regression equations to %BF determined by DXA in obese and non-obese men and women in the United States over the age of 65 years.
Methods
Seventy-eight healthy Caucasian American adults aged 65 and older, screened for metal implants, were recruited from the community. Participants were divided into four subgroups based on gender (female; male) and obesity determined from body mass index (BMI≤30, non-obese; BMI>30, obese) (Table 1). Written informed consent, previously approved by the University of Pittsburgh Institutional Review Board, was obtained from each participant. Participants underwent a whole body DXA scan (Hologic QDR 1000/W, Bedford, MA, USA) lying supine and %BF was determined as total body fat mass/total body mass.
Table 1. Subject Population Characteristics.
| Mean (SD) [Range] | Females | Males | ||
|---|---|---|---|---|
| Non-obese (n=20) | Obese (n=19) | Non-obese (n=20) | Obese (n=19) | |
| Age (yrs) | 75.97 (5.27) [66.95-85.66] | 75.91 (4.99) [66.69-83.68] | 76.02 (5.58) [65.68- 85.02] | 74.17 (4.47) [66.46-82.24] |
| BMI (kg/m2) | 25.08 (3.07) [19.86-29.76] | 34.27 (3.94) [30.18-47.03] | 26.31 (2.70) [19.75-29.71] | 33.70 (3.24) [30.14-41.26] |
| Mass (kg) | 62.95 (7.15) [52.2-76.50] | 85.08 (13.33) [65.3-124.2] | 79.40 (10.78) [56.00-97.10] | 101.61 (15.05) [83.30-133.81] |
| Height (m) | 1.59 (0.06) [1.46-1.66] | 1.57 (0.07) [1.46-1.71] | 1.73 (0.06) [1.62-1.82] | 1.73 (0.06) [1.62-1.85] |
Skinfold thickness measurements (ST) were performed by a trained technician with a Lange skinfold caliper (Beta Technology Inc, Cambridge, MD, USA) at chest, midaxillary, tricep, bicep, subscapular, abdomen, suprailiac, and thigh sites on the right side of the body while standing in a relaxed position. Measurements were taken three times at each site and averaged. Body fat percentage was calculated for each regression equation using the appropriate skinfold measurements (Table 2). V, DW and JP were converted to %BF using Siri's 2-compartment equation (32). Siri's equation was selected to allow for comparisons to previous research (18, 22, 25-27, 29, 30, 33). It should also be noted that Heyward et al. has previously reported nearly identical %BF estimates using either Siri's equation or Brozek's equation (18).
Table 2. Skinfold thickness equations to estimate %BF.
| Model | Ref. No. | Equation |
|---|---|---|
| Visser 4 skinfold (V) | [21] | BD = 1.0688 + 0.0212(SexA) − 0.0356log10 (Sum 4) |
| Durnin and Womersley (DW) | [22] | |
| Men | BD = 1.1715 - 0.0779log10(Sum 4) | |
| Women | BD = 1.1339 − 0.0645log10(Sum 4) | |
| Gause-Nilsson (GN) | [23] | %BF = 36.078 + 3.917log10(Sum 4) - 5.114(SexA) + 0.384(Weight) - 0.289(Height) |
| Jackson and Pollock (JP) | [8,9] | |
| Men | BD = 1.112 - 0.00043499(Sum 7) + 0.00000055(Sum 7)2 - 0.00028826(Age) | |
| Women | BD = 1.097 - 0.00046971(Sum 7) + 0.00000056(Sum 7)2 - 0.00012828(Age) | |
| Kwok | [24] | %BF = -27.149 + 6.137(SexB) + 1.120(BMI) + 17.308 log10(Sum 2) |
%BF, body fat percentage; BD, body density (kg/m3); SexA, female=0, male=1; Sum 4, triceps + biceps + subscapular + suprailliac; Sum 2, triceps + biceps; Sum 7, chest + midaxillary + triceps + subscapular + abdomen + suprailiac + thigh; age, age in years; SexB, female=2, male=1; Weight (kg); Height (cm)
Statistical analysis consisted of comparing %BF determined from DXA to %BF determined from each skinfold equation (Table 2). ANOVAs were performed within each subgroup of participants (obese males, obese females, non-obese males, non-obese females). Method type (DXA/JP/V/DW/GN/K) was included as an independent fixed effects and subject as a random effect. The dependent variable was %BF. Statistical significance was set at 0.05 and post hoc analysis was performed using Tukey tests to compare %BF determined from DXA to %BF determined from each skinfold equation (Table 2).
Results
Mean %BF by method type (DXA/JP/V/DW/GN/K) for each subgroup is presented in Table 3. The main effect of method type was statistically significant for all subgroups (p<0.0001).
Table 3. Mean %BF Across Method Types By Gender and Obesity.
| Mean (SD) [Range] Method | Females | Males | ||
|---|---|---|---|---|
| Non-obese (n=20) %BF | Obese (n=19) %BF | Non-obese (n=20) %BF | Obese (n=19) %BF | |
| DXA | 34.18 (6.23) | 44.64 (3.06) | 25.47 (5.54) | 32.96 (4.21) |
| [21.00-41.80] | [40.40-52.10] | [15.60-36.60] | [25.20-41.90] | |
| V | 42.45 (2.55)* | 46.28 (1.08) | 32.07 (1.75)* | 35.36 (1.61)* |
| [36.59-45.63] | [43.41-47.76] | [29.02-35.98] | [31.16-38.41] | |
| DW | 35.96 (4.50) | 42.76 (1.92) | 29.07 (3.78)* | 36.28 (3.52)* |
| [25.71-41.59] | [37.64-45.39] | [22.53-37.59] | [27.11-42.99] | |
| GN | 30.71 (3.31)* | 40.07 (5.23)* | 31.82 (4.29)* | 41.12 (5.99)* |
| [26.08-36.37] | [32.42-55.18] | [22.42-38.56] | [34.18-54.16] | |
| JP | 27.06 (5.01)* | 37.02 (3.57)* | 23.08 (3.96) | 31.35 (3.90) |
| [16.17-33.02] | [27.68-42.91] | [17.69-33.73] | [21.77-39.07] | |
| K | 39.15 (5.28)* | 52.52 (4.66)* | 33.21 (4.11)* | 44.52 (4.97)* |
| [28.88-46.99] | [46.07-65.99] | [24.67-41.28] | [37.42-55.43] | |
Denotes significantly different than DXA (p<0.05). Body Fat Percentage (%BF).
In females, post hoc-analysis revealed that GN and JP significantly underestimated %BF compared to DXA by 3.47%BF and 7.12%BF (mean of within subject differences from DXA) in non-obese females and by 4.57%BF and 7.62%BF in obese females, respectively. V was found to significantly overestimate %BF by 8.26%BF in non-obese females, while in obese subjects there was no significant difference. No significant difference was found between DW %BF and DXA %BF in females regardless of obesity (Figure 1). K significantly overestimated %BF in both non-obese and obese females by 4.97%BF and 7.88%BF, respectively.
Figure 1.
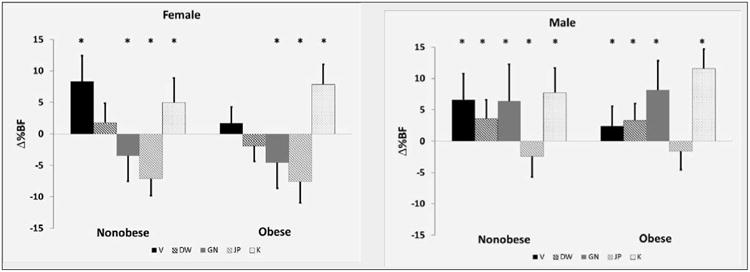
Mean Δ%BF (mean of within subject differences from DXA) for females (left) and males (right). Visser (V) shown by solid black bars, Durnin and Womersley (DW) shown by hashed black bars, Gause_Nilsson (GN) shown by solid gray bars, Jackson and Pollock (JP) shown by hashed gray bars and Kwok (K) shown by dotted bars. Standard deviations are provided. * Denotes significantly different from DXA for each group (p<0.05)
GN and DW significantly overestimated %BF by 6.35%BF and 3.61%BF in non-obese males and by 8.16%BF and 3.32%BF in obese males, respectively. Additionally, V and K significantly overestimated %BF in non-obese males by 6.60%BF and 7.74%BF and in obese males by 2.41%BF and 11.56%BF, respectively. JP %BF was not significantly different than DXA regardless of obesity in males (Figure 1).
Discussion
The goal of this study was to compare %BF determined by DXA to estimated %BF determined by several regression equations using skinfold measurements in non-obese and obese older adults in the United States. Not all regression equations in this study accurately predicted %BF in older Americans. Obesity and gender significantly impacted the accuracy of the skinfold regression equations in varying ways when applied to an older Caucasian American population.
In older Caucasian Americans, DW accurately predicted %BF in females but significantly overestimated %BF in males, regardless of obesity. Previous studies have found mixed results when analyzing the accuracy of DW. Reilly et al. reported no significant differences between DW %BF and %BF in the older adults of the United Kingdom (26). Others found that it underestimated %BF in obese middle-aged females (28, 29). Additionally, studies outside of the United States found conflicting results regarding the accuracy of DW in non-obese males (23, 25-27). DW was found to underestimate %BF in middle-aged obese American males (28, 29). DW was developed using a British population with a larger range of body types and ages. It is also likely more similar in race or ethnicity to American population presented here which could explain its ability to predict %BF in females (22).
JP was found to accurately predict %BF in older Caucasian American males but underestimated %BF in females, regardless of obesity. This is consistent with previous literature which found JP to underestimate %BF in non-obese older females and obese middle-aged females (18, 28, 30). JP was developed in a middle-aged American population with a mean %BF of 24.09% (15), which could account for the underestimation of %BF. Body composition changes with aging as more fat is located internally (18, 20). As such, it is likely that typical skinfold regression equations would underestimate %BF in older adults, especially females.
In general, the remaining regression equations, GN, V and K, did not accurately predict %BF in older Caucasian Americans. GN significantly underestimated %BF in females while overestimating %BF in males. GN used a non-obese Swedish population for the development of their regression equations (23). Although the %BF of GN's population (23) is similar to our non-obese females, GN did not accurately predict %BF in either non-obese or obese females examined. V significantly overestimated %BF in non-obese females and all males, but accurately estimated %BF in obese females. These results, as do previous (31), suggest that V systematically overestimates %BF in non-obese populations due to the body composition of the population used. Visser's female population in the Netherlands, mean %BF of 43.3% and mean BMI of 26.1 kg/m2 (21), had a drastically higher fat content to BMI ratio than the American female population represented in this analysis, mean %BF of 33.4% and mean BMI of 24.9 kg/m2 (non-obese). Thus, V would tend to overestimate %BF in non-obese due to the relatively higher fat content in their population's body composition. Finally, K significantly overestimated %BF in females and males, regardless of obesity. K was developed in a non-obese older Chinese population (24). Differences in obesity, race or ethnicity likely account for the poor prediction accuracy of GN, V and K in our population of older Caucasian Americans.
The population used for this study was an older Caucasian American population and should be considered when applying the findings to other populations. Although a range of body types was used in this analysis, the average BMI of the non-obese groups was close to overweight. While it is possible that different regressions could be more accurate in a normal weight population, the regressions found to be accurate in older Caucasian Americans were accurate regardless of obesity. The equations used for comparison were developed in populations with varying ages, races, ethnicities and incorporated different measurement sites. No clear association between one of these factors and predictive accuracy was obvious. Numerous factors including age, race, ethnicity, gender and obesity should be considered when selecting a predictive regression equation. Finally, DXA was utilized as the reference standard and is a well-established method to provide an accurate measure of %BF (7). Additional accepted methods exist, such as the compartment model, to estimate body composition. While the current findings are limited to DXA as a reference standard, future work should include comparing other accepted reference standards to currently available regression equations.
In conclusion, DW and JP had reasonably good agreement with DXA in older Caucasian American females and males, respectively. The remaining equations significantly overestimated %BF in older Caucasian American males. In general, mixed results were found in females with GN and JP significantly underestimating %BF, while V and K overestimated %BF. These differences translate into potential errors associated with using certain skinfold regression equations to predict %BF in older Caucasian Americans. Numerous factors of a population including age, race, ethnicity, gender and obesity should be considered when selecting a skinfold regression equation to estimate %BF. Additionally, there exists a need to develop accurate regression models that consider obesity, gender, race or ethnicity when predicting %BF in a geriatric American population.
Acknowledgments
Funding and support was provided by The Pittsburgh Claude D. Pepper Older Americans Independence Center (NIH P30 AG024827) & The University of Pittsburgh CTRC (NIH/NCRR/CTRC Grant 1 UL1 RR024153-01). Special thanks to Dr. S. Greenspan, Donna Medich & Adrienne Belasco.
References
- 1.Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. United States: 2012. [DOI] [PubMed] [Google Scholar]
- 2.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity in the United States, 2009-2010. NCHS Data Brief. 2012:1–8. [PubMed] [Google Scholar]
- 3.Lang IA, Llewellyn DJ, Alexander K, Melzer D. Obesity, physical function, and mortality in older adults. United States: 2008. [DOI] [PubMed] [Google Scholar]
- 4.Ostbye T, Dement JM, Krause KM. Obesity and workers' compensation: results from the Duke Health and Safety Surveillance System. United States: 2007. [DOI] [PubMed] [Google Scholar]
- 5.Finkelstein EA, Trogdon JG, Cohen JW, Dietz W. Annual medical spending attributable to obesity: payer-and service-specific estimates. United States: 2009. [DOI] [PubMed] [Google Scholar]
- 6.Shrestha LB, Heisler EJ. In: The Changing Deomgraphic Profile of the United States. Service CR, editor. Washington, DC: 2011. [Google Scholar]
- 7.Salamone LM, Fuerst T, Visser M, Kern M, Lang T, Dockrell M, Cauley JA, Nevitt M, Tylavsky F, et al. Measurement of fat mass using DEXA: a validation study in elderly adults. J Appl Physiol. 2000;89:345–52. doi: 10.1152/jappl.2000.89.1.345. [DOI] [PubMed] [Google Scholar]
- 8.Norgan NG. Laboratory and field measurements of body composition. England: 2005. [DOI] [PubMed] [Google Scholar]
- 9.Heyward VH, Cook KL, Hicks VL, Jenkins KA, Quatrochi JA, Wilson WL. Predictive accuracy of three field methods for estimating relative body fatness of nonobese and obese women. Int J Sport Nutr. 1992;2:75–86. doi: 10.1123/ijsn.2.1.75. [DOI] [PubMed] [Google Scholar]
- 10.Heymsfield SB, Matthews D. Body composition: research and clinical advances--1993 A.S.P.E.N. research workshop. JPEN J Parenter Enteral Nutr. 1994;18:91–103. doi: 10.1177/014860719401800291. [DOI] [PubMed] [Google Scholar]
- 11.Tran ZV, Weltman A. Predicting body composition of men from girth measurements. Hum Biol. 1988;60:167–75. [PubMed] [Google Scholar]
- 12.Tran ZV, Weltman A. Generalized equation for predicting body density of women from girth measurements. Med Sci Sports Exerc. 1989;21:101–4. doi: 10.1249/00005768-198902000-00018. [DOI] [PubMed] [Google Scholar]
- 13.Deurenberg P, Weststrate JA, Seidell JC. Body mass index as a measure of body fatness: age- and sex-specific prediction formulas. England: 1991. [DOI] [PubMed] [Google Scholar]
- 14.Jackson AS, Pollock ML. Generalized equations for predicting body density of men. Br J Nutr. 1978;40:497–504. doi: 10.1079/bjn19780152. [DOI] [PubMed] [Google Scholar]
- 15.Jackson AS, Pollock ML, Ward A. Generalized equations for predicting body density of women. Med Sci Sports Exerc. 1980;12:175–81. [PubMed] [Google Scholar]
- 16.Brozek J, Grande F, Anderson JT, Keys A. Densitometric analysis of body composition: revision of some quantitative assumptions. Ann N Y Acad Sci. 1963;110:113–40. doi: 10.1111/j.1749-6632.1963.tb17079.x. [DOI] [PubMed] [Google Scholar]
- 17.Kaminsky LA Medicine ACoS. ACSM's health-related physical fitness assessment manual. Wolters Kluwer Health/Lippincott Williams & Wilkins health; 2009. [Google Scholar]
- 18.Heyward VH, Wagner DR. Applied body composition assessment. Human Kinetics; 2004. [Google Scholar]
- 19.Kuczmarski RJ. Need for body composition information in elderly subjects. Am J Clin Nutr. 1989;50:1150–7. doi: 10.1093/ajcn/50.5.1150. discussion 231-5. [DOI] [PubMed] [Google Scholar]
- 20.Jensen RK, Fletcher P. Distribution of mass to the segments of elderly males and females. United States: 1994. [DOI] [PubMed] [Google Scholar]
- 21.Visser M, van den Heuvel E, Deurenberg P. Prediction equations for the estimation of body composition in the elderly using anthropometric data. England: 1994. [DOI] [PubMed] [Google Scholar]
- 22.Durnin JV, Womersley J. Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. Br J Nutr. 1974;32:77–97. doi: 10.1079/bjn19740060. [DOI] [PubMed] [Google Scholar]
- 23.Gause-Nilsson I, Dey DK. Percent body fat estimation from skin fold thickness in the elderly. Development of a population-based prediction equation and comparison with published equations in 75-year-olds. J Nutr Health Aging. 2005;9:19–24. [PubMed] [Google Scholar]
- 24.Kwok T, Woo J, Lau E. Prediction of body fat by anthropometry in older Chinese people. Obes Res. 2001;9:97–101. doi: 10.1038/oby.2001.12. [DOI] [PubMed] [Google Scholar]
- 25.Ravaglia G, Forti P, Maioli F, Boschi F, Cicognani A, Gasbarrini G. Measurement of body fat in healthy elderly men: a comparison of methods. J Gerontol A Biol Sci Med Sci. 1999;54:M70–6. doi: 10.1093/gerona/54.2.m70. [DOI] [PubMed] [Google Scholar]
- 26.Reilly JJ, Murray LA, Wilson J, Durnin JV. Measuring the body composition of elderly subjects: a comparison of methods. England: 1994. [DOI] [PubMed] [Google Scholar]
- 27.Aghdassi E, Tam C, Liu B, McArthur M, McGeer A, Simor A, Allard JP. Body fat of older adult subjects calculated from bioelectric impedance versus anthropometry correlated but did not agree. United States: 2001. [DOI] [PubMed] [Google Scholar]
- 28.Teran JC, Sparks KE, Quinn LM, Fernandez BS, Krey SH, Steffee WP. Percent body fat in obese white females predicted by anthropometric measurements. Am J Clin Nutr. 1991;53:7–13. doi: 10.1093/ajcn/53.1.7. [DOI] [PubMed] [Google Scholar]
- 29.Gray DS, Bray GA, Bauer M, Kaplan K, Gemayel N, Wood R, Greenway F, Kirk S. Skinfold thickness measurements in obese subjects. Am J Clin Nutr. 1990;51:571–7. doi: 10.1093/ajcn/51.4.571. [DOI] [PubMed] [Google Scholar]
- 30.Clasey JL, Kanaley JA, Wideman L, Heymsfield SB, Teates CD, Gutgesell ME, Thorner MO, Hartman ML, Weltman A. Validity of methods of body composition assessment in young and older men and women. J Appl Physiol. 1999;86:1728–38. doi: 10.1152/jappl.1999.86.5.1728. [DOI] [PubMed] [Google Scholar]
- 31.Guerra RS, Amaral TF, Marques E, Mota J, Restivo MT. Accuracy of Siri and Brozek equations in the percent body fat estimation in older adults. J Nutr Health Aging. 2010;14:744–8. doi: 10.1007/s12603-010-0112-z. [DOI] [PubMed] [Google Scholar]
- 32.Siri WE. Body composition from fluid spaces and density: analysis of methods. 1961. Nutrition. 1993;9:480–91. discussion, 92. [PubMed] [Google Scholar]
- 33.Kerrigan DC, Lee LW, Collins JJ, Riley PO, Lipsitz LA. Reduced hip extension during walking: healthy elderly and fallers versus young adults. United States: 2001. [DOI] [PubMed] [Google Scholar]