

Abstract
Adapted tango dancing improves mobility and balance in older adults and additional populations with balance impairments. It is composed of very simple step elements. Adapted tango involves movement initiation and cessation, multi-directional perturbations, varied speeds and rhythms. Focus on foot placement, whole body coordination, and attention to partner, path of movement, and aesthetics likely underlie adapted tango’s demonstrated efficacy for improving mobility and balance. In this paper, we describe the methodology to disseminate the adapted tango teaching methods to dance instructor trainees and to implement the adapted tango by the trainees in the community for older adults and individuals with Parkinson’s Disease (PD). Efficacy in improving mobility (measured with the Timed Up and Go, Tandem stance, Berg Balance Scale, Gait Speed and 30 sec chair stand), safety and fidelity of the program is maximized through targeted instructor and volunteer training and a structured detailed syllabus outlining class practices and progression.
Keywords: Behavior, Issue 94, Dance, tango, balance, pedagogy, dissemination, exercise, older adults, Parkinson's Disease, mobility impairments, falls
Introduction
Older adults and individuals with Parkinson’s Disease (PD) suffer decreased quality of life (QOL), 1-3 poor mobility, and high risk of falls 4 secondary to their motor and cognitive impairments. Physical activities that challenge mobility have beneficial effects on balance and can increase self-efficacy in performing activities of daily living (ADLs). 5 Specifically, exercise programs that 1) incorporate dynamic balance practice and 2) involve motor adaptation according to task and environmental demands can rehabilitate balance impairment.6
Dance has recently garnered attention as a potentially effective exercise therapy to address balance impairments. Frequent participation in partnered dance is associated with superior balance, gait, and reaction time in older dancers compared to age-matched non-dancers.7 In institutional settings, adapted Argentine tango (adapted tango) has improved mobility, balance and QOL in those with PD,8-12 stroke,13 and older individuals with visual impairment.14 Adapted tango is designed to address motor impairments including those specific to individuals with PD, i.e., bradykinesia, shortened stride length, backward instability, turning issues, and freezing of gait.
Composed of simple step elements, adapted tango involves movement initiation and cessation, multi-directional perturbations, varied speeds and rhythms. Participants focus on foot placement, whole body coordination, and attention to partner, path of movement, and aesthetics. Within the context of adapted tango, partner dancing is a sophisticated, yet accessible system of tactile communication that conveys motor intentions and goals between a ‘leader’ (planner of movement) and ‘follower’ (externally cued mover).
To ensure engaging, effective exercise programs like adapted tango are accessible by community-dwelling older adults, individuals with PD, and others with motor impairments, adapted tango must be disseminated beyond the academic research setting and into the community. Few evidence-based exercise programs are being systematically disseminated through delivery systems.15 This has resulted in insufficient numbers of adequately trained fitness personnel to provide community-based exercise activities suited to the unique needs of individuals with motor impairments. 16 This paper outlines methodology for dissemination of adapted tango, including standardization of an evidence-based curriculum and comprehensive training of dance teachers without clinical qualifications.
The adapted tango program described here incorporates key, novel elements based upon curricula developed through an empirical approach in several studies. 9,11-13,17 Uniquely, the program described here implemented an uninvestigated dose of 20, 1.5h biweekly sessions, which meets recommendations that older adults exceed 150 min of weekly exercise, 18 and provides additional learning time for individuals with PD to overcome motor learning challenges. 19 The program also expanded the rhythmic training component to harness the known movement facilitation effects of auditory cueing for PD. 20-22
The teacher training workshop focuses on the mechanics of teaching adapted tango, and includes didactic and experiential instruction regarding teaching populations with sensory and motor impairments (e.g., older adults and individuals with PD). A manual composed for this workshop provides a description of the five sections of the Adapted Tango class, a complete syllabus that describes the plan for each lesson (including rhythms, steps of the day, and embellishments) as well as information about people with movement disorders and motor impairments, fall risk and prevention. Classroom management, partnering and rhythmic training are also described in detail.
Any attempt to disseminate academically developed methodology into a community-based setting should include measures to ensure that program quality, safety and participant satisfaction are not sacrificed. Herein the methodology for assessing feasibility, efficacy and generalizability of a disseminated program are described. These measure include 1) evaluation of teacher trainees for teaching the adapted tango syllabus, as per instructions provided in the manual and 15 hr workshop, 2) measurement of adverse events and falls in and out of the class, 3) investigation of participant attrition and satisfaction 4) comparison of the feasibility, adherence and efficacy measures between older adults and individuals with PD, and 5) changes in mobility compared to results from previous studies.8,9,12
A successful dissemination should allow teacher trainees to deliver classes with very low incidence of adverse events (i.e., less than or equal to 1 event during a 12 week course of instruction or 48 classes). Additionally mobility improvements, as demonstrated by decreased fall risk, improved functional mobility, and increased lower body strength should be similar to those from prior studies.8 Finally, a well delivered program should have low attrition, (>80% compliance), and be acceptable for individuals with PD as well as older and oldest-old individuals (85+ years) residing in senior independent living communities.
Protocol
NOTE: The Institutional Review Board at Emory University School of Medicine approved this work. Participants provided written informed consent before participating.
1. Recruitment of Teacher Trainees
Recruit 5-10 teacher trainees from the available population of therapists, professional dance and fitness instructors in the referent area.
- Teacher Trainee Qualifications
- Ensure that teachers have 2 years professional dance teaching experience, clear understanding of movement principles as well as how to convey them, and effective classroom management.
- Verify teachers' past experience working with older and impaired populations.
- Ensure teachers have a reputation for compassionate demeanor, attentiveness, understanding, reliability, maturity, willingness to teach impaired populations and patience.
2. Training of Teacher Trainees in Adapted Tango Methods
Provide all teacher trainees with the Adapted Tango Manual (unpublished, created for the workshop). Instruct trainees to read the manual prior to the training workshop and to refer frequently to the manual to plan classes and troubleshoot.
- Implement the Adapted Tango Teacher training program (developed by MEH) as a 15 hr workshop (12 hr group instruction in workshop format with 3 hr of individual instruction with the trainer), with a strictly followed agenda, guided by the Adapted Tango Manual which delineates all aspects of adapted tango.
- Use the manual to provide information about people with movement disorders and motor impairments, falls risk and prevention and to serve as a guideline for didactic instruction during the adapted tango teacher training workshop.
- At the workshop, describe the sections and theory of the Adapted Tango class.
- In group and pairs, breakdown and practice the adapted tango syllabus, published elsewhere, 13 for the adapted tango program, which includes a series of 24 unique lesson plans that describe the rhythms, steps of the day, and embellishments.
- Explain classroom management tips and techniques
- Explain and practice partnering enhancement tips and techniques.
- Explain basic music theory and practice rhythmic entrainment/music comprehension guide, as detailed in the manual.
- Explain methods for maintaining safety in the class, with exercises designed to promote effective balance management, including falls detection through evaluating limits of stability and falls prevention techniques.
Instruct trainees to follow the syllabus closely to ensure program fidelity.
After the 12 hr workshop, spend 3 hr individually with each teacher in additional training, to answer questions, and to ensure that each teacher fully comprehends adapted tango methods and importance of strict adherence to safety protocol and the detailed syllabus.
Request weekly reports from teachers about progress in classes.
3. Select Sites to Host Classes.
NOTE: Senior living communities (SLCs) often have facilities appropriate for classes. Administrators are interested in providing enrichment activities for their SLC residents, and are often happy to host classes that may include some non-residents in exchange for the provision of high quality exercise classes to residents free of charge.
Approach senior living community administrators to inquire about hosting classes at their facilities. Gain support from the administrators with letters of support. Offer the classes free of charge to all residents within a particular community.
Establish clear rules of procedure, i.e., advertisement, classroom setup and breakdown, visitor expectations, etc.
Communicate frequently with SLC administrators, staff, instructors, and class coordinators for feedback and to maintain a positive relationship.
4. Participant Recruitment
- Recruit older adults and individuals with PD through flyers, referral, PD newsletters, support groups, senior living communities, and websites.
- Ensure that Individuals with PD have received a diagnosis of idiopathic 'definite PD' (Hoehn and Yahr (H&Y) stages I-III)23 and demonstrate benefit from anti-parkinsonian medication.
- Ensure that both individuals with PD and older adults have no history of other neurological insult, and are able to walk 3+ meters with or without assistance.
5. Participant Pre-test Evaluation
NOTE: Conduct pre-tests within 1 week before starting classes.
Schedule each participant for an initial testing session (pre-test) at a participant preferred time of day to minimize medication related performance fluctuations and to ensure all individuals with PD are tested while 'ON' medications.
Obtain written informed consent from each participant prior to their participation.
- Request participants to complete a questionnaire regarding their age, education, medical history, fall history, use of assistive devices such as canes/walkers, and current medications within a week prior or during their initial testing session. Review the form with all participants to ensure completeness/accuracy.
- Classify participants as 'fallers' if they report an unintentional loss of balance that resulted in landing on a lower surface or the ground one or more times in the previous year.
- Provide questionnaires to participants to complete within a week prior or during their initial testing session, detailed below.
- The Fear of Falling (FoF) and Quality of Life (QoL) Measures, which are single items included in a general health questionnaire.
- The Composite Physical Function Index (CPF).
- The Beck Depression Inventory-II (BDI-II). 24
- Administer measures of cognition, PD severity (if applicable), mobility, and fall risk according to standard procedures, detailed below. Train two or more research assistants who are not teacher-trainees to help administer assessments. Videotape all assessments for blinded ratings by qualified research assistants, i.e., doctorate of physical therapy and medical students.
- The The Unified Parkinson's Disease Rating Scale motor subscale III (UPDRS-III). 25
- The Montreal Cognitive Assessment (MoCA). 26
- The Berg Balance Scale (BBS). 27
- The Timed Up and Go. 28
- Gait Speed assessment by timing gait speed with a stopwatch over a 20 foot straight path. Begin the stopwatch when the first heel passes the start line, and stop the stopwatch when the second heel passes the finish line.
- The 30-Second Chair Stand: Count the number of times one can rise from a chair, with arms crossed over the chest, without lifting the feet from the ground, in 30 sec.
- The Tandem Stance by timing the length of time the participant can stand with one foot directly in front of the other in a straight line. The cutoff time will be 60 sec.
- At the conclusion of the testing session, provide participants with a calendar that details their adapted tango dance class schedule.
- Instruct participants not to change habitual exercise routines during the course of the six-month study. Instruct participants to record on the calendar any major medical or adverse events, including any 'falls', i.e., a slip or trip, in which they unexpectedly lost their balance and landed on the ground or a lower level.
- On the date that such an event happens instruct participants to jot a brief note on their calendar detaining circumstances and outcome of the event (e.g.: 'Tripped on cat resulting in fall to knees, no medical attention sought.' or 'Attended regularly scheduled neurology appointment; Sinemet dosing increased from 4 to 5 tablets per day.')
- Instruct participants that their calendars will be reviewed twice: once at the conclusion of the dance classes and again 10-12 weeks after that. In the interim remind participants to continue to attend all regularly scheduled medical appointment and seek medical attention as needed for adverse events that occur outside class time.
6. Volunteer Recruitment
NOTE: This section describes methods for volunteer recruitment. Given the high fall risk of participants, able-bodied volunteers are crucial to the success of the adapted tango program.
Recruit student volunteers from local undergraduate and graduate pre-health list-serves and local community volunteer organizations to serve as dance partners and assistants.
Require all student volunteers fulfill CITI requirements of human research, so as to ensure that they understand human research principles.
Invite able-bodied family members (spouses, children, grandchildren) to participate in the classes as volunteer dance partners. Explain they will not always be partnered with their loved one but will be expected to rotate through dance partners several times per class.
7. Safety Training Procedure
NOTE: Given participants' mobility limitations falls are an ever-present threat before, during, and after each class. Vigilant safety procedures must be enacted to minimize risk of harm. This section describes methods for ensuring safe classes.
Meet with volunteers in small groups of 5-10 individuals for 1.5 hr. Educate them about aging-related posture and gait problems. Instruct them on falls detection/prevention and adapted tango methods. More details are provided elsewhere.10
- Review the charts of all participants.
- Identify participants with higher risk for falls to the research assistants, student volunteers and teachers, who are responsible for their safety.
- Follow this approach to partnering:
- Partner new volunteers first with higher functioning individuals with PD and older adults (e.g. low fall risk as determined by falls history, and standard clinical instruments) and observe the volunteers for attentiveness to their partner, ability to support the partner if necessary, and their ability to grasp and apply adapted tango concepts. Partner lower functioning individuals at higher fall risk with these volunteers after they have demonstrated satisfactory understanding of these concepts. NOTE: Never partner two individuals with PD or two older frail individuals together, because of their mobility limitations. Always partner individuals with PD with able-bodied volunteers or family members/friends.
- Partner together high-functioning older adults without PD who have been determined to have low risk of falls after their initial mobility assessment, only if volunteers, family, friends are unavailable.
Keep weekly contact with the teachers, and the study assistants to address issues of the most vulnerable in the dance classes and ensure appropriate partners are assigned to them.
Allow no more than 10 older adults with motor impairments and/or individuals with PD to attend class with accompanying healthy partners at any given time to maintain a manageable class size.
Instruct teacher trainees and healthy volunteer assistants to monitor all participants' safety vigilantly. Frequently remind assistants to monitor participants for fatigue and postural instability.
Encourage participants to take regular breaks ad libitum. Instruct the teacher to institute frequent timed breaks for participants during each class if participants fatigue easily but are reluctant to initiate their own break.
8. Adapted Tango Classes
Assign participants, after the pre-test evaluation, to 1.5 hr of progressive adapted Argentine tango 2 days a week for 12 weeks at a local community center or SLC. The classes are taught by teacher trainees trained in adapted tango methodology as described in the Adapted Tango manual.
Offer the classes in adapted tango 4 times per week to give participants 48 opportunities to attend a class. Require participants to attend at least 20 lessons to receive a previously demonstrated therapeutic dose.
- Explain the general class structure, which consists of the following guidelines for the classes led by the teacher-trainee:
- Lead a warm-up consisting of breathing, limbering and postural alignment performed individually and to upbeat music.
- Introduce a novel step element and practice one of the following 'partnering enhancement exercises.'
- Instruct both partners to close their eyes, while in the closed practice position, and practice shifting weight from one foot to the other, alternating who 'leads' and who 'follows.'
- Instruct the partners to stand side by side, and practice walking around the room, first on the same foot, (i.e., both step on the right foot), then on opposite feet (either both on the 'outside' leg, or both on the 'inside' leg).
- Instruct partners to place their palms together (but not gripping hands) and to choose a leader. Instruct the leader to move his/her hands randomly in front of him/her and instruct the 'follower' to mirror the motions of the leader by maintaining continual hand contact.
- Instruct the 'follower' to close their eyes while the partnership is holding elbows. NOTE: The 'leader' should practice shifting the weight of their follower through first shifting their own weight, and then through guiding the follower to shift weight through a movement of the chest and arms.
- Instruct the leader to walk towards the follower, as the follower walks backward. Ensure that the leader walks to the outside of the partner (OP), and then back in front of the partner, but without looking at the feet, looking only at the shoulders of their partner.
- Introduce several different rhythms and instruct participants to practice with a partner. Amalgamate the novel step of the day to previously learned steps and practice with a partner.
- Follow general principles guiding partnering and group flow:
- Instruct participants to perform all steps in either an adaptation of the ballroom frame, i.e., holding each other's bent elbows and maintaining forearms parallel to the floor or the 'best-friends position,' i.e., walking side by-side with inside arm around partner's shoulder.
- Designate leader and follower roles within each partnered pair. Instruct leaders to choose direction, timing and size of each successive step, and communicate this information to their partner through moving their frame and center of mass. Instruct followers to attend to sensory cues for movement direction, timing and amplitude of steps, communicated from their partner to them via the frame and center of mass. Instruct Followers to wait to receive the movement cue before moving.
- Instruct participants and volunteers to dance both the leader and follower roles every class, i.e., switching roles every other song with their partners. Enhance learning by rotating partners every 15 min, a widely practiced method in ballroom and social dancing class.
Visit the classes frequently to ensure safe practice, adherence to the syllabus, and availability to assist the teacher trainees as needed.
Instruct teachers and volunteers to remind participants every two weeks to use theircalendars to record any adverse events (falls, medical problems) during the study (6 months total).
Ensure a trained research assistant is present at every class to help monitor training fidelity, record participant attendance, and record the number and details of incidents within class (falls, other accidents, near-misses).
- If a fall or other adverse event occurs, utilize the following protocol to ensure participant safety and allow for subsequent retrospective analysis.
- Ensure that a trained research assistant or class teacher assesses the individual or individuals involved in the event and determine if medical attention is needed. Interview the individual who fell to determines possible mechanisms of injury (e.g.: trip, crumple, which body part hit first, was there a head strike?). NOTE: Any headstrike, loss of consciousness, confusion, or focal injury warrants immediate medical attention.
- If the participant (s) are alert and oriented, and not complaining of any focal pain, assist them to a chair and mandate a 10 min rest period. After this time, assess participant preference for continuing in class versus continued rest. Ensure that participants dictate their own level of readiness to return to dancing and if they opt to do so ensure that they pair with the teacher or a trusted volunteer who has demonstrated competency at fall prevention.
- After the class, ensure that the teacher and trained research assistant debrief and accurately record all of the details of the adverse event. Send the fall details to PI for root cause analysis. Based upon the analysis, implement changes to prevent future adverse events (eg: room restructuring, different partnering, modifications of certain tango step, mandated rest breaks for certain participants).
9. Participant Post-test Evaluations
NOTE: Conduct this evaluation within one week after the 20th class the participant attended.
Schedule a testing session with each participant within one week of finishing the required class dose.
Re-The questionnaires and measures detailed in step 5.5. Ensure that the same trained research assistant helps to The assessments.
Question participants about medical/exercise changes during the preceding 10-12 weeks, and review participants' calendars with them. Record the number of falls or other adverse events they experienced during the course of the study.
Request participants complete an Exit Questionnaire including 1) items about class enjoyment, desire to continue, and improvements in physical and mental well-being rated on a 5-point Likert scale (1 = strongly agree to 5 = strongly disagree) and 2) open ended questions regarding what participants liked best/least about the program and recommendations for program improvements.
10. Participant Follow-up Evaluations
NOTE: Conduct this evaluation within 10-12 weeks after the 20th class the participant attended.
Schedule a testing session with each participant.
Re-The questionnaires and measures detailed in step 5.5. Ensure that the same trained research assistant helps to The assessments.
Question participants about medical/exercise changes during the preceding 10-12 weeks and review participants' calendars. Record the number of falls or other adverse events they experienced from the conclusion of the classes to the follow-up evaluation.
11. Statistical Analysis
Calculate descriptive statistics for all baseline variables.
Use Chi square tests to determine differences between groups on dichotomized data (e.g., attendance and fall occurrence).
Calculate Cohen's d effect sizes, i.e., a standardized measure of the strength of a phenomenon, for changes from pre to post and pre to follow up on the measures of efficacy. NOTE: As this protocol is primarily concerned with dissemination and implementation of the methodology of this program, hypothesis testing is inappropriate for making inferences about efficacy in this context.
Representative Results
The methods detailed above describe rigorous evaluation of adapted tango dissemination in an effort to ensure quality programming becomes available to community dwelling individuals with balance impairments. When this adapted tango program was implemented in community based settings around the Atlanta, GA metro area over the summer of 2012, it was found to be feasible, efficacious and generalizable, although effect sizes were generally small. Nine dance instructors without clinical qualifications participated in 15 hr of training, consisting of: a 12 hr workshop on adapted tango methods, PD-specific motor impairments, and fall prevention, followed by an additional 3 hr of individual training from the senior author. Teacher-trainees had 2-25 years of experience teaching dance and >1 year working with older adults in a fitness/dance setting. Based upon their demonstrated proficiency with safety concepts and adapted tango methods, seven teacher-trainees were selected to teach Tango in five different senior living communities located in the greater Atlanta metro area. The PI (MEH) attended each of the classes at least three times. Each of the teachers delivered the expected syllabus on the expected day, in the correct order. Two non-injurious falls—involving two self-reported frequent fallers—occurred out of 48 offered tango classes for individuals with PD and 2 non-injurious falls occurred out of 144 offered tango classes for older adults. In these instances participants resumed dancing after a short break. Altogether, the teacher trainees taught 192 classes in adapted tango according to the methods described in the Adapted Tango Manual.
Several student volunteers, who dedicated 600+ volunteer hours to efforts related to Tango, were relatively easily recruited through undergraduate and graduate pre-health list serves. All volunteers underwent fall-prevention training and were assessed for safe practices before being allowed to partner with the highest fall risk participants. In attendance, each class for those with PD averaged M = 5.5, SD = 2 volunteers and M = 3.9, SD = 2 caregivers, friends, and relatives. Data regarding precise number of volunteers per older adult class is unavailable but fewer volunteers and fewer caregivers, friends, relatives attended the older adult classes.
Some data for those with PD have been previously published.29 Eighty-eight participants (age range: 36-95 years) were recruited for participation in the adapted tango classes (PD: n = 25; older adults: n = 63). Table 1 shows the baseline characteristics of the participants initially assigned to adapted tango. Sixty-seven participants (PD: n = 23, older adults: n = 44) completed 20 lessons in 10-12 weeks. Overall adherence was 76.1% but there was a significant difference between PD participants with 92% adherence (previously reported)29 and older adults with 70% adherence (p = 0.028). PD and older adult participants who did not complete the program cited illness, family commitments, other time commitments, and lack of interest as reasons for their withdrawal.
Efficacy Measures. Mobility and balance gains were similar to those observed in prior studies of adapted tango conducted in controlled academic settings.14 However, effect sizes were generally small. The changes noted are detailed here. Both groups were able to complete more rises during the 30 second chair stand and received higher scores on the BBS at post testing with gains maintained at follow-up. Gait speed and tandem stance for individuals with PD did not increase substantially at post-testing but demonstrated some increase at follow-up testing. Older adults demonstrated faster gait speed, faster TUG performance, and longer time in tandem stance from pre-to-post with gains maintained at follow-up. Figure 1 demonstrates efficacy outcomes in terms of mean change and effect sizes for each group. Cohen's d effects sizes of 0.41 and above are considered 'practically significant'.30
Falls. Amongst the Older adult cohort, 122 falls were reported in 21,900 person days in the year prior at a rate of 0.0056 falls per person-day. Twelve falls were reported in 3,612 person days in the 12 week intervention period at a rate of .0033 falls per person-day and 7 falls were reported in 3,444 person days in the 12 weeks post-intervention at a rate of 0.0020 falls per person-day. Amongst the PD cohort, because of an outlier who fell 3-4 times per day, 1,289 falls were reported in 8,760 person days in the year prior at a rate of 0.1471 falls per person-day. One hundred twelve falls were reported in 1,932 person days in the 12 week intervention period at a rate of .0580 falls per person-day and 140 falls were reported in 1,764 person days in the 12 weeks post-intervention at a rate of 0.0794 falls per person-day.
At baseline, a greater proportion of the PD sample fell in the year before the study than older adults (i.e., 60% versus 38%). Falls outside of class during the 3 month class period and in the 3 months after the class were rare, although a greater proportion of those with PD experienced a fall compared to the older adult cohort. Figure 2 compares percentages of the groups who did or did not report falls in the year prior, during the intervention, and in the ten-twelve weeks after the intervention.
Satisfaction. The program was well received as per the Exit Questionnaire, and both PD and older adult participants strongly agreed they enjoyed the class and would continue classes if given the opportunity. They agreed they noted improved coordination, walking, strength, endurance, and balance and were more physically and mentally active. The only marginally significant difference between those with PD and the older adults was that older adults more strongly agreed they noted balance improvements (p = 0.075). Numerical ranking responses regarding enjoyment of the program from an exit questionnaire administered to all participants at the conclusion of the program are detailed in Table 2. Table 3 provides a summary of open-ended responses to questions soliciting feedback about the program. Participants in both groups in particular praised the quality of the instruction, the energy of the instructors, the format of the class, the attention received, and feedback given. Many participants appreciated the opportunity to meet new people and among those with PD, the opportunity to forge new friendships with other individuals with PD. A few participants wished there had been more dance while others found the class duration too long. The most frequent recommendation for future classes was to spend more time dancing.
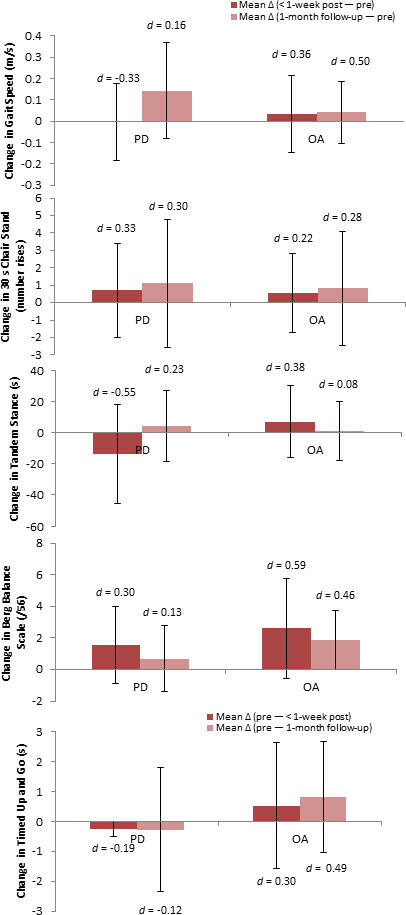 Figure 1:Change in Mobility & Balance Efficacy Measures. PD: Parkinson's disease; OA: Older Adults. The values presented are mean change scores +/- the standard deviation of change. Change score values are calculated as 'post minus pre' and 'follow-up minus pre' for gait speed, 30-s Chair Stand, Tandem Stance and the Berg Balance Scale. Change score values are calculated as 'pre minus post' and 'pre minus follow-up' for the Timed Up & Go. Positive change indicates improvement on the outcome. Cohen's d estimates of effect size are placed above each group's change score. Cohen's d effects sizes of .41 and above are considered 'practically significant'. 30
Please click here to view a larger version of this figure.
Figure 1:Change in Mobility & Balance Efficacy Measures. PD: Parkinson's disease; OA: Older Adults. The values presented are mean change scores +/- the standard deviation of change. Change score values are calculated as 'post minus pre' and 'follow-up minus pre' for gait speed, 30-s Chair Stand, Tandem Stance and the Berg Balance Scale. Change score values are calculated as 'pre minus post' and 'pre minus follow-up' for the Timed Up & Go. Positive change indicates improvement on the outcome. Cohen's d estimates of effect size are placed above each group's change score. Cohen's d effects sizes of .41 and above are considered 'practically significant'. 30
Please click here to view a larger version of this figure.
 Figure 2: Fall Incidence Outside of Class Before, During, and After the Intervention. The percentage of the sample considered Fallers (with a history of at least one fall in the prior year) and Non-Fallers (no history of falls in the prior year) within the PD group (red bars), and the Older Adults group (pink bars) are depicted, along with the percentages of the sample who did or did not report a fall outside of class during the ten-twelve week interventional period and in the ten-twelve weeks following cessation of the intervention. The p values are the levels of significance between groups determined with Chi square tests. Although those with PD were on average younger than the older adult cohort, they were more likely to experience falls during the study. Please click here to view a larger version of this figure.
Figure 2: Fall Incidence Outside of Class Before, During, and After the Intervention. The percentage of the sample considered Fallers (with a history of at least one fall in the prior year) and Non-Fallers (no history of falls in the prior year) within the PD group (red bars), and the Older Adults group (pink bars) are depicted, along with the percentages of the sample who did or did not report a fall outside of class during the ten-twelve week interventional period and in the ten-twelve weeks following cessation of the intervention. The p values are the levels of significance between groups determined with Chi square tests. Although those with PD were on average younger than the older adult cohort, they were more likely to experience falls during the study. Please click here to view a larger version of this figure.
| Individuals with PD | Older Adults | ||
| n=25 | n=63 | ||
| M (SD) | M (SD) | ||
| Sex | 12 F; 13 M | 49F; 14M | |
| Age (years) | 68.4 (7.5) | 82.3 (8.8) | |
| Education (years) | 16.5 (2.1) | 14.2 (3.1) | |
| Number Co-morbidities | 3.3 (1.7) | 3.2 (1.9) | |
| Number Prescription Medications | 5.4 (4.5) | 3.3 (2.0) | |
| Use of Assistive Device (%) | 29% | 69% | |
| Fear of Falling (FoF) | 3.0 (1.5) | 2.9 (1.7) | |
| Quality of Life (QoL) | 5.2 (0.9) | 5.4 (1.2) | |
| Composite Physical Function (CPF) (/24) | 20.3 (4.9) | 17.8 (4.7) | |
| Montreal Cognitive Assessment (MoCA) (/30) | 26.0 (2.8) | 22.5 (4.0) | |
| Beck Depression Inventory-II (BDI-II) (/63) | 12.1 (9.6) | 6.6 (4.7) | |
| UPDRS Motor Subscale III (n=24) | 28.1 (6.9) | ~ | |
| Gait Speed (m/s) | 0.97(.24) | 0.88(.23) | |
| 30 s Chair Stand (Number of Rises) | 11.5(4) | 7.9(5) | |
| Berg Balance Scale (/56 points) | 51.2(4.5) | 46.1(8.7) | |
| Tandem Stance (s) | 26.1(26) | 8.3(16) | |
| Timed Up and Go (s) | 11.9(8) | 12.9(5) |
Table 1: Adapted Tango Baseline Participant Demographics & Outcome Measure Baselines. Participant-reported co-morbidities included arthritis, diabetes, high blood pressure, heart problems and osteoporosis, among others. FoF & QoL are based upon participant ratings regarding worry about falling / quality of life from 1 (low) to 7 (high). For the Composite Physical Function Index, the Montreal Cognitive Assessment, and the Berg Balance Scale higher values indicate greater physical function, cognitive ability, and balance respectively. For BDI-II, higher values indicate greater depression.
| Total Sample (n=67) | PD (n=23) | Older Adult (n=44) | p value | |
| Enjoyment | 1[1,1] | 1[1,1] | 1[1,1] | 0.725 |
| Balance | 2[1,3] | 2[2,3] | 2[1,3] | 0.075 |
| Walking | 2[1,3] | 2[2,3] | 2[1,3] | 0.427 |
| Mood | 2[1,3] | 2[1.25,2] | 2[1,3] | 0.713 |
| Coordination | 2[1,3] | 2[2,3] | 2[1,3] | 0.766 |
| Strength | 2[1,3] | 2.5[2,3] | 2[1,3] | 0.328 |
| Endurance | 2[1,3] | 2[2,3] | 2[1,3] | 0.783 |
| Continuing | 1[1,2] | 1.5[1,2] | 1[1,2] | 0.988 |
| Physically More Active | 2[1,3] | 2[1.25,3] | 2[1,3] | 0.876 |
| Mentally More Active | 2[1,3] | 2[1,3] | 2[1,3] | 0.659 |
Table 2: Participant Satisfaction. Participants indicated level of agreement (1 = strongly agree to 5 = strongly disagree) with statements regarding the class and improvements in their physical and mental well-being. Values are represented as Median [1st, 3rd quartile]. There were no differences between those with PD and older adults in self-reported satisfaction.
| PD | Older Adults | |
| What did you like best? | ||
| Instructors and helpers—11 | Instructors and helpers—18 | |
| Being able to socialize—11 | Exercise—16 | |
| Opportunity to dance—3 | Opportunity to dance—14 | |
| Structured/Scheduled activity—1 | Being able to socialize—12 | |
| Feeling of accomplishment—1 | Bodily improvements (balance, walking, energy etc.)—6 | |
| Bodily improvements (balance, walking, energy etc.)—1 | Being 'challenged to think & act'—1 | |
| Flexibility with attendance—1 | All of it—1 | |
| Handouts with brief descriptions—1 | ||
| What did you like least? | ||
| More dancing, less exercise requested—4 | Duration too long—11 | |
| Nothing—3 | Nothing—8 | |
| Travel & Distance—3 | Other—5 | |
| Attendance and Record Keeping Pressure—2 | Program duration (20 lessons) too short—4 | |
| Transportation to class dependant on others—1 | Hearing/Audio—2 | |
| Music system did not work well—1 | ||
| Warm up too long—1 | ||
| Too overprotected at times—1 | ||
| Number of chairs in the room made me fearful of running into them—1 | ||
| Not enough emphasis on keeping up with the music—1 | ||
| Female partners (felt safer with male partners)—1 | ||
| Duration of individual classes (1.5 h) too long—1 | ||
| Recommendations | ||
| Nothing—5 | Nothing—11 | |
| More Dancing—5 | Have more volunteer partners available—10 | |
| Shorter classes or more breaks—2 | Other—6 | |
| Include other Latin dances such as the cha cha—1 | Shorter classes—5 | |
| Provide tango music to listen to at home—1 | Visual Stimuli and Materials—4 | |
| Fewer chairs in room—1 | Program Duration (10-12 weeks) too short—3 | |
| Make-up class options—1 | Positioning and Point of View of Instructor—3 | |
| Better volunteer awareness of PD limitations—1 | More Movement—2 | |
| Have a focus group to share experiences—1 | ||
| Allow more opportunities to take notes—1 | ||
| Use name tags for the first few classes—1 | ||
| Recruit more male volunteers to partner—1 |
Table 3: Participant Feedback. Participants completed an open-ended Exit Questionnaire regarding what they liked best and least about the class and suggestions for improvement. Their responses are summarized here.
Discussion
Engaging in habitual exercise remains overwhelmingly poor in the general older adult population: only 1 in 8 older adults engage in strength or balance-challenging activities. 31 Recently, exercise has gained approval as a complementary approach to accompany conventional medicine. To further ‘aging in place’ and maintain independence in a growing older population, the widespread implementation of evidence-based exercise programs is necessary. Additionally, given that pharmacological and surgical approaches incompletely address motor and cognitive challenges of the growing PD population, access to complementary therapies, like adapted tango, is necessary. Since 2006, this adapted tango program has been iterated, refined and tested several times, but only at academic centers, not in a community-based setting. 10,13 The methods described above provide a guide to dissemination of adapted tango to the community in such a way that the fidelity, efficacy, safety, and enjoyment of the program are preserved.
Translating health behavior research into sustainable applications is frequently overlooked 32 and underfunded. 33 This methodological guide may allow wider dissemination of adapted tango thus providing access to needed therapy for numerous community dwelling older adults and individuals with balance impairments. Key to dissemination of adapted tango are the selection of appropriate teacher trainees, proper safety training, ample volunteer/family member recruitment, and rigorous assessment of participants before and after completion of the program.
Without a qualified pool of teacher trainees, the adapted tango program will not function. Trainees must possess not only dance knowledge and skill but also a willingness to work outside the traditional realm of able-bodied dance. Teacher trainee enthusiasm, patience, and attention to detail (especially safety) cannot be overstated. One of the main barriers to a multitude of engaging exercise activities for older adults and those with balance impairments is the inability to guarantee safety. Indeed, safety cannot be guaranteed within the adapted tango curricula but if the measures described above regarding volunteer recruitment, participant file review, and partnering are followed, adverse events would be kept to a minimum.
Rigorous assessment of participants before and after the tango program with validated standard measures is necessary to demonstrate that community-based tango is as efficacious as that conducted in academic centers. One of the main limitations of the study as we have implemented it here is the small sample size. Although we were able to show dissemination did not compromise effect size, this should be replicated in future larger studies. The replicated demonstration of efficacy may lead to increased awareness of the benefits of complementary therapy and foster further accessibility to those in need.
The adapted tango dance manual (unpublished), adapted tango class syllabus, this text, and accompanying video are designed to allow individuals in diverse communities to implement this program. Yet, successful utilization of these print and video resources assumes some baseline knowledge of dance, older adults, movement disorders, and fall risk. The above protocol also assumes prior knowledge or familiarity with pre-and-post assessment tests. While all of these tests are cited in validated research papers available to the wider community, implementation of each research measure from a written description alone would be daunting. However, many of these tests are commonly utilized within the physical therapy community. Therefore, it may be advantageous to partner with a physical therapist when attempting to implement this program. Physical therapy involvement could help with implementing pre and post testing, fine-tuning fall prevention strategies and further dissemination/implementation of the program itself, with added expertise to ensure safety.
As stated earlier, implementation of a dancing exercise program for individuals with balance impairments is a big risk and represents a potentially unsafe situation if proper measures are not taken. Future dissemination of this program will necessitate strict safety standards to ensure community leaders and community facilities are willing to host such a program. Integral to safety is also the recruitment of volunteers and family members to partner during the class. While urban areas generally contain an abundance of pre-medical and other health profession students, rural areas lacking major academic centers may find volunteer recruitment more difficult. In this scenario we suggest reaching out to local schools/churches/clubs to enlist able-bodied youth in community service projects to partner for these dance classes.
Lack of mechanistic understanding may prevent more rapid evolution of dance/exercise as a complementary medicine. However, several mechanisms may explain the generally positive changes in physical function produced by adapted tango. The creativity involved in a dance form through exposure to novel steps, and choreographic patterns could tap into mechanisms of neural plasticity. A recent study of adapted tango noted improvement in PD disease severity 29 leading to speculation about potential neuroprotective or neurorestorative effects of adapted tango. The positive functional gains of older adults undergoing regular aerobic activity may be explained by plasticity-related changes in synaptogenesis, angiogenesis and neurogenesis. 34 Future research should delineate ideal frequency, duration and intensity of dance sessions to obtain and retain gains in function.
Individuals with PD were considerably more likely to comply with therapy and finish the program than were older adults, which is curious given that individuals with PD are less active than age-matched peers without PD. 35 Further, the PD group came from the community and needed to travel to the classes; whilst the older adults received the therapy at their senior living communities. As PD remains a condition with many intractable symptoms, those with PD may be more likely to comply with therapy suggestions, including novel, and appealing non-pharmacological treatments. Older adults lost to attrition may have felt less urgency to adopt a new exercise habit. Traditional exercise programs for older adults suffer more than 30% attrition, 36 which is comparable to the rate observed here for the older adult cohort.
The etiology of high satisfaction with the program is likely multifactorial. Music, which has been found to activate specific neural pathways associated with emotion, might reduce stress and enhance social relationships. 37In a randomized controlled trial of Tango over 2 weeks (meeting 1.5 hr and 4 times per week) with middle-aged adults with self-referred symptoms of anxiety, and depression, significant improvements in their symptoms were noted at post-test, and maintained at a 1 month follow-up and similar improvements were noted in the same population after 8 weeks of tango dance. 38 Because social dance often involves meeting regularly to work in pairs or groups for honing skill and/or to enjoy the activity, dance may encourage teamwork that can allow the cultivation of friendships and larger community involvement. Further, therapies involving the arts and self-expression, both emotional and physical, may be especially helpful for managing motor and cognitive symptoms resulting from aging-related morbidities. Therapies that 1) allow the patient to regain and exert control on their body and 2) involve extensive social interaction have been shown to be effective at improving quality of life. 39 Future research should evaluate the role of a regained locus of control and consider depression and cognitive impairment as they relate to interventional success.
Limitations with dissemination media (ie: text and video), safety concerns, and potential difficulty in recruiting teachers and volunteers may limit further dissemination of adapted tango. As this study was primarily methodological in focus, hypothesis testing to determine the significance of results was not performed, but will be necessary to perform in future work. The effect sizes in this work for the mobility measures were relatively small, which does call into question the true efficacy of this form of therapy. Evaluating measures of cognition, psychosocial function and quality of life, not performed here, are needed.
That the program was safely implemented by novice teachers in the community and for individuals with varied impairments and a large age range (36-95 years) suggests the generalizability of the program, and flexibility for addressing multiple needs. Rehabilitation to restore and/or improve function in people with PD and older adults must be efficient and effective. Creating sustained behavioral change through targeted and effective programs may be most effective at addressing functional independence issues for older adults with and without movement disorders. 40 Although effect sizes are often compromised during dissemination, 32 this study suggests that adapted tango could be disseminated in the community under the instruction of non-clinically trained individuals, with only minimally attenuated effect sizes. More research is needed to refine dissemination methods while maintaining program fidelity.
Disclosures
Financial Disclosure/Conflict of Interest: There are no conflicts of interest to report.
Funding Sources: Dan and Merrie Boone Foundation, Emory Center for Injury Control, Emory Center for Health in Aging, Department of VA R&D Service Career Development Awards to ME Hackney (E7108M and N0870W), National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR000454. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Acknowledgments
We would like to thank the teachers, Ronda and Manuel Patino, and Gabriela Lopez of Tango Rio, Erik Renz, Sarah Kelley Kerr, Mark Needelman and Shelley Brooks. We also acknowledge volunteers Adrienne Wimberly, Allison Bascas, Marco Coelho, Dabin Choi, Carly DiLeo, Margaret Fang, Kevin Huang, Twinkle Mehta, Malije Obi, Mina Taheb, Diana Tiwari, Kedra Woodard, Dawa Tsering, Sabine Povian, Dhondup Tso King, Mylinh Vo, Rebecca Dillard and Marisa Warner. We acknowledge Medlock Gardens retirement community for providing space for the adapted tango workshop, Clairmont Oaks retirement community and Wesley Woods Towers for providing space for the interventions and we thank the administrative staff of each institution. We acknowledge Dr. William De L’Aune for statistical assistance. The study was supported by the Dan and Merrie Boone Foundation, the Emory Center for Injury Control, and the Emory Center for Health in Aging. This study was also supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number UL1TR000454. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The Emory School of Medicine Discovery Program supported KE McKee, and Department of VA R&D Service Career Development Awards (E7108M and N0870W) supported ME Hackney. We would also like to thank Mr. Aaron Bozzorg.
References
- Muslimovic D, Post B, Speelman JD, Schmand B, de Haan RJ. Determinants of disability and quality of life in mild to moderate Parkinson disease. Neurology. 2008;70(23):2241–2247. doi: 10.1212/01.wnl.0000313835.33830.80. [DOI] [PubMed] [Google Scholar]
- Possin KL, Filoteo JV, Song DD, Salmon DP. Spatial and object working memory deficits in Parkinson's disease are due to impairment in different underlying processes. Neuropsychology. 2008;22(5):585–595. doi: 10.1037/a0012613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hausdorff JM, et al. A common cognitive profile in elderly fallers and in patients with Parkinson's disease: the prominence of impaired executive function and attention. Exp. Aging Res. 2006;32(4):411–429. doi: 10.1080/03610730600875817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Camicioli R, Majumdar SR. Relationship between mild cognitive impairment and falls in older people with and without Parkinson's disease: 1-Year Prospective Cohort Study. Gait Posture. 2010;32(1):87–91. doi: 10.1016/j.gaitpost.2010.03.013. [DOI] [PubMed] [Google Scholar]
- Gitlin LN, et al. Tailored activities to manage neuropsychiatric behaviors in persons with dementia and reduce caregiver burden: a randomized pilot study. Am J Geriatr Psychiatry. 2008;16(3):229–239. doi: 10.1097/JGP.0b013e318160da72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hirsch MA, Toole T, Maitland CG, Rider RA. The effects of balance training and high-intensity resistance training on persons with idiopathic Parkinson's disease. Arch Phys Med Rehabil. 2003;84(8):1109–1117. doi: 10.1016/s0003-9993(03)00046-7. [DOI] [PubMed] [Google Scholar]
- Verghese J. Cognitive and mobility profile of older social dancers. J Am Geriatr Soc. 2006;54(8):1241–1244. doi: 10.1111/j.1532-5415.2006.00808.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hackney ME, Earhart GM. Effects of dance on movement control in Parkinson's disease: a comparison of Argentine tango and American ballroom. J Rehabil Med. 2009;41(6):475–481. doi: 10.2340/16501977-0362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hackney ME, Earhart GM. Effects of dance on gait and balance in Parkinson's disease: a comparison of partnered and nonpartnered dance movement. Neurorehabil Neural Repair. 2010;24(4):384–392. doi: 10.1177/1545968309353329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hackney ME, Earhart GM. Recommendations for implementing partnered dance classes for persons with Parkinson Disease. Am J Dance Ther. 2010;32(1):41–45. doi: 10.1007/s10465-010-9086-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hackney ME, Kantorovich S, Earhart GM. A study on the effects of Argentine tango as a form of partnered dance for those with Parkinson disease and the healthy elderly. Am J Dance Ther. 2007;29(2):109–127. [Google Scholar]
- Hackney ME, Kantorovich S, Levin R, Earhart GM. Effects of tango on functional mobility in Parkinson's disease: a preliminary study. J Neurol Phys Ther. 2007;31(4):173–179. doi: 10.1097/NPT.0b013e31815ce78b. [DOI] [PubMed] [Google Scholar]
- Hackney ME, Hall CD, Echt KV, Wolf SL. Application of adapted tango as therapeutic intervention for patients with chronic stroke. J Geriatr Phys Ther. 2012;35(4):206–217. doi: 10.1519/JPT.0b013e31823ae6ea. [DOI] [PubMed] [Google Scholar]
- Hackney ME, Hall CD, Echt KV, Wolf SL. Dancing for balance: feasibility and efficacy in oldest-old adults with visual impairment. Nurs Res. 2013;62(2):138–143. doi: 10.1097/NNR.0b013e318283f68e. [DOI] [PubMed] [Google Scholar]
- Orleans CT, Gruman J, Ulmer C, Emont SL, Hollendonner JK. Rating our progress in population health promotion: report card on six behaviors. Am. J. Health Promot. 1999;14(2):75–82. doi: 10.4278/0890-1171-14.2.75. [DOI] [PubMed] [Google Scholar]
- Aas RW, Grotle M. Clients using community occupational therapy services: sociodemographic factors and the occurrence of diseases and disabilities. Scand. J. Occup. Ther. 2007;14(3):150–159. doi: 10.1080/11038120600968811. [DOI] [PubMed] [Google Scholar]
- Hackney ME, Earhart GM. Short duration, intensive tango dancing for Parkinson disease: an uncontrolled pilot study. Complement Ther Med. 2009;17(4):203–207. doi: 10.1016/j.ctim.2008.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chodzko-Zajko WJ, et al. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009;41(7):1510–1530. doi: 10.1249/MSS.0b013e3181a0c95c. [DOI] [PubMed] [Google Scholar]
- Stephan MA, Meier B, Zaugg SW, Kaelin-Lang A. Motor sequence learning performance in Parkinson's disease patients depends on the stage of disease. Brain Cogn. 2011;75(2):135–140. doi: 10.1016/j.bandc.2010.10.015. [DOI] [PubMed] [Google Scholar]
- Dibble LE, et al. Sensory cueing effects on maximal speed gait initiation in persons with Parkinson's disease and healthy elders. Gait Posture. 2004;19(3):215–225. doi: 10.1016/S0966-6362(03)00065-1. [DOI] [PubMed] [Google Scholar]
- Howe TE, Lovgreen B, Cody FW, Ashton VJ, Oldham JA. Auditory cues can modify the gait of persons with early-stage Parkinson's disease: a method for enhancing parkinsonian walking performance. Clin. Rehabil. 2003;17(4):363–367. doi: 10.1191/0269215503cr621oa. [DOI] [PubMed] [Google Scholar]
- Rochester L, et al. The effect of external rhythmic cues (auditory and visual) on walking during a functional task in homes of people with Parkinson's disease. Arch Phys Med Rehabil. 1016;86(5):999–1006. doi: 10.1016/j.apmr.2004.10.040. [DOI] [PubMed] [Google Scholar]
- Racette BA, Rundle M, Parsian A, Perlmutter JS. Evaluation of a screening questionnaire for genetic studies of Parkinson's disease. Am J Med Genet. 1999;88(5):539–543. [PubMed] [Google Scholar]
- Beck AT, Steer RA, Ball R, Ranieri W. Comparison of Beck Depression Inventories -IA and -II in psychiatric outpatients. J Pers Assess. 1996;67(3):588–597. doi: 10.1207/s15327752jpa6703_13. [DOI] [PubMed] [Google Scholar]
- Goetz CG, et al. Movement Disorder Society-sponsored revision of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. 2008;23(15):2129–2170. doi: 10.1002/mds.22340. [DOI] [PubMed] [Google Scholar]
- Nasreddine ZS, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi: 10.1111/j.1532-5415.2005.53221.x. [DOI] [PubMed] [Google Scholar]
- Berg K, Wood-Dauphinee S, Williams JI. The Balance Scale: reliability assessment with elderly residents and patients with an acute stroke. Scand J Rehabil Med. 1995;27(1):27–36. [PubMed] [Google Scholar]
- Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed U. Go Test. Phys Ther. 2000;80(9):896–903. [PubMed] [Google Scholar]
- McKee KE, Hackney ME. The effects of adapted tango on spatial cognition and disease severity in Parkinson's disease. J Mot Behav. 2013;45(6):519–529. doi: 10.1080/00222895.2013.834288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferguson CJ. An Effect Size Primer: A Guide for Clinicians and Researchers. Prof Psychol-Res Pr. 1037;40(5):532–538. [Google Scholar]
- Merom D, et al. Prevalence and correlates of participation in fall prevention exercise/physical activity by older adults. Prev Med. 2012;55(6):613–617. doi: 10.1016/j.ypmed.2012.10.001. [DOI] [PubMed] [Google Scholar]
- Kottke TE, Pronk NP. Physical activity optimizing practice through research. Am. J. Prev. Med. 2006;31(4):8–10. doi: 10.1016/j.amepre.2006.06.011. [DOI] [PubMed] [Google Scholar]
- Woolf SH. The meaning of translational research and why it matters. JAMA. 2008;299(2):211–213. doi: 10.1001/jama.2007.26. [DOI] [PubMed] [Google Scholar]
- Hirsch MA, Farley BG. Exercise and neuroplasticity in persons living with Parkinson's disease. Eur J Phys Rehabil Med. 2009;45(2):215–229. [PubMed] [Google Scholar]
- Toth MJ, Fishman PS, Poehlman ET. Free-living daily energy expenditure in patients with Parkinson's disease. Neurology. 1997;48(1):88–91. doi: 10.1212/wnl.48.1.88. [DOI] [PubMed] [Google Scholar]
- Jancey J, et al. Reducing attrition in physical activity programs for older adults. J Aging Phys Act. 2007;15(2):152–165. doi: 10.1123/japa.15.2.152. [DOI] [PubMed] [Google Scholar]
- Boso M, Politi P, Barale F, Enzo E. Neurophysiology and neurobiology of the musical experience. Functional neurology. 2006;21(4):187–191. [PubMed] [Google Scholar]
- Pinniger R, Thorsteinsson EB, Brown RF, Mckinley P. Intensive tango dance program for people with self-referred affective symptoms. Music and Medicine. 2013;5(1):15–22. [Google Scholar]
- Modugno N, et al. Active theater as a complementary therapy for Parkinson's disease rehabilitation: a pilot study. TheScientificWorldJournal. 2010;10:2301–2313. doi: 10.1100/tsw.2010.221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Speelman AD, et al. How might physical activity benefit patients with Parkinson disease. Nat Rev Neurol. 2011;7(9):528–534. doi: 10.1038/nrneurol.2011.107. [DOI] [PubMed] [Google Scholar]