

Abstract
Exstrophy of the urinary bladder is a rare congential anomaly. The most common malignancy is an adenocarcinoma in these patients. Squamous cell carcinoma (SCC) occurring in these patients is uncommon and usually has a bad prognosis. The management of these patients is challenging and may require extensive reconstructive procedures. We report a case of SCC in a corrected bladder exstrophy patient who presented with an ulcerated mass in the lower abdomen extending to the base of the penis. Six months after extensive radical ablative surgery with reconstruction of the abdominal wall, the patient remained free of recurrence.
Keywords: Bladder exstrophy, bladder tumor, squamous cell carcinoma
INTRODUCTION
Exstrophy of the urinary bladder is a rare congential anomaly with an incidence of 1 in 10,000 to 1 in 50,000 live births.[1] One of the long-term complications of exstrophy bladder is development of adenocarcinoma due to mucosal metaplasia to intestinal epithelial elements. The occurrence of squamous cell cancer is very rare in these patients. The management of these patients is challenging as this may require extensive reconstructive procedures. We report such a case in an adult male.
CASE REPORT
A 42-year-old, unmarried male reported with a mass in the lower abdomen of 6 months and ulceration over the mass of 2 months duration. He had undergone repair of exstrophy of the bladder at the age of 20 years elsewhere, the details of which were not available. He was totally incontinent even after the surgery. Examination revealed a large ulcerating mass in the lower abdomen extending to the base of the penis [Figure 1]. Routine laboratory investigations were normal. Contrast-enhanced computed tomography showed the whole of the reconstructed bladder filled with a solid enhancing mass, with involvement of the upper tract [Figure 2]. Biopsy of the fungating mass showed well-differentiated squamous cell carcinoma (SCC). Hence, radical cystectomy along with penectomy and lymphadenectomy were performed. The bowel was not healthy and bilateral ureterostomies were fashioned. The presence of symphyseal diastasis made the surgery quite easy. With the help of plastic surgeons, the defect in the abdominal wall was closed using a pedicled, anterolateral thigh flap [Figure 3]. The post-operative period was uneventful. The final histopathological report showed well-differentiated SCC and lymph nodes showed reactive hyperplasia. At 6 months of follow-up, the patient was asymptomatic and healthy.
Figure 1.
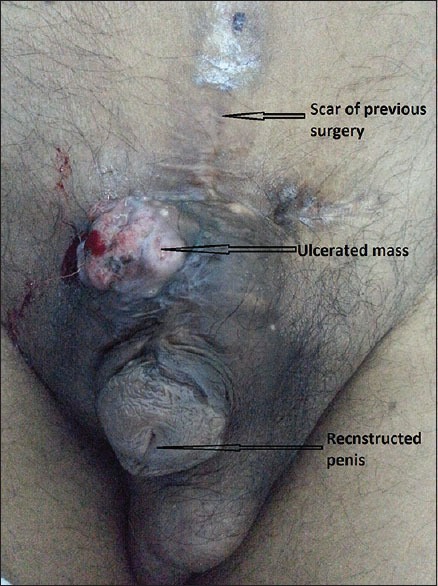
The ulcerated mass in the lower abdomen
Figure 2.

Contrast-enhanced computed tomography showing the reconstructed bladder filled with uniformly homogenous mass
Figure 3.

Post-operative appearance of the patient
DISCUSSION
The incidence of SCC of the urinary bladder varies from 3% to 40%, the higher incidence being in the Middle East countries where schistosomiasis is prevalent. SCC accounts for 3–5% of malignancies in exstrophy bladder. About 60% of the malignancies in ectopia vesica occur in the 5th and 6th decades of life.[2]
Despite bladder closure or diversion surgery within the first year of life, patients with exstrophy have an almost 700-fold greater incidence of bladder cancer than the age-matched normal population. Early reconstruction is not protective. In a cohort of 740 patients of exstrophy epispadias syndrome, with meticulous follow-up, not a single case of malignancy was detected even after 25 years by Gearhart et al.[3] Because these exstrophy bladder patients are at risk of developing malignancy, meticulous follow-up detects cancer at earlier stages and reduces the occurrence of advanced malignancy and hence the morbid surgeries. This emphasizes the need for proper patient education and meticulous and rigorous follow-up. Flexible cystoscopy with urine cytology annually after the age of 25 years is the recommended follow-up protocol for these patients.[3]
The prognosis of SCC of the bladder is poor with advanced stage at detection. Kassouf et al. reported a median recurrence-free survival of 5.1 months.[4] Twenty-seven patients diagnosed with non-bilharzial pure SCC of the bladder with clinical stages of T2 (13 patients), T3b (nine patients) and T4b (five patients) at the MD Anderson Cancer Center were reviewed. In 10 of 20 patients who underwent radical cystectomy, the disease recurred after a median duration of 5.1 months and seven died: Three of local recurrence, one of distant recurrence and three of both.
Our patient did not have any predisposing factors like bladder stone, chronic infection and self-intermittent catheterization that usually led to the development of SCC. In spite of extensive growth, the tumor remained well differentiated and there was no lymph node metastasis. In most of the reported cases also, the tumor was well differentiated; however the status of the lymph nodes has not been mentioned.[2]
Zaghloul et al. in their series of bladder adenocarcinoma in 192 patients reported radical cystoprostatectomy and pelvic lymphadenectomy with or without post-operative radiotherapy as the treatment modality of choice, and no difference was noted in the treatment of adenocarcinoma in exstrophy patients compared with primary adenocarcinoma.[5] Till date, no data are available to assess the differential prognosis of SCC and adenocarcinoma with regard to the exstrophy patients as most are case reports.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Gearhart JP, Mathews RI. Exstrophy-Epispadias Complex. In: Kavoussi LR, Partin AW, Novick AC, Peters CA, editors. Campbell Walsh Urology. 10th ed. Philadelphia, PA: WB Saunders; 2012. pp. 3325–79. [Google Scholar]
- 2.Haji AG, Chitra TK, Sharma S, Vijaya Kumar DK, Gangadharan VP. Squamous cell carcinoma in bladder exstrophy. Indian J Med Pediatr Oncol. 2008;29:28–30. [Google Scholar]
- 3.Gearhart JP. Neoplasms in adult exstrophy patients. BJU Int. 2001;88:647–8. doi: 10.1046/j.1464-4096.2001.2429.x-i7. [DOI] [PubMed] [Google Scholar]
- 4.Kassouf W, Spiecs PE, Seifker-Radke A, Swanson D, Grossman HB, Kamat AM, et al. Outcome and pattern of recurrence of non Bilharzial pure SCC of bladder: A contemporary review of the series of Texas MD Anderson memorial cancer centere experience. Cancer. 2007;110:764–9. doi: 10.1002/cncr.22853. [DOI] [PubMed] [Google Scholar]
- 5.Zaghloul MS, Nouh A, Nazmy M, Ramzy S, Zaghloul AS, Sedira MA, et al. Long-term results of primary adenocarcinoma of the urinary bladder: A report on 192 patients. Urol Oncol. 2006;24:13–20. doi: 10.1016/j.urolonc.2005.05.027. [DOI] [PubMed] [Google Scholar]