

Abstract
Background
The Intramedullary Skeletal Kinetic Distractor (ISKD) (Orthofix Inc, Lewisville, TX, USA) is an intramedullary device designed for more comfortable limb lengthening than that with external fixators; lengthening is achieved with this nail using rotational oscillation between two telescoping sections. However, the degree to which this device achieves this goal and its complication rate have not been fully documented.
Questions/purposes
We determined (1) the frequency with which distraction was not achieved at the desired rate, (2) whether pain differed between patients with normally and abnormally distracting nails, (3) risk factors for abnormal nails, and (4) other complications.
Methods
We analyzed 35 lengthening segments (26 femurs, nine tibias) in 19 patients. Mean length achieved was 47 mm. Femoral nails were categorized into four groups according to distraction rate: normal, runaway (unintentionally faster rate [> 1.5 mm/day]), difficult-to-distract (slower rate [< 0.8 mm/day] requiring manual manipulation but not requiring general anesthesia), and nondistracting (slower rate [< 0.8 mm/day] requiring manual manipulation under general anesthesia or reosteotomy). Possible risk factors, including age, BMI, preoperative thigh circumferences, degree of intramedullary overreaming, and length of the thicker portion of the nail within the distal fragment, were compared among groups. VAS pain scores were compared among groups under three conditions: rest, physiotherapy, and distraction motion. Complications were also analyzed. Minimum followup was 15 months (mean, 26 months; range, 15–38 months) after first-stage surgery.
Results
Abnormal distraction rate was observed in 21 of 35 segments (60%; 17 femurs, four tibias). VAS pain scores showed no differences among groups during rest or physiotherapy but were higher (p = 0.02) in the problematic nails (7–8 points) versus normal nails (3 points) during distraction. Only mean length of the thicker portion of the nail within the distal fragment differed between normally and abnormally distracting nails (95 mm versus 100 mm; p = 0.03), although this was unlikely to be clinically important. Complications occurred in 10 patients (53%), including five with decreased ankle ROM during distraction, four with delayed bone healing, and one with mechanical device failure during distraction.
Conclusions
Rate control was difficult to achieve with the ISKD nail for femoral and tibial lengthenings, complications were relatively common, and among patients in whom rate control was not achieved, pain levels were high. Based on our findings, we believe that surgeons should avoid use of this nail.
Level of Evidence
Level IV, therapeutic study. See Instructions for Authors for a complete description of levels of evidence.
Introduction
Limb lengthening using an external fixator is associated with many problems, such as pin tract infection, pin-associated pain, scarring, and discomforts from the bulky frame [14, 17]. Because of this, several intramedullary lengthening devices have been developed [1–3, 5–8, 11, 19]. The Intramedullary Skeletal Kinetic Distractor (ISKD) is an intramedullary device that provides limb lengthening without any external device [5]. It lengthens by small rotational oscillations (3°–9°) between two telescoping sections of the nail. Since this device distracts gradually by a patient’s manual oscillation of his/her limb during daily movement and without any help from external fixators, it is believed to provide a comfortable limb lengthening. Some complications have been reported with the ISKD, such as difficulty in controlling distraction rate [10, 13, 15, 18], device failure [4, 15], and delayed union [10, 18]. However, no studies have documented pain according to distraction rate. And, importantly, to our knowledge, no studies have determined whether the ISKD indeed provides low pain levels during lengthening.
We therefore determined (1) the frequency with which distraction was not achieved at the desired rate with this nail (ie, normal versus runaway, difficult-to-distract, and nondistracting nails), (2) whether pain differed between patients with nails that distracted at the normal rate and those that did not, (3) risk factors for nails that did not distract at the normal rate, and (4) other complications with the use of these nails.
Patients and Methods
Patients
This study has a retrospective comparative design and was approved by the institutional review board at our institution. From March 2010 to March 2012, we analyzed 19 patients (35 lower limbs: 26 femurs, nine tibias) that underwent limb lengthening using the ISKD. No patients were lost to followup. During this period, we generally used this nail under the following general indications. In the femur, this nail was recommended because femoral lengthening with an external device usually causes severe pain during ROM because the pin penetrates the fascia lata and thus may decrease knee ROM and leave ugly scars. In the tibia, this nail was used only when patients demanded the internal lengthener despite our recommendation to use external devices. During this period, we also used lengthening over nail or lengthening and then nail, and the ISKD nail was used in 10% of our patients. We favored other approaches, especially in tibial lengthening because tibial lengthening with the ISKD has several weaknesses, including limited weightbearing during distraction and thus difficulty in preventing equinus contracture. All patient data were collected on a precomposed form prospectively. All patients underwent stature lengthening for familial short stature (16 patients; 24 femurs, eight tibias) or leg length discrepancy (three patients; two femurs, one tibia) with the ISKD. The mean preoperative height was 154 cm (range, 143–167 cm). The leg length discrepancy in the three patients was caused by motorcycle accident (one femur) and congenital hypoplasia (one femur, one tibia). All patients were skeletally mature with no history of medical illness, soft tissue compromise, or infections. There was no significant preoperative deformity. The mean age of the patients was 28 years (range, 17–73 years). Proximal tibia vara was concomitant in four tibias. All radiographic measurements including leg length were obtained using long standing radiographs. Minimum followup was 15 months (mean, 26 months; range, 15–38 months) after first-stage surgery.
Surgical Procedures
The operative procedure for femoral lengthening with the ISKD started with the patient on a fracture table in the supine position. The first step was to save the image of the lesser trochanter with the patella facing forward and to insert two parallel 5-mm Schanz pins both proximal and distal to the osteotomy site to maintain the preoperative rotational status. Multiple drilling was done in the area between 3 cm distal to the more distal hole of the proximal interlocking screw holes and 3 cm proximal to the junction of the two sliding sections of the intramedullary nail. The osteotomy level was determined at the area between 9.5 cm from the proximal tip in the femoral nail (7.5 cm in the tibial nail) and 11 cm from the distal tip. In all cases, this area included the point where the femur had a maximum curvature; we chose that point to be osteotomized to minimize the friction between the inner cortex of the femur and the intramedullary nail. The entry point for the nail was determined either at the piriformis fossa or at the tip of the greater trochanter depending on the type of ISKD nail used. If the diameter of the femoral medullary canal was too narrow, the 10.7-mm tibial ISKD was applied using a trochanteric entry point. The medullary canal was overreamed by a minimum of 1.5 to 2 mm wider than the nail diameter used, and then careful percutaneous osteotomy was performed to make a complete transverse osteotomy. Subsequently, the nail was inserted completely and the interlocking screws were fixed. The osteotomy site was lengthened by 1.5 to 2.0 mm during surgery through rotatory movement and the lengthening was confirmed by both the monitor of the ISKD and the C-arm. After completion of one leg, surgery on the other leg was performed in the same manner after change of surgical draping.
The operative procedure for tibial lengthening with the ISKD was performed in the supine position on an ordinary operation table. Fibular osteotomy was performed at first at the junction of the middle and distal 1/3. The entry point of the intramedullary nail in the coronal plane was determined along the anatomic axis of the tibia and a little modified if the tibia showed a proximal varus deformity. Proximal and distal fibulas were fixed to the tibia using cortical or cannulated screws to prevent distal and proximal migration, respectively. The subsequent procedure including determination of the level of osteotomy was similar to that of femur lengthening surgery. At the end of surgery, autologous bone marrow aspirate concentrate and autologous platelet-rich plasma were injected at the osteotomy site to enhance bone healing for all cases, including tibias and femurs.
Postoperative Rehabilitation and Evaluation
Postoperatively, all patients were educated about how to lengthen their limbs and modify the amount of their daily activities according to the distracted length. Total nonweightbearing and limited bed activities were asked for about 1 week postoperatively to avoid distraction during the latent period. In all patients, we recommended limiting weightbearing to 20 kg or less through the lengthening period.
All patients were reviewed clinically and radiographically every week until the desired length was achieved and followed monthly until the radiographic consolidation of three cortices was confirmed. Since most patients underwent bilateral limb lengthening, they were allowed to move in a wheelchair only until the radiographic evidence of one cortical consolidation. Full weightbearing was allowed thereafter.
Distraction rates were represented by the distraction index, which was defined as the length of the callus regeneration on a radiograph divided by the number of days for distraction. The target distraction rates were set as 8 to 9 mm/day for the tibia and 1.0 to 1.2 mm/day for the femur. Femoral nails were divided into four groups according to distraction index. A distraction index of 0.8 to 1.5 mm/day without forceful manipulation by medical personnel or reosteotomy was considered normal (Table 1). In contrast to normal nails, problematic nails included runaway nails, difficult-to-distract nails, and nondistracting nails. Runaway nails were defined as segments that showed a faster-than-desired rate (> 1.5 mm/day), resulting not from intentional efforts but rather from daily activities. Difficult-to-distract nails were defined as segments that showed a slower-than-desired rate (< 0.8 mm/day) and required manual manipulation by medical staff but did not require general anesthesia. Nondistracting nails were defined as segments that showed a slower-than-desired rate (< 0.8 mm/day) and required manual manipulation by medical staff under general anesthesia or reosteotomy for further distraction.
Table 1.
Definitions of the four femoral nail groups based on distraction rate
| Nail group | Definition |
|---|---|
| Normal | Segments showing a distraction index of 0.8–1.5 mm/day without forceful manipulation by medical staff or reosteotomy |
| Problematic | |
| Runaway | Segments showing faster rate (> 1.5 mm/day), lengthened not by intentionally faster distraction but by patients’ daily activities |
| Difficult to distract | Segments showing slower rate (< 0.8 mm/day), requiring manual manipulation by medical staff but not requiring general anesthesia |
| Nondistracting | Segments showing slower rate (< 0.8 mm/day), requiring manual manipulation by medical staff under general anesthesia or reosteotomy for further distraction |
The rate was modulated based on the weekly radiographic evaluation. If the rate was too fast, the patients were asked to be nonweightbearing and reduce the level of their daily activities. If the rate was too slow, patients were asked to bear weight up to the limitation, increase their level of daily activities, and perform more rotating maneuvers by themselves.
After grouping of the segments, the distraction and consolidation indexes and the percentages of the problematic nails were summarized and compared between femurs and tibias. The consolidation index was defined as the number of days spent until radiographic evidence of consolidation of the regenerate bone after surgery (one or there cortices), divided by the length of callus regeneration.
We compared various possible factors, including age, BMI, preoperative thigh circumference, degree of intramedullary overreaming, and length of the thicker portion of the nail within the distal fragment (osteotomy level) (Fig. 1). The length of the thicker portion of the nail within the distal fragment has been reported to be associated with runaway nails if less than 80 mm and nondistracting nails if more than 125 mm [16]. Pain was evaluated using a 0- to 10-point VAS under three different circumstances (rest, physiotherapy, and distraction motion) and compared among groups. The pain VAS score was self-recorded by each patient on the preoperatively given pain questionnaire. Each patient was asked to report the average pain VAS score on the distracted segment. We also recorded other complications, including mechanical failure, which was defined either as breakage of the nail or failure of the internal mechanism to activate; marked decrease in ROM during the distraction phase, which was defined as a decreased ROM of the joints above and below the nail of more than 50% of the preoperative state; delayed union; nonunion requiring bone graft; and deep infection.
Fig. 1.
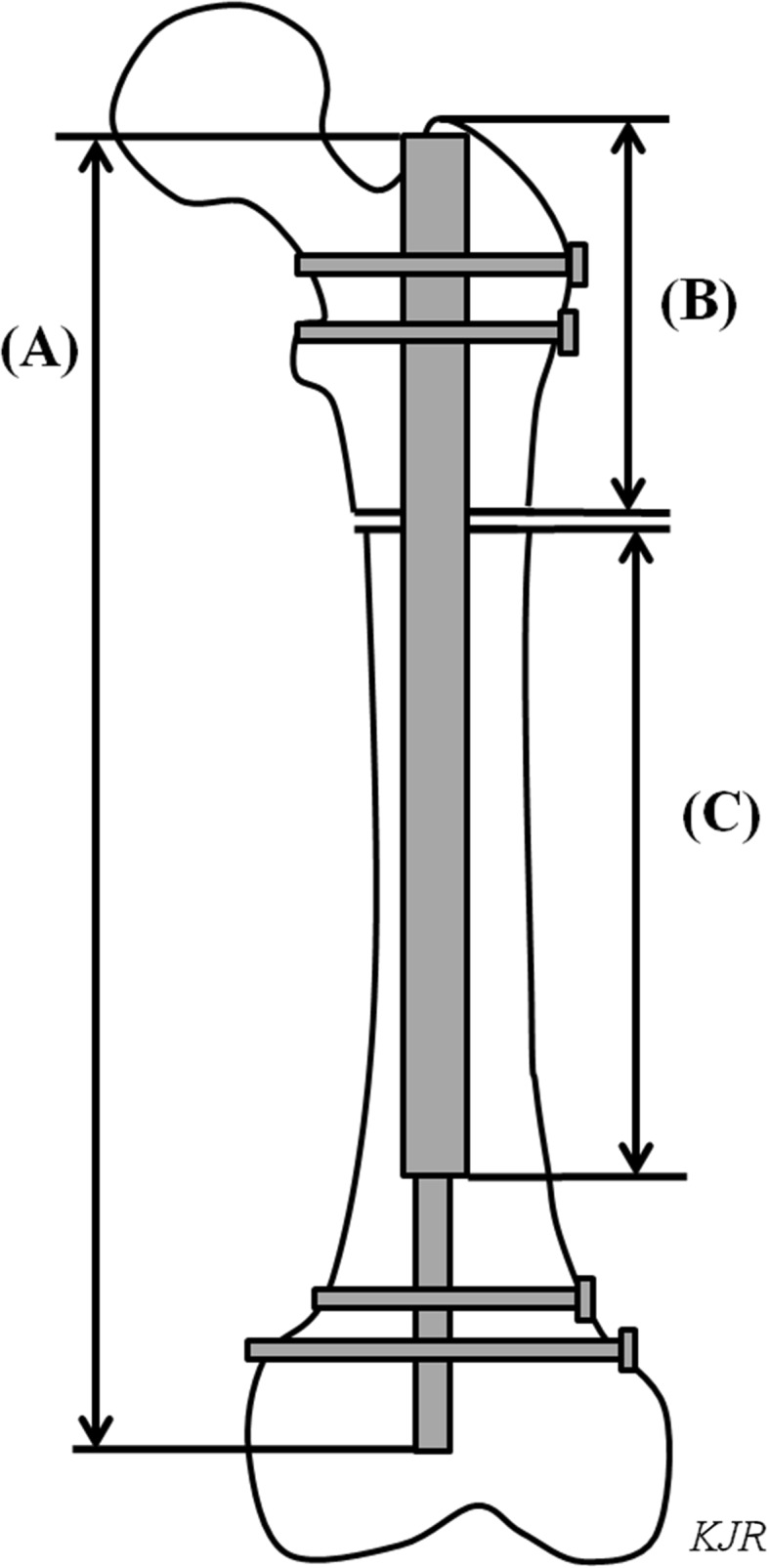
A schematic image of the left femur with the ISKD device inside shows the total length of the nail (A), the length of the proximal fragment (B), and the length of the thicker portion of the nail within the distal fragment (C).
The desired lengthening was achieved in all patients including all problematic nails. Mean lengthening gain was 47 mm (range, 40–60 mm). The mean time spent for distraction was 54 days (range, 15–90 days). The mean distraction indexes were 1.5 ± 0.6 mm/day (range, 0.6–3.8 mm/day) and 0.9 ± 0.2 mm/day (range, 0.4–1.3 mm/day) in femurs and tibias, respectively (Table 2). The mean consolidation index (for three cortices) was lower (p < 0.001) for femurs (17 ± 11 days/cm; range, 8–35 days/cm) than for tibias (36 ± 8 days/cm; range, 32–97 days/cm).
Table 2.
Summary of data pertaining to lower-extremity limb lengthenings with the ISKD
| Variable | Femurs (n = 26) | Tibias (n = 9) | p value |
|---|---|---|---|
| Distraction index (mm/day)* | 1.5 ± 0.6 (0.6–3.8) | 0.9 ± 0.2 (0.4–1.3) | |
| Consolidation index (1 cortex) (days/cm)* | 14 ± 6 (6–35) | 26 ± 14 (15–51) | 0.002 |
| Consolidation index (3 cortices) (days/cm)* | 17 ± 11 (8–35) | 36 ± 8 (32–97) | < 0.001 |
| Nail group (number of nails) | |||
| Normal nails | 9 (35%) | 5 (56%) | 0.48 |
| Problematic nails | 17 (65%) | 4 (44%) | 0.43 |
| Runaway nails | 6 (23%) | 0 (0%) | |
| Difficult-to-distract nails | 8 (31%) | 4 (44%) | |
| Nondistracting nails | 3 (12%) | 0 (0 %) | |
* Values are expressed as mean ± SD, with range in parentheses.
Statistics
All continuous variables were tested for normality using the Shapiro-Wilk test and followed a normal distribution. Each continuous measurement is expressed as mean ± SD with range. Two of us (DHL, KJR) performed the radiographic measurements and showed almost perfect interrater agreement for mechanical failure, marked decrease in ROM during the distraction phase, delayed unions, and nonunions (κ values, 0.91–0.94). The interobserver correlation was good or excellent for distraction and consolidation indexes (correlation coefficient, 0.89 and 0.92, respectively).
We performed a post hoc power analysis for VAS pain score and found that our sample size achieved a statistical power of 0.8 with a significance of 0.05 and an effect size of 1.4 points on the 10-point VAS scale. Student’s t-test was used to determine differences in distraction and consolidation indexes and pain VAS scores between femurs and tibias. The chi-square test was used to determine differences in numbers of problematic nails and complications between femurs and tibias. The four kinds of ISKD nail groups were compared via Kruskal-Wallis test. A p value of less than 0.05 was considered statistically significant. The statistical software R (Version 2.12; The R Project for Statistical Computing, Vienna, Austria) was used for all statistical analyses.
Results
The desired rate of distraction was achieved in 14 segments (40%; nine femurs, five tibias) and not achieved in 21 segments (17 femurs, four tibias). The numbers of problematic nails were not different between femurs and tibias (p = 0.43). This included six runaway nails (six femurs, no tibias), 12 difficult-to-distract nails (eight femurs, four tibias), and three nondistracting nails (three femurs, no tibias) (Table 2).
During the distraction motion, pain was greater in the problematic nail groups, with VAS scores of 7 points in the runaway nails, 7 points in the difficult-to-distract nails, and 8 points in the nondistracting nails compared to 3 points in the normal group (p = 0.02; Table 3). During rest or physiotherapy, there were no differences in VAS pain scores among the groups.
Table 3.
Comparison between normal and problematic nails in femurs
| Variable | Normal nails (n = 9) | Problematic nails (n = 17) | p value | ||
|---|---|---|---|---|---|
| Runaway nails (n = 6) | Difficult-to-distract nails (n = 8) | Nondistracting nails (n = 3) | |||
| Age (years)* | 28 ± 8 | 33 ± 20 | 26 ± 7 | 24 ± 9 | 0.48 |
| BMI (kg/m2)* | 23 ± 5 | 22 ± 3 | 22 ± 5 | 23 ± 8 | 0.87 |
| Thigh circumference (mm)* | 406 ± 25 | 409 ± 32 | 402 ± 21 | 405 ± 21 | 0.81 |
| Overreaming (mm)* | 2.0 ± 0.4 | 2.1 ± 0.3 | 1.9 ± 0.4 | 2.1 ± 0.3 | 0.85 |
| LTDF (mm)* | 95 ± 6 | 93 ± 6 | 100 ± 7 | 100 ± 4 | 0.03 |
| Consolidation index (3 cortices) (days/cm)† | 15 (11–17) | 20 (8–35) | 17 (13–24) | 18 (13–25) | 0.44 |
| VAS score for pain (0–10 points) (points)* | |||||
| Rest | 2 ± 1 | 2 ± 1 | 2 ± 1 | 2 ± 1 | 0.58 |
| Physiotherapy | 3 ± 1 | 3 ± 2 | 2 ± 1 | 2 ± 1 | 0.73 |
| Distraction motion | 3 ± 1 | 7 ± 1 | 7 ± 1 | 8 ± 1 | 0.02 |
* Values are expressed as mean ± SD; †values are expressed as mean, with range in parentheses; LTDF = length of the thicker portion of the nail within the distal fragment.
The only factor we found that was associated with problematic nails was the length of the thicker portion of the nail within the distal fragment, which was lower in the normal and runaway nails (Fig. 2) than in the difficult-to-distract and nondistracting nails. However, this difference, while statistically significant (p = 0.03), was not likely to be clinically important, as the mean difference among these groups was no more than about 5 mm (Table 3). No other factors we examined were different among groups.
Fig. 2A–D.

Images illustrate a case of a runaway nail in femoral lengthening with a distraction index of 3.8 mm/day. (A) AP and (B) lateral radiographic views show a 4-cm distraction reached at 11 days postoperatively without any intervention for rapid distraction. Followup (C) AP and (D) lateral radiographic views show three cortical consolidations at 60 days postoperatively (consolidation index = 15 days/cm).
Complications were common in this series, with 10 of 19 patients (53%) having one or more complications, including one femoral segment and nine tibial segments (Table 4). Mechanical failure was found in one tibial lengthening, which was converted to the lengthening over nail technique with the ISKD nail maintained in situ. Marked decrease in ROM during the distraction phase (ankle equinus contracture) was observed in five tibias (56%). These equinus contractures were relieved with the aid of physical exercises. Three tibias (33%) showed delayed bone healing, with consolidation indexes (three cortices) of greater than 60 days/cm, compared to one femur (4%). No segments were found to have nonunion requiring bone graft or deep intramedullary infections.
Table 4.
Other complications of lower-extremity limb lengthening with the ISKD
| Complication | Number of segments | p value | |
|---|---|---|---|
| Femurs (n = 26) | Tibias (n = 9) | ||
| Mechanical failure | 0 | 1 (11%) | 0.26 |
| Marked decrease in ROM during distraction phase | 0 | 5 (56%) | < 0.001 |
| Delayed union | 1 (4%) | 3 (33%) | 0.05 |
| Nonunion requiring bone graft | 0 | 0 | 0.99 |
| Deep infection | 0 | 0 | 0.99 |
Discussion
Several intramedullary lengthening devices have been developed since the 1970s [1–3, 5–8, 11, 19] to avoid bulky external fixators. However, most of them have not succeeded because of a considerable amount of pain during distraction, weakness or mechanical instability of the nail, inaccurate control of the lengthening, or deep infection [1–3, 5, 7, 19]. We therefore determined (1) the frequency with which distraction was not achieved at the desired rate with this nail (ie, normal versus runaway, difficult-to-distract, and nondistracting nails), (2) whether pain differed between patients with nails that distracted at the normal rate and those that did not, (3) risk factors for nails that did not distract at the normal rate, and (4) other complications with the use of these nails. Rate control was difficult to achieve with the ISKD nail for femoral and tibial lengthenings, complications were relatively common, and among patients in whom rate control was not achieved, pain levels were high.
This study had a number of limitations. First, the pain VAS score was based on patients’ subjective assessment, and there is still a chance that the patients were unable to identify or differentiate exactly from which segment the pain came from. Also, it is difficult to be certain that the pain VAS score at the time the patient answered the survey represented the average pain he or she actually had over the three different followup intervals. Second, the length of the thicker portion of the nail within the distal fragment in this study was between 93 and 100 mm. These were within the range of 80 and 125 mm suggested by others [16], and although we found statistical differences between the nail types, the absolute difference was small (only 7 mm on average), and so this is likely not to be a clinically relevant difference. Third, the autologous bone marrow aspirate concentrate and platelet-rich plasma were injected at the osteotomy site at the end of the index surgery for all cases. We strongly believe that they have some positive effect on callus regeneration (we had no nonunion case even with six cases of runaway nails), but this is still controversial as large randomized trials are lacking. The consolidation indexes in our patients could be different from those in other reports using the ISKD. Fourth, we had only nine patients who underwent tibial lengthening, which limited our ability to subcategorize or analyze them separately; certainly larger studies are called for on this point. Fifth, another internal lengthening device, the PRECICE® nail, is thought to be promising and gaining popularity with better rate control. Comparing the available internal lengthening devices would offer a promising direction for future study.
We found that only a minority of the segments treated with this nail achieved distraction at the desired rate. Problems of rate control have been reported to be the major disadvantage in the ISKD nail [10, 12, 15, 16, 18]. Distraction rate is important for callus regeneration in distraction osteogenesis [10], and uncontrolled rate, either too fast or too slow, can result in nonunion or premature consolidation. Previous reports on the ISKD recommended to educate the patients to minimize their activities and reduce weightbearing to prevent unexpected lengthening [14, 18]. However, from our experience, if runaway distraction occurs, restriction of daily activities and even absolute bed rest cannot control the rate effectively. We observed a higher rate of difficult-to-distract and nondistracting nails (43% in femurs, 44% in tibias) when compared to other studies in the literature [10, 12, 15, 16, 18].
Although a major part of the design rationale of the nail we studied was a reduction in pain, we found that ISKD could provoke a considerable amount of pain, and this was correlated with the loss of rate control. If the nail distracted too fast, as happened with runaway nails, pain increased, which we believe may have been from muscle cramping. If it distracted too slowly, such as in difficult-to-distract or nondistracting nails, the required physician’s intervention provoked considerable pain as well. However, significant pain was not noted during rest and physiotherapy in the four groups. To our knowledge, pain for distraction in the ISKD device has not been described in the literature.
We investigated factors that may be associated with rate control and observed that the length of the thicker portion of the nail within the distal fragment was different among our four groups, with the smallest in runaway nails and the largest in nondistracting nails. The magnitude of our finding is in fact quite small and may be of questionable clinical importance. However, this phenomenon has been described previously in the literature by Simpson et al. [16], who reported that runaway nails occur more often when this length is less than 80 mm (lower osteotomy level), and nondistracting nails occur more often when this length is more than 125 mm (higher osteotomy level). We found a similar tendency with the osteotomy level but lacked enough data to suggest certain critical points. Our findings may support the assumption of Kubiak et al. [12] as to why the femoral ISKD shows an uncontrollable rate. They suggested that the use of a straight nail in a curved femur predisposes to binding of superior and inferior aspects of the anterior cortices at the osteotomy site. The mechanism of the ISKD demands a much smaller amount of rotation to be activated than the Albizzia nail, so it could be easily affected by the minor forces of the surrounding environment. We believe that unpredictable friction force between the bone and the ISKD nail is one of the important factors in loss of rate control. Modifications in the mechanical properties of the nail, surgical instruments, or standardized localization of the osteotomy level seem to be necessary to improve the rate control in the ISKD nail.
We found that complications with this nail were quite common. Others have had similar problems [4, 10, 13] Among the ISKD-related reports, four articles described the results of tibial lengthening [9, 10, 15, 18]. Kenaway et al. [10] reported one case (8%) of poor regenerate among 12 tibias and Wang and Edwards [18] reported three cases (60%) of poor regenerate among five tibias. We experienced three cases (33%) of poor callus regenerate in tibial lengthening. The rate of poor callus regeneration in tibial lengthening with the ISKD seems to be higher than that with external fixators, and we believe that the limited weightbearing to reduce mechanical stresses to the device and the axial rotations to activate the device producing shear force to the regenerate bone might adversely affect bone healing in the tibia. Mechanical failure is another problem of the ISKD. Burghardt et al. [4] reported overall 6.2% of mechanical failures with 242 segments of lower-limb lengthening with the ISKD. They described that the key ring collar that surrounds the junction between the two telescopic sections connected by a threaded rod is the weakest point of the device. We experienced one mechanical failure in tibial lengthening in which the nail failed to further distract during the distraction period.
We found that we achieved successful limb lengthening with this device using physiologic limb motions and low levels of pain in the patients whose nails achieved normal distraction rates. However, in the other patients, who constituted a majority of those in this study, pain levels were high and complications frequent. We therefore recommend the use of other intramedullary nails and that future efforts focus on the design of nails with better rate control.
Acknowledgments
The authors thank Dr. Hyun Woo Kim and Dr. Jin Ho Hwang for their valuable advice and fruitful discussions.
Footnotes
Each author certifies that he or she, or a member of his or her immediate family, has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research ® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA approval status, of any drug or device before clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation that all investigations were conducted in conformity with ethical principles of research, and that the informed consent for participation in the study was obtained.
This work was performed at CHA Bundang Medical Center, Kyungki-do, Republic of Korea.
References
- 1.Baumann E, Harms J. [The extension nail: a new method for lengthening of the femur and the tibia] [in German] Arch Orthop Unfallchirurg. 1997;90:139–146. doi: 10.1007/BF00414987. [DOI] [PubMed] [Google Scholar]
- 2.Baumgart R, Bets Z, Schweiberer L. A fully implantable motorized intramedullary nail for limb lengthening and bone transport. Clin Orthop Relat Res. 1997;343:135–143. [PubMed] [Google Scholar]
- 3.Bliskonov AI. [Lengthening of the femur using implantable appliances][in Czech] Acta Chir Orthop Traumatol Cech. 1984;51:454–466. [PubMed] [Google Scholar]
- 4.Burghardt RD, Herzenberg JE, Specht SC, Paley D. Mechanical failure of the Intramedullary Skeletal Kinetic Distractor in limb lengthening. J Bone Joint Surg Br. 2011;93:639–643. doi: 10.1302/0301-620X.93B5.25986. [DOI] [PubMed] [Google Scholar]
- 5.Cole JD, Justin D, Kasparis T, DeVlught D, Knoblocj C. The Intramedullary Skeletal Kinetic Distractor (ISKD): first clinical results of a new intramedullary nail for lengthening of the femur and tibia. Injury. 2001;32:SD129–SD139. [DOI] [PubMed]
- 6.García-Cimbrelo E, Curto de la Mano A, García-Rey E, Cordero J, Marti-Ciruelos R. The intramedullary elongation nail for femoral lengthening. J Bone Joint Surg Br. 2002;84:971–977. [DOI] [PubMed]
- 7.Guichet JM, Casar RS. Mechanical characterization of a totally intramedullary gradual elongation nail. Clin Orthop Relat Res. 1997;337:281–290. doi: 10.1097/00003086-199704000-00032. [DOI] [PubMed] [Google Scholar]
- 8.Guichet JM, Deromedis B, Donnan LT, Peretti G, Lascombes P, Bado F. Gradual femoral lengthening with the Albizzia intramedullary nail. J Bone Joint Surg Am. 2003;85:838–848. doi: 10.2106/00004623-200305000-00011. [DOI] [PubMed] [Google Scholar]
- 9.Hankemeier S, Pape HC, Gosling T, Hufner T, Richter M, Krettek C. Improved comfort in lower limb lengthening with the intramedullary skeletal kinetic distractor: principles and preliminary clinical experiences. Arch Orthop Trauma Surg. 2004;124:129–133. doi: 10.1007/s00402-003-0625-6. [DOI] [PubMed] [Google Scholar]
- 10.Kenawey M, Krettek C, Liodakis E, Meller R, Hankemeier S. Insufficient bone regenerate after intramedullary femoral lengthening: risk factors and classification system. Clin Orthop Relat Res. 2011;469:264–273. doi: 10.1007/s11999-010-1332-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Krieg AH, Speth BM, Foster BK. Leg lengthening with a motorized nail in adolescents: an alternative to external fixators? Clin Orthop Relat Res. 2008;466:189–197. doi: 10.1007/s11999-007-0040-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kubiak E, Strauss E, Grant A, Feldman D, Egol KA. [Early complications encountered using a self-lengthening intramedullary nail for the correction of limb length inequality][in Turkish] Joint Dis Relat Surg. 2007;18:52–57. [Google Scholar]
- 13.Mahboubian S, Seah M, Fragomen AT, Rozbruch SR. Femoral lengthening with lengthening over a nail has fewer complications than intramedullary skeletal kinetic distraction. Clin Orthop Relat Res. 2012;470:1221–1231. doi: 10.1007/s11999-011-2204-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res. 1990;250:81–104. [PubMed] [Google Scholar]
- 15.Schiedel FM, Pip S, Wacker S, Pöpping J, Tretow H, Leidinger B, Rödl R. Intramedullary limb lengthening with the Intramedullary Skeletal Kinetic Distractor in the lower limb. J Bone Joint Surg Br. 2011;93:788–792. doi: 10.1302/0301-620X.93B6.25581. [DOI] [PubMed] [Google Scholar]
- 16.Simpson AH, Shalaby H, Keenan G. Femoral lengthening with the Intramedullary Skeletal Kinetic Distractor. J Bone Joint Surg Br. 2009;91:955–961. doi: 10.1302/0301-620X.91B7.21466. [DOI] [PubMed] [Google Scholar]
- 17.Tjernstrom B, Olerud S, Rehnberg L. Limb lengthening by callus distraction: complications in 53 cases operated 1980–1991. Acta Orthop Scand. 1994;65:447–455. doi: 10.3109/17453679408995491. [DOI] [PubMed] [Google Scholar]
- 18.Wang K, Edwards E. Intramedullary skeletal kinetic distractor in the treatment of leg length discrepancy—a review of 16 cases and analysis of complications. J Orthop Trauma. 2012;26:e138–e144. doi: 10.1097/BOT.0b013e318238b5b1. [DOI] [PubMed] [Google Scholar]
- 19.Witt AN, Jager M. Results of animal experiments with an implantable femur distractor for operative leg lengthening. Arch Orthop Unfallchir. 1977;88:273–279. doi: 10.1007/BF00416617. [DOI] [PubMed] [Google Scholar]