

Abstract
Background
Femoroacetabular impingement (FAI) may constrain hip articulation and cause chondrolabral damage, but to our knowledge, in vivo articulation and femur-labrum contact patterns have not been quantified.
Purpose
In this exploratory study, we describe the use of high-speed dual-fluoroscopy and model-based tracking to dynamically measure in vivo hip articulation and estimate the location of femur-labrum contact in six asymptomatic hips and three hips with FAI during the impingement examination. We asked: (1) Does femur-labrum contact occur at the terminal position of impingement? (2) Could range of motion (ROM) during the impingement examination appear decreased in hips with FAI? (3) Does the location of femur-labrum contact coincide with that of minimum bone-to-bone distance? (4) In the patients with FAI, does the location of femur-labrum contact qualitatively correspond to the location of damage observed intraoperatively?
Methods
High-speed dual-fluoroscopy images were acquired continuously as the impingement examination was performed. CT arthrogram images of all subjects were segmented to generate three-dimensional (3-D) surfaces for the pelvis, femur, and labrum. Model-based tracking of the fluoroscopy images enabled dynamic kinematic observation of the 3-D surfaces. At the terminal position of the examination, the region of minimal bone-to-bone distance was compared with the estimated location of femur-labrum contact. Each patient with FAI underwent hip arthroscopy; the location of femur-labrum contact was compared qualitatively with damage found during surgery. As an exploratory study, statistics were not performed.
Results
Femur-labrum contact was observed in both groups, but patterns of contact were subject-specific. At the terminal position of the impingement examination, internal rotation and adduction angles for each of the patients with FAI were less than the 95% confidence intervals (CIs) for the asymptomatic control subjects. The location of minimum bone-to-bone distance agreed with the region of femur-labrum contact in two of nine hips. The locations of chondrolabral damage identified during surgery qualitatively coincided with the region of femur-labrum contact.
Conclusions
Dual-fluoroscopy and model-based tracking provided the ability to assess hip kinematics in vivo during the entire impingement examination. The high variability in observed labrum-femur contact patterns at the terminal position of the examination provides evidence that subtle anatomic features could dictate underlying hip biomechanics. Although femur-labrum contact occurs in asymptomatic and symptomatic hips at the terminal position of the impingement examination, contact may occur at reduced adduction and internal rotation in patients with FAI. Use of minimum bone-to-bone distance may not appropriately identify the region of femur-labrum contact. Additional research, using a larger cohort and appropriate statistical tests, is required to confirm the findings of this exploratory study.
Electronic supplementary material
The online version of this article (doi:10.1007/s11999-014-3919-9) contains supplementary material, which is available to authorized users.
Introduction
During the last decade, femoroacetabular impingement (FAI) has been implicated as a possible cause of hip osteoarthritis [6, 13, 20]. Although the exact mechanism responsible for osteoarthritis is unclear, it is believed that abnormal articulation and impingement in hips with FAI causes chondrolabral injury [13, 30]. Differing patterns of chondrolabral damage identified intraoperatively and through diagnostic imaging have led to separate hypothesized mechanisms of impingement for each FAI subtype [4–7, 22]. Specifically, in pincer FAI, contact between the femoral neck and prominent acetabular rim is thought to produce direct compression and subsequent damage to the capsular surface of the labrum [4–7, 22]. In contrast, cam FAI is thought to damage the acetabular chondrolabral junction (usually preserving the outer surface of the labrum) as the aspherical femoral head enters the acetabulum during hip flexion and internal rotation [4–7, 22]. Successful treatment of FAI relies on characterization of the pathoanatomy, including the location and severity of impingement. For this purpose, the impingement process may be visible at the time of surgery [21]. However, accurate, three-dimensional (3-D) quantification of joint articulation (ie, kinematics) with accompanying measurements of the in vivo impingement site in the native hip remain elusive. These data could confirm or refute clinically hypothesized mechanisms of chondrolabral injury in hips with FAI.
The most common approach to measure hip kinematics, skin marker motion analysis, has identified gross reductions in range of motion (ROM) in hips with FAI [16, 18, 19, 25]. However, among other limitations, movement of the skin marker relative to the underlying bone (i.e., soft tissue motion artifact) prohibits accurate measurements and direct observation of hip articulation. Computer simulations have been used to estimate ROM and the location of impingement [2, 8, 11, 27]. Unfortunately, these simulations are driven using oversimplified, generic kinematics and/or assume terminal motion occurs as a result of direct collision between bones. Although FAI has been described as a condition of “repetitive abnormal contact between bony prominences” [22], the impingement process is likely to first involve contact between the femur and labrum before direct collision between the femur and pelvis bones. Accordingly, the location of femur-labrum contact may differ from where the distance between bones is a minimum.
Therefore, the purpose of this exploratory study was to use high-speed dual-fluoroscopy and model-based tracking to accurately measure dynamic hip articulation in vivo and identify locations of impingement in asymptomatic hips and hips with FAI during the impingement examination (90° flexion then maximal adduction and internal rotation). Only the motion of the bones is quantified dynamically using dual-fluoroscopy and model-based tracking. However, 3-D surface geometry of the labrum, generated from contrast-enhanced CT scans, can be assumed to move with the pelvis. Overlap between the femur and labrum surfaces can estimate the location of femur-labrum contact, whereas the region where bone-to-bone distance between the pelvis and femur is a minimum can serve as the location of possible bony impingement. Using these data, we asked: (1) Does femur-labrum contact occur at the terminal position of impingement? (2) Could ROM during the impingement examination appear decreased in hips with FAI? (3) Does the location of femur-labrum contact coincide with that of minimum bone-to-bone distance? (4) In patients with FAI, does the location of femur-labrum contact qualitatively correspond to the location of damage observed intraoperatively?
Patients and Methods
Study Participants
With institutional review board approval from The University of Utah, eight individuals were screened for grossly abnormal morphologic features and signs of osteoarthritis on an AP radiograph. Two individuals failed the AP screening. The first, a 20-year-old man, had findings consistent with undiagnosed Perthes; he subsequently recalled a history of hip pain during youth and young adulthood. The second, a 31-year-old woman, had very externally rotated ilia and bilateral acetabular retroversion. The six remaining individuals, who reported no history of hip pain, were enrolled as asymptomatic control subjects (Table 1).
Table 1.
Subject demographics
| Variable | Six asymptomatic control subjects | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|---|
| Gender | 2F, 4M | Male | Female | Female |
| Age (years) | 26 ± 3.7 | 25 | 23 | 26 |
| Height (cm) | 177 ± 12 | 180 | 168 | 173 |
| Weight (kg) | 65 ± 9.0 | 85.6 | 63.5 | 56.7 |
| BMI (kg/m2) | 21 ± 1.2 | 26.2 | 22.6 | 19 |
| Alpha angle* (°) | 45 ± 2.6 | 80 | 71 | 70 |
| Lateral center edge angle (°) | 34 ± 5.8 | 20 | 42 | 45 |
* Alpha angle measured on AP radiograph for asymptomatic control subjects and frog-leg lateral radiograph for patients.
Three patients with symptomatic FAI also were enrolled in this study (Table 1). These patients presented to a coauthor’s (SKA) clinic with continued left hip pain for greater 2 years that limited exercise and activities of daily living. Conservative treatment, including physical therapy, NSAIDs, and cessation of activity had failed. All patients reported pain during the impingement and flexion-abduction external rotation maneuvers and exhibited restricted ROM on gross inspection.
In the coauthor’s (SKA) clinic, the AP and frog-lateral view are the preferred radiographic projections to diagnose radiographic pincer and cam-type FAI, respectively. Therefore, these views were obtained of the three patients as part of the diagnostic workup (Fig. 1). Patient 1 presented with a pistol-grip cam deformity and mildly shallow acetabulum. Patient 2 presented with protrusio, a downward sloping sourcil, a large pincer groove, and a large bony prominence located on the anterolateral femoral neck. Patient 3 presented with mixed FAI, including acetabular overcoverage, femoral head asphericity, and a pincer groove on the anterolateral femoral neck. All three patients were treated with arthroscopic femoral osteochondroplasty, acetabuloplasty, and labral repair. The location and type of chondrolabral damage observed intraoperatively were recorded.
Fig. 1A–F.

(A) The AP radiograph for Patient 1 shows a mildly shallow acetabulum and (B) the frog-leg lateral radiograph shows decreased femoral head-neck offset. (C) The AP radiograph for Patient 2 shows protrusio and (D) the frog-leg lateral radiograph shows the pincer groove and femoral neck prominence. (E) The AP radiograph for Patient 3 shows acetabular overcoverage, and (F) the frog-leg lateral radiograph shows the pincer groove.
CT Arthrography and 3-D Reconstruction
CT arthrogram images of all study participants were obtained using a Siemens SOMATOM Definition Scanner (Siemens Medical Solutions USA, Inc, Malvern, PA, USA) [15]. The pelvis and proximal femora were imaged at 1 mm slice thickness, 342 ± 19.7 mm field of view (FOV) using a 512 × 512 matrix. To establish the femoral anatomic coordinate system, CT images of the knees were acquired at 3 mm slice thickness, with the same FOV and matrix as the hip. Images at the location of the hip were upsampled to ×3 resolution to reduce staircase artifact [15] and then segmented semiautomatically in Amira® (5.4.1, Visage Imaging, San Diego, CA, USA) to delineate the pelvis, femur, and acetabular labrum. Three-dimensional surfaces of each bone were generated to define anatomic coordinate systems, and then input to model-based tracking.
Dual-fluoroscopy
Following a validated protocol [17], dual-fluoroscopy video was acquired at 100 Hz during the entire impingement examination. The impingement examination was selected as it is a standard examination to test for FAI and is believed to place the hip in terminal ROM [13, 23, 24]. Each study participant was positioned supine on a radiolucent table with the left hip centered in the combined FOV of both fluoroscopes. A wide seatbelt-like strap secured the anterior-superior iliac spines to the table to ensure the pelvis remained in the FOV during the examination. The impingement examination began with the participant in the supine position with straight but relaxed legs. An orthopaedic surgeon (SKA) manipulated the lower limb of interest to approximately 90° hip and knee flexion and then simultaneously to maximum hip internal rotation and adduction. The leg then was returned to the starting position. Two trials were completed. The average fluoroscope tube voltage and current were 79 ± 7.0 kVp and 3.0 ± 0.37 mA, respectively.
Model-based Tracking
Model-based tracking dynamically determined the position and orientation of the pelvis and femur throughout the entire impingement examination [9, 17]. Briefly, images of a calibration cube established the relative position and perspective of the two fluoroscopes. Knowing this geometry, digitally reconstructed radiographs of the bone of interest relative to the two imaging planes were created via ray trace projection through the isolated bone image stacks. The user initially moved the bone in six degrees of freedom manually (three translations, three rotations) to approximately match the digitally reconstructed radiographs to fluoroscope images for the first frame of the video. Model-based tracking software then automatically determined the optimal pose and orientation of the bone for each video frame of the entire examination by iteratively changing the six degrees of freedom to maximize the normalized cross-correlation between pixel intensities in the digitally reconstructed radiographs and the fluoroscope images. Using cadaver hips, we previously validated the dual-fluoroscopy and model-based tracking approach to quantify hip kinematics during clinical examinations with translational and rotational tracking errors less than 0.48 mm and 0.58°, respectively [17].
Joint Angles
Anatomic coordinate systems of the pelvis and femur were established following the International Society of Biomechanics recommendations, with modifications to standardize landmark selection from the 3-D surfaces [17, 29]. Joint angles were calculated using the Grood and Suntay convention [14]. Joint angles for the entire impingement examination were plotted. For each participant, joint angles were reported as the average of the two trials. To facilitate comparisons between participants, joint angles were linearly interpolated between the start and end of the examination, the first peak in flexion, and the point of maximum internal rotation in flexion (defined as the terminal position of the examination).
Regions of Minimum Bone-to-Bone Distance and Femur-Labrum Contact
The 3-D surfaces and bone positions obtained by model-based tracking were imported into PostView (Musculoskeletal Research Laboratories, University of Utah, Salt Lake City, UT, USA) to observe motion. A custom tool in PostView measured bone-to-bone distance between the acetabular rim and femoral neck at the terminal point of the impingement examination. The minimum bone-to-bone distance at this time was averaged between the two trials for each participant and then reported as the average and standard deviation of all participants.
For the trial with a flexion angle closest to 90° at the terminal point at the examination, the location of possible bony impingement, based on the proximity of the femur relative to the pelvis, initially was defined by the location, termed a surface node, with the minimum bone-to-bone distance value. The region of possible bony impingement was expanded to contain this location and all nodes with bone-to-bone values in 0.5 mm of the minimum distance. The value of 0.5 mm was chosen to represent the average root mean square error of bone-to-bone distance measurements, as previously reported [17]. For the purpose of estimating the femur-labrum contact site, the 3-D surface for the labrum was assumed to move with the pelvis, without deformation. The estimated location of impingement between the femur and labrum was highlighted as the region of nodes where the femoral neck and rigid labrum surfaces overlapped, also obtained at the terminal position. The bone-to-bone and femur-labrum contact regions were compared qualitatively. If these two regions overlaid one another by 25% or more, good agreement between bone-to-bone distance and femur-labrum contact was noted. Because of the small number of participants and the exploratory nature of this study, statistical analyses were not performed.
Results
Except for one asymptomatic participant, contact occurred between the femur and labrum at the terminal position of the impingement examination. Patterns of femur-labrum contact were observed to be subject-specific, varying among the asymptomatic control subjects and the patients. In general, contact occurred between the femoral head-neck junction (Fig. 2) and the labrum in the 1 to 2 o’clock positions (3 o’clock represents anterior for the left hip) (Fig. 3). However, the location of impingement for Patient 2 was near the middle of the neck, distal in comparison to all other participants (Fig. 2).
Fig. 2A–I.

The locations of minimum bone-to-bone distance and labral contact at the terminal position of the impingement examination (maximum internal rotation in flexion) on the femur are shown for: (A) a 22-year-old asymptomatic man; (B) a 23-year-old asymptomatic man; (C) a 22-year-old asymptomatic man; (D) a 28-year-old asymptomatic man; (E) a 31-year-old asymptomatic woman; (F) a 27-year-old asymptomatic woman; (G) Patient 1, a 25-year-old man; (H) Patient 2, a 23-year-old woman; and (I) Patient 3, a 26-year-old woman. The region of minimum bone-to-bone distance is the region of the anterosuperior femoral head and neck closest to the acetabular rim. The region of labrum contact was defined as the region of overlap between the anterosuperior femoral head and neck and rigid labrum surface. (E) No contact between the labrum and anterosuperior femoral head and neck was detected for this asymptomatic control subject. (C and H) Regions of minimum bone-to-bone distance and femur-labrum contact overlapped by more than 25%.
Fig. 3A–I.

The locations of minimum bone-to-bone distance and labral contact at the terminal position of the impingement examination (maximum internal rotation in flexion), on the pelvis and labrum are shown for: (A) a 22-year old asymptomatic man; (B) a 23-year-old asymptomatic man; (C) a 22-year old asymptomatic man; (D) a 28-year-old asymptomatic man; (E) a 31-year-old asymptomatic woman; (F) a 27-year-old asymptomatic woman; (G) Patient 1, a 25-year-old man; (H) Patient 2, a 23-year-old woman; and (I) Patient 3, a 26-year-old woman. The region of minimum bone-to-bone distance is the region of the acetabular rim closest to the anterosuperior femoral head and neck. The region of labrum contact was defined as the region of overlap between the anterosuperior femoral head and neck and rigid labrum surface. (C) For this asymptomatic control subject, the location of labral contact was directly above the region of minimum bone-to-bone distance. (E) No contact between the labrum and anterosuperior femoral head and neck was detected for this asymptomatic control subject. (C and H) The regions of minimum bone-to-bone distance and femur-labrum contact overlapped by more than 25%.
The plotted joint angles showed possible deficiencies in internal rotation and adduction in the patients with FAI compared with the asymptomatic control subjects (Fig. 4). Specifically, at the terminal position of the impingement examination, internal rotation and adduction angles for each of the patients with FAI were less than the respective 95% confidence intervals (CIs) for the asymptomatic control subjects (Table 2). Hip flexion at the terminal position was approximately 90° to 100° for all participants, except Patient 2 who experienced flexion greater than 100° (Table 2).
Fig. 4A–D.

(A) Flexion, (B) adduction, and (C) internal rotation angles of the asymptomatic control subjects and patients with FAI during the impingement examination are shown. The angles are presented as mean ± 95% CIs for the asymptomatic control subjects. (D) Anterior views are shown for a subject with a normal hip at points of interest corresponding to x-axis tick marks on the joint angle plots: T1 = neutral/start of the examination; T2 = approximate midpoint of flexion; T3 = maximum flexion; T4 = maximum internal rotation in flexion/terminal position.
Table 2.
Joint angles at the terminal position of the impingement examination
| Study participants | Flexion (°) | Adduction (°) | Internal rotation (°) |
|---|---|---|---|
| Asymptomatic control subjects* | 93.0 (86.2–99.7) | 10.5 (6.7–14.4) | 19.1 (14.5–23.7) |
| Patient 1 | 94.7 | 5.7 | 11.6 |
| Patient 2 | 107.0 | 2.2 | 7.8 |
| Patient 3 | 97.1 | 3.2 | 9.7 |
* Data presented as mean (95% CI).
In the terminal position of the impingement examination, the minimum bone-to-bone distance between the acetabular rim and femur head and neck was on average (± SD) 3.0 ± 0.53 mm when considering all study participants; direct bone contact was not observed in any of the participants. The location of minimum bone-to-bone distance showed good agreement with the region of femur-labrum contact in only two participants, as displayed on the femur (Fig. 2) and acetabulum (Fig. 3). In the cases with disagreement, the region of femur-labrum contact appeared more superior to the region of minimum bone-to-bone distance.
With respect to the femur, the location of femur-labrum contact occurred on the cam lesion in Patient 1 and on the bony prominence lateral to the pincer groove in Patient 2 (Fig. 5). For Patient 3, contact with the anterosuperior labrum occurred directly along the pincer groove on the anterior femur (Fig. 5) (Video 1. Supplemental materials are available with the online version of CORR®).
Fig. 5A–F.

Positions of the pelvis, femur, and labrum for the patients at the terminal position of the impingement examination, maximum internal rotation in flexion, are shown. The black box highlights the enlarged region (shown to the right) to show the location of femur-labrum contact (*). (A) The position of Patient 1 in the terminal position is shown. (B) For Patient 1, contact between the femur and labrum occurs on the cam lesion. (C) The position of Patient 2 in the terminal position is shown. (D) The labrum contacts the bony prominence on the femur for Patient 2. (E) The position of Patient 3 in the terminal position is shown. (F) For Patient 3, the pincer groove on the femur contacts the labrum.
At the time of surgery, mechanical changes at the femoral head-neck junction in the pincer groove of Patient 3 were observed (Fig. 6). The labral tear observed during arthroscopy in Patient 1 and cartilage delamination in Patient 2 were located in the anterosuperior region of the acetabulum (Fig. 6). These areas of damage observed intraoperatively qualitatively compared well with the location of femur-labrum contact on the femur (Fig. 2) and acetabulum (Fig. 3).
Fig. 6A–C.
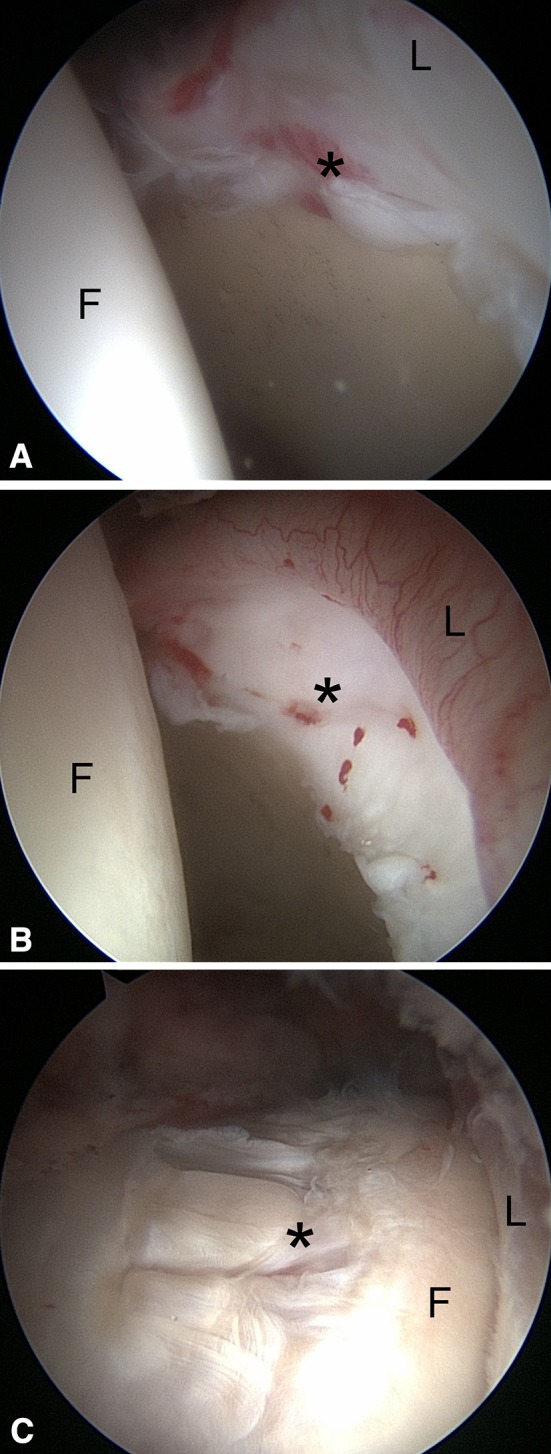
Arthroscopic images were obtained through an anterolateral portal (70° scope). (A) A labral tear and bruising (*) are seen at the anterosuperior chondrolabral junction in Patient 1. (B) Cartilage delamination (*) is observed at the anterosuperior chondrolabral junction in Patient 2. (C) Mechanical wear (*) is present at the location of the pincer groove on the anterolateral femoral neck in Patient 3. F = Femoral head, L = Labrum.
Discussion
Although germane to understanding mechanisms of soft tissue damage in the hip, the natural articulation between the femur, pelvis, and labrum has not been observed in vivo in the hip. In this study, we describe the use of high-speed dual-fluoroscopy and model-based tracking to measure in vivo hip articulation and estimate the locations of femur-labrum contact in six subjects with asymptomatic hips and three patients with FAI during the impingement examination. We investigated four specific questions and found that: (1) contact between the femur and labrum occurs in asymptomatic hips and hips with FAI at the terminal position of the impingement examination, but the patterns of contact are subject-specific; (2) hips with FAI conceivably could have reduced ROM during the impingement examination, as seen in the three patients with FAI, femur-labrum contact occurred at adduction and internal rotation angles less than the 95% CI of the mean of the asymptomatic cohort; (3) the actual location of femur-labrum contact coincided with the region of minimum bone-to-bone distance in only two of the nine participants; and (4) in the three patients with FAI, the location of femur-labrum contact qualitatively corresponded to the location of damage observed intraoperatively.
This study has some limitations. First, given the demanding experimental and computational methods, our sample size was small and statistical comparisons between groups were not performed. Nonetheless, our data represent the most accurate assessment of in vivo hip articulation in asymptomatic control subjects and patients with FAI to date. Second, subjects with asymptomatic hips were enrolled based only on an absence of grossly abnormal deformities and osteoarthritic changes, as visible on an AP film, and no history of hip pain. It is possible that other radiographic views would indicate the presence of deformities typically seen in patients with FAI. However, cutoff values and views in which to diagnose FAI have yet to be firmly established. Thus, we believe use of an AP film to screen for obvious deformities and absence of hip pain provided sufficient criteria to define a control group for this exploratory study. Third, as the labrum was not visible in the dual-fluoroscopy images, locations where the femur overlapped the labrum at the terminal position of the examination provided an estimate of the impingement site. In reality, the labrum would undergo deformation as it was compressed, stretched, or pushed aside. Nevertheless, by highlighting regions where the femur overlapped with the labrum using an imaging system with submillimeter accuracy, we believe the location of femur-labrum contact was accurately represented. Use of overlapping surfaces as a measure of soft tissue strain has been used in other dual-fluoroscopy studies, such as those of the ankle and knee [10, 28]. In addition, our results are supported by those of a cadaver experiment, where strain in the anterosuperior labrum was increased substantially during the impingement examination compared with neutral position [26]. Fourth, in the current study, the arthroscopic tool used to observe intraarticular damage in the three patients with FAI was not aligned spatially with the dual-fluoroscopy system. Thus, we could only qualitatively compare the location of intraarticular damage with that of femur-labrum contact estimated by model-based tracking. Finally, hyaline cartilage geometry was not included. While the presence of cartilage on the femur could change the location of femur-labrum contact, cartilage is thin or nonexistent in the femoral neck region. Therefore, it is expected that the region of contact would not change substantially if cartilage had been included.
In this study, impingement between the femur head-neck junction and anterosuperior labrum was observed in hips with FAI and asymptomatic hips. We found femur-labrum contact patterns to have high intersubject variability. Subtle differences in hip anatomy, even between individuals with asymptomatic hips, were likely responsible for the observed variability. Similarly, a subject-specific finite element modeling study of 10 healthy subjects (similar age and stature to those in the current study) showed wide variability in cartilage contact stress patterns between individuals [15]. The authors suggested that the subtle variation in cartilage and bone geometry was responsible for the resulting cartilage stress patterns [15]. Accordingly, hip function, including impingement, could be governed largely by the underlying anatomy. The use of dual-fluoroscopy and model-based tracking on a larger cohort could confirm which morphologic features drive femur-labrum contact patterns, and therefore deserve the most attention at the time of surgery.
The observed femur-labrum impingement suggests the impingement examination places the hip in a terminal position. Hip flexion angles were similar among the patients and asymptomatic control subjects, and were near 90° (except for Patient 2 who experienced greater hip flexion). This similarity implies the impingement examination was performed as intended (90° hip flexion then adduction and internal rotation). On the contrary, each of the patients with FAI exhibited adduction and internal rotation angles less than the 95% CI of the asymptomatic control subjects, consistent with clinical observations and ROM studies [1, 12, 13]. However, with a limited sample size, and in the absence of statistical tests, it is possible these observed decreases were the effect of chance. Use of dual-fluoroscopy on a larger sample size during clinical examinations will need to confirm the trends we observed for the three patients with FAI. Others have found statistically significant differences in ROM in patients with FAI using reflective markers placed on the skin [16, 18, 25]. For example, Hunt et al. found decreased hip adduction, internal rotation, and extension at the stance phase of walking [16]. In a similar study of walking and stair climbing, Rylander et al. found decreased hip internal rotation and sagittal plane ROM in patients with FAI compared with controls [25]. However, without direct observation of joint articulation, it is unknown if the reduced ROM reported in these studies is the result of impingement or other possible factors such as muscular compensation or pain avoidance. In the future, dual-fluoroscopy of subjects undergoing active, load-bearing activities will enable direct comparisons to the existing literature and allow us to investigate if the bony abnormalities of FAI alter ROM during dynamic activities.
FAI has been described as a condition of “repetitive abnormal contact between bony prominences” [22]. However, in our study, we did not observe direct bone-to-bone contact in any of the participants; the minimum distance between the femoral neck and acetabular rim averaged 3 mm. Still, we choose to highlight the area of minimum bone-to-bone distance for the purpose of comparing it with the estimated location of femur-labrum contact. Software to plan surgery for patients with FAI has been developed that predicts the impingement site based on direct bone collision between the femur and pelvis [3, 8, 27]. However, the region where the two bones are close to one another may differ from the actual location of femur to labrum contact (i.e., impingement). Given that regions of femur-labrum contact did not always correspond to the region of minimum bone-to-bone distance, we believe it may be ill-advised to assume that the region where the pelvis and femur bones collide in simulations is the same as that where the femur directly contacts the labrum. Software that relies on direct bone-to-bone contact likely overestimates ROM and may not provide an accurate description of true hip arthrokinematics if not validated appropriately. We will need to analyze a larger cohort of subjects with dual-fluoroscopy to confirm femur-labrum contact occurs in regions outside those where bones are close to one another.
With use of dual-fluoroscopy and model-based tracking in a cohort of live subjects, we found hip articulation to be a highly complex and variable process. In this exploratory study, femur-labrum contact during the impingement examination was observed in hips with FAI and asymptomatic hips. While more subjects are needed to confirm the trend, each of three patients with FAI experienced internal rotation and adduction angles less than the 95% CI of the asymptomatic subjects. The high intersubject variability in the pattern of femur-labrum contact provides evidence that subtle anatomic features could dictate underlying hip biomechanics. Overall, these femur-labrum patterns may not be predicted by the location of minimum bone-to-bone distance, highlighting the need to include labral anatomy in future analyses. Collectively, our data motivate the development of patient-specific approaches to diagnose and treat FAI. For example, knowing the location of labrum contact on a per-patient basis could influence the chosen surgical approach. Additional research, using a larger cohort and appropriate statistical tests, is required to confirm the findings of this exploratory study.
Electronic supplementary material
Acknowledgments
We thank Blake Zimmerman, Department of Bioengineering, University of Utah, and Justine Goebel, Department of Bioengineering, University of Utah, for assistance with segmentation and model-based tracking.
Footnotes
The institution of one or more of the authors (ALK) has received, during the study period, funding from the LS Peery Discovery Program in Musculoskeletal Restoration. One of the authors certifies that he (SKA) has or may receive payments or benefits, during the study period, an amount of USD 10,000–USD 100,000 from Pivot Medical (Sunnyvale, CA, USA) and an amount of USD 10,000–USD 100,000 from Arthrocare Corp (Austin, TX, USA). One of the authors certifies that he (CLP) has or may receive payments or benefits, during the study period, an amount of USD 10,000–USD 100,000 from Biomet (Warsaw, IN, USA).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
References
- 1.Audenaert E, Van Houcke J, Maes B, Vanden Bossche L, Victor J, Pattyn C. Range of motion in femoroacetabular impingement. Acta Orthop Belg. 2012;78:327–332. [PubMed] [Google Scholar]
- 2.Audenaert EA, Mahieu P, Pattyn C. Three-dimensional assessment of cam engagement in femoroacetabular impingement. Arthroscopy. 2011;27:167–171. doi: 10.1016/j.arthro.2010.06.031. [DOI] [PubMed] [Google Scholar]
- 3.Audenaert EA, Peeters I, Vigneron L, Baelde N, Pattyn C. Hip morphological characteristics and range of internal rotation in femoroacetabular impingement. Am J Sports Med. 2012;40:1329–1336. doi: 10.1177/0363546512441328. [DOI] [PubMed] [Google Scholar]
- 4.Beaule PE, Hynes K, Parker G, Kemp KA. Can the alpha angle assessment of cam impingement predict acetabular cartilage delamination? Clin Orthop Relat Res. 2012;470:3361–3367. doi: 10.1007/s11999-012-2601-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Beaule PE, O’Neill M, Rakhra K. Acetabular labral tears. J Bone Joint Surg Am. 2009;91:701–710. doi: 10.2106/JBJS.H.00802. [DOI] [PubMed] [Google Scholar]
- 6.Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005;87:1012–1018. doi: 10.1302/0301-620X.87B7.15203. [DOI] [PubMed] [Google Scholar]
- 7.Bedi A, Dolan M, Leunig M, Kelly BT. Static and dynamic mechanical causes of hip pain. Arthroscopy. 2011;27:235–251. doi: 10.1016/j.arthro.2010.07.022. [DOI] [PubMed] [Google Scholar]
- 8.Bedi A, Dolan M, Magennis E, Lipman J, Buly R, Kelly BT. Computer-assisted modeling of osseous impingement and resection in femoroacetabular impingement. Arthroscopy. 2012;28:204–210. doi: 10.1016/j.arthro.2011.11.005. [DOI] [PubMed] [Google Scholar]
- 9.Bey MJ, Zauel R, Brock SK, Tashman S. Validation of a new model-based tracking technique for measuring three-dimensional, in vivo glenohumeral joint kinematics. J Biomech Eng. 2006;128:604–609. doi: 10.1115/1.2206199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bingham JT, Papannagari R, Van de Velde SK, Gross C, Gill TJ, Felson DT, Rubash HE, Li G. In vivo cartilage contact deformation in the healthy human tibiofemoral joint. Rheumatology (Oxford). 2008;47:1622–1627. doi: 10.1093/rheumatology/ken345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chang TC, Kang H, Arata L, Zhao W. A pre-operative approach of range of motion simulation and verification for femoroacetabular impingement. Int J Med Robot. 2011 Jun 18 [Epub ahead of print]. [DOI] [PubMed]
- 12.Clohisy JC, Knaus ER, Hunt DM, Lesher JM, Harris-Hayes M, Prather H. Clinical presentation of patients with symptomatic anterior hip impingement. Clin Orthop Relat Res. 2009;467:638–644. doi: 10.1007/s11999-008-0680-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112–120. doi: 10.1097/01.blo.0000096804.78689.c2. [DOI] [PubMed] [Google Scholar]
- 14.Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng. 1983;105:136–144. doi: 10.1115/1.3138397. [DOI] [PubMed] [Google Scholar]
- 15.Harris MD, Anderson AE, Henak CR, Ellis BJ, Peters CL, Weiss JA. Finite element prediction of cartilage contact stresses in normal human hips. J Orthop Res. 2012;30:1133–1139. doi: 10.1002/jor.22040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hunt MA, Guenther JR, Gilbart MK. Kinematic and kinetic differences during walking in patients with and without symptomatic femoroacetabular impingement. Clin Biomech (Bristol, Avon). 2013;28:519–523. [DOI] [PubMed]
- 17.Kapron A, Aoki S, Peters CL, Mass SA, Bey MJ, Zauel R, Anderson AE. Accuracy and feasibility of dual fluoroscopy and model-based tracking to quantify in vivo hip kinematics during clinical exams. J Appl Biomech. 2014 Feb 25 [Epub ahead of print]. [DOI] [PMC free article] [PubMed]
- 18.Kennedy MJ, Lamontagne M, Beaule PE. Femoroacetabular impingement alters hip and pelvic biomechanics during gait walking biomechanics of FAI. Gait Posture. 2009;30:41–44. doi: 10.1016/j.gaitpost.2009.02.008. [DOI] [PubMed] [Google Scholar]
- 19.Lamontagne M, Kennedy MJ, Beaule PE. The effect of cam FAI on hip and pelvic motion during maximum squat. Clin Orthop Relat Res. 2009;467:645–650. doi: 10.1007/s11999-008-0620-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lavigne M, Parvizi J, Beck M, Siebenrock KA, Ganz R, Leunig M. Anterior femoroacetabular impingement: Part I. Techniques of joint preserving surgery. Clin Orthop Relat Res. 2004;418:61–66. doi: 10.1097/00003086-200401000-00011. [DOI] [PubMed] [Google Scholar]
- 21.Lee CB, Clark J. Fluoroscopic demonstration of femoroacetabular impingement during hip arthroscopy. Arthroscopy. 2011;27:994–1004. doi: 10.1016/j.arthro.2011.01.020. [DOI] [PubMed] [Google Scholar]
- 22.Pfirrmann CW, Mengiardi B, Dora C, Kalberer F, Zanetti M, Hodler J. Cam and pincer femoroacetabular impingement: characteristic MR arthrographic findings in 50 patients. Radiology. 2006;240:778–785. doi: 10.1148/radiol.2403050767. [DOI] [PubMed] [Google Scholar]
- 23.Philippon M, Schenker M, Briggs K, Kuppersmith D. Femoroacetabular impingement in 45 professional athletes: associated pathologies and return to sport following arthroscopic decompression. Knee Surg Sports Traumatol Arthrosc. 2007;15:908–914. doi: 10.1007/s00167-007-0332-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Philippon MJ, Maxwell RB, Johnston TL, Schenker M, Briggs KK. Clinical presentation of femoroacetabular impingement. Knee Surg Sports Traumatol Arthrosc. 2007;15:1041–1047. doi: 10.1007/s00167-007-0348-2. [DOI] [PubMed] [Google Scholar]
- 25.Rylander J, Shu B, Favre J, Safran M, Andriacchi T. Functional testing provides unique insights into the pathomechanics of femoroacetabular impingement and an objective basis for evaluating treatment outcome. J Orthop Res. 2013;31:1461–1468. doi: 10.1002/jor.22375. [DOI] [PubMed] [Google Scholar]
- 26.Safran MR, Giordano G, Lindsey DP, Gold GE, Rosenberg J, Zaffagnini S, Giori NJ. Strains across the acetabular labrum during hip motion: a cadaveric model. Am J Sports Med. 2011;39(suppl):92S–102S. doi: 10.1177/0363546511414017. [DOI] [PubMed] [Google Scholar]
- 27.Tannast M, Kubiak-Langer M, Langlotz F, Puls M, Murphy SB, Siebenrock KA. Noninvasive three-dimensional assessment of femoroacetabular impingement. J Orthop Res. 2007;25:122–131. doi: 10.1002/jor.20309. [DOI] [PubMed] [Google Scholar]
- 28.Wan L, de Asla RJ, Rubash HE, Li G. In vivo cartilage contact deformation of human ankle joints under full body weight. J Orthop Res. 2008;26:1081–1089. doi: 10.1002/jor.20593. [DOI] [PubMed] [Google Scholar]
- 29.Wu G, Siegler S, Allard P, Kirtley C, Leardini A, Rosenbaum D, Whittle M, D’Lima DD, Cristofolini L, Witte H, Schmid O, Stokes I; Standardization and Terminology Committee of the International Society of Biomechanics. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion: part I. Ankle, hip, and spine. International Society of Biomechanics. J Biomech. 2002;35:543–548. [DOI] [PubMed]
- 30.Zebala LP, Schoenecker PL, Clohisy JC. Anterior femoroacetabular impingement: a diverse disease with evolving treatment options. Iowa Orthop J. 2007;27:71–81. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.