

Abstract
Background
The aim of this study was to follow up the 17 children, from a total group of 208 children with autism spectrum disorder (ASD), who “recovered from autism”. They had been clinically diagnosed with ASD at or under the age of 4 years. For 2 years thereafter they received intervention based on applied behavior analysis. These 17 children were all of average or borderline intellectual functioning. On the 2-year follow-up assessment, they no longer met criteria for ASD.
Methods
At about 10 years of age they were targeted for a new follow-up. Parents were given a semistructured interview regarding the child’s daily functioning, school situation, and need of support, and were interviewed using the Vineland Adaptive Behavior Scales (VABS) and the Autism – Tics, Attention-deficit/hyperactivity disorder (AD/HD), and other Comorbidities (A-TAC) telephone interview.
Results
The vast majority of the children had moderate-to-severe problems with attention/activity regulation, speech and language, behavior, and/or social interaction. A majority of the children had declined in their VABS scores. Most of the 14 children whose parents were A-TAC-interviewed had problems within many behavioral A-TAC domains, and four (29%) had symptom levels corresponding to a clinical diagnosis of ASD, AD/HD, or both. Another seven children (50%) had pronounced subthreshold indicators of ASD, AD/HD, or both.
Conclusion
Children diagnosed at 2–4 years of age as suffering from ASD and who, after appropriate intervention for 2 years, no longer met diagnostic criteria for the disorder, clearly needed to be followed up longer. About 3–4 years later, they still had major problems diagnosable under the umbrella term of ESSENCE (Early Symptomatic Syndromes Eliciting Neurodevelopmental Clinical Examinations). They continued to be in need of support, educationally, from a neurodevelopmental and a medical point of view. According to parent interview data, a substantial minority of these children again met diagnostic criteria for ASD.
Keywords: autism spectrum disorder, autistic traits, AD/HD, A-TAC, Vineland, cure
Video abstract
Introduction
Most studies report that children once diagnosed with an autism spectrum disorder (ASD) still meet diagnostic criteria for the disorder when evaluated several years later, suggesting a high degree of diagnostic stability for the overall spectrum of ASDs.1–3 However, the stability has been demonstrated to vary across subtypes of ASD diagnoses.4 Charman5 discussed that a diagnosis of classic autism was more stable than a PDD-NOS (pervasive developmental disorder, not otherwise specified) diagnosis or atypical autism and introduced the term “working diagnosis” to be used in children with a clinical presentation not indisputably consistent with a definite ASD diagnosis. The stability of an initial ASD diagnosis in community settings was studied by Daniels et al.6 These authors reported that 22% of the children had received a current diagnosis that was different from their initial one. PDD-NOS was the least stable diagnosis, and stability was largely dependent on the specific initial ASD diagnosis. Factors reported to be influential with regard to stability were diagnosing clinician, region, when in time a child was initially diagnosed, and a history of autistic regression.
A long-term follow-up study of 28 children, using Autism Diagnostic Interview – Revised (ADI-R) criteria to classify ASD, revealed that the ASD diagnoses generally remained stable between preschool and elementary school age but that many children demonstrated significant improvements in symptom severity.7
In a study of optimal outcome in individuals with autism, it was documented that a group with clear early histories of autism at follow-up showed normal language, face recognition, communication, and social interaction – and no autism symptoms. Although possible deficits in more subtle aspects of social interaction or cognition were not ruled out, the results substantiated the possibility of optimal outcome from ASDs and an overall level of functioning within normal limits for a subgroup.8
In early studies9 (see also the work by Broderick10), children diagnosed with ASD who, on follow-up (usually after intensive intervention), no longer met diagnostic criteria for the disorder, or who had improved cognitively, were sometimes described as having “recovered”.
We have previously presented data from a naturalistic intervention study, including preschool children with ASD, referred to a specialized autism center. After a 2-year follow-up, one subgroup did not fully meet criteria for ASD but had autistic traits. The aims of this study were to perform a second follow-up when the children with autistic traits and without intellectual disability (ID) were at young school age, to assess their current adaptive, developmental, behavioral, and ASD profiles and to analyze the proportion that might again meet criteria for ASD. Our study looks at such a group of “recovered from autism” children several years after “recovery”, with a view to establishing their longer-term prognosis.
Subjects
Original study group
The original study group was population-based and representative – except for the most severely multi-impaired children with autism who had been referred to their local habilitation center.11–16
The children had been examined by a research team including neuropediatricians/child psychiatrists, psychologists, and speech and language pathologists when included in the study – Time 1 (T1) – before interventions started and at follow-up 2 years later – Time 2 (T2). Interventions had been of different intensities and all based on applied behavior analysis, intensive and nonintensive.12 At the 2-year follow-up, some children were found no longer to meet full criteria for ASD.
The original study group consisted of the 313 preschool children (birth-years 2002–2006) in the county of Stockholm who had been diagnosed by clinicians – after multidisciplinary assessment – as suffering from ASD before 4.5 years of age. Of these 313 children, 25 had been referred to their local habilitation center, mainly due to complex medical needs and severe multi-impairments. Of the remaining 288 children, 24 had been referred to the center prior to study start, 37 families declined participation, 15 families could not communicate in either Swedish or English, two children moved abroad, and another two were referred to local habilitation centers due to complex medical needs. Thus, 208 children (176 boys and 32 girls) were included in the 2-year follow-up study,11 and of these, 198 could be followed up for 2 years at the Autism Center for Young Children (ACYC).12 The distribution of DSM-IV-TR (the Diagnostic and Statistical Manual of Mental Disorders, 4th edition – text revision) ASD subgroups at T1 and T2, respectively, was 62% and 53% with autistic disorder (AD), 26% and 29% with PDD-NOS, 4% and 7% with Asperger syndrome, and 9% and 11% with autistic traits. At T2, 48% of the children had ID, 25% had borderline intellectual functioning, 26% had average intelligence quotient (IQ), and in 1% of the children no cognitive test had been performed.12 In four children with autistic traits at T2, ID was considered the main disorder, and these children were not included in this second follow-up.
At T2, all parents had been offered several interviews: The Diagnostic Interview for Social and Communication disorders,17 The Autism Behavior Checklist,18 and a structured clinical interview including all aspects of the child’s development – Paris Autism Research International Sibpair Study19 and the Vineland Adaptive Behavior Scales-II.20 All clinical information was pooled and evaluated according to the DSM-IV-TR criteria.21
Of the 198 children, who were assessed after 2 years, 21 did not meet full criteria for ASD, according to DSM-IV-TR,21 but all had some autistic traits. Of these 21 children, four met criteria for ID and 17 did not. These remaining 17 children, in addition to their autistic traits, had a variety of other developmental problems in areas of speech and language, attention, activity regulation, and behavior. From the point of view of “autism”, they did not meet diagnostic criteria for any ASD, and would, by some, therefore be considered “recovered from autism”. We wanted to examine them again several years later, at Time 3 (T3), to ascertain what had happened to them, both in terms of developmental/psychiatric/adaptive functioning and further intervention needed.
Present study group
Thus, the present study group consisted of 17 children: 13 boys and four girls (age range, 8–11 years; median, 10 years). At the initial referral to the ACYC at original study start, they all had a diagnosis of ASD according to DSM-IV-TR. When assessed by the study team shortly after inclusion, nine met criteria for PDD-NOS and the other eight were regarded as having autistic traits only. At the 2-year follow-up (T2), at ages 4.5–6.5 years, all were found to have autistic traits and, in addition, various other developmental deviations in areas of speech and language, attention and activity regulation, and behavioral problems. They all had IQs within the area of average or borderline intellectual functioning.12
Methods
At T3, the parents of the children were again contacted by letter and telephone. Two interviews (a clinical semistructured interview and the Vineland Adaptive Behavior Scales [VABS])20 were conducted by the first author (MBO), and a third interview (the Autism – Tics, Attention-deficit/hyperactivity disorder [AD/HD], and other Comorbidities [A-TAC])22 was conducted over the telephone by an experienced layperson from a market research center.
Parental semistructured interview
A semistructured telephone interview was conducted with one of each child’s parents, to obtain information about the child’s current situation in and out of school. Questions on the type of school and school support were raised, as were questions pertaining to different developmental domains: speech and language, social abilities, activity and impulsivity regulation, attention span, and externalizing behavior. Parents were also asked if the child had had any new clinical assessments at a Child and Adolescent Mental Health Service (CAMHS) and/or a pediatric department since the research follow-up at the ACYC (T2), if the family had any ongoing contacts with a pediatrician/neuropediatrician, child psychiatrist, or habilitation center, and if the parents found that the services they received met their needs.
A-TAC interview
A-TAC22–24 inventory interview was performed with one of the child’s parents. The A-TAC is a screening interview focusing on virtually all common child and adolescent psychiatry and is designed for use by laymen over the phone. The A-TAC has been validated against clinically ascribed diagnoses cross-sectionally22,23 and longitudinally,24 and has been found to be a sensitive tool to screen for ASD, AD/HD, tics, learning disorder, and developmental coordination disorder (DCD).21 For ASD, AD/HD, and learning disorder, two cutoffs exist: 1) “high”, which is a clinical proxy for a clinical diagnosis with moderate sensitivity but high specificity; and 2) “low”, which is a broad screening level with high sensitivity but moderate specificity designed to capture pronounced subthreshold traits of clinical disorder.23,24
Vineland Adaptive Behavior Scales interview
The VABS20 was also used with one of the child’s parents. This interview includes Communication, Daily Living Skills, and Social Domains, and a Composite score. The interview is administered to a parent or caregiver using a semistructured interview format, which provides a targeted assessment of adaptive behavior. The interview was given on the telephone, taking approximately 45–60 minutes. Of the children in the study, all had had complete VABS results, both at T1 and T2.
Statistical analyses
Differences between the three time points and between the three VABS subscale mean scores (Communication, Daily Living Skills, Social Domains) were analyzed with a repeated measures analysis of variance (ANOVA). In this analysis, partial eta squared (η2partial) was used as a measure of effect size. The ANOVA was followed up by post hoc analysis (Bonferroni) in order to study differences between specific time points. An α level of 0.05 was used for all statistical analyses.
Ethical approval
The study was approved by the ethical committee at Karolinska Institutet.
Results
Of the 17 children, parents of 16 (12 boys and four girls [age range, 7–11 years; mean age, 9 years]) could be reached. For one family, contact details could not be obtained. Parents of all 16 children participated in the semistructured interview and in the Vineland interview. Parents of 14 children participated in the A-TAC interview.
Semistructured interview
School situation
All but one of the 16 children studied according to the normal curriculum. One child studied according to a specialized curriculum for children with ID, but in a regular classroom. Four other children had special tutoring or an assistant at school. Five parents expressed that their children did not have sufficient support in school.
Social interaction
Parents of 13 of the 16 children reported that their children had various difficulties with social interaction. Problems included difficulties with mentalizing and hyperactivity/impulsivity, leading to inability to foresee consequences of their own actions. Typical problems reported were “difficulties to interact with more than one person at a time”, “plays only with younger children”, “easily deceived”, and “does not understand other children’s games”.
AD/HD symptoms
Parents of 13 of the 16 children reported problems in their children regarding attention, and nine of these also had problems with hyperactivity and/or impulsivity. The reported symptoms within the AD/HD spectrum were mainly in accordance with the situation at T2, and one child had now received a diagnosis of AD/HD at clinical assessment in between T2 and T3. At T3, a total of four of the 16 children had pharmacological treatment for AD/HD.
Speech and language
Of the 16 children, parents of 12 reported that their children had problems with speech and language (within at least one of the following language domains: grammar, expressive speech, vocabulary, pragmatic deficiency, and articulation). Of these 12 children, four had or had had regular contact with a speech and language pathologist and/or attended/had attended a special speech/language class.
Behavior
Parents of 15 children reported that their children had behavioral problems. In three of these children, the problems were severe (externalizing, often aggressive behavior). These three children also had clear indications of ASD combined with attention/hyperactivity/impulsivity symptoms.
New clinical assessments (dyslexia not included)
Two children had had a further neuropsychiatric/neurodevelopmental assessment in between T2 and T3. One child had received a diagnosis of AD/HD and the other of Asperger syndrome.
Regular contacts with pediatric/psychiatric or habilitation services
Seven children had some contact with the CAMHS, and five of the 16 children were followed up by a pediatrician on a regular basis. Three of these five had overweight problems, another had diabetes type 1, and yet another had a chromosomal abnormality.
A-TAC interview
Most children presented problems within several areas (Table 1). Five modules were targeted: ASD, AD/HD, tic disorder, DCD, and learning disorder. Three children had symptom levels corresponding to a clinical proxy of ASD and six reached the cutoff for the broad screening diagnosis. Three children had symptom levels corresponding to a clinical proxy of AD/HD, and another six encompassed the broad screening cutoff. Five children had symptom levels corresponding to tic disorder, one had DCD, and one had symptom levels corresponding to learning disorder.
Table 1.
Screening diagnoses in individual children according to A-TAC
| Child number | Screening diagnoses
|
Number of screening diagnoses | |||||||
|---|---|---|---|---|---|---|---|---|---|
| ASD
|
AD/HD
|
TDs | DCD | ID
|
|||||
| High | Low | High | Low | High | Low | ||||
| 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | –a | 4 |
| 2 | 1 | –a | 1 | –a | 1 | 0 | 0 | 1 | 3 |
| 3 | 1 | –a | 1 | –a | 1 | 1 | 0 | 0 | 4 |
| 4 | 1 | –a | 0 | 1 | 0 | 0 | 0 | 0 | 2 |
| 5 | 0 | 1 | 1 | –a | 1 | 0 | 0 | 0 | 3 |
| 6 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 2 |
| 7 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 3 |
| 8 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 3 |
| 9 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| 10 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 11 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 12 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 13 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| 14 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
Note:
In cases in which one of the “high” diagnoses applies, the threshold for the corresponding “low” diagnosis is automatically met, meaning that these are not included in the total number of screening diagnoses.
Abbreviations: A-TAC, Autism – Tics, AD/HD, and other Comorbidities; ASD, autism spectrum disorder; AD/HD, attention-deficit/hyperactivity disorder; TDs, tic disorders; DCD, developmental coordination disorder; ID, intellectual disability.
Vineland Adaptive Behavior Scales
A 3×3 repeated measures ANOVA with T1, T2 and T3 and Subscale (Communication, Daily Living Skills, Social Domains) as within-subject factors and VABS score as the dependent variable showed a significant main effect of Time (F2,60=7.36, P=0.003, η2partial =0.33). As can be seen in Figure 1, mean VABS scores increased for all subscales between T1 and T2, but then decreased – also for all subscales – between T2 and T3. Post hoc analysis (Bonferroni) showed that the overall increase between T1 and T2 was significant (P=0.036), as was the decrease between T2 and T3 (P=0.005). The difference between T1 and T3 was not significant (P=0.879). Finally, there was no main effect of Subscale (F2,60=2.84, P=0.074, η2partial =0.16) and no Time × Subscale interaction (F4,60=1.70, P=0.163, η2partial =0.10); that is, there was no significant difference between the three subscales regarding the pattern with increasing VABS scores between T1 and T2 and decreasing scores between T2 and T3.
Figure 1.
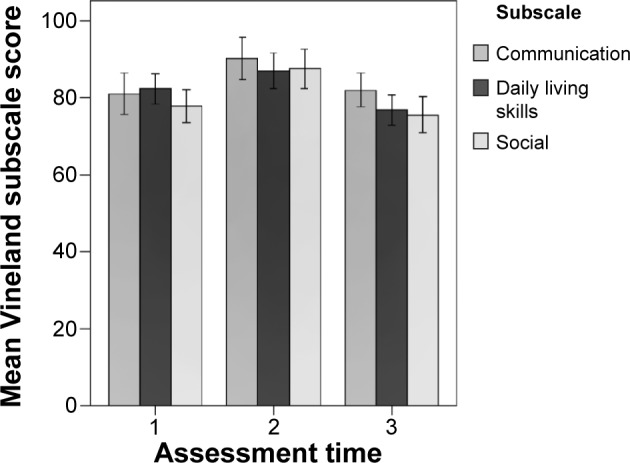
Mean VABS scores with 95% confidence intervals for the three assessment times and for the three subscales.
Abbreviation: VABS, Vineland Adaptive Behavior Scales.
Discussion
This study analyzed the longer-term outcomes for a group of 17 children who, at a previous follow-up after ASD intervention, 3–4 years earlier, had “recovered from” ASD, meaning that they no longer met clinical diagnostic criteria for ASD.
The study group was small but comprised all the children no longer diagnosable as ASD from a large and representative group originally diagnosed with ASD (at 2–4.5 years of age), 2 years after the start of ASD intervention. Parents of 16 of these 17 children took part in the longer-term outcome study.
At the new follow-up around age 10 years, all the children had major behavioral and/or academic problems. Of the 13 children with social interaction problems in the semistructured parental interview, 12 also had repeated tantrums, nine had difficulties with hyperactivity or impulsivity, and two with passivity. Eleven of the children had difficulties concentrating, and ten had speech problems. Hence, it was evident that a majority of the children had problems in several different domains.
According to the A-TAC interview, three of the 14 children who participated were considered to again meet full criteria for ASD. Of the remaining 13 children, another six had pronounced subthreshold ASD symptoms.
Overall, according to the clinical interview and the A-TAC interview, there were high rates of attention deficits and difficulties with regulating activity level and impulsivity. Many children also had tic disorders, and the vast majority had some problems with speech and language. No child was without developmental/neuropsychiatric problems at this school-age follow-up.
Thus, our study group had several remaining neurodevelopmental/neuropsychiatric symptoms, in some cases with levels corresponding to clinical neurodevelopmental disorders/diagnoses. Of the nine children with either high or low score for ASD in the A-TAC interview, seven also had high or low scores for AD/HD, thus supporting the high co-occurrence between the two disorders. There are many studies reporting strong relationships between ASD (or social-communication traits) and AD/HD (or hyperactive traits) in children and adolescents, supporting the evidence for the coexistence of ASD and AD/HD.25–27
Different types of behavioral problems were very common and of a severe degree, with externalizing behavior in three of the 16 children. In a study of tantrum profiles in children, aged 3–16 years, with ASD, AD/HD, and combined ASD and AD/HD, it was found that tantrum behaviors were observed at relatively high levels in children with ASD alone, with AD/HD alone, and with comorbid ASD and AD/HD, and that tantrum behavior was highest in the combined ASD and AD/HD group.28
Concerning adaptive functions, VABS scores showed that a majority of the children at this time had declined since the former period of measurement. The reasons for this are difficult to know. It is possible that this is merely an effect of a regression to the mean, considering that these 17 children had been chosen because of their good progress (“recovered” from ASD). It is also possible that both the children and their parents had been helped by earlier applied behavior analysis interventions, which in some children had been of intensive type and in some of a targeted type (mediated by the ACYC), by parental education and general family support from the ACYC. The behavioral interventions had been terminated after 2 years, and also parent training and general family support were reduced as the children grew older. At the same time, higher demands were being placed on the children in school compared to preschool, all of which may have contributed to the declining trend. On top of this, many did not have sufficient support in school according to their needs.
Study limitations include a small number of cases and, at T3, information based only on parent report in telephone interviews. This is in contrast to T2, when the children were comprehensively assessed by different members of the study team and a questionnaire was filled out by nursery school staff, apart from parental interviews. Another limitation is the lack of a comparison group consisting of age- and IQ-matched children still meeting criteria for ASD. Corresponding data from other subgroups will be presented in forthcoming studies.
The study revealed, however, that most preschool children, once diagnosed with ASD – but found to be under the threshold for a diagnosis of ASD 2 years later – at further follow-up, still have different combinations of neurodevelopmental/neuropsychiatric problems, and that some again meet full criteria for ASD. The majority of children have different problems that accord with the umbrella term of ESSENCE (Early Symptomatic Syndromes Eliciting Neurodevelopmental Clinical Examinations)29 even after appropriate intervention for 2 years. Children in this group had autistic symptoms, attention deficits, hyperactivity/impulsivity, other behavioral problems, and language difficulties.
All these children are in continued need of support, educationally, from a neurodevelopmental and medical point of view, for several years during childhood. However, our current societal system to a large extent restricts services to certain diagnoses, such as ID and ASD. This means that many children with combinations of developmental problems – autistic symptoms, and attention, language, and behavioral problems – and their parents, do not receive the appropriate support that they need from habilitation services and society.
Conclusion
In conclusion, our study revealed that children diagnosed at preschool age as suffering from ASD and who, after appropriate intervention for 2 years, no longer met diagnostic criteria for the disorder, need to be followed up carefully for several more years. They still have problems that are diagnosable under the umbrella term of ESSENCE, and they are in continued need of support. Some of these children again meet diagnostic criteria for ASD.
Acknowledgments
Financial support was given through a grant support from Prima Child and Adult Psychiatry, from Kempe Carlgrens Foundation, from the Wilhelm and Martina Lundgren Research Foundation (MBO), from the LifeWatch Award, Niclas Öberg Foundation (EF), and from Per and Annmari Ahlqvist Foundation (CG). We are much obliged to the families who have taken part in the study.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Lord C, Risi S, DiLavore PS, Shulman C, Thurm A, Pickles A. Autism from 2 to 9 years of age. Arch Gen Psychiatry. 2006;63:694–701. doi: 10.1001/archpsyc.63.6.694. [DOI] [PubMed] [Google Scholar]
- 2.Chawarska K, Klin A, Paul R, Macari S, Volkmar F. A prospective study of toddlers with ASD: short-term diagnostic and cognitive outcomes. J Child Psychol Psychiatry. 2009;50:1235–1245. doi: 10.1111/j.1469-7610.2009.02101.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kočovská E, Billstedt E, Ellefsen A, et al. Autism in the Faroe Islands: diagnostic stability from childhood to early adult life. Sci World J. 2013;2013:592371. doi: 10.1155/2013/592371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wiggins LD, Baio J, Schieve L, Lee LC, Nicholas J, Rice CE. Retention of autism spectrum diagnoses by community professionals: findings from the autism and developmental disabilities monitoring network, 2000 and 2006. J Dev Behav Pediatr. 2012;33:387–395. doi: 10.1097/DBP.0b013e3182560b2f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Charman T. What does the term ‘working diagnosis’ mean? J Autism Dev Disord. 2005;35:539–540. doi: 10.1007/s10803-005-5068-1. [DOI] [PubMed] [Google Scholar]
- 6.Daniels AM, Rosenberg RE, Law JK, Lord C, Kaufmann WE, Law PA. Stability of initial autism spectrum disorder diagnoses in community settings. J Autism Dev Disord. 2011;41:110–121. doi: 10.1007/s10803-010-1031-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Moss J, Magiati I, Charman T, Howlin P. Stability of the autism diagnostic interview-revised from pre-school to elementary school age in children with autism spectrum disorders. J Autism Dev Disord. 2008;38:1081–1091. doi: 10.1007/s10803-007-0487-9. [DOI] [PubMed] [Google Scholar]
- 8.Fein D, Barton M, Eigsti IM, et al. Optimal outcome in individuals with a history of autism. J Child Psychol Psychiatry. 2013;54:195–205. doi: 10.1111/jcpp.12037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.McEachin JJ, Smith T, Lovaas OI. Long-term outcome for children with autism who received early intensive behavioral treatment. Am J Ment Retard. 1993;97:359–372. [PubMed] [Google Scholar]
- 10.Broderick AA. Autism, “recovery (to normalcy)”, and the politics of hope. Intellect Dev Disabil. 2009;47:263–281. doi: 10.1352/1934-9556-47.4.263. [DOI] [PubMed] [Google Scholar]
- 11.Fernell E, Hedvall Å, Norrelgen F, et al. Developmental profiles in preschool children with autism spectrum disorders referred for intervention. Res Dev Disabil. 2010;31:790–799. doi: 10.1016/j.ridd.2010.02.003. [DOI] [PubMed] [Google Scholar]
- 12.Fernell E, Hedvall Å, Westerlund J, et al. Early intervention in 208 Swedish preschoolers with autism spectrum disorder. A prospective naturalistic study. Res Dev Disabil. 2011;32:2092–2101. doi: 10.1016/j.ridd.2011.08.002. [DOI] [PubMed] [Google Scholar]
- 13.Eriksson MA, Westerlund J, Hedvall Å, Åmark P, Gillberg C, Fernell E. Medical conditions affect the outcome of early intervention in preschool children with autism spectrum disorders. Eur Child Adolesc Psychiatry. 2013;22:23–33. doi: 10.1007/s00787-012-0312-7. [DOI] [PubMed] [Google Scholar]
- 14.Höglund Carlsson L, Norrelgen F, Kjellmer L, Westerlund J, Gillberg C, Fernell E. Coexisting disorders and problems in preschool children with autism spectrum disorders. Sci World J. 2013;2013:213979. doi: 10.1155/2013/213979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Barnevik Olsson M, Höglund Carlsson L, Westerlund J, Gillberg C, Fernell E. Autism before diagnosis: crying, feeding and sleeping problems in the first two years of life. Acta Paediatr. 2013;102:635–639. doi: 10.1111/apa.12229. [DOI] [PubMed] [Google Scholar]
- 16.Hedvall Å, Westerlund J, Fernell E, Holm A, Gillberg C, Billstedt E. Autism and developmental profiles in preschoolers: stability and change over time. Acta Paediatr. 2013;103:174–181. doi: 10.1111/apa.12455. [DOI] [PubMed] [Google Scholar]
- 17.Wing L, Leekam SR, Libby SJ, Gould J, Larcombe M. The diagnostic interview for social and communication disorders: background, inter-rater reliability and clinical use. J Child Psychol Psychiatry. 2002;43:307–325. doi: 10.1111/1469-7610.00023. [DOI] [PubMed] [Google Scholar]
- 18.Krug DA, Arick J, Almond P. Behavior checklist for identifying severely handicapped individuals with high levels of autistic behavior. J Child Psychol Psychiatry. 1980;21:221–229. doi: 10.1111/j.1469-7610.1980.tb01797.x. [DOI] [PubMed] [Google Scholar]
- 19.Philippe A, Martinez M, Guilloud-Bataille M, et al. Genome-wide scan for autism susceptibility genes. Paris Autism Research International Sibpair Study. Hum Mol Genet. 1999;8:805–812. doi: 10.1093/hmg/8.5.805. [DOI] [PubMed] [Google Scholar]
- 20.Sparrow SS, Cicchetti DV, Balla DA. Vineland Adaptive Behavior Scales: Second Edition (Vineland™-II) Livonia, MN: Pearson Assessments; 2005. [Google Scholar]
- 21.American Psychiatric Association (APA) Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington, DC: American Psychiatric Association; 2000. DSM-IV-TR. [Google Scholar]
- 22.Hansson SL, Svanström Röjvall A, Råstam M, Gillberg C, Anckarsäter H. Psychiatric telephone interview with parents for screening of childhood autism-tics, AD/HD and other comorbidities (A-TAC): preliminary reliability and validity. Br J Psychiatry. 2005;187:262–267. doi: 10.1192/bjp.187.3.262. [DOI] [PubMed] [Google Scholar]
- 23.Larson T, Anckarsäter H, Gillberg IC, et al. The autism-tics, AD/HD and other comorbidities inventory (A-TAC): further validation of a telephone interview for epidemiological research. BMC Psychiatry. 2010;10:1. doi: 10.1186/1471-244X-10-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Larson T, Lundström S, Nilsson T, et al. Predictive properties of the A-TAC inventory when screening for childhood-onset neurodevelopmental problems in a population-based sample. BMC Psychiatry. 2013;13:233. doi: 10.1186/1471-244X-13-233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.St Pourcain B, Mandy WP, Heron J, Golding J, Davey Smith G, Skuse DH. Links between co-occurring social-communication and hyperactive-inattentive trait trajectories. J Am Acad Child Adolesc Psychiatry. 2011;50:892–902. doi: 10.1016/j.jaac.2011.05.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.van der Meer JM, Oerlemans AM, van Steijn DJ, et al. Are autism spectrum disorder and attention deficit/hyperactivity disorder different manifestations of one overarching disorder? Cognitive and symptom evidence from a clinical and population-based sample. J Am Acad Child Adolesc Psychiatry. 2012;51:1160–1172. doi: 10.1016/j.jaac.2012.08.024. [DOI] [PubMed] [Google Scholar]
- 27.Musser ED, Hawkey E, Kachan-Liu SS, et al. Shared familial transmission of autism spectrum and attention-deficit/hyperactivity disorders. J Child Psychol Psychiatry. 2014;55:819–827. doi: 10.1111/jcpp.12201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Goldin RL, Matson JL, Tureck K, Cervantes PE, Jang J. A comparison of tantrum behavior profiles in children with ASD, ADHD and comorbid ASD and ADHD. Res Dev Disabil. 2013;34:2669–2675. doi: 10.1016/j.ridd.2013.04.022. [DOI] [PubMed] [Google Scholar]
- 29.Gillberg C. The ESSENCE in child psychiatry: Early Symptomatic Syndromes Eliciting Neurodevelopmental Clinical Examinations. Res Dev Disabil. 2010;31:1543–1551. doi: 10.1016/j.ridd.2010.06.002. [DOI] [PubMed] [Google Scholar]