

Abstract
AIM: To investigate the pathological characteristics and carcinogenesis mechanism of benign lymphoadenosis of oral mucosa (BLOM).
METHODS: The expressions of Ki-67, CD34 and apoptosis were evaluated by immunohistochemical SP staining in 64 paraffin-embedded tissue samples. Of them, 9 were from BLOM with dysplasia, 15 from BLOM without dysplasia, 15 from oral squamous cell carcinoma (OSCC), 15 from oral precancerosis, and 10 from normal tissues. Cell proliferation, apoptosis and angiogenesis of tissue samples were also analyzed.
RESULTS: The expression of Ki-67 in BLOM with dysplasia, oral precancerosis and OSCC was significantly higher than in BLOM without dysplasia and normal mucosa. The microvascular density (MVD) in BLOM with and without dysplasia, oral precancerosis, and OSCC was significantly higher than in normal mucosa. Apoptosis in BLOM and oral precancerosis was significantly higher than in OSCC and normal mucosa.
CONCLUSION: Benign lymphoadenosis of oral mucosa has potentialities of cancerization.
Keywords: Benign lymphoadenosis of oral mucosa, Ki-67, Microvascular density, Apoptosis
INTRODUCTION
Benign lymphoadenosis of oral mucosa (BLOM), which could be commonly found clinically, usually occurs in the mucosae of lips, cheeks, tongue or gingiva. Sometimes, BLOM may develop in all of the oral mucosa and accompany other oral diseases. As far as we know, few reports have ever mentioned BLOM, and there has been no international definition about it. Most researchers considered it as a kind of reactive proliferation. Since 1970s, our department have been studying BLOM from the aspects of morphology and immunopathology. Ultrastructural changes of this disease is similar to that of leukoplakia[1,2]. Clinically, BLOM has a malignant trend[3,4]. At present, it is regarded as a kind of precancerous lesion[5]. To investigate the pathological characteristics and carcinogenesis mechanism of BLOM, we studied cell proliferation, cell apoptosis and angiogenesis of different types of oral mucosa diseases, including BLOM with dysplasia and without dysplasia, OSCC, oral precancerosis and normal tissues by immunohistochemistry method.
MATERIALS AND METHODS
Materials
A total of 64 paraffin-embedded tissue samples were from Pathological Research Laboratory, School of Stomatology, Peking University. Of them, 9 were from BLOM with dysplasia, 15 from BLOM without dysplasia, 15 from oral OSCC (8 in stage III, 7 in stage I or II), 15 from oral precancerosis, and 10 from normal tissues around the neoplasms. Streptavidin-biotin- immunoperoxidase system kit was purchased from Fuzhou Maixin Immunotech Corporation, China; mouse monoclonal antihuman Ki-67 antibody was provided by Beijing Immunotech Zhonghshan Corporation, China; and cell death detection kit was from Boehringer Mannheim, Germany.
Immunohistochemistry protocol for Ki-67 and CD34
Five micrometer thick sections were dewaxed with xylene, and rehydrated in graded ethanol. Endogenous peroxidase activity was blocked by immersion of slides in methanol with 0.03% hydrogen peroxide for 10 min. In order to retrieve antigenicity, these sections were then heated in a pressure cooker in 10 mmol/L citrate buffer (pH 6, 90 s after water boiled). After washing in distilled water, these sections were rinsed in phosphate-buffered saline (PBS) and incubated for 60 min at room temperature with CD34 or Ki-67 mAb. Reaction was visualized with a streptavidin-biotin-immunoperoxidase system using diaminobenzidine (DAB) as chromogen. All sections were then counterstained with hematoxylin.
Positive staining for CD34 or Ki-67 was regarded as positive control. For negative control, the primary antibodies were replaced with PBS. Staining was measured as the percentage of positively stained nuclei (Ki-67, labeling index, LI) or cytoplasm (CD34, microvascular density, MVD). Ki-67 reaction was scored at 400 magnification, a total of 1 000 epithelial cells (normal tissue and BLOM) or tumor cells (OSCC) were evaluated. Reactive nuclei were considered positive, regardless of staining intensity. The percentage of Ki-67 positive was then calculated and positivity of lymphocytes was not evaluated. Criteria for counting included individual or cluster of cells with or without lumen positivity for CD34 immunoreactivity. Areas of inflammation, necrosis, and fibrosis were excluded. For determination of mean MVD, sections were first observed under low power (200) for areas with dense vascularity. These were then counted in three different fields under high power (400). The average counts were recorded as MVD for each case.
TUNEL protocol for apoptosis evaluation
Detection of apoptosis in tissue was determined by TUNEL assay, employing in situ. The procedure is based on the detection of chromatin DNA strand breaks, the most characteristic biochemical feature of apoptosis caused by activation of endogenous nuclease activity.
Sections were dewaxed, rehydrated, and washed in distilled water for 10 min. The nuclei in tissue sections were stripped from proteins with 4% pepsin diluted in sterile buffer (10 mm Tris-HCl, pH 7.4) for 60 min at 37 °C, followed by quenching of endogenous peroxidase. The sections were rinsed in 50 μL of a label mixture containing the labeled nucleotide and enzyme, and incubated in a humidified chamber for 60 min at 37 °C. After washing with PBS, the sections were incubated for 30 min at 37 °C with alkaline phosphatase reagent. The substrate reaction was developed using diethyl chlorophosphite (DECP) and counterstained with nuclei fast red.
Positive staining for CD34 or Ki-67 was regarded as positive control. For negative control, the primary antibodies were replaced with PBS. A cell was considered apoptotic only when unequivocal nuclear labeling was observed in the areas with no inflammation. Cells exhibiting necrotic nuclear karyorrhexis as well as those in necrotic foci were excluded. TUNEL reactivity was always estimated in relation to characteristic histological criteria of apoptosis, including overall shrinkage, homogenously dark basophilic nuclei, presence of nuclear fragments, sharply delineated cell borders and homogenous eosinophilic cytoplasm. To evaluate the different rates of TUNEL reactivity in each sample, 1 000 cells were counted randomly under high power (400) and the percentage of positively stained nuclei (AI) was calculated.
Statistical analysis
The expression of Ki-67, MVD and extent of TUNEL reactive nuclei in different tissue samples was analyzed by t-test and χ2-test using SPSS10.0 for Windows. P<0.05 was considered significant.
RESULTS
The histological characteristics of BLOM is that lymphoid follicles or dense lymphocytes foci could be seen in the basal cell layer. The expression of Ki-67, which was stained brown in nuclei, could be found in normal tissues, BLOM, BLOM with dysplasia, precancerosis and OSCC. Positive cells distributed dispersedly in epithelium of normal tissues and BLOM without dysplasia (Figure 1A). Meanwhile, many cells appeared positive in lymphoid follicles. The expression of Ki-67 obviously increased in BLOM with dysplasia and in some samples Ki-67 positively stained nuclei were seen in all layers of epithelium (Figure 1B). The expression of Ki-67 also increased in precancerous tissues and OSCC, in the center of which positive cells distributed diffusely (Figure 1C). The positive rates of Ki-67 expression in different groups are shown in Table 1.
Figure 1.
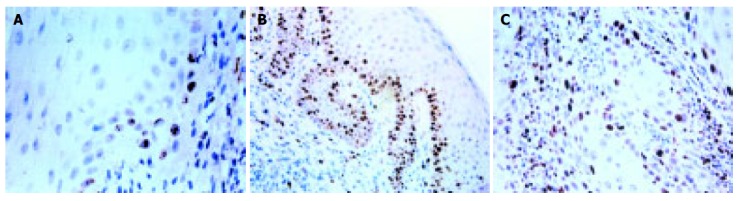
Ki-67 expression in A: BLOM without dysplasia (IHC ×400), B: BLOM with dysplasia (IHC ×200), and C: oral cancer (IHC ×200).
Table 1.
The positive rates of Ki-67 expression in different groups (mean±SD)
| Group | Ki-67 positive rate (%) |
| Normal | 14.19 ± 6.18 |
| BLOM | 22.29 ± 11.39 |
| BLOM with dysplasia | 45.42 ± 9.89a |
| Precancerosis | 47.15 ± 6.84ac |
| OSCC | 65.89 ± 9.09ace |
P<0.05 vs normal,
P<0.05 vs BLOM,
P<0.05 vs BLOM with dysplasia.
The expression of CD34 was positive in all samples, and distributed punctately, located in the cytoplasm of vascular endotheliocytes (Figure 2A). Only a few microvessels in the connective tissues of normal mucosa could be seen. But in BLOM, BLOM with dysplasia and precancerosis, their number increased obviously (Figure 2B). A great amount of microvessels also could be found in OSCC. MVD values in different groups are shown in Table 2.
Figure 2.
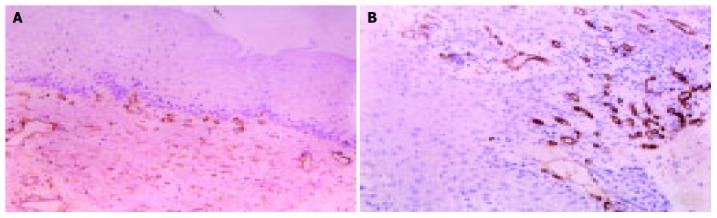
CD34 expression in A: BLOM without dysplasia (IHC ×100) and B: BLOM with dysplasia (IHC ×100).
Table 2.
MVD in different groups (mean±SD)
| Group | MVD value |
| Normal | 14.31 ± 2.71 |
| BLOM | 44.81 ± 10.20 |
| BLOM with dysplasia | 43.89 ± 8.78a |
| Precancerosis | 45.28 ± 11.09ac |
| OSCC | 62.73 ± 8.13ace |
P<0.05 vs normal,
P<0.05 vs BLOM,
P<0.05 vs BLOM with dysplasia.
Cell apoptosis was found in 2/10 normal tissues, 10/15 BLOM, 8/9 BLOM with dysplasia, 13/15 precancerosis and 8/15 OSCC. Apoptosis was seldom seen in the stromal layer of normal mucosa, but it increased obviously in BLOM, BLOM with dysplasia and precancerosis (Figure 3). At the same time, apoptosis could be found in connective tissues of BLOM, BLOM with dysplasia and precancerosis. The positive rate of apoptosis in OSCC was significantly lower than that in other groups except the normal mucosa.
Figure 3.
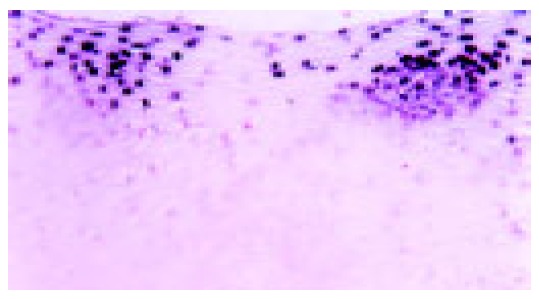
Apoptosis in BLOM with dysplasia (TUNEL ×200).
DISCUSSION
Ki-67 is an acknowledged marker that indicates the proliferation capacity of cells, and many studies demonstrated that it was overexpressed in oral premalignancy and oral cancer[6-9]. Tabor et al[10] studied 43 samples from patients who had undergone resection of their squamous cell carcinoma in oral cavity/oropharynx. With the consensus score, 12 samples were classified as normal, and 31 as dysplastic (21 mild, 6 moderate, and 4 severe). They found that there was a high coincidence between loss of heterozygosity (LOH) and the expression of Ki-67. The Ki-67 index in LOH-positive cases was significantly higher than that in LOH-negative cases. It was suggested that the expression of Ki-67 was correlated with other factors (beta-catenin, p53R2, etc)[11-14]. Other scholars found there was a significant correlation between Ki-67 LI, stroma/tumor proportion and the degree of keratinization[15,16]. In the present study, over-expression was found in the epithelium of BLOM with dysplasia, precancerosis and OSCC. But the expression in epithelium of BLOM without dysplasia was similar to that in the normal mucosa and there was an abundant expression in lymphoid follicles. This suggested that the epithelial cells of BLOM without dysplasia had not undergone genetic transformation, and the cells of germinal center had a strong proliferation capacity. In the connective tissues of BLOM and BLOM with dysplasia, a great amount of positive cells could be found in the center of lymphoid follicles. However, no obvious difference was revealed. This indicated that the center had a strong capacity of proliferation, but not a malignant trend, because the proliferation of lymphocytes was a kind of benign and reactive proliferation. Why we considered BLOM benign was also due to this reason. The number of Ki-67 positive cells and the staining in BLOM without dysplasia had no obvious difference from those in normal mucosa, indicating that epithelial cells did not appear abnormal. In the epithelium of BLOM with dysplasia and precancerosis, the number of positive cells obviously increased and the distribution of positive cells extended from the lower basal layer to the upper basal layer and prickle cell layer. In some samples, positive cells were distributed in all the layers of epithelium. This indicated that the proliferation capacity of basal cells was strengthened.
Angiogenesis is a process involved in the development of new blood vessels, by the division and migration of existing vasculature[17-20]. It is an important mechanism to sustain tumorigenic potential in neoplasm and in dysplastic lesions, indicating abundant capillaries leading to intense vascularization in cancer. Therefore, evaluation of angiogenesis may be of prognostic significance in the assessment of tumor progression. Iwasa et al[21] suggested that negative DNA instability lesions had a higher MVD in proliferating cell nuclear antigen (PCNA)-positive cells than positive DNA instability lesions. Other scholars proved that in non-small cell lung cancer and oral cancer, the mean AIs of the lower-MVD and the higher-MVD patients were significantly differen. Our study has confirmed that insufficient angiogenesis could accelerate apoptotic cell death. The angiogenesis in BLOM with and without dysplasia, and in precancerosis was significantly higher than in normal tissue, and new blood vessels were more abundant. Sauter et al[17] suggested that the angiogenesis in precancerosis was between oral normal tissue and OSCC.
Apoptosis is a programmed cell death under genetic control. A fine balance between the cell proliferation and cell death is very important to normal development and maintenance of tissue size and shape. In another word, the imbalance between the positive and negative regulation of cell growth could cause a series of diseases including neoplasm. In neoplasm, the disorder of homeostasis may result in the development of tumor[25-27]. Some studies showed that epidermal growth factor receptor blockade, cyclin dependent kinase inhibitor and 5-FU could induce cell apoptosis[28-30]. Other scholars also found that the overexpression of p27(Kip1) and retinoic acid receptor could induce growth arrest and apoptosis in an oral cancer cell line[31,32]. Results of the present study indicated that the apoptosis was significantly higher in BLOM, BLOM without dysplasia, and precancerosis than in normal tissue. However, it was lower in tumor tissue (OSCC). This suggested that the body tried to control the balance of cell number by increasing cell apoptosis with the increase in cell proliferation. However if the body fails, tumor develops. Similar result could be found in the study of Guan et al[33,34].
Previous studies also showed that BLOM should be regarded as a kind of precancerous lesion. In the present study, the cell proliferation, angiogenesis and apoptosis of BLOM were similar to that of precancerosis, and in BLOM without dysplasia the angiogenesis was significantly higher than that in normal oral tissue. But the expression of Ki-67 was similar to that in normal tissue. Therefore, the changes of cell proliferation, cell apoptosis, and angiogenesis in connective tissue were earlier than in epithelium; BLOM had the potential of carcinogenesis. Many factors may induce the proliferation of cancer cells, enhance their survival by escape of apoptosis, and provide abundant nutrients during early-stage carcinogenesis of oral precancerous lesions. Comparison of gene expression profiles between head and neck squamous cell carcinoma and normal tissues showed that altered expression levels of genes were involved in the control of cell growth and differentiation, angiogenesis, apoptosis, cell cycle, and signaling, most of which had not been previously described in head and neck squamous cell carcinoma[35]. Which factor contributes to cell proliferation, and inhibits cell apoptosis during the carcinogenesis of BLOM is still a subject to be investigated in future.
Footnotes
Science Editor Zhu LH Language Editor Elsevier HK
References
- 1.Sun KH, Wu QG, Zheng LF. Clinicopathological analysis of 70 cases of benign lymphoadenosis of oral mucosa. Zhonghua Kouqiang Yixue Zazhi. 1986;21:137–139. [PubMed] [Google Scholar]
- 2.Sun KH, Yu SF, Wu QG, Zheng LF, Wei MJ. Ultrastructural and immunopathological study of benign lymphoadenosis of oral mucosa. Zhonghua Kouqiang Yixue Zazhi. 1992;27:104–106. [PubMed] [Google Scholar]
- 3.Harsany DL, Ross J, Fee WE. Follicular lymphoid hyperplasia of the hard palate simulating lymphoma. Otolaryngol Head Neck Surg. 1980;88:349–356. doi: 10.1177/019459988008800406. [DOI] [PubMed] [Google Scholar]
- 4.Wright JM, Dunsworth AR. Follicular lymphoid hyperplasia of the hard palate: a benign lymphoproliferative process. Oral Surg Oral Med Oral Pathol. 1983;55:162–168. doi: 10.1016/0030-4220(83)90172-x. [DOI] [PubMed] [Google Scholar]
- 5.Yu SF. Kouqiang Zuzhi Binglixue(5th edition) Beijing: People抯 health publishing house; 2003. pp. 203–204. [Google Scholar]
- 6.Carlos de Vicente J, Herrero-Zapatero A, Fresno MF, López-Arranz JS. Expression of cyclin D1 and Ki-67 in squamous cell carcinoma of the oral cavity: clinicopathological and prognostic significance. Oral Oncol. 2002;38:301–308. doi: 10.1016/s1368-8375(01)00060-4. [DOI] [PubMed] [Google Scholar]
- 7.Farrar M, Sandison A, Peston D, Gailani M. Immunocytochemical analysis of AE1/AE3, CK 14, Ki-67 and p53 expression in benign, premalignant and malignant oral tissue to establish putative markers for progression of oral carcinoma. Br J Biomed Sci. 2004;61:117–124. doi: 10.1080/09674845.2004.11732655. [DOI] [PubMed] [Google Scholar]
- 8.Alves FA, Pires FR, De Almeida OP, Lopes MA, Kowalski LP. PCNA, Ki-67 and p53 expressions in submandibular salivary gland tumours. Int J Oral Maxillofac Surg. 2004;33:593–597. doi: 10.1016/j.ijom.2004.01.010. [DOI] [PubMed] [Google Scholar]
- 9.Hafian H, Venteo L, Sukhanova A, Nabiev I, Lefevre B, Pluot M. Immunohistochemical study of DNA topoisomerase I, DNA topoisomerase II alpha, p53, and Ki-67 in oral preneoplastic lesions and oral squamous cell carcinomas. Hum Pathol. 2004;35:745–751. doi: 10.1016/j.humpath.2004.02.004. [DOI] [PubMed] [Google Scholar]
- 10.Tabor MP, Braakhuis BJ, van der Wal JE, van Diest PJ, Leemans CR, Brakenhoff RH, Kummer JA. Comparative molecular and histological grading of epithelial dysplasia of the oral cavity and the oropharynx. J Pathol. 2003;199:354–360. doi: 10.1002/path.1285. [DOI] [PubMed] [Google Scholar]
- 11.Sato K, Okazaki Y, Tonogi M, Tanaka Y, Yamane GY. Expression of beta-catenin in rat oral epithelial dysplasia induced by 4-nitroquinoline 1-oxide. Oral Oncol. 2002;38:772–778. doi: 10.1016/s1368-8375(02)00044-1. [DOI] [PubMed] [Google Scholar]
- 12.Yanamoto S, Kawasaki G, Yoshitomi I, Mizuno A. Expression of p53R2, newly p53 target in oral normal epithelium, epithelial dysplasia and squamous cell carcinoma. Cancer Lett. 2003;190:233–243. doi: 10.1016/s0304-3835(02)00588-8. [DOI] [PubMed] [Google Scholar]
- 13.Xie X, Clausen OP, Boysen M. Bag-1 expression as a prognostic factor in tongue squamous cell carcinomas. Laryngoscope. 2004;114:1785–1790. doi: 10.1097/00005537-200410000-00021. [DOI] [PubMed] [Google Scholar]
- 14.Bowen SL, Bloor BK, Leigh IM, Waseem A. Adducin expression in cutaneous and oral lesions: alpha- and beta-adducin transcripts down-regulate with keratinocyte differentiation in stratified epithelia. J Pathol. 2003;201:119–126. doi: 10.1002/path.1389. [DOI] [PubMed] [Google Scholar]
- 15.Bettendorf O, Herrmann G. Prognostic relevance of Ki-67 antigen expression in 329 cases of oral squamous cell carcinoma. ORL J Otorhinolaryngol Relat Spec. 2002;64:200–205. doi: 10.1159/000058025. [DOI] [PubMed] [Google Scholar]
- 16.Kurokawa H, Matsumoto S, Murata T, Yamashita Y, Tomoyose T, Zhang M, Fukuyama H, Takahashi T. Immunohistochemical study of syndecan-1 down-regulation and the expression of p53 protein or Ki-67 antigen in oral leukoplakia with or without epithelial dysplasia. J Oral Pathol Med. 2003;32:513–521. doi: 10.1034/j.1600-0714.2003.00117.x. [DOI] [PubMed] [Google Scholar]
- 17.Sauter ER, Nesbit M, Watson JC, Klein-Szanto A, Litwin S, Herlyn M. Vascular endothelial growth factor is a marker of tumor invasion and metastasis in squamous cell carcinomas of the head and neck. Clin Cancer Res. 1999;5:775–782. [PubMed] [Google Scholar]
- 18.Chimenos-Küstner E, Font-Costa I, López-López J. Oral cancer risk and molecular markers. Med Oral Patol Oral Cir Bucal. 2004;9:381–384; 381-384;. [PubMed] [Google Scholar]
- 19.Shieh YS, Lee HS, Shiah SG, Chu YW, Wu CW, Chang LC. Role of angiogenic and non-angiogenic mechanisms in oral squamous cell carcinoma: correlation with histologic differentiation and tumor progression. J Oral Pathol Med. 2004;33:601–606. doi: 10.1111/j.1600-0714.2004.00252.x. [DOI] [PubMed] [Google Scholar]
- 20.Sotiriou C, Lothaire P, Dequanter D, Cardoso F, Awada A. Molecular profiling of head and neck tumors. Curr Opin Oncol. 2004;16:211–214. doi: 10.1097/00001622-200405000-00003. [DOI] [PubMed] [Google Scholar]
- 21.Iwasa M, Imamura Y, Noriki S, Nishi Y, Kato H, Fukuda M. Immunohistochemical detection of early-stage carcinogenesis of oral leukoplakia by increased DNA-instability and various malignancy markers. Eur J Histochem. 2001;45:333–346. doi: 10.4081/1642. [DOI] [PubMed] [Google Scholar]
- 22.Tanaka F, Otake Y, Yanagihara K, Kawano Y, Miyahara R, Li M, Ishikawa S, Wada H. Correlation between apoptotic index and angiogenesis in non-small cell lung cancer: comparison between CD105 and CD34 as a marker of angiogenesis. Lung Cancer. 2003;39:289–296. doi: 10.1016/s0169-5002(02)00534-2. [DOI] [PubMed] [Google Scholar]
- 23.Hannen EJ, Riediger D. The quantification of angiogenesis in relation to metastasis in oral cancer: a review. Int J Oral Maxillofac Surg. 2004;33:2–7. doi: 10.1054/ijom.2003.0433. [DOI] [PubMed] [Google Scholar]
- 24.Lim JJ, Kang S, Lee MR, Pai HK, Yoon HJ, Lee JI, Hong SP, Lim CY. Expression of vascular endothelial growth factor in salivary gland carcinomas and its relation to p53, Ki-67 and prognosis. J Oral Pathol Med. 2003;32:552–561. [PubMed] [Google Scholar]
- 25.Birchall M, Winterford C, Tripconi L, Gobé G, Harmon B. Apoptosis and mitosis in oral and oropharyngeal epithelia: evidence for a topographical switch in premalignant lesions. Cell Prolif. 1996;29:447–456. doi: 10.1111/j.1365-2184.1996.tb00987.x. [DOI] [PubMed] [Google Scholar]
- 26.Grabenbauer GG, Suckorada O, Niedobitek G, Rodel F, Iro H, Sauer R, Rodel C, Schultze-Mosgau S, Distel L. Imbalance between proliferation and apoptosis may be responsible for treatment failure after postoperative radiotherapy in squamous cell carcinoma of the oropharynx. Oral Oncol. 2003;39:459–469. doi: 10.1016/s1368-8375(03)00005-8. [DOI] [PubMed] [Google Scholar]
- 27.Chrysomali E, Nikitakis NG, Tosios K, Sauk JJ, Papanicolaou SI. Immunohistochemical evaluation of cell proliferation antigen Ki-67 and apoptosis-related proteins Bcl-2 and caspase-3 in oral granular cell tumor. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96:566–572. doi: 10.1016/s1079-2104(03)00371-8. [DOI] [PubMed] [Google Scholar]
- 28.Holsinger FC, Doan DD, Jasser SA, Swan EA, Greenberg JS, Schiff BA, Bekele BN, Younes MN, Bucana CD, Fidler IJ, et al. Epidermal growth factor receptor blockade potentiates apoptosis mediated by Paclitaxel and leads to prolonged survival in a murine model of oral cancer. Clin Cancer Res. 2003;9:3183–3189. [PubMed] [Google Scholar]
- 29.Mihara M, Shintani S, Nakashiro K, Hamakawa H. Flavopiridol, a cyclin dependent kinase (CDK) inhibitor, induces apoptosis by regulating Bcl-x in oral cancer cells. Oral Oncol. 2003;39:49–55. doi: 10.1016/s1368-8375(02)00019-2. [DOI] [PubMed] [Google Scholar]
- 30.Ohtani T, Hatori M, Ito H, Takizawa K, Kamijo R, Nagumo M. Involvement of caspases in 5-FU induced apoptosis in an oral cancer cell line. Anticancer Res. 2000;20:3117–3121. [PubMed] [Google Scholar]
- 31.Supriatno K, Hoque MO, Bando T, Yoshida H, Sato M. Overexpression of p27(Kip1) induces growth arrest and apoptosis in an oral cancer cell line. Oral Oncol. 2002;38:730–736. doi: 10.1016/s1368-8375(02)00011-8. [DOI] [PubMed] [Google Scholar]
- 32.Hayashi K, Yokozaki H, Naka K, Yasui W, Lotan R, Tahara E. Overexpression of retinoic acid receptor beta induces growth arrest and apoptosis in oral cancer cell lines. Jpn J Cancer Res. 2001;92:42–50. doi: 10.1111/j.1349-7006.2001.tb01046.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Guan WQ, Yu SF, Gao Y. Expression of bcl-2, p53 protein in oral leukoplakia and squamous cell carcinoma. Linchuang Yu Shiyan Binglixue Zazhi. 1999;4:123–125. [Google Scholar]
- 34.Nikitakis NG, Sauk JJ, Papanicolaou SI. The role of apoptosis in oral disease: mechanisms; aberrations in neoplastic, autoimmune, infectious, hematologic, and developmental diseases; and therapeutic opportunities. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;97:476–490. doi: 10.1016/j.tripleo.2003.12.032. [DOI] [PubMed] [Google Scholar]
- 35.Lin DT, Subbaramaiah K, Shah JP, Dannenberg AJ, Boyle JO. Cyclooxygenase-2: a novel molecular target for the prevention and treatment of head and neck cancer. Head Neck. 2002;24:792–799. doi: 10.1002/hed.10108. [DOI] [PubMed] [Google Scholar]