

Abstract
Introduction For infants under 6 months, the literature recommends 1,000-Hz tympanometry, which has a greater sensitivity for the correct identification of middle ear disorders in this population.
Objective To systematically analyze national and international publications found in electronic databases that used tympanometry with 226-Hz and 1,000-Hz probe tones.
Data Synthesis Initially, we identified 36 articles in the SciELO database, 11 in the Latin American and Caribbean Literature on the Health Sciences (LILACS) database, 199 in MEDLINE, 0 in the Cochrane database, 16 in ISI Web of Knowledge, and 185 in the Scopus database. We excluded 433 articles because they did not fit the selection criteria, leaving 14 publications that were analyzed in their entirety.
Conclusions The 1,000-Hz tone test has greater sensitivity and specificity for the correct identification of tympanometric curve changes. However, it is necessary to clarify the doubts that still exist regarding the use of this test frequency. Improved methods for rating curves, standardization of normality criteria, and the types of curves found in infants should be addressed.
Keywords: speech language and hearing sciences, hearing, acoustic impedance tests, otitis media with effusion, spontaneous otoacoustic emissions
Introduction
Tympanometry is effective in the early identification of changes in the external ear (EE) and middle ear (ME), and its use is well established for children and adults. However, its use for newborns and infants is still controversial. The literature recommends 1,000-Hz tympanometry for infants under 6 months, which has a greater sensitivity for the correct identification of ME dysfunction in this population.1 2
Literature Review
ME alterations have a high incidence in children. The presence of otitis media with effusion, cerumen, vernix, or other causes of conductive hearing loss contribute to a large number of false-positive results in neonatal hearing screening and may also delay the completion of diagnostic audiology. Therefore, it is important to identify hearing screening failures caused by transient changes in the ME and EE through an instrument that allows quick, accurate, and noninvasive assessment.1 2
One of the assessment tools used in routine audiology of the ME is the measurement of acoustic impedance, which is a general term related to the transfer of acoustic energy, either by facilitation (admittance) of or opposition (impedance) to the passage of sound energy. This is influenced by the amount of sound energy that is absorbed and reflected by the tympanic membrane (TM). When it is more compliant, the TM absorbs more energy and therefore allows greater admittance of the system. On the other hand, the more rigid the TM, the more energy will be reflected, creating greater system impedance.3 4
Tympanometry is a measure of the variation of the acoustic impedance of the tympanic ossicular system caused by pressure variations introduced into the external auditory canal and indicates the condition of the ME and auditory pathways.4 In audiology, the most commonly used probe tone has a low frequency of 226 Hz; however, more modern equipment includes additional probe tones such as 660, 678, and 1,000 Hz.
Tympanometry is a common practice in children and adults, and its specifications are very well established. However, there are many uncertainties regarding the specificity and sensitivity of the probe tones used in the evaluation of neonates and infants. The literature has shown that in neonates and infants, tympanograms obtained with a low-frequency probe tone can be recorded as normal, even in the presence of altered ME function.2 3 4 5 6 High-frequency probe tones, in particular 1,000 Hz, have a higher sensitivity for the identification of ME changes and therefore should be used in neonates and infants under 6 or 7 months of age if possible.2 4 5 6 7 8
The objectives of this study were to systematically analyze national and international scientific publications on the application of tympanometry in infants using 226-Hz and 1,000-Hz test tones and to compare sensitivity and specificity between these two test tones.
To investigate the number of publications on this topic, two researchers independently conducted a bibliographic survey in the SciELO, Latin American and Caribbean Literature on the Health Sciences (LILACS), MEDLINE, Cochrane, Scopus, and ISI Web of Knowledge electronic databases. For the search strategy, the Descriptors in Health Sciences (MeSH, created by the National Library of Medicine) term acoustic impedance tests was combined with the words neonate and infant. National and international articles published in the past 10 years were examined, delimiting the period between January 2001 and December 2011.
The inclusion criteria for the full analysis of texts were as follows: original article or case report; infants up to 7 months old as the research subjects; use of 1,000-Hz probe tone as tone test during tympanometry; description of tympanometric curves obtained; and published in Portuguese, English, or Spanish.
The articles that met the inclusion criteria were selected for review in full, analyzed, and organized in a database with the following parameters: author(s), title, source, year, research type, sample characteristics, test tones used, main findings, and classification of tympanometric curves.
Discussion
Initially, 447 articles were identified. Thirty-six articles were found in the SciELO database, 11 in the LILACS database, 199 in MEDLINE, 0 in the Cochrane database, 16 in ISI Web of Knowledge, and 185 in the Scopus database. We excluded 433 publications because they did not fit the selection criteria, leaving 14 publications that were analyzed in their entirety. The route taken for selection and analysis of text is shown in Fig. 1.
Fig. 1.
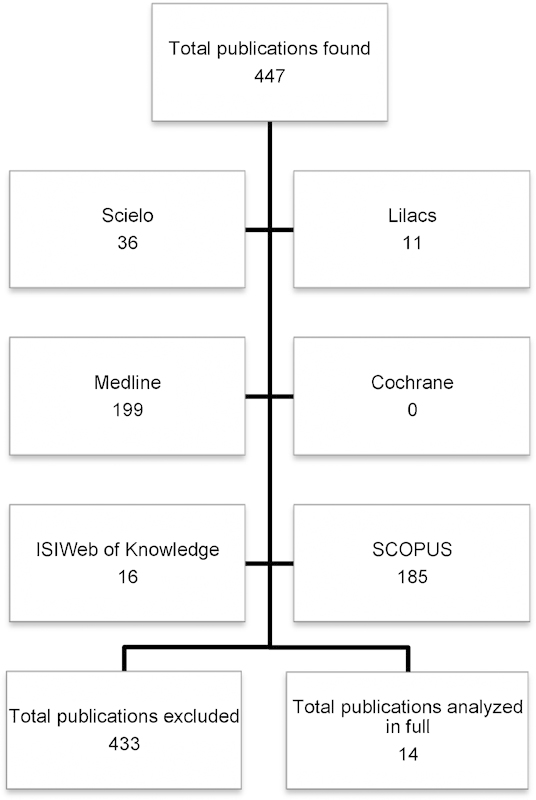
Route taken for selection and analysis of text.
The 14 selected publications were analyzed considering the source and year of publication. It was found that in the 10-year period investigated (2001 to 2011), the number of studies performed on tympanometry with high-frequency probe tones was not significant, but the number of publications increased from the year 2006 (Table 1).
Table 1. List of studies on tympanometry with high- and low-frequency probe tones from 2001 to 2011.
| Author | Title | Source | Year |
|---|---|---|---|
| Kei et al1 | High-frequency (1,000 Hz) tympanometry in normal neonates | J Am Acad Audiol | 2003 |
| Margolis et al2 | Tympanometry in newborn infants, 1-kHz norms | J Am Acad Audiol | 2003 |
| Baldwin7 | Choice of probe tone and classification of trace patterns in tympanometry undertaken in early infancy | Int J Audiol | 2006 |
| Calandruccio et al31 | Normative multifrequency tympanometry in infants and toddlers | J Am Acad Audiol | 2006 |
| Swanepoel et al29 | Infant hearing screening at immunization clinics in South Africa | Int J Pediatr Otorhinolaryngol | 2006 |
| Alaerts et al15 | Evaluation of middle ear function in young children: clinical guidelines for the use of 226- and 1,000-Hz tympanometry | Otol Neurotol | 2007 |
| Silva et al27 | Tympanometry in neonates with normal otoacoustic emissions: measurements and interpretation | Rev Bras Otorrinolaringol | 2007 |
| Swanepoel et al8 | High-frequency immittance for neonates: a normative study | Acta Otolaryngol | 2007 |
| Shahnaz et al6 | Multifrequency tympanometry in neonatal intensive care unit and well babies | J Am Acad Audiol | 2008 |
| Garcia et al22 | Acoustic immittance measures in infants with 226- and 1,000-Hz probes: correlation with otoacoustic emissions and otoscopy examination | Rev Bras Otorrinolaringol (Engl Ed) | 2009 |
| Zhiqi et al25 | Tympanometry in infants with middle ear effusion having been identified using spiral computerized tomography | Am J Otolaryngology | 2010 |
| Camboim et al23 | Comparative analysis of otoacoustic emissions with tympanometry in 0- to 6-mo infants | Revista CEFAC | 2012 |
| Tazinazzio et al24 | Otoacoustic emissions and acoustic immittance measurements using 226-Hz and 1,000-Hz probe tones in neonates | Revista CEFAC | 2011 |
| Lewis et al30 | A comparison of tympanometry with 226-Hz and 1,000-Hz probe tones in children with Down syndrome | Int J Pediatr Otorhinolaryngol | 2011 |
A thorough analysis of the publications was performed considering the characteristics of the sample, the test tone frequencies used in tympanometry, the main findings identified, and the classification of tympanometric curves (Table 2). This information is presented and discussed hereafter, with the assistance of other theoretical publications considered relevant for the purpose of better understanding the topic in question.
Table 2. Main characteristics of studies with test tones of 226- and 1,000-Hz.
| Author | Sample characteristics | Probe tones | Main findingsa | Classification of curves |
|---|---|---|---|---|
| Kei et al1 | 122 neonates, aged 1–6 d with OAEs present | 226 Hz; 1,000 Hz | 1,000 Hz: type 1, 225 ears; type 2, 14 ears; type 3, 3 ears; other atypical forms, 2 ears. 226 Hz: single peak, 115 ears; DP, 116 ears; multiple peak, 9 ears; invalid curves, 3 ears. |
1,000 Hz: type 1 (A), normal; types 2 and 3 (B, DP), altered 226 Hz, single peak: normal; DP, altered |
| Margolis et al2 | 65 infants, average age of 3.9 wk | 1,000 Hz | Single peak curves found in the majority of infants. Authors did not state the number of curves encountered. | Single peak: normal |
| Baldwin7 | 104 children between 2 and 19 wk with normal hearing and 107 infants aged 2–21 wk with temporary conductive hearing loss | 226 Hz; 678 Hz; 1,000 Hz | Infants with abnormal ME and normal tympanograms (type A): 94.9% with 226 Hz, 1.3% with 678 Hz, and 0% with 1,000 Hz. | Positive peak: normal Flat, descending negative peak, or undetermined: altered |
| Calandruccio et al31 | 33 children between 4 wk and 2 y and 33 adults with a mean age of 30.3 y | 226 Hz; 630 Hz; 1,000 Hz | 226 Hz: higher proportion of type 1B1G; 23.1% type 3B1G in children aged 4–10 wk and 6.8% in children aged 11–19 wk. 1,000 Hz: children showed greater variability of types, with 1B1G and 3B1G having equal distribution. |
Type 1B1G, 3B1G, 3B3G, and 5B3G tympanograms (Vanhuyse et al21) |
| Swanepoel et al29 | 510 infants, aged 0–12 mo | 226 Hz; 1,000 Hz | 87% of tympanograms displayed a peak, DP type curves present in 4.5% of cases. | Tympanogram with peak: ME normal DP type curve: ME altered |
| Alaerts et al15 | 110 infants up to 9 mo and 15 adults between 17 and 27 y with normal hearing | 226 Hz; 1,000 Hz | 226 Hz: number of cases of type A increased with increasing age; number of cases of type D decreased with increasing age. 1,000 Hz: number of cases of type D increased with increasing age. |
Types A and D: normal Types B, C, and Du: altered Types 1 and 4u: normal Types 2, 3, and 4u: altered |
| Silva et al27 | 110 neonates between 6 and 30 d with TEOAEs present | 226 Hz; 678 Hz; 1,000 Hz | 226 Hz: 47.7% single peak; 52.3% DP. 678 Hz: 25.4% single peak; 67.3% ASS; 7.3% I. 1,000 Hz: 70.9% single peak; 28.2% ASS; 0.9% I. |
Single peak and DP: normal ASS and I: normal or altered |
| Swanepoel et al8 | 143 infants between 0 and 4 wk of age | 1,000 Hz | 8% of tympanograms showed no peak. 6% were DP-type curves. 57% sensibility. 95% specificity. |
Tympanogram with peak: ME normal DP-type curve: ME altered |
| Shahnaz et al6 | 33 neonates from ICU and 16 healthy infants between 21 and 28 d; 42 infants between 6 d and 23 wk and 33 preterm neonates between 32 and 51 wk with BAEPs present compared with 16 adults between 18 and 32 y with normal hearing | 226 Hz; 1,000 Hz | Newborns and infants showed a great variability of complex tympanometric patterns with 226 Hz. With increasing test frequency, the ratio of single peak curves increased and with 1,000 Hz the rate was 64%. | Model: Vanhuyse et al21
226 Hz: 13% 1B1G and 85% complex multiple peak tympanograms 1,000 Hz: predominantly 3B1G (50%) and 1B1G (38%) |
| Garcia et al22 | 60 infants between 0 and 4 mo in the absence and presence of OAEs | 226 Hz; 1,000 Hz | OAEs present: 226 Hz: 61% A; 27% D; 8.3% B; 3.7% C. 1,000 Hz: 60% A; 11.6% D; 13.4% I; 5% B; 10% C. OAEs absent: 226 Hz: 53.3% A; 31.7% D; 13.3% B; 1.7% C. 1,000 Hz: 20% A; 2% D; 0% I; 70% B; 8% C. |
Types A, D, and I: normal Types B and C: altered Type ASS: normal or altered |
| Zhiqi et al25 | 52 infants between 42 d and 6 mo | 226 Hz; 1,000 Hz | 226 Hz: Group with normal ME: 51.06% single peak; 44.68% DP; 2.13% flat; 2.13% with negative pressure. Group with ME effusion: 77.19% single peak; 19.30% DP; 3.51% flat. 1,000 Hz: Group with normal ME: 97.87% single peak. Group with ME effusion: 98.25% flat. |
Single peak: normal tympanogram Flat: altered (ME effusion) |
| Tazinazzio et al24 | 52 infants between 11 and 51 d with OAEs present and absent; at 1,000 Hz, the number of ears was less because blocked curves were excluded (occurrence of the occlusion effect) | 226 Hz; 1,000 Hz | OAEs present and normal curves: 226 Hz, 82 ears; 1,000 Hz, 66 ears. OAEs present and altered curves: 226 Hz, 0 ears; 1,000 Hz, 6 ears. OAEs absent and normal curves: 226 Hz, 19 ears; 1,000 Hz, 8 ears. OAEs absent and altered curves: 226 Hz, 3 ears; 1,000 Hz, 13 ears. |
Types A and D: normal Types As, B, and flat: altered |
| Lewis et al30 | 26 children with Down syndrome between 6 and 18 mo | 226 Hz; 1,000 Hz | 226 Hz: ME no fluid: type B, 7 ears; type A, 17 ears. ME with fluid: type A, 0 ears; type B, 2 ears. 1,000 Hz: ME no fluid: type A, 24 ears; type B, 0 ears. ME with fluid: type B, 2 ears; type A, 0 ears. |
Type A: normal Type B: altered |
| Camboim et al23 | 118 infants between 0 and 6 mo with OAEs present and absent | 226 Hz; 1,000 Hz | 1,000 Hz: high correlation between normal curves (type A and DP) and presence of OAEs, as well as altered curves (not type A or DP) and absence of OAEs. | Types A and DP: normal Types C, Ad, As, and B: altered |
Abbreviations: BAEPs, brainstem auditory evoked potentials; ICU, intensive care unit; ME, middle ear; OAEs, evoked otoacoustic emissions; TEOAEs, transient evoked otoacoustic emissions.
Information taken from the Results section of publications.
Test Frequency and Age
In neonates and infants, growth entails changes in the ear that generate mechanical alterations, which can influence tympanogram recordings. These changes include increased EE, mastoid, and ME cavity; mass reduction of the ME due to changes in bone density; and bone formation in the wall of the external auditory canal.4 In addition, the resonance of the ME is modified according to age; the resonance frequency of the ME is lower in babies when compared with the values of an adult.9 Sagging of the ear canal can also cause movement of the wall of the ear canal.10 11
In the literature, there are notable divergences in the age at which the high-frequency probe test is recommended. There are indications for its use in children under 7 months of age,2 4 5 6 7 8 less than 6 months old,12 13 less than 4 months old,14 and under 5 months of age.7 Other authors claim that for use of 1,000-Hz test tones in infants up to 3 months old and between 3 and 9 months of age, ME evaluation must be performed in two stages. Initially, the 1,000-Hz test tone should be used and in cases of failure with this tone, testing should then be performed with a 226-Hz probe tone. The use of a low test frequency of 226 Hz has also been indicated for the assessment of infants over 9 months.15
Classification of Tympanometric Curves
According to the literature, tympanometric curves are usually classified as follows: type A (normal curve having a single peak of admittance between −150 and 100 daPa and a volume of 0.2 to 1.8 mL); flat or type B (flat curve with no admittance peak); type C (admittance peak shifted to negative pressures); As (curve with low admittance); Ad (interval between the two branches of the curve equal to or greater than 100 daPa)16; DP (double peak curve)17; ASS (asymmetrical curve with peak at high positive pressure); and I (inverted curve with an inverted configuration compared with the normal curve).18 However, there are also other less common types of tympanometric curves.19 20 21
Among the studies analyzed in the current review, it was observed that there was a consensus that the type A curve indicated a normal ME,1 15 17 18 19 and B, C, As, and Ad curves implied an altered ME.15 22 23 24 25
Regarding the DP curve, also called a type D curve, five studies showed that this curve indicates normality of the ME in the case of neonates.15 22 23 24 26 According to one author,3 this type of tympanogram is most often identified in the neonate population when tympanometry testing is performed with a 226-Hz probe tone. This is because such registration occurs when measurement is performed at the resonant frequency of the ME and in the case of this population, this frequency is shifted to lower values.
Regarding the I and ASS curves, it was found that there are disagreements with regards to their normal standards and which parameters should be used for classification of a normal or altered curve. The ASS curve and the I curve can be identified in subjects with and without alteration of the ME and can be regarded as normal or altered.22 27 One publication stated that the I curve should be classified as normal in infants.22
Besides the ambiguity that exists in the classification of curves with a 1,000-Hz probe tone, another issue regarding high-frequency tympanometry in neonates is the high number of unclassified or indeterminate curves obtained by the use of classification systems designated for the low-frequency tone test in adults and older children.7 This has created more doubt and questions regarding curve classification and the parameters that define categorization as normal or abnormal.
In a study using 1,000-Hz testing, the authors classified curves as follows: type 1 (similar to type A), type 2 (similar to type B), type 3 (similar to DP), and atypical forms. With a 226-Hz tone test, in addition to using the classification of DP, the authors also used the nomenclature single-peak tympanogram, multiple-peak tympanogram, and invalid tympanogram. From this perspective, the authors concluded that there is no direct correspondence between ME condition and tympanometry curve type. However, the type 1 curve, which was obtained in 92.3% of neonates, indicated an ME without alterations.1
It has been hypothesized that changes in the patterns of tympanometry may also vary according to the age of the individuals assessed. In one study using a 226-Hz probe tone, the percentage of type A curves increased with increasing age, and the percentage of DP curves decreased.15 Furthermore, the use of the 1,000-Hz tone decreased the prevalence of flat tympanograms and increased DP curves in a group of children. However, it should be mentioned that the sample surveyed included no children with ME alterations.
Changes in the quantitative values of tympanometry can be justified by the rapid anatomical growth of the ear in neonates during the first 6 weeks of life.28 An increase in resonance frequency occurs in the ear of neonates, and this shifts the type of tympanometric curve from DP to single peak. This alteration can be explained by anatomical evidence showing that the physical structure of the ear changes from a state allowing positive reactance (dominated by mass) to one allowing negative reactance (dominated by stiffness). When the ME reaches negative reactance, the low-frequency tone test becomes an appropriate tool to evaluate the peripheral auditory system. That is, with the evaluation of ear reactance, it is possible to identify the resonance frequency, and if this is low, the use of a high-frequency tone is sufficiently sensitive. However, if this frequency approaches the frequency of the adult, the conventional 226-Hz tone should be used. Such changes in resonance frequency may be due to intrasubject variability or true evolution of ME function with age.26
Relationship between Tympanometry and Other Audiological Evaluations
Other procedures used to identify hearing loss in infants include measurement of otoacoustic emissions (OAEs) and brainstem auditory evoked potentials. It is possible to correlate the results of these procedures and tympanometry traces to better assess hearing condition.
The literature indicates that the 1,000-Hz probe tone has a higher correlation with the responses of transient otoacoustic emissions (TOAEs) and distortion product otoacoustic emissions.23 24 29 The 1,000-Hz tone displays this correlation in both the evaluation of normal ears and ears with ME alterations. Tympanometry with a 226-Hz tone provides results consistent with assessment of OAEs in the presence of a normal ME only.23
For infants with TOAEs present, both probe tones have good specificity but, for infants with TOAEs absent, the 1,000-Hz tone is more sensitive for the identification of possible alterations in the ME.22 From this perspective, the use of tympanometry with a 1,000-Hz tone in infants is the most appropriate procedure for detecting changes in the ME, especially when TOAEs are absent.24
On the other hand, different tympanometry curve types can be identified even in the presence of different OAE recordings. The reason for the detection of heterogeneous curves even with the presence of OAEs, which suggest normal ME function, is unclear. It may be due to the fact that light dysfunction of the ME is not able to prevent OAE recording or may even be caused by inadequate sealing of the probe, resulting in movement-generated artifacts.1
The relationship between responses to 226- and 1,000-Hz probe tones and OAE recordings was also analyzed in a study of children with Down syndrome, showing a strong correlation between 1,000-Hz tympanometry and OAE results.30
Test Frequency Most Suitable for Evaluation of Infants
Despite the fact that it has been used for decades, the 226-Hz tone test is not the most appropriate for assessing infants,1 2 5 6 7 8 22 23 24 27 mainly because, as already mentioned, this population has maturational characteristics that are distinct from children older than 6 months of age and adults.
Among the sources analyzed, were identified three studies that used testing tones of 678 and 630 Hz in addition to 226 and 1,000 Hz. In all three studies, the authors observed that the 1,000-Hz tone test showed better results for the characterization of tympanograms when compared with other frequencies.7 27 31
Studies have shown that the efficacy of the 1,000-Hz tone in relation to the 226-Hz and 678-Hz probe tones is justified by the fact that mass components are larger at high-frequency probe tones and lower at low-frequency probe tones, which modifies the resonance characteristics of the ME.1 2 Changes in the wall of the external auditory canal, ME mobility, and tympanometric characteristics are observed in the first months of life. This is because the ME of children is dominated by the component of mass, and the resonance frequency tends to be lower when compared with normal adults, in whom the system is controlled by stiffness.14 A Brazilian study investigating resonance frequency reported a value of 250 Hz in children between 2 and 12 days and a value of 385 Hz in children between 72 and 84 days.32
Conclusion
After the analysis of several publications, it was found that both the test tones of 226 and 1,000 Hz show false-positive results (indicating the presence of alterations in the ME when they do not exist) and false-negative results (when changes are not detected even in their presence). However, both false-positives and false-negatives are less frequent with the 1,000-Hz probe tone. For this reason, the test frequency of 1,000 Hz is more sensitive and specific than the frequency of 226 Hz for the assessment of ME alterations in neonates. Therefore, it is concluded that this probe tone is most appropriate for evaluating infants less than 6 months of age. Although the literature confirms that the 1,000-Hz tone test is the most appropriate for assessment in this population, further studies are needed to clarify the doubts that still exist regarding the use of tympanometry with a high-frequency tone. In addition, better systems for the classification of curves and normality criteria should be investigated.
References
- 1.Kei J, Allison-Levick J, Dockray J. et al. High-frequency (1000 Hz) tympanometry in normal neonates. J Am Acad Audiol. 2003;14(1):20–28. doi: 10.3766/jaaa.14.1.4. [DOI] [PubMed] [Google Scholar]
- 2.Margolis R H, Bass-Ringdahl S, Hanks W D, Holte L, Zapala D A. Tympanometry in newborn infants—1 kHz norms. J Am Acad Audiol. 2003;14(7):383–392. [PubMed] [Google Scholar]
- 3.Carvallo R M. Rio de Janeiro, Brazil: Guanabara Koogan; 2003. Medidas eletroacústicas imitância acústica; pp. 1–22. [Google Scholar]
- 4.Margolis R H, Hunter L L. São Paulo, Brazil: Manole; 2001. Timpanometria: princípios básicos e aplicações clínicas; pp. 85–126. [Google Scholar]
- 5.Sininger Y S. Audiologic assessment in infants. Curr Opin Otolaryngol Head Neck Surg. 2003;11(5):378–382. doi: 10.1097/00020840-200310000-00012. [DOI] [PubMed] [Google Scholar]
- 6.Shahnaz N, Miranda T, Polka L. Multifrequency tympanometry in neonatal intensive care unit and well babies. J Am Acad Audiol. 2008;19(5):392–418. doi: 10.3766/jaaa.19.5.3. [DOI] [PubMed] [Google Scholar]
- 7.Baldwin M. Choice of probe tone and classification of trace patterns in tympanometry undertaken in early infancy. Int J Audiol. 2006;45(7):417–427. doi: 10.1080/14992020600690951. [DOI] [PubMed] [Google Scholar]
- 8.Swanepoel W, Werner S, Hugo R, Louw B, Owen R, Swanepoel A. High frequency immittance for neonates: a normative study. Acta Otolaryngol. 2007;127(1):49–56. doi: 10.1080/00016480600740563. [DOI] [PubMed] [Google Scholar]
- 9.Weatherby L A, Bennett M J. The neonatal acoustic reflex. Scand Audiol. 1980;9(2):103–110. doi: 10.3109/01050398009076343. [DOI] [PubMed] [Google Scholar]
- 10.Keefe D H, Bulen J C, Arehart K H, Burns E M. Ear-canal impedance and reflection coefficient in human infants and adults. J Acoust Soc Am. 1993;94(5):2617–2638. doi: 10.1121/1.407347. [DOI] [PubMed] [Google Scholar]
- 11.Gravel J S, Hood L J. São Paulo, Brazil: Manole; 2001. Avaliação audiológica infantil; pp. 301–322. [Google Scholar]
- 12.Joint Committee on Infant Hearing . Year 2007 Position Statement: Principles and Guidelines for Early Hearing Detection and Intervention Programs. Pediatrics. 2007;120(4):898–921. doi: 10.1542/peds.2007-2333. [DOI] [PubMed] [Google Scholar]
- 13.Newborn Hearing Screening and Assessment Tympanometry in babies under 6 months. A Recommended Test Protocol [cited November 20, 2012] Available at: http://hearing.screening.nhs.uk/audiologyprotocols#fileid10753
- 14.Holte L, Margolis R H, Cavanaugh R M Jr. Developmental changes in multifrequency tympanograms. Audiology. 1991;30(1):1–24. doi: 10.3109/00206099109072866. [DOI] [PubMed] [Google Scholar]
- 15.Alaerts J, Luts H, Wouters J. Evaluation of middle ear function in young children: clinical guidelines for the use of 226- and 1,000-Hz tympanometry. Otol Neurotol. 2007;28(6):727–732. doi: 10.1097/mao.0b013e3180dca1e5. [DOI] [PubMed] [Google Scholar]
- 16.Jerger J. Clinical experience with impedance audiometry. Arch Otolaryngol. 1970;92(4):311–324. doi: 10.1001/archotol.1970.04310040005002. [DOI] [PubMed] [Google Scholar]
- 17.Lidén G. The scope and application of current audiometric tests. J Laryngol Otol. 1969;83(6):507–520. doi: 10.1017/s0022215100070651. [DOI] [PubMed] [Google Scholar]
- 18.Margolis R H, Smith P. New York, NY: Grune and Stratton; 1978. Tympanometry in infants: state of art. [Google Scholar]
- 19.Sutton G Baldwin M Brooks D Gravel J Thornton R Tympanometry in neonates and infants under 4 months: a recommended test protocol Manchester, England 2002 [cited November 20, 2012]. Available at: http://hearing.screening.nhs.uk/
- 20.Marchant C D, McMillan P M, Shurin P A. et al. Objective diagnosis of otitis media in early infancy by tympanometry and ipsilateral acoustic reflex thresholds. J Pediatr. 1986;109:590–595. doi: 10.1016/s0022-3476(86)80218-9. [DOI] [PubMed] [Google Scholar]
- 21.Vanhuyse V J, Creten W L, Van Camp K J. On the W-notching of tympanograms. Scand Audiol. 1975;4(1):45–50. [Google Scholar]
- 22.Garcia M V, Azevedo M F, Testa J R. Accoustic immitance measures in infants with 226 and 1000 hz probes: correlation with otoacoustic emissions and otoscopy examination. Braz J Otorhinolaryngol. 2009;75(1):80–89. doi: 10.1016/S1808-8694(15)30836-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Camboim E D Correia A MN Vasconcelos D Torres R Scharlach R C Azevedo M F Comparative analysis of otoacoustic emissions with tympanometry in 0-6 month infantsRev CEFAC-Speech, Language, Hearing Sciences and Education Journal [online] 2012; 14(3):403-412 [cited November 20, 2012]. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1516-18462012000300004&lng=en&nrm=iso
- 24.Tazinazzio T G Diniz T A Marba S TM Colella-Santos M F Otoacoustic emissions and acoustic immitance measurements using 226 Hz and 1000 Hz probe tones in neonatesRev CEFAC-Speech, Language, Hearing Sciences and Education Journal [online] 2011; 13(3):479-488 [cited November 20, 2012]. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1516-18462011000300011&lng=pt&nrm=iso
- 25.Zhiqi L, Kun Y, Zhiwu H. Tympanometry in infants with middle ear effusion having been identified using spiral computerized tomography. Am J Otolaryngol. 2010;31(2):96–103. doi: 10.1016/j.amjoto.2008.11.008. [DOI] [PubMed] [Google Scholar]
- 26.Meyer S E, Jardine C A, Deverson W. Developmental changes in tympanometry: a case study. Br J Audiol. 1997;31(3):189–195. doi: 10.3109/03005364000000021. [DOI] [PubMed] [Google Scholar]
- 27.Silva K A, Novaes B A, Lewis D R, Carvallo R M. Tympanometry in neonates with normal otoacoustic emissions: measurements and interpretation. Braz J Otorhinolaryngol. 2007;73(5):633–639. doi: 10.1016/S1808-8694(15)30123-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mazlan R, Kei J, Hickson L. et al. High frequency immittance findings: newborn versus six-week-old infants. Int J Audiol. 2007;46:711–717. doi: 10.1080/14992020701525858. [DOI] [PubMed] [Google Scholar]
- 29.Swanepoel W, Hugo R, Louw B. Infant hearing screening at immunization clinics in South Africa. Int J Pediatr Otorhinolaryngol. 2006;70(7):1241–1249. doi: 10.1016/j.ijporl.2006.01.002. [DOI] [PubMed] [Google Scholar]
- 30.Lewis M P, Bradford Bell E, Evans A K. A comparison of tympanometry with 226 Hz and 1000 Hz probe tones in children with Down syndrome. Int J Pediatr Otorhinolaryngol. 2011;75(12):1492–1495. doi: 10.1016/j.ijporl.2011.06.008. [DOI] [PubMed] [Google Scholar]
- 31.Calandruccio L, Fitzgerald T S, Prieve B A. Normative multifrequency tympanometry in infants and toddlers. J Am Acad Audiol. 2006;17(7):470–480. doi: 10.3766/jaaa.17.7.2. [DOI] [PubMed] [Google Scholar]
- 32.André K D, Sanches S GG, Carvallo R MM. Middle ear resonance in infants: age effects. Int Arch Otorhinolaryngol. 2012;16(3):353–357. doi: 10.7162/S1809-97772012000300009. [DOI] [PMC free article] [PubMed] [Google Scholar]