

Abstract
China has launched a general practice (GP)-orientated primary care reform in 2009 to develop a more productive, coordinated, and cost-effective system to maintain and improve the health and well-being of one-fifth of the world population. The restructure of the health care system with a focus on primary care requires practitioners working on GP as gatekeepers for service delivery that is responsive to the needs of people. It is particularly prioritised to establish a sound education and training system to ensure that the competencies of practitioners are aligned with local health care needs. This article aims to provide a brief review of the development of GP, including exemplary model of education and training currently implemented in southern China, as well as the challenges to be addressed in the next step. There is a shortage of well-trained and qualified general practitioners in China where more than half of the licensed clinicians in primary care are educated below the undergraduate level. Although there is a stepwise increase in recognition that the capacity of GP is pivotal to the success of primary care development in China, challenges coming from resource restriction, rural and urban disparity, social attitude, and community involvement are highlighted as major bottlenecks that currently hinder the rapid development of GP in China. Supportive policy and guidelines are necessary to build up strong GP recognition and ensure adequate resources to underpin a robust primary care system to deliver affordable and effective health care services for the world’s largest population. It might share some similar experiences with other countries that are struggling to develop a GP-based primary care system.
Keywords: general practice, education and training, health care reform, southern China
Introduction
General practice (GP) was officially introduced by the World Organization of Family Doctors (WONCA) into China as a synonymous translation of ‘family medicine’ and ‘primary care’ in the late 1980s.1 Followed by the inauguration of the General Practice Branch in the Chinese Medical Association (CMA) in 1989, a number of national textbooks2-4 on the principle and praxis in GP have been published. Frequent communications and collaborations with domestic and overseas academics have also been taking place in the past 20 years, especially in southern China, which refers to the vast geographic region in the south of China. It mainly covers nine provinces, namely Guangdong, Guangxi, Hainan, Hunan, Fujian, Jiangxi, Yunnan, Guizhou, and Sichuan. This trans-Pearl River Delta has been considered to have more rapid pace in economical development compared to other regions in China. Province along the eastern sea coast, e.g., Guangdong province, plays a leading role in trend-setting implementation of policy initiatives with developed primary care infrastructure. It thus provides an opportunity to look into the development of GP education and training in China. This review started with an introduction of the policy initiatives on GP, and then moved on to the status quo of GP education and training, followed by a discussion on the challenges to be addressed in the next decades.
Policy initiatives on GP
The central government has been issuing a series of official documents and guidelines5-10 since 1997 with attempts to re-build the community-based health care system. It aimed to provide primary care service that is safe, effective, convenient, and affordable by general practitioners, i.e., clinical physicians in the township health centres (THCs) and village clinics (VCs) in rural areas, and community health centres (CHCs) in urban areas. Such revitalisation of general practitioners for the delivery of primary care services to all citizens has now been recognised to be paramount with a slow but stable progress.11 Medical universities in eastern seaboards in China, including Beijing, Tianjin, Shanghai, Zhejiang, Guangdong, Anhui, Heilongjiang, etc., have also started to take up pilot initiatives to reshape medical education using a new bio-psycho-social medical model in response to the series of national calls for developing GP education and training.12-21 It aimed to change the traditional, physician-led, disease-focused medical pattern, which was largely based at hospital settings into the patient-centred practice with family as a unit at the community setting. A more recent comprehensive primary care reform.22 launched in early 2009 with the strategic goal of ‘Healthy China 2020’23 has led to a widely embraced consensus that GP as an emerging discipline is equally important as other medical specialities. It has also been recognised that the objective of medical education is to cultivate doctors who not only deliver treatments to patients who are suffering from diseases, but also promote health awareness from a population perspective.24 In view that both noncommunicable and communicable diseases threats are simultaneously encountered in China with their epidemiology related to a wide range of social, psychological, and economic factors,25,26 the health care reform also expects GP education and training to include better health and better health care for all, rather than increasing the disparity in income, health, and health care across areas with different socio-economic statuses. Health care professionals nurtured in the track of clinical medicine with the knowledge and expertise in preventive care will remain and continue to be considered as the mainstay and cadre of the primary care providers to deliver community health services,24 Thus, the extent to which clinical professionals are specialised in GP directly dominates the prospects of primary care in China.
Education and training on GP in southern China
Unlike many other developed countries such as the United States and Canada, the entrance to tertiary medical universities in China starts after the completion of high school. Although high school graduates are provided with the options to select programmes and disciplines at various universities, the enrolment in these clinical programmes is predominantly determined by quota availability and students’ academic performance in the annually held National Matriculation Examination, which is the prerequisite for admission to tertiary education. Currently, multiple programmes in clinical medicine are available at the undergraduate level in China. Some medical universities run 3- or 4-year combined programmes for students to pursue an associate degree. Most medical universities provide a normative 5-year programme in clinical medicine towards bachelor degree, followed by a 3-year postgraduate programme with a master degree. In a very limited number of prestigious medical universities, there are articulated programmes covering both undergraduate and postgraduate education levels, which last for 7 years towards a master degree and 8 years towards a doctoral degree. China’s current education system is little flexible in allowing students to switch programmes after enrolment in the university regardless of their interests and aptitudes. It is therefore crucial to deliver good-quality GPorientated medical education to students enrolled in the GP stream to better master the substantial body of GP knowledge, attitude, and skills that are indispensable for optimal practice in the community after graduation.
The past decade has witnessed a rapid development of the GP education and training system across southern China, especially in Guangdong province, where there is a growing recognition and value for GP. Since 1997, the 5-year, undergraduate-level curriculum for GP has been piloted at Guangzhou Medical University (GZMU), which demonstrated the commencement of GP as an independent discipline. Later in 2003, the General Practice Education and Training Centre of Guangdong province was established and affiliated with GZMU to authorise accreditation and certification for qualified GP personnel and to ensure the workforce competency and community health service delivery in southern China. An education and training system embedded with both preventive and curative perspectives starting from degree-awarding undergraduate and postgraduate education to non-degree-awarding continuing medical education have been developed. Both theoretical and practical teaching methods are adopted. Theoretical teaching method covers both problem-based learning and conventional lecture-based learning. Teaching activities are often performed in the face-to-face classroom setting, and paper-based examination is often used for evaluation. Practical teaching often takes place in the clinic setting at the community with the evaluation focusing on practical skills. Although variations exist in terms of theory and practical teaching in different areas, such training aims to enrich the knowledge and expertise of trainees and students who are required to complete and pass all the examinations to continue their career in GP. Such holistic system has served as an exemplary model imitated by other medical universities in southern China (Figure 1).
Figure 1.
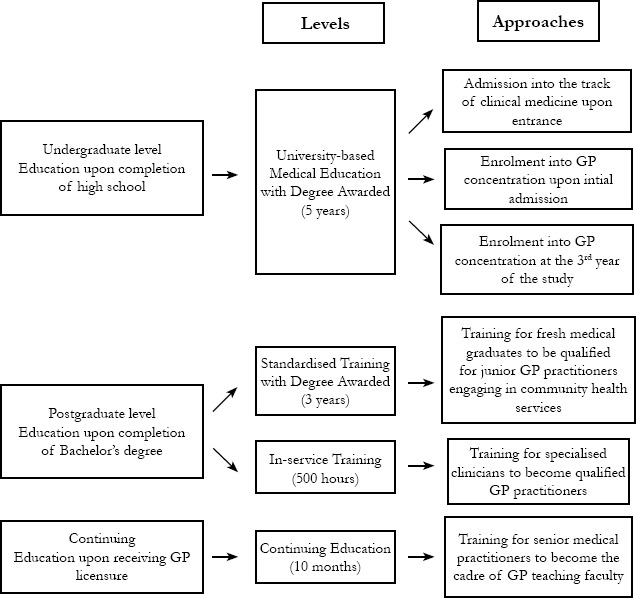
Education and training framework in southern China
Reference: Wang HHX, Wang JJ. Developing primary care in China. In: Griffiths sM, tang JL, Yeoh eK, eds. Routledge Handbook of Global Public Health in Asia. oxford: Routledge publisher. April 2014. PP. 584-600 (IsBn 978-0-415-64382-5)
Undergraduate-level degree-awarding curriculum
At the undergraduate level, clinical medical students are enrolled in the GP stream either through entrance or in the mid-period of their 5-year study in the medical university. Apart from the courses in the general clinical medicine, major courses related to GP include foundations of GP, community medicine, community health service management, disease prevention, community rehabilitation and nursing, community emergency and first aid, application of statistical softwares in the community, etc. Non-clinical medical students, they also have exposure to knowledge and expertise in generalised preventive health care, which are regularly integrated via both compulsory and elective courses into their entire 5-year study to obtain the Bachelor’s degree.
Postgraduate-level degree-awarding curriculum
The 3-year GP-standardised training is the core element for fresh medical graduates who wish to engage in community health services in the primary care setting. A typical training programme consists of a 3-month theory study on GP, followed by a 26-month clinical rotation and expertise training, and a 7-month community-based health service practice. Clinical rotations take place in hospital-based departments, including internal medicine, neurology, paediatrics, surgery, gynaecology & obstetrics, emergency, dermatology, ophthalmology, ENT, infectious diseases, psychiatry, rehabilitation, and Traditional Chinese Medicine with different lengths of duration. Upon completion of the standardised training programme, the candidates receive GP-qualifying certificates and are therefore qualified for GP registrar after passing the National Health Professional Technical Qualifying Examination.
In-service training programmes for specialised clinicians
A 500-hour in-service training programme is offered to specialised clinicians. It consists of 240-hour theory, 200-hour clinical exposure, and 60-hour community practice. The courses cover various aspects of GP foundation, generalised medical care, community prevention, health maintenance, and rehabilitation. Each aspect contains both theory teaching and clinical and community exposure. The emphasis is mainly on doctor-patient interpersonal relationship, healthy lifestyle promotion, life-cycle health care, and clinical treatment strategies in GP. Programme completion is mandatory for these nongeneral practitioners to convert themselves into general practitioners such that they can continue their engagement in community health service provision.
Training programmes for cadre of GP faculty and other managerial workforce
A 10-month in-service full-time study including 1-month theory training, 7-month clinical rotation, followed by a 2-month community-based health service practice is also provided for senior medical practitioners and licensed GP registrars to become the cadre of GP faculty. Compared with the in-service training for specialists, the emphasis has been shifted to community psychological consultation, health care records, chronic disease management, and literature search for conducting future evidence-based studies in the community setting. Training programmes for managerial staff and other health care professionals, including nurses, pharmacists, and care providers, are also established to improve the quality and the standard of primary care delivery teams in the community. In addition, senior medical practitioners with grass-root working experience in the primary care are invited to enrol as GP faculty to provide high-quality education and training. The training syllabus and teaching curriculum are also standardised in all affiliated GP training centres.
Currently, most of GP faculties consist of teachers from local medical universities and experienced senior general practitioners from the community. GP faculties receive remuneration for full-time or part-time teaching activities, and a set of standards and guidelines are established to ensure the teaching quality. GP in-service training and continuing education have become mandatory nationwide for such practitioners in both urban and rural areas. Although the outcomes of education and training require further evaluation, trained general practitioners are acquiring a good local reputation and public acceptance. In view of the emerging models of primary care delivery creating favourable environment in southern China,11,27 general practitioners with good qualifications and professional competence would attract large numbers of patients at the community level.28
Barriers and challenges
The current comprehensive health reform in China aims to develop a more productive, coordinated, and cost-effective approach to improve the health and well-being of one-fifth of the world population.27,29 The restructure of the health care system with a focus on primary care requires general practitioners as gatekeepers for service delivery that is responsive to the needs of people. The current obstacles to the success of GP education and training in the health system are mainly resource availability and sustainability, social attitude on GP recognition, as well as policy support to attract and retain GP workforce.
Poor educational level
Data from the China Health Statistics in 2011 revealed that 61.4% of licensed general practitioners in urban areas and 85.0% of licensed general practitioners in rural areas do not hold a bachelor’s degree from medical university30 (Table 1). The majority of these practitioners had their medical training at either senior college (with associate degree) or junior college after the completion of secondary school. Compared to medical universities, such medical colleges often provide inferior quality of GP knowledge and skills. Thus, the health care system is under threat from low-quality primary care delivered by these under-qualified general practitioners. It becomes particularly paramount to raise the education level for general practitioners. Meanwhile, joint collaborations among different government sectors at different levels are required to contribute to an overall substantive change to address the urgent need of qualified GP workforce.
Table 1. Profiles of general practitioners in urban and rural areas in southern China30,31 .
| 2005 | 2010 | |||||||
| Urban | Rural | Urban | Rural | |||||
| Number | % | Number | % | Number | % | Number | % | |
| Population (million) | 181.34 | - | 270.66 | - | 220.78 | - | 246.50 | - |
| Registered practitioners | 2,679 | - | 139,965 | - | 34,674 | - | 152,080 | - |
| Practitioners per 1,000 population | 0.01 | - | 0.52 | - | 0.16 | - | 0.62 | - |
| Gender | ||||||||
| Male | 1,165 | 43.5 | 95,552 | 68.3 | 16,331 | 47.1 | 103,566 | 68.1 |
| Female | 1,514 | 56.5 | 44,413 | 31.7 | 18,343 | 52.9 | 48,514 | 31.9 |
| Age (years) | ||||||||
| Less than 25 | 40 | 1.5 | 1707 | 1.2 | 35 | 0.1 | 152 | 0.1 |
| 25-34 | 726 | 27.1 | 44,685 | 31.9 | 9,119 | 26.3 | 33,914 | 22.3 |
| 35-44 | 593 | 22.1 | 43,366 | 31.0 | 11,546 | 33.3 | 62,657 | 41.2 |
| 45-54 | 1,056 | 39.4 | 33,874 | 24.2 | 7,663 | 22.1 | 33,458 | 22.0 |
| 55-59 | 188 | 7.0 | 12,658 | 9.0 | 3,988 | 11.5 | 16,273 | 10.7 |
| 60 and above | 76 | 2.8 | 3,675 | 2.6 | 2,358 | 6.8 | 5,779 | 3.8 |
| Education level | ||||||||
| Master’s degree or above | 7 | 0.3 | 74 | 0.1 | 555 | 1.6 | 304 | 0.2 |
| Bachelor’s degree | 668 | 24.9 | 7,869 | 5.6 | 12,864 | 37.1 | 22,660 | 14.9 |
| Associate’s degree | 1,061 | 39.6 | 45,055 | 32.2 | 13,523 | 39.0 | 64,786 | 42.6 |
| Junior college | 773 | 28.8 | 68,164 | 48.7 | 6,761 | 19.5 | 55,205 | 36.3 |
| High school or below | 169 | 6.3 | 18,802 | 13.4 | 1,006 | 2.9 | 9,277 | 6.1 |
Rural and urban disparity
Generally, there are substantial disparities in the socio-economic status between urban and rural areas. Nationwide statistics in 2006 depicted that the average monthly income of health care practitioners in urban areas was 3.16 times their counterparts in rural areas,31 and the number decreased to 2.44 in 2011.30 Although the situation seems to be slightly improved, such disparity in the per capita income levels might still weaken the confidence of medical graduates to work in rural areas. High-quality medical resources are often concentrated in the secondary or tertiary health care facilities in big cities, leading to poor accessibility to resources at the grass-root level. Bottlenecks in human resources in less developed regions include not only the shortfall of primary care providers, but also the variability in the clinical expertise of general practitioners. Currently, the migration of primary care workforce from urban to rural areas for improving the quality of primary care services for rural population is simply encouraged by national policy on a voluntary basis. The detailed statistics on the duration of general practitioners working in rural areas are not available yet; however, the incentives in promoting the migration of urban personnel are limited in general and are only available in a few areas. A gap still exists in the supportive policies to sustain general practitioners in the rural areas. In the long term, rural areas are more likely to have general practitioners with deficient competence and much lower education level, and are also prone to struggle with ‘brain drain’ compared to that in affluent areas. Constraints in physical resources include the lack of suitable training bases, poor quality of equipments and supplies, and non-existence of convenient working environment to carry out clinical training and community practice. The drawbacks of education resources include the inferior teaching standards, library support, Internet access, etc., in medical universities and training centres located outside the urban areas. The resource hardship in the infrastructure is further magnified and exacerbated by limited or unstable funding support to contribute to facility renovation, technology innovation, and faculty development.
Community involvement and social empowerment
Active involvement and social support from wider communities also play pivotal roles in ensuring the success of GP education and training. However, there is a widespread misunderstanding that primary health care practice at the grass-root community level is ’second class’ with inferior standard and quality compared to that in large-scale secondary and tertiary hospitals in urban areas. The branch of GP in medical education is often deemed as a simple collection of several independent subjects rather than a holistic approach and coordinated discipline than spanning full spectrum of health care with a population perspective. This unjustified assumption in turn accompanied with a prevailing attitude that generalised practitioners are low-tech and unprofessional compared to specialised medical practitioners who were the core in the conventional medical approach. Sound evidence from population-based studies in China is essential to demonstrate the achievements of primary care in improving health outcomes in a most cost-effective way. Moreover, both the general population and medical students need to be convinced and motivated to embrace the idea that generalised practitioners can make a significant contribution to the primary care infrastructure as they can better provide people-centred care in a comprehensive and continuous manner with a flexibility that allows them to adapt to the specific needs of the community they serve. In addition, under-developed clinical training and community practice bases have deteriorated the quality of GP education; thus, it requires active participation of communities in close relationship with medical universities. Currently, there are few initiatives that have realised the advantages of communities in enabling not only the local provision of social support for GP trainees, but also the deeper understanding of the ecological model for the social determinants of health.
Career advancement and policy support
Another unfavourable circumstance that impedes GP education and training is that GP health care professionals tend to be less prioritised in terms of employment benefits and career promotion compared to those specialised practitioners. National statistics in 2011 demonstrated that the average monthly income of clinical physicians working in specialist care was 2.98 times that of the general practitioners.30 The less favourable policy under which general practitioners are generally remunerated at lower rates than other medical specialists would further hinder the process of recruiting and retaining sufficient general practitioners. Strong support from the government is also needed to inaugurate pragmatic policies with effective implementation to guarantee GP as an indispensible discipline at the undergraduate-level medical education. Difficulties also derive from the current policy gap between the completion of the postgraduate-level standardised training and the attainment of the master-level medical degree. Joint collaboration and creative solutions are needed among different sectors related to health, education, and human resources at the government level to ensure the vocation retention and career prospects of GP workforce at primary health care faculties, especially in less-developed, sub-urban, and rural areas. Staff remuneration is often considered as one of the most unsatisfied aspects among general practitioners. Favourable policies are often deficient to narrow the salary gap between primary care practitioners and specialised care practitioners, especially in the initial stages of GP development. In some areas, there is pilot policy implementation with favourable remuneration and career advancement to attract general practitioners to work in rural areas; however, the outcome is yet to be evaluated.
Implications
Similar to China, there has also been a recent shift in the focus from specialist-based secondary care to GP-based primary care in terms of both health care service delivery and medical education in Malaysia.32 Both countries share some similarities in terms of the education level of general practitioners and social recognition of GP discipline. It is common that the percentage of general practitioners receiving vocational training or postgraduate-level education is low and GP tends to be considered as a less desirable career path with lower prestige due to the perception of both medical students and the general public. A correct understanding of the GP-based primary care as the cost-effective approach to achieve optimal health for all might help build up prestige and appreciation for GP in the health care sector. Communications and exchanges among general practitioners, primary care researchers, and policy makers between Malaysia and China will be significant in GP development in the next decades. The geographic advantages would allow southern China to have more frequent communications with its neighbours in Asia Pacific regions to gain successful experience, which in turn might bring about a quicker pace in primary care development. It is expected to have a developed GP education and training system in response to the vision and mission of the national health care reform with consequent improvement in its population health outcomes. The experience of GP education and training in southern China might allow general practitioners and researchers from other countries that are struggling with the development of the GP-based primary care system to watch and learn.
Summary
The shortfall in GP education and training is currently prevailing in most of the areas, and China’s current health care reform still remains a long way ahead. Its aspiration to provide all citizens with safe, effective, convenient, and affordable basic care continuously demands a good GP education and training system with clearly established targets and benchmarks. Although there is a stepwise increasing recognition that the capacity of GP is pivotal to the success of primary care development in China, this review highlighted that future development needs to overcome the challenges in resource restriction, rural and urban disparity, social attitude, and community involvement. Supportive policy and guidelines are necessary to build up GP recognition and ensure adequate resources to underpin the robust primary care systems to deliver an affordable and effective health care service for the world’s largest population.
Acknowledgement
The authors acknowledge National Education Sciences “Eleventh Five-Year Strategic Plan” Key Project, Ministry of Education (DIA060145), Guangdong Education Sciences “Eleventh Five-Year Strategic Plan” Annual Project, Department of Education, Guangdong province (2010tjk274), and Medical Education Project Fund, Society of Medical Education, Chinese Medical Association & Medical Education Committee, and Chinese Association of Higher Education (2012-QK-2) for providing funds.
Conflict of interest
There was no conflict of interest among the authors.
Contributor Information
HHX Wang, School of Public Health and Primary Care, Faculty of Medicine, The Chinese University of Hong Kong; Hong Kong, PR China, Email: haoxiangwang@cuhk.edu.hk; General Practice and Primary Care, Institute of Health and Wellbeing, University of Glasgow; UK, Email: Haoxiang.Wang@glasgow.ac.uk.
JJ Wang, School of Public Health, Guangzhou Medical University; Guangzhou, Guangdong Province, PR China, Email: wjiaji@163.com.
ZH Zhou, School of Public Health, Guangzhou Medical University; Guangzhou, PR China.
XW Wang, Guangdong General Practice Education and Training Centre; Guangzhou, PR China.
L XU, Guangdong General Practice Education and Training Centre; Guangzhou, PR China.
References
- 1.Wu CR. Hangzhou: Hangzhou University Press; 1993. An introduction to general family medicine. [Google Scholar]
- 2.Gu Y, Lu F. Beijing: World Publishing Corporation; 1995. Theory and praxis in general practice. [Google Scholar]
- 3.Yang BH. Beijing: People’s Medical Publishing House; 2001. An overview of general practice. [Google Scholar]
- 4.Liang WN. Beijing: Peking Union Medicai College Press; 2005. Introduction to general practice. [Google Scholar]
- 5.Decision on healthcare reform and development. Central Committee of the Communist Party of China. http://www.moh.gov.cn/wsb/pM30115/200804/18540.shtml State Council, PR China. Available at. 1997
- 6.Decision on establishing basic medical insurance system for urban employees. No. 44 documents. State Council. http://www.gov.cn/banshi/2005-08/04/content_20256.htm Available at. 1998
- 7.Opinions on developing community health services in the cities. No. 326 document. Division of Primary and Women’s Health, Ministry of Health, China. http://www.moh.gov.cn/publicfiles/business/htmlfiles/mohfybjysqwss/pfybj/200804/18183.htm Available at. 1999
- 8.Guidance on pharmaceutical and healthcare system reform in urban areas. No. 16 document. State Council. http://www.moh.gov.cn/wsb/pzcjd/200804/23961.shtml Available at. 2000
- 9.Guidance on accelerating the community health service development in urban areas. No. 186 document. Ministry of Health. http://www.moh.gov.cn/mohfybjysqwss/s6746/200804/18181.shtml Available at. 2002
- 10.The implementation scheme of establishing national exemplary community health service regions. No. 252 document. Ministry of Health. http://www.moh.gov.cn/mohfybjysqwss/s6456/200804/17116.shtml Available at. 2003
- 11.Wang HHX, Wang JJ. In: Routledge Handbook of Global Public Health in Asia. (ISBN 978-0-415-64382-5) Griffiths SM, Tang JL, Yeoh EK, editors. Oxford: Routledge publisher; April 2014. Developing Primary Care in China; pp. 584–600. [Google Scholar]
- 12.Pilot regulations on standardised training of general practitioners. No. 610 document. Ministry of Health, PR China. http://wsb.moh.gov.cn/mohkjjys/s6755/list.shtml Available at. 1999
- 13.Opinions on developing general practice education. No. 34 document. Ministry of Health, PR China. http://www.moh.gov.cn/wsb/pzcjd/200804/23866.shtml Available at. 2000
- 14.The basic requirements of clinical and community training base of general practice. Ministry of Health, PR China. http://wsb.moh.gov.cn/mohkjjys/s3593/201301/4b20176ade4449f097bc2551298c2d06.shtml Available at. 2000
- 15.Guidance on developing community health services in the cities. No. 10 document. State Council, PR China. http://www.gov.cn/zwgk/2006-02/23/content_208882.htm Available at. 2006
- 16.Guidance and opinions on strengthening healthcare professionals cadre for community health service in urban areas. No. 69 document. Ministry of Human Resources and Social Security, Ministry of Health, Ministry of Education, PR China. http://www.gov.cn/zwgk/2006-08/10/content_359177.htm 2006
- 17.Opinion on strengthening the education and discipline construction for general practice and community nursing in tertiary medical universities. No. 13 document. Ministry of Education, PR China. http://www.moe.gov.cn/publicfiles/business/htmlfiles/moe/s3864/201010/xxgk_109616.html Available at. 2006
- 18.Announcement on construction plan of general practitioner-based healthcare professional cadre. No. 561 document. National Development and Reform Commission, PR China. http://www.ndrc.gov.cn/shfz/yywstzgg/ygzc/t20100430_359849.htm Available at. 2010
- 19.Trans-service training syllabus for general practitioners in grass-roots healthcare facilities. No. 211 document. Ministry of Health, PR China. http://www.moh.gov.cn/mohkjjys/s3593/201101/50340.shtml Available at. 2010
- 20.Announcement on in-service training syllabus for community health workforce. No. 76 document. Ministry of Health, PR China. http://www.moh.gov.cn/mohkjjys/s3594/201005/47278.shtml Available at. 2010
- 21.Guidance opinion on establishing general practitioner-based system. No. 23 document. State Council, PR China. http://www.gov.cn/zwgk/2011-07/07/content_1901099.htm Available at. 2011
- 22.Opinions on deepening pharmaceutical and healthcare system reform. No. 9 document. State Council. http://www.gov.cn/jrzg/2009-04/06/content_1278721.htm Available at. 2009
- 23.Healthy China Plan 2020. Ministry of Health. http://www.gov.cn/gzdt/2008-01/07/content_851780.htm Available at. 2008
- 24.Wang JJ, Liu YH, Wang XW. et al. The exploration and practice in the construction of general practice education system in Guangdong province in China [In Chinese] Chinese General Practice. 2006;9(15):1228–30. [Google Scholar]
- 25.Wang HHX, Wong MCS, Wong SYS. et al. The profile of cardiovascular multimorbidity among patients in primary care in southern China: a cross-sectional study. Int J Cardiol. 2013;163(Suppl 2):S28. [Google Scholar]
- 26.Wang HHX, Wong MCS, Wong SYS. et al. Factors associated with cardiovascular multimorbidity among primary care patients in southern China. Int J Cardiol. 2013;163(Suppl 2):S8–9. [Google Scholar]
- 27.Wang HHX, Wong SYS, Wong MCS, Ann Fam Med. 6. Vol. 11. 26: 2013. Patients’ experiences in different models of community health centers in Southern China; p. 517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wang JJ, Zhong NS, Zhu AR. Review of the development of family physicians and general practitioners with Chinese characteristics [In Chinese] Chinese Rural Health Service Administration. 2009;29(9):663–5. [Google Scholar]
- 29.Wang HHX, Wong MCS, Wong SYS. et al. The impact of cardiovascular multimorbidity on healthcare service utilisation under three primary care organisational models in China. Int J Cardiol. 2013;163(Suppl 2):S1–2. [Google Scholar]
- 30.2011 China Health Statistics Yearbook: Center for Health Statistics and Information, Ministry of Health, PR China. 2011
- 31.2006 China Health Statistics Yearbook: Center for Health Statistics and Information, Ministry of Health, PR China. 2006
- 32.Ng CJ, Leong KC, Teng CL. What do medical students think about primary care in Malaysia? A qualitative study. Education for Primary Care. 2005;16(5):575–80. [Google Scholar]