

Abstract
Background:
Despite the importance of patients’ adherence to their drug treatments for achieving desired therapeutic goals and the proven role 3-hydroxy-3-methylglutaryl coenzyme A inhibitors (statins) for the health status of patients with cardiovascular diseases, there is not enough information regarding diabetic patients’ adherence to statin therapy in developing countries. In this clinical study we aimed to assess the adherence of diabetes type 2 patients to statin therapy in a research based community clinic in Iran.
Materials and Methods:
In this prospective clinical study which was done at Isfahan Endocrinology and Metabolism Research Center, 204 diabetic type 2 patients under treatment with statin were interviewed twice and their demographic data (age, gender, body mass index, education), statin information (type, dose) and their serum lipid profile were recorded. Three months after the initial visits, patients were assessed using pill counting method and according to patients’ self-reporting and also assessed low-density lipoprotein (LDL) cholesterol goal attainment <100 mg/dl.
Results:
Adherence rate was 79.7% and 69% according to pill counting and self-reporting among study population. Moreover, 68.4% of patients achieved their LDL cholesterol goal of <100 mg/dl and adherent patients reached therapeutic goal significantly more than those who were considered non-adherence to statin therapy (P < 0.01).
Conclusion:
Adherence to statin therapy, as reflected by pill count method, is significantly related to LDL cholesterol goal achievement in patients with diabetes and dyslipidemia. Pill count method can be used to identify patients who are nonadherent to statin therapy and at high risk for failure to attain LDL cholesterol goals.
Keywords: Diabetes, drug adherence, pill count method, statins
INTRODUCTION
It is estimated that more than 4 million adults had diabetes in 2011, which showed 35% increment during past 7 years. Expanding epidemic of obesity is responsible in large part for a high prevalence of diabetes mellitus and impaired fasting glucose among Iranian adults.[1] Therefore, an increase in the risk of cardiovascular diseases including coronary heart disease (CHD), is anticipated.[2,3] In fact, the presence of diabetes is somehow considered equivalent to that of a history for CHD. Consequently, the coexistence of diabetes and hypercholesterolemia further raises the risk of cardiovascular morbidity and mortality.[4]
Effective lipid lowering therapies especially statins are widely available to decline the cardiovascular risk across a wide range of patients particularly those with type 2 diabetes.[5,6] Patients with type 2 diabetes are benefitted from statin therapy by decreasing the risk of CHD and related clinical outcomes.[7]
Unfortunately, despite the availability of effective pharmacologic treatment and well-publicized therapeutic guidelines, elevated serum cholesterol levels remain uncontrolled in patients with hypercholesterolemia especially those with diabetes.[8] The percentage of controlled cholesterol among United States adults receiving treatment increased from 45.0% in 1999-2000 to 63.6% in 2009-2010. However high low-density lipoprotein (LDL) cholesterol remains the common problem in health care system.[8]
Significant gap between expected and actual benefit of statins may be attributed to the lack of enough follow-up or inappropriate titration of the starting statin dose. In addition, poor adherence may be considered amongst the most important reasons of failure to achieve the goals for dyslipidemia.[5,9] In a retrospective cohort study, the proportion of days covered by statin treatment was 79% among elderly patients (23.5% with diabetes) during the first 3 months. Although adherence fell dramatically to 42% after 120 months follow-up.[10]
To the best of our knowledge, there is not enough information regarding statin adherence and/or goal attainment rates of LDL cholesterol of patients with type 2 diabetes in developing countries. To address these issues, we conducted a study to evaluate the adequacy of diabetic patients’ adherence to statin therapy for lipid management in a research based community clinic in Iran.
MATERIALS AND METHODS
We conducted a prospective clinical study in patients with type 2 diabetes under treatment with statins. Participants enrolled in Isfahan Endocrinology and Metabolism Research Center (IEMRC). IEMRC is one of the largest outpatient diabetes research centers in the central part of Iran which also provides medical care and educational program for patients with diabetes. The study protocol of this observational research project was approved by the institutional board for human studies at Isfahan University of medical sciences (registration number, 3,87,311). All patients received a 15 min explanation of the study protocol in simple language by the principal investigator Farsaei and if they announced to join the study, they were recruited. They also were free to leave the study whenever they want without depriving from normal medical care.
All patients who took statins were identified during 3 months and included to the study. Among enrolled patients who did not have documented LDL cholesterol within 90 days after study inclusion or those who did not keep their scheduled visit 3 months after their initial visit were excluded.
Totally, 204 patients with diabetes and prescription of statins were included during a 3-month sampling period. Pharmacist interviewed patients and filled out demographic data (age, body mass index [BMI], sex, education) and statin information (type, dose and initial number of prescribed statin) in data gathering form.
In addition, data regarding LDL cholesterol over the same period were included to evaluate the relationship between LDL level and statin adherence. Since metformin could have a significant effect on lipid profile, data regarding administration dose of metformin were also gathered to compare between groups.
All included patients were asked to return 3 months after initial visit for counting remained statins and calculate statin adherence. Subsequently, in the second visit remained medications in blisters were counted in all participants and adherence was calculated.
In our study with pill count method, adherence of patients was expressed as a percentage of medicines taken during 3 months relative to the number of medicines that should have been taken during the same period.[11] Adherence was considered when this ratio exceeding 80% for all of their medications including statins. Correspondingly patients that took <80% of their medications were classified as nonadherent.[11]
In addition, self-reporting was used to report medication behavior of patients during 3 months. In the same manner patients declared taking <80% of their prescribed statins were considered nonadherent to their treatment. Medication possession ratio (MPR) was also calculated during 3 months of study to evaluate its correlation with mean LDL cholesterol level. MPR was defined as the percentage of days when medication was available for patients.[12]
Finally, understanding the barriers to adherence was performed by patients’ self-reporting.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation and categorical data as a percentage. Kolmogrov-Smirnov test was carried out to assess the distribution of continuous variables. Student's t-test, Chi-square, and Mann–Whitney U-test were used to evaluate results. In addition, Pearson correlation was used to evaluate the association between MPR and LDL cholesterol level.
Data processing was performed by SPSS statistical software version 11.5 software (SPSS Inc., Chicago, IL, USA), and two-tailed P < 0.05 was considered for statistical significance in all analyses.
Ethical issues
The research protocol for this study was approved by the board of human studies of the Isfahan University of Medial Sciences. Also, researchers preserved privacy and confidentiality of all patients’ information.
RESULTS
Among 204 patients met inclusion criteria, 46 patients were excluded during the study and final analyses were conducted with the data from 158 patients who completed the study [Figure 1]. Lovastatin was prescribed for more than 98% of patients in our study with dose of 10.2 ± 3.7 mg daily and <2% of patients received atorvastatin or simvastatin as cholesterol lowering agent. Therefore the analysis was not conducted based on type of statins.
Figure 1.
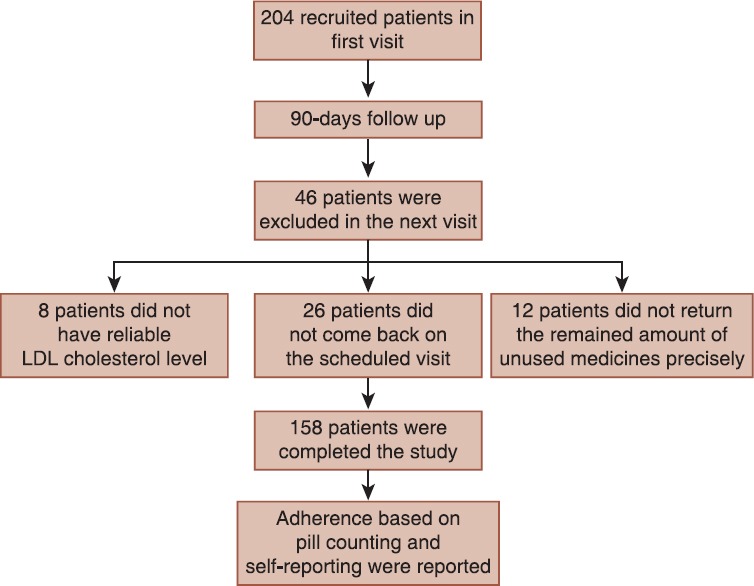
Follow-up chart of the studied patients
Overall, 20.3% (n = 32) of patients were considered nonadherent to statin therapy and only 31.6% (n = 50) of patients achieved their LDL cholesterol goal <100 mg/dl.
Although higher percent of males had adherence ≥80% to statin therapy than females but there was no significant difference between genders [Table 1]. Once again, the rate of LDL goal attainment was higher among men however it was not significant [Table 2]. Furthermore, other demographic characteristics including age, BMI, control of diabetes (hemoglobin A1c) and education did not significantly affect on adherence and LDL goal achievement [Tables 1 and 2].
Table 1.
Demographic characteristics of the studied patients and adherence to statin therapy
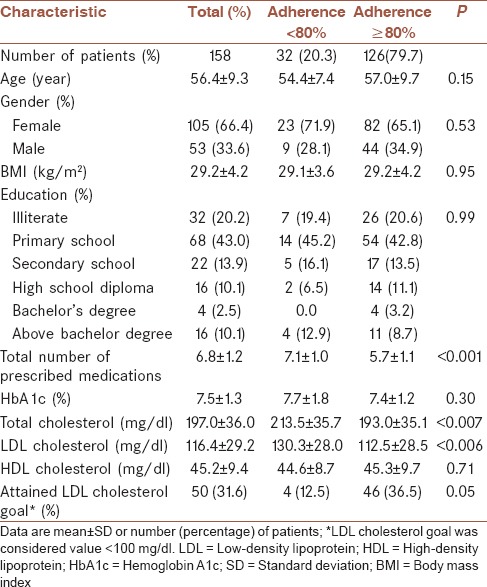
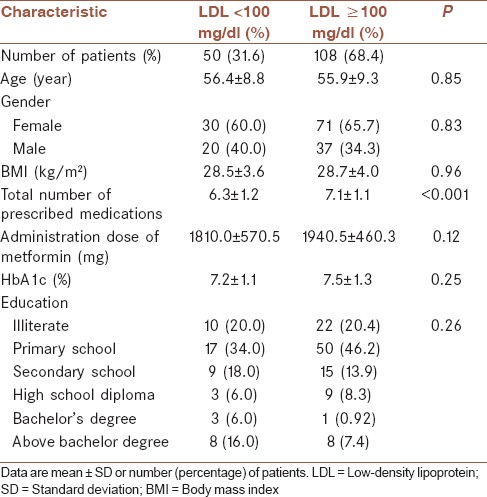
Table 2.
LDL cholesterol goal attainment and related factors
In this study, patients with adherence ≥80% had lower total and LDL cholesterol than those with adherence <80% (P < 0.01). Moreover, adherent patients reached therapeutic goal significantly more than those who were considered non-adherence to statin therapy (P < 0.01).
In addition, number of prescribed medications had a significant effect on statin adherence and LDL goal attainment. Patients with adherence ≥80% or LDL <100 mg/dl had lower prescribed medication in comparison with adherence <80% or LDL ≥100 mg/dl, respectively. According to self-reporting, most of studied population (69%) were adherent to statin and 49 patients (31%) were nonadherent.
The mean of MPR of statins during 3 months was 0.89 ± 0.24 and Pearson correlation showed the weak inverse relationship between MPR and LDL cholesterol, however this was not statistically significant (r = −0.16, P = 0.08).
A Chi-square test showed that there was a significant relationship between adherence reporting by pill counting and self-reporting (P < 0.01). Since 92% of self-reported adherent patients were also considered, adherent based on pill counting and 50% of patients who reported non-adherence to statin treatment had adherence <80% according to pill counting.
Possible factors influencing patient's adherence to statin therapy are illustrated in Figure 2. The most frequent barrier to adherence was reported as forgetting to take statins (50%). Discontinuation of medication when LDL cholesterol had been controlled or when patients were outside their home were other frequent factors related to non-adherence. In addition, an insufficient amount of prescribed statins which led to finish them before next visit and experienced side effects such as headache and gastrointestinal problems are other reasons of non-adherence to statins in patients with type 2 diabetes.
Figure 2.
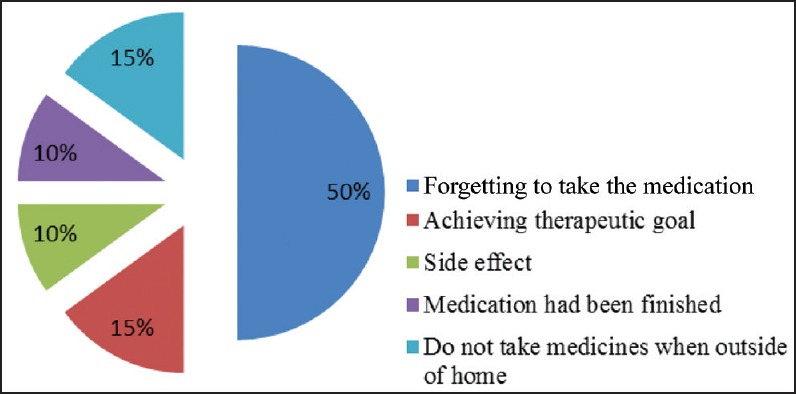
Reasons of non-adherence to statin in patients with type 2 diabetes
DISCUSSION
In spite of the importance of adherence to statin therapy for achieving therapeutic goals, there are limited reports about adherence to statin therapy and its associated factors especially in developing countries.
Meaningful reduction in LDL cholesterol was shown to be associated with pill count exceeding 80%.[13] Therefore, we also considered the adherence when patients took more than 80% of pills that should have been taken.
There is limited data about patients’ adherence to statins in developing countries. However, a recent evaluation of 248 Iranian patients with type 2 diabetes showed more than one-third of them were non-adherence to oral hypoglycemic agents.[14] Moreover, the overall prevalence of therapeutic noncompliance of patients with diabetes was 67.9% in Saudia Arabia.[15]
Our results revealed that according to the pill counting, at least one fifth of patients with type 2 diabetes were nonadherent to statin treatment. In addition, both pill count and self-report agreed in defining adherent and nonadherent patients.
Unfortunately, there is not any database for medications in community pharmacies which demonstrates adherence in Iran so we considered pill counting and self-reporting to evaluate that. Other reports showed different range of adherence to statin therapy which may be related to study population, setting and method of adherence measurement.[16] In these studies, more than 60% of patients had good adherence to statin therapy especially during the 1st month of treatment.[10,17,18,19]
A meta-analysis in 2012 showed 49.0% and 90.3% of patients were adherent to statins in observational and randomized studies respectively after 1-year follow-up.[20] In comparison to conducted studies, relatively high level of adherence reported by patients in our study. This comparison is not rational because of heterogeneities of study population and method of adherence assessment between studies.
Likelihood of dumping unused medications by patients before pill counting falsely increases calculated adherence.[21] In addition, pills may be lost or stolen rather than taken which can affect pill count and consequently adherence measurement. However, pill count and self-report have some limitations that cause overestimation of adherence but significance of this result is that we could find a significant relationship between adherence measured by pill counting and LDL goal attainment. Significant association between adherence and clinical outcomes were also found in similar studies.[17,18,22]
Small percentage of our study population had reached LDL cholesterol <100 mg/dl (31.6%). It is similar to conducted studies reported overall 32-44% of patients with diabetes and dyslipidemia attained their LDL cholesterol level <100 mg/dl.[17,23] These findings show that in spite of the importance of statin therapy to decrease risk of CHD, the major proportion of patients receiving statin therapy did not achieve LDL cholesterol goal. It seems inadequate adherence to statin therapy yet remains the main reason of this failure in developing and also developed countries.
Inadequate adherence can be laid at many doors. Poly-pharmacy is common among patients with type 2 diabetes which implies to the prescription of oral hypoglycemic, antihypertensive and lipid-lowering medications for an individual. It is also a growing barrier to adherence and attainment of therapeutic goal.[24,25] In a similar manner, in our study nonadherent patients had more prescribed medications. In addition, limited time spent during office or clinic visits contributes to inadequate attention to multiple aspects of this care.[26]
It is necessary to increase awareness of the most important causes of non-adherence and find solutions to improve adherence.[5] Forgetting is one of the most frequent causes of non-adherence in patients with diabetes which also reported in our study, inasmuch as it has also been mentioned a barrier to insulin injection especially in patients with type 2 diabetes.[14,27]
Therefore the development of interventions such as using daily pill box or filling log books of daily medication use may be useful to improve adherence.[28] Another previous study also demonstrated an improvement of adherence and related outcomes in patients with type 2 diabetes by involving a pharmacist in the multidisciplinary team.[29] However, more studies will be needed to evaluate the effects of different interventions on adherence.[30] Prescribing adequate amount of statins between physicians’ visits is another solution to improve adherence. This makes patients sure of having enough available medications to use before physicians’ visit.
In addition, patient education and better interactions of patient and health care team will have the enormous effect on improving medication adherence. Another factor could influence on adherence was socioeconomic position including patients’ income. Although because of our local culture, we could not evaluate this factor but a recent cohort study showed a decrease in adherence with decreasing income in patients with established cardiovascular disease especially among men aged 40-64 years.[30] Therefore, other studies will be needed to focus on other risk indicators associated with non-adherence to statin medications with diabetes especially in developing countries.
There is controversy that increased medication adherence is associated with reduced healthcare expenses particularly during the years immediately following the onset of diabetes. However, medication adherence can improve health care outcome.[31,32] Therefore, education regarding adherence is necessary peculiarly for patients with low socioeconomic level.[32]
Adherence measurement, by using pharmacy record data about refilling prescription, may be easier and more precise than pill counting. Therefore the development of these systems is necessary in different setting of health care system. Finally, it should be mentioned pill count can be used to identify patients who are nonadherent to statin therapy and at high risk for failure to achieve LDL cholesterol goals.
CONCLUSION
Non-adherence to statins seems to be a significant issue in health care system for diabetic patients in Iran. Emphasis should be put on health care delivery systems and policy organizations to improve health care providers and patient alliance and promote clinical programs to enhance medication adherence.
Finding novel methods to improve adherence has giant potential to improve health outcomes and potentially decline health care costs. According to most probable barriers to adherence in our study, patient education and using pill boxes to decrease forgetting to take medication seems to be useful to increase adherence.
AUTHOR'S CONTRIBUTION
All authors contributed for the design, data collection, data analysis and manuscript preparation.
ACKNOWLEDGMENTS
This study was financially supported by the vice-chancellery for research and technology of the Isfahan University of Medical Sciences. Authors would like to thank all personnel of the Isfahan Endocrinology and Metabolism Research Center for their sincere help.
Footnotes
Source of Support: This study was financially supported by Isfahan University of Medical Sciences
Conflict of Interest: No conflict of interests.
REFERENCES
- 1.Esteghamati A, Etemad K, Koohpayehzadeh J, Abbasi M, Meysamie A, Noshad S, et al. Trends in the prevalence of diabetes and impaired fasting glucose in association with obesity in Iran: 2005-2011. Diabetes Res Clin Pract. 2014;103:319–27. doi: 10.1016/j.diabres.2013.12.034. [DOI] [PubMed] [Google Scholar]
- 2.Wannamethee SG, Shaper AG, Whincup PH, Lennon L, Sattar N. Impact of diabetes on cardiovascular disease risk and all-cause mortality in older men: Influence of age at onset, diabetes duration, and established and novel risk factors. Arch Intern Med. 2011;171:404–10. doi: 10.1001/archinternmed.2011.2. [DOI] [PubMed] [Google Scholar]
- 3.An J, Nichol MB. Multiple medication adherence and its effect on clinical outcomes among patients with comorbid type 2 diabetes and hypertension. Med Care. 2013;51:879–87. doi: 10.1097/MLR.0b013e31829fa8ed. [DOI] [PubMed] [Google Scholar]
- 4.Maningat P, Gordon BR, Breslow JL. How do we improve patient compliance and adherence to long-term statin therapy? Curr Atheroscler Rep. 2013;15:291. doi: 10.1007/s11883-012-0291-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bates TR, Connaughton VM, Watts GF. Non-adherence to statin therapy: A major challenge for preventive cardiology. Expert Opin Pharmacother. 2009;10:2973–85. doi: 10.1517/14656560903376186. [DOI] [PubMed] [Google Scholar]
- 6.Cheetham TC, Niu F, Green K, Scott RD, Derose SF, Vansomphone SS, et al. Primary nonadherence to statin medications in a managed care organization. J Manag Care Pharm. 2013;19:367–73. doi: 10.18553/jmcp.2013.19.5.367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kazerooni R, Watanabe JH, Bounthavong M. Association between statin adherence and cholesterol level reduction from baseline in a veteran population. Pharmacotherapy. 2013;33:1044–52. doi: 10.1002/phar.1305. [DOI] [PubMed] [Google Scholar]
- 8.Muntner P, Levitan EB, Brown TM, Sharma P, Zhao H, Bittner V, et al. Trends in the prevalence, awareness, treatment and control of high low density lipoprotein-cholesterol among United States adults from 1999-2000 through 2009-2010. Am J Cardiol. 2013;112:664–70. doi: 10.1016/j.amjcard.2013.04.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zhang R, Lee JY, Jean-Jacques M, Persell SD. Factors influencing the increasing disparity in LDL cholesterol control between white and black patients with diabetes in a context of active quality improvement. Am J Med Qual. 2013;12:12. doi: 10.1177/1062860613498112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Benner JS, Glynn RJ, Mogun H, Neumann PJ, Weinstein MC, Avorn J. Long-term persistence in use of statin therapy in elderly patients. JAMA. 2002;288:455–61. doi: 10.1001/jama.288.4.455. [DOI] [PubMed] [Google Scholar]
- 11.Sarayani A, Jahangard-Rafsanjani Z, Hadjibabaie M, Ahmadvand A, Javadi M, Gholami K. A comprehensive review of adherence to diabetes and cardiovascular medications in Iran; implications for practice and research. J Diabetes Metab Disord. 2013;12:57. doi: 10.1186/2251-6581-12-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Spence MM, Makarem AF, Reyes SL, Rosa LL, Nguyen C, Oyekan EA, et al. Evaluation of an outpatient pharmacy clinical services program on adherence and clinical outcomes among patients with diabetes and/or coronary artery disease. J Manag Care Pharm. 2014;20:1036–45. doi: 10.18553/jmcp.2014.20.10.1036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lee JK, Grace KA, Taylor AJ. Effect of a pharmacy care program on medication adherence and persistence, blood pressure, and low-density lipoprotein cholesterol: A randomized controlled trial. JAMA. 2006;296:2563–71. doi: 10.1001/jama.296.21.joc60162. [DOI] [PubMed] [Google Scholar]
- 14.Farsaei S, Sabzghabaee AM, Zargarzadeh AH, Amini M. Adherence to glyburide and metformin and associated factors in type 2 diabetes in Isfahan, Iran. Iran J Pharm Res. 2011;10:933–9. [PMC free article] [PubMed] [Google Scholar]
- 15.Khan AR, Al-Abdul Lateef ZN, Al Aithan MA, Bu-Khamseen MA, Al Ibrahim I, Khan SA. Factors contributing to non-compliance among diabetics attending primary health centers in the Al Hasa district of Saudi Arabia. J Family Community Med. 2012;19:26–32. doi: 10.4103/2230-8229.94008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Clifford S, Perez-Nieves M, Skalicky AM, Reaney M, Coyne KS. A systematic literature review of methodologies used to assess medication adherence in patients with diabetes. Curr Med Res Opin. 2014;30:1071–85. doi: 10.1185/03007995.2014.884491. [DOI] [PubMed] [Google Scholar]
- 17.Parris ES, Lawrence DB, Mohn LA, Long LB. Adherence to statin therapy and LDL cholesterol goal attainment by patients with diabetes and dyslipidemia. Diabetes Care. 2005;28:595–9. doi: 10.2337/diacare.28.3.595. [DOI] [PubMed] [Google Scholar]
- 18.Pittman DG, Chen W, Bowlin SJ, Foody JM. Adherence to statins, subsequent healthcare costs, and cardiovascular hospitalizations. Am J Cardiol. 2011;107:1662–6. doi: 10.1016/j.amjcard.2011.01.052. [DOI] [PubMed] [Google Scholar]
- 19.Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in elderly patients with and without acute coronary syndromes. JAMA. 2002;288:462–7. doi: 10.1001/jama.288.4.462. [DOI] [PubMed] [Google Scholar]
- 20.Lemstra M, Blackburn D, Crawley A, Fung R. Proportion and risk indicators of nonadherence to statin therapy: A meta-analysis. Can J Cardiol. 2012;28:574–80. doi: 10.1016/j.cjca.2012.05.007. [DOI] [PubMed] [Google Scholar]
- 21.Thompson N, Nazir N, Cox LS, Faseru B, Goggin K, Ahluwalia JS, et al. Unannounced telephone pill counts for assessing varenicline adherence in a pilot clinical trial. Patient Prefer Adherence. 2011;5:475–82. doi: 10.2147/PPA.S24023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Al-Hayek AA, Robert AA, Alzaid AA, Nusair HM, Zbaidi NS, Al-Eithan MH, et al. Association between diabetes self-care, medication adherence, anxiety, depression, and glycemic control in type 2 diabetes. Saudi Med J. 2012;33:681–3. [PubMed] [Google Scholar]
- 23.Beaton SJ, Nag SS, Gunter MJ, Gleeson JM, Sajjan SS, Alexander CM. Adequacy of glycemic, lipid, and blood pressure management for patients with diabetes in a managed care setting. Diabetes Care. 2004;27:694–8. doi: 10.2337/diacare.27.3.694. [DOI] [PubMed] [Google Scholar]
- 24.Hosokawa M, Hamasaki A, Nagashima K, Harashima S, Toyoda K, Fujita Y, et al. Lack of goal attainment regarding the low-density lipoprotein cholesterol level in the management of type 2 diabetes mellitus. Intern Med. 2013;52:2409–15. doi: 10.2169/internalmedicine.52.0599. [DOI] [PubMed] [Google Scholar]
- 25.Kulkarni SP, Alexander KP, Lytle B, Heiss G, Peterson ED. Long-term adherence with cardiovascular drug regimens. Am Heart J. 2006;151:185–91. doi: 10.1016/j.ahj.2005.02.038. [DOI] [PubMed] [Google Scholar]
- 26.Woodard LD, Landrum CR, Urech TH, Wang D, Virani SS, Petersen LA. Impact of clinical complexity on the quality of diabetes care. Am J Manag Care. 2012;18:508–14. [PMC free article] [PubMed] [Google Scholar]
- 27.Farsaei S, Radfar M, Heydari Z, Abbasi F, Qorbani M. Insulin adherence in patients with diabetes: Risk factors for injection omission. Prim Care Diabetes. 2014;8:338–45. doi: 10.1016/j.pcd.2014.03.001. [DOI] [PubMed] [Google Scholar]
- 28.Farsaei S, Sabzghabaee A, Zargarzadeh A, Amini M. Adherence to oral hypoglycemic medication in type 2 diabetic patients in Isfahan, Iran: Prevalence and barriers to adherence. Pharm World Sci. 2010;32:677–77. [Google Scholar]
- 29.Farsaei S, Sabzghabaee AM, Zargarzadeh AH, Amini M. Effect of pharmacist-led patient education on glycemic control of type 2 diabetics: A randomized controlled trial. J Res Med Sci. 2011;16:43–9. [PMC free article] [PubMed] [Google Scholar]
- 30.Wallach-Kildemoes H, Andersen M, Diderichsen F, Lange T. Adherence to preventive statin therapy according to socioeconomic position. Eur J Clin Pharmacol. 2013;69:1553–63. doi: 10.1007/s00228-013-1488-6. [DOI] [PubMed] [Google Scholar]
- 31.Cheng SH, Chen CC, Tseng CH. Does medication adherence lead to lower healthcare expenses for patients with diabetes? Am J Manag Care. 2013;19:662–70. [PubMed] [Google Scholar]
- 32.Bitton A, Choudhry NK, Matlin OS, Swanton K, Shrank WH. The impact of medication adherence on coronary artery disease costs and outcomes: A systematic review. Am J Med. 2013;126:357.e7–357.e27. doi: 10.1016/j.amjmed.2012.09.004. [DOI] [PubMed] [Google Scholar]