

Abstract
Background:
The most common drug abuse among athletes is anabolic steroids which lead to the development of cardiovascular diseases and sudden death. Thus, the aim of this study was to evaluate cardiovascular outcomes of anabolic consumption in body building athletes.
Materials and Methods:
Totally, 267 male athletes at the range of 20-45 years old with the regular consumption of anabolic steroids for >2 months with at least once weekly. High-density lipoprotein (HDL), low-density lipoprotein (LDL), triglyceride (TG), and hematocrit (Hct) levels were measured after 10 h of fasting. Data analysis was performed using K2, t-test, ANOVA and correlation coefficient through SPSS 17.
Results:
There was a nonsignificant difference between groups regarding HDL, TG, and total cholesterol. There was a significant decrease in the total and categorized LDL and Hct levels in consumers of anabolic steroid versus nonusers (P = 0.01 and P = 0.041, respectively). Results showed a significant increase in systolic and diastolic blood pressure (SBP and DBP) in anabolic steroid users which associates with duration of abuse (P = 0.02 and P = 0.03, respectively). No significant electrocardiography changes were found within the follow-up period.
Conclusion:
Increase in SBP or DBP is a common complication of these drugs which can lead serious vascular disorders. The lower LDL cholesterol level might be due to the higher amounts of lipid consumption in these athletes.
Keywords: Anabolic steroids, body building, cardiovascular, complication, dyslipidemia, hypertension, lipid index
INTRODUCTION
Drug abuse and its related side effects are common apprehensions of physician's councils and sport federations. Delivered statistical reports from laboratory of international committees implies that the most common drug abuse among athletes are anabolic steroids which leads to the development of dangerous side effects as cardiovascular diseases (CVD) and sudden death in athletes. Anabolic steroids are a family of hormones derived from testosterone which exert both anabolic and androgen properties which were originally developed in the late 1930s.[1] All major professional sports organizations ban the use of anabolic steroids. Almost all side effects of anabolic steroids are related to their androgen properties.[2,3,4] There is a tremendous effort to enhance anabolic to androgen ratio of these steroids as much as possible.
Anabolic steroids are applicable through oral, injection, and dermal routes according to their molecular structure. General side effects of these agents are CVD, testicular atrophy, increased libido, hepatic disorders, psychological problems, and so on.[5,6] Although Cardiovascular side effects are among the most threatening side effects of anabolic steroids which might manifest later in life but The prevalence and underlying mechanisms of Anabolic steroid-induced cardiovascular toxicity remain poorly understood. Electrocardiography (ECG) abnormalities as left ventricular hypertrophy (LVH) and arrhythmia are common in these cases. The risk of coronary thrombosis and myocardial infarction is also noticeable in this population.[7,8,9,10]
As taking anabolic steroids are common in many body building clubs in our province, and there are no comprehensive data regarding side effects of anabolic steroids this study evaluated the association between occurrence of CVD and anabolic steroid consumption in athletes.
MATERIALS AND METHODS
This case-control study was performed from 2013 to 2014 and includes 267 male athletes at the range of 20-45 years old with the regular consumption of anabolic steroids for more than 2 months. This study was performed in Isfahan Legal medicine, Isfahan, Iran. Case group include 219 male bodybuilders using anabolic steroids regularly for more than two menthes, and control group were 48 age-matched subjects volunteered for this study without consumption of anabolic steroid. Participants were counseled as to the hazardous health effects associated with the use of exogenous androgens and informed that they were free to withdraw from the study at any time. Subjects provided written informed consent. Exclusion criteria include diabetes mellitus, hepatic disorders, abnormally elevated liver enzymes, hyperlipidemia, cigarette smoking, and pre-existing cardiac disorder. All volunteer participants signed informed consent forms. High-density lipoprotein (HDL), low-density lipoprotein (LDL), triglyceride (TG), and hematocrit (Hct) levels were measured. Lipid profile was evaluated after 10 h of fasting. LDL and Hct were evaluated in divided groups as LDL (group I: LDL <100, group 2: 100 < LDL <160 and group 3: LDL >160) and Hct (group I: Hct <39, group 2: 40< Hct <52 and group 3: LDL >52).[11,12] ECG was also taken. All participants filled questioners. All of these variables were checked out before and after steroid consumption. For assessing blood pressure, after a resting period of 5 min in the supine position, systolic and diastolic blood pressure (SBP and DBP) were measured with a sphygmomanometer.[13] Data are expressed as mean ± standard deviation data analysis was performed using K2, t-test, ANOVA, and correlation coefficient through Statistical Package for the Social Sciences version 17.0 (SPSS Inc, Chicago, IL, USA).
RESULTS
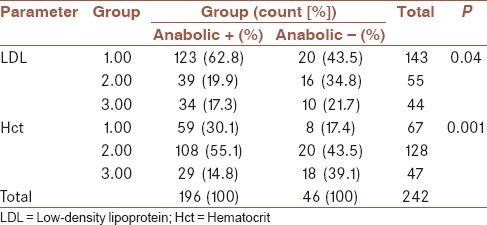
Participants were matched regarding age and duration of drug abuse. The mean value of age of participants in anabolic positive and negative group was 28.37 ± 4.86 and 29.65 ± 7.19, respectively, which shows a nonsignificant relationship between groups (P > 0.05). Education level of participants in groups shows a nonsignificant difference between groups. The mean value of HDL, LDL, and Hct measures of participants are included in Tables 1, which shows a nonsignificant difference between groups. There was a significant decrease in the total and categorized LDL and Hct levels in consumers of anabolic steroid versus nonusers (0.01 and 0.041, respectively) [Table 2]. There was no correlation between duration of consumption and LDL increase.
Table 1.
The mean value of HDL, LDL, TG, and Hct in anabolic positive and negative group
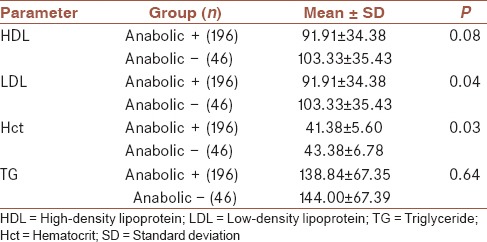
Table 2.
The mean value of categorized LDL and Hct in anabolic positive and negative group
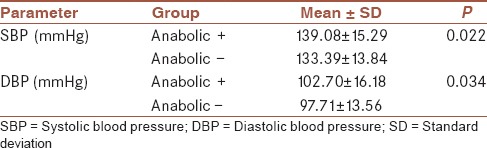
Comparing mean SBP and DBP in case and control groups of our study revealed that abusing anabolic steroids may elevate both SBP and DBP significantly (0.02 and 0.001, respectively) and the amount of increase correlates with duration of abuse. Meaning that the much longer anabolic steroid abused, the higher SBP and DBP rises (0.027 and 0.016, respectively) [Table 3]. Furthermore, analyzes showed that among anabolic consumers, 70% of subjects were categorized in hypertensive level (stage 1 and 2), while in the control group 35% suffered from hypertension (data not shown). No ECG changes were found within the follow-up period except occurrence of LVH in one case.
Table 3.
The mean value of SBP and DBP in anabolic positive and negative group
DISCUSSION
Anabolic androgenic steroids are associated with direct effects such as cardiac muscle hypertrophy and myocardial fibrosis and indirect effects, including dyslipidemia, hypertension, arrhythmia, and myocardial infarction. It is likely that chronic exposure to these agents can result in significant alterations in the cardiovascular system, and their safety has not been fully established.[14]
One of the main findings of our investigation was finding an association between steroid consumption and changes in lipid profile. Steroid abuse was not associated with altered HDL, TG, total cholesterol level and ECG abnormalities. A 20% increase in LDL plasma level and 20-70% decrease in HDL plasma level have been reported using anabolic steroid consumption.[7,15] We have found a significant association between anabolic steroid consumption and mean plasma level of LDL. We observed a decrease in mean plasma level of LDL. Interestingly, this finding is in contrast with previously reported findings. This might be due to the higher energy consumption consequent to the higher activity following anabolic steroid consumption. But we have not observed any significant decline in mean HDL plasma level, in which this finding is not in parallel with our finding. No change in TG and total cholesterol has been demonstrated by Hartgens et al. using consumption of anabolic steroids.[16]
The relation between anabolic steroid abuse and blood pressure is controversial. A link between anabolic steroid abuse and increase in blood pressure has been reported majority of related studies.[17,18,19,20] Whereas some others have shown no association.[21,22,23,24] Our results support the first hypothesis, indicating that anabolic steroids increase SBP and DBP and the amount of increase are associated with duration of abuse. The definite mechanism by which anabolic steroid increase blood pressure is not clear, but it has been suggested that overproduction of 11-β-deoxycorticosterone by adrenal cortex may be responsible. In addition, androgens may also increase renal renin secretion resulting blood pressure increase.[25]
Electrocardiography abnormalities as LVH and arrhythmia were also reported using anabolic steroid consumption,[7,8,9,10] but surprisingly, no ECG abnormalities have been seen in our survey. An increase in the mean value of Hct with a significant difference between drug users and nonusers is in accordance with previous findings. This polycythemia has been attributed to the androgenic entity of these agents.
In our survey, we did not observe decreased HDL, altered TG/total cholesterol or sudden cardiac death. But we did not follow up cases for development of CVD.
AUTHOR'S CONTRIBUTION
FGH contributed in the conception of the work, clinical studies, literature search, data acquisition, conducting the study, and agreed for all aspects of the work. MRPA contributed in the conception of the work, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work. GRM contributed in the conception of the work, agreed for all aspects of the work. MB contributed in the conception of the work, conducting the study, revising the draft, approval of the final version of the manuscript and agreed for all aspects of the work. PP contributed in the conception and design of the work, revising the draft, approval of the final version of the manuscript, conducting the study, data acquisition and agreed for all aspects of the work.
ACKNOWLEDGMENT
This research was financially supported by Isfahan Clinical Toxicology Research Center, Isfahan University of Medical Sciences, Isfahan, Iran (Project No. 290224).
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Hoberman JM, Yesalis CE. The history of synthetic testosterone. Sci Am. 1995;272:76–81. doi: 10.1038/scientificamerican0295-76. [DOI] [PubMed] [Google Scholar]
- 2.Kopera H. The history of anabolic steroids and a review of clinical experience with anabolic steroids. Acta Endocrinol Suppl (Copenh) 1985;271:11–8. doi: 10.1530/acta.0.109s00011. [DOI] [PubMed] [Google Scholar]
- 3.Pope H, Brower K. Anabolic-androgenic steroid abuse. In: Sadock B, Sadock V, editors. Comprehensive Textbook of Psychiatry. Philadelphia, PA: Lippincott Williams & Wilkins; 2005. pp. 1318–28. [Google Scholar]
- 4.Sheffield-Moore M, Urban RJ. An overview of the endocrinology of skeletal muscle. Trends Endocrinol Metab. 2004;15:110–5. doi: 10.1016/j.tem.2004.02.009. [DOI] [PubMed] [Google Scholar]
- 5.O’Sullivan AJ, Kennedy MC, Casey JH, Day RO, Corrigan B, Wodak AD. Anabolic-androgenic steroids: Medical assessment of present, past and potential users. Med J Aust. 2000;173:323–7. doi: 10.5694/j.1326-5377.2000.tb125667.x. [DOI] [PubMed] [Google Scholar]
- 6.Evans NA. Gym and tonic: A profile of 100 male steroid users. Br J Sports Med. 1997;31:54–8. doi: 10.1136/bjsm.31.1.54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sader MA, Griffiths KA, McCredie RJ, Handelsman DJ, Celermajer DS. Androgenic anabolic steroids and arterial structure and function in male bodybuilders. J Am Coll Cardiol. 2001;37:224–30. doi: 10.1016/s0735-1097(00)01083-4. [DOI] [PubMed] [Google Scholar]
- 8.Dickerman RD, Schaller F, Zachariah NY, McConathy WJ. Left ventricular size and function in elite bodybuilders using anabolic steroids. Clin J Sport Med. 1997;7:90–3. doi: 10.1097/00042752-199704000-00003. [DOI] [PubMed] [Google Scholar]
- 9.Severo CB, Ribeiro JP, Umpierre D, Da Silveira AD, Padilha MC, De Aquino Neto FR, et al. Increased atherothrombotic markers and endothelial dysfunction in steroid users. Eur J Prev Cardiol. 2013;20:195–201. doi: 10.1177/2047487312437062. [DOI] [PubMed] [Google Scholar]
- 10.Angell P, Chester N, Green D, Somauroo J, Whyte G, George K. Anabolic steroids and cardiovascular risk. Sports Med. 2012;42:119–34. doi: 10.2165/11598060-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 11.National Institutes of Health; National Heart Lung, and Blood Institute; 2002 National Cholesterol Education Program. Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III): Final Report. NIH Publication No. 02-5215; September. 2002 [Google Scholar]
- 12.McMullin MF, Bareford D, Campbell P, Green AR, Harrison C, Hunt B, et al. Guidelines for the diagnosis, investigation and management of polycythaemia/erythrocytosis. Br J Haematol. 2005;130:174–95. doi: 10.1111/j.1365-2141.2005.05535.x. [DOI] [PubMed] [Google Scholar]
- 13.The 1988 report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure. Arch Intern Med. 1988;148:1023–38. [PubMed] [Google Scholar]
- 14.Higgins JP, Heshmat A, Higgins CL. Androgen abuse and increased cardiac risk. South Med J. 2012;105:670–4. doi: 10.1097/SMJ.0b013e3182749269. [DOI] [PubMed] [Google Scholar]
- 15.Lenders JW, Demacker PN, Vos JA, Jansen PL, Hoitsma AJ, van’t Laar A, et al. Deleterious effects of anabolic steroids on serum lipoproteins, blood pressure, and liver function in amateur body builders. Int J Sports Med. 1988;9:19–23. doi: 10.1055/s-2007-1024972. [DOI] [PubMed] [Google Scholar]
- 16.Hartgens F, Rietjens G, Keizer HA, Kuipers H, Wolffenbuttel BH. Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein (a) Br J Sports Med. 2004;38:253–9. doi: 10.1136/bjsm.2003.000199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Santos MA, Oliveira CV, Silva AS. Adverse cardiovascular effects from the use of anabolic-androgenic steroids as ergogenic resources. Subst Use Misuse. 2014;49:1132–7. doi: 10.3109/10826084.2014.903751. [DOI] [PubMed] [Google Scholar]
- 18.Urhausen A, Albers T, Kindermann W. Are the cardiac effects of anabolic steroid abuse in strength athletes reversible? Heart. 2004;90:496–501. doi: 10.1136/hrt.2003.015719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Di Bello V, Giorgi D, Bianchi M, Bertini A, Caputo MT, Valenti G, et al. Effects of anabolic-androgenic steroids on weight-lifters’ myocardium: An ultrasonic videodensitometric study. Med Sci Sports Exerc. 1999;31:514–21. doi: 10.1097/00005768-199904000-00004. [DOI] [PubMed] [Google Scholar]
- 20.Riebe D, Fernhall B, Thompson PD. The blood pressure response to exercise in anabolic steroid users. Med Sci Sports Exerc. 1992;24:633–7. [PubMed] [Google Scholar]
- 21.Krieg A, Scharhag J, Albers T, Kindermann W, Urhausen A. Cardiac tissue Doppler in steroid users. Int J Sports Med. 2007;28:638–43. doi: 10.1055/s-2007-964848. [DOI] [PubMed] [Google Scholar]
- 22.Nottin S, Nguyen LD, Terbah M, Obert P. Cardiovascular effects of androgenic anabolic steroids in male bodybuilders determined by tissue Doppler imaging. Am J Cardiol. 2006;97:912–5. doi: 10.1016/j.amjcard.2005.10.026. [DOI] [PubMed] [Google Scholar]
- 23.D’Andrea A, Caso P, Salerno G, Scarafile R, De Corato G, Mita C, et al. Left ventricular early myocardial dysfunction after chronic misuse of anabolic androgenic steroids: A Doppler myocardial and strain imaging analysis. Br J Sports Med. 2007;41:149–55. doi: 10.1136/bjsm.2006.030171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lane HA, Grace F, Smith JC, Morris K, Cockcroft J, Scanlon MF, et al. Impaired vasoreactivity in bodybuilders using androgenic anabolic steroids. Eur J Clin Invest. 2006;36:483–8. doi: 10.1111/j.1365-2362.2006.01667.x. [DOI] [PubMed] [Google Scholar]
- 25.Kuipers H, Wijnen JA, Hartgens F, Willems SM. Influence of anabolic steroids on body composition, blood pressure, lipid profile and liver functions in body builders. Int J Sports Med. 1991;12:413–8. doi: 10.1055/s-2007-1024704. [DOI] [PubMed] [Google Scholar]