

Abstract
Situs inversus totalis (SIT) is a rare congenital condition in which the abdominal and thoracic organs are on the opposite sides to their normal anatomic positions. Reports of laparoscopic surgery for colorectal cancer with SIT are very few. Due to the mirror-image transposition of organs and vascular abnormalities, laparoscopic surgery for patients with SIT is technically complicated. Therefore, it has been reported as easier for left-handed surgeons. This report presents that operative procedures can be conducted as usual by changing the positions of the operator and assistants, even if the operator is right-handed. A 71-year-old woman visited our hospital with a 2-month history of hematochezia. Colonoscopy revealed an ulcerative tumor in the sigmoid colon and biopsy confirmed well-differentiated adenocarcinoma. Laparoscopic sigmoidectomy radical lymphadenectomy was performed. The operating time was 189 minutes and blood loss was 13 mL. The patient was discharged on postoperative day 7, without any complications. We report that complicated surgical procedures for patients with SIT can be simplified by changing viewpoints. Due to the altered anatomy in SIT, the positions of the operator and assistants are very important. Location of the pelvis is almost the same as in orthotopic patients, by moving the operator from the left side to the right side of the patient. Changing the position of the operator to the right side seems to be effective for patients with SIT during pelvic procedures.
Key words: Laparoscopic sigmoidectomy, Laparoscopic surgery, Situs inversus totalis, Colon cancer
Situs inversus is a rare autosomal recessive disorder in which organs are transposed from the normal anatomic location to the opposite side of the body. When both abdominal and thoracic viscera are involved, including dextrocardia, this situation is referred to as situs inversus totalis (SIT). Due to the mirror-image transposition of organs and vascular abnormalities, surgical procedures for patients with SIT become technically more complicated, particularly for cases involving laparoscopic surgery. Few reports have described laparoscopic surgery in patients with SIT, and the majority of those have involved laparoscopic cholecystectomy.1,2 Including the present case, only 5 cases of laparoscopic surgery for colorectal malignancy have been reported.3–6 This report is the first in the English literature to describe laparoscopic sigmoidectomy for sigmoid colon cancer in a patient with SIT. Laparoscopic sigmoidectomy was safely completed in this case using the usual operative procedure.
Case Report
A 71-year-old woman visited our hospital with a 2-month history of hematochezia. Colonoscopy revealed an ulcerative tumor in the sigmoid colon, 30 cm from the anal verge. Biopsy confirmed well-differentiated adenocarcinoma. She was referred to our hospital for further evaluation and surgical treatment. She was 153 cm tall and weighed 50.5 kg. Appendectomy had been performed at 19 years old, and caesarean sections at 33 and 35 years old. Abdominal examination revealed scars in the lower midline and left lower quadrant. Laboratory examination confirmed no anemia (red blood cell count, 422 × 104/mm2; hemoglobin, 11.1 g/dL; hematocrit, 34.6%), or hepatic, renal, and electrolyte dysfunction. Serum carcinoembryonic antigen level was not elevated (4.3 ng/mL; reference range, 0–5 ng/mL).
Chest radiography showed dextrocardia (Fig. 1). Abdominal computed tomography (CT) revealed complete transposition of the abdominal viscera, confirming SIT. Furthermore, the inferior mesenteric artery was located on the right side on CT angiography. CT colonography and colonoscopy showed an ulcerated lesion in the sigmoid colon (Fig. 2).
Fig. 1.
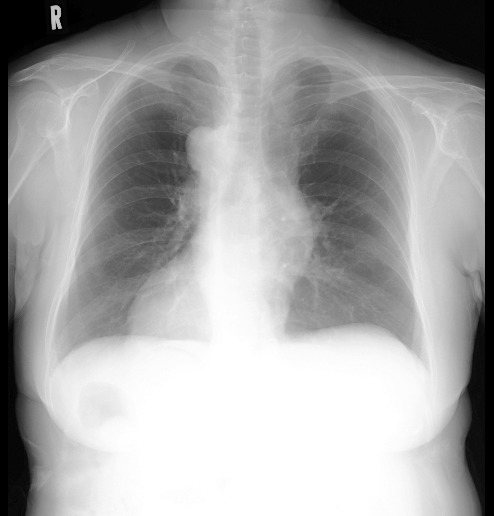
Chest radiography showing dextrocardia.
Fig. 2.

Preoperative images. (a) Abdominal computed tomography (CT) shows inversion of the abdominal viscera, with the liver on the left and spleen on the right. (b) Three-dimensional CT angiography shows the inferior mesenteric artery located on the right side. (c) CT colonography shows an ulcerated lesion in the sigmoid colon.
Based on these findings, laparoscopic sigmoidectomy with radical lymphadenectomy was performed. After inducing general anesthesia, the patient was placed in a modified lithotomy position. The operator and endoscopist were situated on the left, and the first assistant on the right, the reverse of locations for orthotopic patients. Sigmoidectomy was performed laparoscopically using 5 trocars: a 12-mm supra-umbilical trocar for the camera placed using the Hasson technique; a 12-mm trocar in the right iliac fossa as a working port and for the introduction of the laparoscopic Echelon; a 5-mm trocar in the right flank for traction; and 2 other 5-mm trocars in the left iliac fossa and flank as working ports (Fig. 3). Abdominal air pressure was set at 10 mmHg. A flexible camera was introduced into the peritoneal cavity. The sigmoid colon, as expected, was noted to be on the right side along with the spleen. The liver was in the left upper quadrant. A tumor was observed in the sigmoid colon on the right side. The sigmoid and descending colons were mobilized using ultrasonic dissection (Harmonic Scalpel II, Ethicon Endo-Surgery, Cincinnati, Ohio). The right ureter was clearly identified and avoided during dissection. The inferior mesenteric artery and vein were isolated and divided using endoscopic vascular clips (Fig. 4a). The operator then moved to the right with the first assistant on the left to mobilize the sigmoid-rectum and form the anastomosis, because the operator was right-handed and the location of the rectum was the same as that in orthotopic patients. The distal rectosigmoid colon was divided using an articulating endoscopic linear stapler (Powered Echelon Flex Endopath Stapler, Ethicon Endo-Surgery; Fig. 4b). Using a longitudinal incision of about 4 cm at the supra-umbilical trocar site, the specimen was extracted and resected. A purse-string suture was used to hold the anvil of a circular stapling device in the proximal colon. The colon was then returned to the abdomen, and the abdominal incision was closed. After restoring pneumoperitoneum, a 29-mm end-to-end anastomotic stapling device (CDH29, Ethicon Endo-Surgery) was inserted anally, and the anastomosis was completed (Fig. 4c). Total operating time was 189 min, and the volume of blood loss was 13 mL.
Fig. 3.
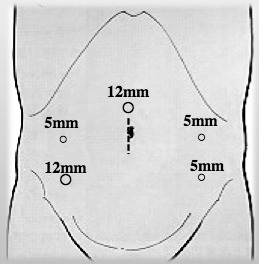
Trocar placement for laparoscopic sigmoidectomy in patients with situs inversus totalis (SIT).
Fig. 4.

Intraoperative findings. (a) Division of the inferior mesenteric artery at its origin. (b) The distal rectosigmoid is divided using an articulating endoscopic linear stapler. (c) Intracorporeal anastomosis using the end-to-end anastomotic stapler.
According to the Japanese classification of colorectal carcinoma,7 macroscopically, the tumor was a 25 × 23-mm type 2 lesion in the sigmoid colon. Histologic examination of the resected specimen identified moderately differentiated adenocarcinoma (type 2, pSS, pN0, LN 0/18, sH0, sP0, cM0, ly1, v0, pStage II). The patient was started on a clear liquid diet on postoperative day 1. Medical therapy was offered and movement encouraged from postoperative day 1. No intra- or perioperative complications were encountered. The patient was discharged on postoperative day 7 and experienced no postoperative complications.
Discussion
SIT is a rare congenital condition in which the structures of the abdominal and thoracic cavities are in completely opposite positions to normal. The incidence of SIT is 1 per 5000 to 20,000 people.8 Cardiac and intestinal malformations, as well as other visceral and vascular anomalies that can be associated with SIT, follow variable patterns.9
To safely perform laparoscopic surgery, careful assessment of the anatomy using preoperative imaging is vitally important. CT angiography and CT colonography are useful for clarifying the anatomy and allowing preoperative planning of laparoscopic procedures. In our institution, laparoscopic surgery of the sigmoid colon and rectum are always performed using 5 ports. In the present case, the positions of the operator and assistants were reversed from those used for orthotopic patients, but trocars did not differ from the usual locations. Though the operator in this case was right-handed, the procedure for ligation of the vascular pedicle through the left flank trocar did not prove onerous. Resection and anastomosis were likewise performed without much difficulty. This was because the position of the right-handed operator had been reversed with those of the assistants, enabling the operator to continuously maintain the same field of vision and conduct the operative procedures almost as usual. Sigmoid dissection and division, and the anastomotic procedure were all able to be performed with the right hand through a 12-mm trocar in the right iliac fossa. Oms and Badia10 reported a potential advantage for left-handed operators during laparoscopic procedure in patients with SIT. It is surely obvious that left-handed operations are important to surgical procedures in laparoscopic surgery; however, being a right-handed operator is not disadvantageous if the positions are changed. Choi et al11 suggested that laparoscopic abdominoperineal resection could be safely performed in a patient with SIT by moving the surgeon. Because the view of the rectum is almost the same in SIT as in orthotopic patients, in surgeries of the rectum from the sigmoid colon, changing the position of the operator to the right side seems to be very effective during pelvic procedures.
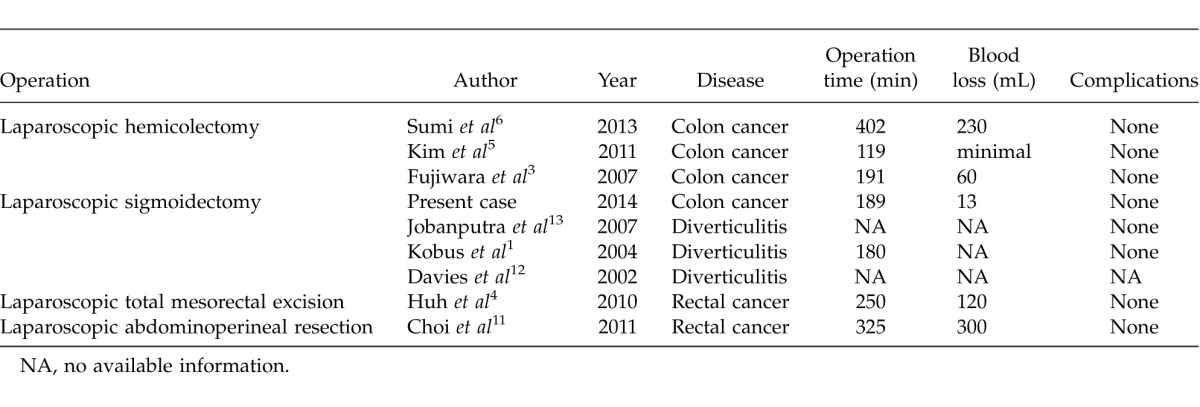
Most reports of laparoscopic surgery in patients with SIT have involved cholecystectomy. A review of the English literature showed that laparoscopic colectomy has only been reported in 8 patients with SIT (Table 1).1,3–6,11–13 No complications were reported with those cases or our own case.
Table 1.
Reports of laparoscopic colorectal surgery for situs inversus totalis in the English literature
In conclusion, laparoscopic surgery represents a technical challenge for the surgeon, but remains a good option for patients with SIT. Laparoscopic colectomy should not be considered a contraindicated surgery for patients with SIT. If care is taken to understand the mirror-image anatomy and preoperatively plan laparoscopic procedures, patients with SIT should achieve the full benefits of minimally invasive surgery.
Acknowledgments
The authors declare no conflicts of interest. The authors thank the patient and all support staff at the Department of Surgery, Iwate Prefectural Ninohe Hospital.
References
- 1.Kobus C, Targarona EM, Bendahan GE, Alonso V, Balague C, Vela S, et al. Laparoscopic surgery in situs inversus: a literature review and a report of laparoscopic sigmoidectomy for diverticulitis in situs inversus. Langenbecks Arch Surg. 2004;389(5):396–399. doi: 10.1007/s00423-004-0500-0. [DOI] [PubMed] [Google Scholar]
- 2.Machado NO, Chopra P. Laparoscopic cholecystectomy in a patient with situs inversus totalis: feasibility and technical difficulties. JSLS. 2006;10(3):386–391. [PMC free article] [PubMed] [Google Scholar]
- 3.Fujiwara Y, Fukunaga Y, Higashino M, Tanimura S, Takemura M, Tanaka Y, et al. Laparoscopic hemicolectomy in a patient with situs inversus totalis. World J Gastroenterol. 2007;13(37):5035–5037. doi: 10.3748/wjg.v13.i37.5035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Huh JW, Kim HR, Cho SH, Kim CY, Kim HJ, Joo JK, et al. Laparoscopic total mesorectal excision in a rectal cancer patient with situs inversus totalis. J Korean Med Sci. 2010;25(5):790–793. doi: 10.3346/jkms.2010.25.5.790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kim HJ, Choi GS, Park JS, Lim KH, Jang YS, Park SY, et al. Laparoscopic right hemicolectomy with D3 lymph node dissection for a patient with situs inversus totalis: report of a case. Surg Today. 2011;41(11):1538–1542. doi: 10.1007/s00595-010-4530-7. [DOI] [PubMed] [Google Scholar]
- 6.Sumi Y, Tomono A, Suzuki S, Kuroda D, Kakeji Y. Laparoscopic hemicolectomy in a patient with situs inversus totalis after open distal gastrectomy. World J Gastrointest Surg. 2013;5(2):22–26. doi: 10.4240/wjgs.v5.i2.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Japanese Society for Cancer of the Colon and Rectum. Japanese Classification of Colorectal Carcinoma. 7th ed. Tokyo: Kanehara and Co; 2009. [Google Scholar]
- 8.Nursal TZ, Baykal A, Iret D, Aran O. Laparoscopic cholecystectomy in a patient with situs inversus totalis. J Laparoendosc Adv Surg Tech A. 2001;11(4):239–241. doi: 10.1089/109264201750539772. [DOI] [PubMed] [Google Scholar]
- 9.Iwamura T, Shibata N, Haraguchi Y, Hisashi Y, Nishikawa T, Yamada H, et al. Synchronous double cancer of the stomach and rectum with situs inversus totalis and polysplenia syndrome. J Clin Gastroenterol. 2001;33(2):148–153. doi: 10.1097/00004836-200108000-00012. [DOI] [PubMed] [Google Scholar]
- 10.Oms LM, Badia JM. Laparoscopic cholecystectomy in situs inversus totalis: the importance of being left-handed. Surg Endosc. 2003;17(11):1859–1861. doi: 10.1007/s00464-003-9051-7. [DOI] [PubMed] [Google Scholar]
- 11.Choi SI, Park SJ, Kang BM, Lee KY, Lee HC, Lee SH, et al. Laparoscopic abdominoperineal resection for rectal cancer in a patient with situs inversus totalis. Surg Laparosc Endosc Percutan Tech. 2011;21(2):e87–90. doi: 10.1097/SLE.0b013e31820b0258. [DOI] [PubMed] [Google Scholar]
- 12.Davies H, Slater GH, Bailey M. Laparoscopic sigmoid colectomy for diverticular disease in a patient with situs inversus. Surg Endosc. 2003;17(1):160–161. doi: 10.1007/s00464-002-4231-4. [DOI] [PubMed] [Google Scholar]
- 13.Jobanputra S, Safar B, Wexner SD. Laparoscopic diverticular resection with situs inversus totalis (SIT): report of a case. Surg Innov. 2007;14(4):284–286. doi: 10.1177/1553350607311089. [DOI] [PubMed] [Google Scholar]