

Abstract
Duplication of the appendix is a rare congenital anomaly that, in adults, is most often found incidentally during surgery for other reasons. Appendicitis in the duplicated appendix is very rare and has been reported less than 10 times in the medical literature. We describe a 33-year-old woman with worsening periumbilical pain, nausea, vomiting, and fever. Physical examination showed localized peritonitis in the right lower quadrant. She had an elevated white blood cell count with neutrophilia. Computed tomography showed acute ruptured appendicitis. Diagnostic laparoscopy showed 2 appendices attached via separate bases to a single cecum with no other concurrent anomalies. Both appendices were removed laparoscopically. Histopathology confirmed normal appendiceal tissue in one and severe acute transmural appendicitis in the other. Awareness of appendiceal duplication and a thorough intraoperative inspection are critical to assess the presence of significant associated anomalies and avoid life-threatening complications.
Key words: Ruptured appendicitis, Appendiceal duplication, Acute abdomen, Cave-Wallbridge classification
Acute appendicitis is one of the most common causes of emergent abdominal surgery in the United States (US).1 The lifetime risk for acute appendicitis is 8.6% in males and 6.7% in females in the US.2 Anatomic anomalies complicating its diagnosis and management are rare. The anomalies known to complicate management include high-lying appendix, malrotation, situs inversus, and the duplication of hindgut structures, including the cecum and appendix. Less than 100 appendiceal duplications have been documented in the literature to date,3 of which less than 15 are cases complicated by acute appendicitis, including the case we present herein.
Case Report
A 33-year-old African-American female presented to the Emergency Department with migratory right lower quadrant pain of 4 days duration associated with nausea and vomiting. Clinical evaluation showed that she was febrile and had a tender right lower quadrant with rebound tenderness and guarding. Her white blood cell count was elevated with neutrophilia. Computed tomography scan of the abdomen showed possible acute appendicitis with perforation and purulent fluid collection in the pelvis. Diagnostic laparoscopy revealed 2 appendices attached via separate bases to 1 cecum. The anterior appendix was inflamed with a gangrenous tip while the posterior appendix was grossly normal (Fig. 1). Both appendices were located on the taenia-coli. No other intra-abdominal anomalies were discovered. Subsequently an emergent laparoscopic appendectomy was performed. Histopathology confirmed normal appendiceal tissue in one specimen and severe acute transmural appendicitis in the other (Fig. 2). There were no postoperative complications. The patient was discharged home in stable condition after 3 days in the hospital.
Fig. 1.

Normal appearing appendix (specimen A on top); inflamed appendix with congested surface, fibrinopurulent exudate on serosa, and prominent vessels (specimen B on bottom).
Fig. 2.

Histologic sections of appendices. (Left) Specimen A normal appendicular tissue. (Right) Specimen B severe acute transmural appendicitis.
Discussion
Duplication in the digestive tract is a rare complication in adults since more than 80% of cases present as an acute abdomen or bowel obstruction before the age of 2.4 Appendiceal duplication is extremely rare with an incidence of 0.004% to 0.009% in appendectomy specimens.5,6 Appendiceal duplication can be isolated or associated with cecal duplication. Appendiceal duplications were first classified in 1936 by Cave,7 updated in 1962 by Wallbridge,8 and then again by Bierman in 1993.9 They classified the major kinds of anomalies into Types A, B, C, and D. Type A has a single cecum with various degrees of incomplete appendiceal duplication. Type B has a normal appendix that arises from the cecum and is subdivided into 4 separate types depending on where the second appendix is located. Type B1 (avian-type appendix) arises symmetrically from the other side of the ileocecal valve; this resembles the arrangement in birds. Type B2 (tenia coli type) arises anywhere along the lines of the tenia coli. Type B3 arises from the hepatic flexure,9 and Type B4 arises from the splenic flexure.6 Type C is a duplication of the cecum, each containing an appendix. Type D, the most recently described type by Mesko et al in 1986,10 is a horseshoe appendix—a single appendix with 2 openings into the cecum. A case of appendiceal triplication has also been reported.11 Coker et al12 suggested an embryologic etiology for these anomalies (Table 1).13
Table 1.
Modified Cave-Wallbridge duplicate appendix classification scheme. Modified from Coker et al12
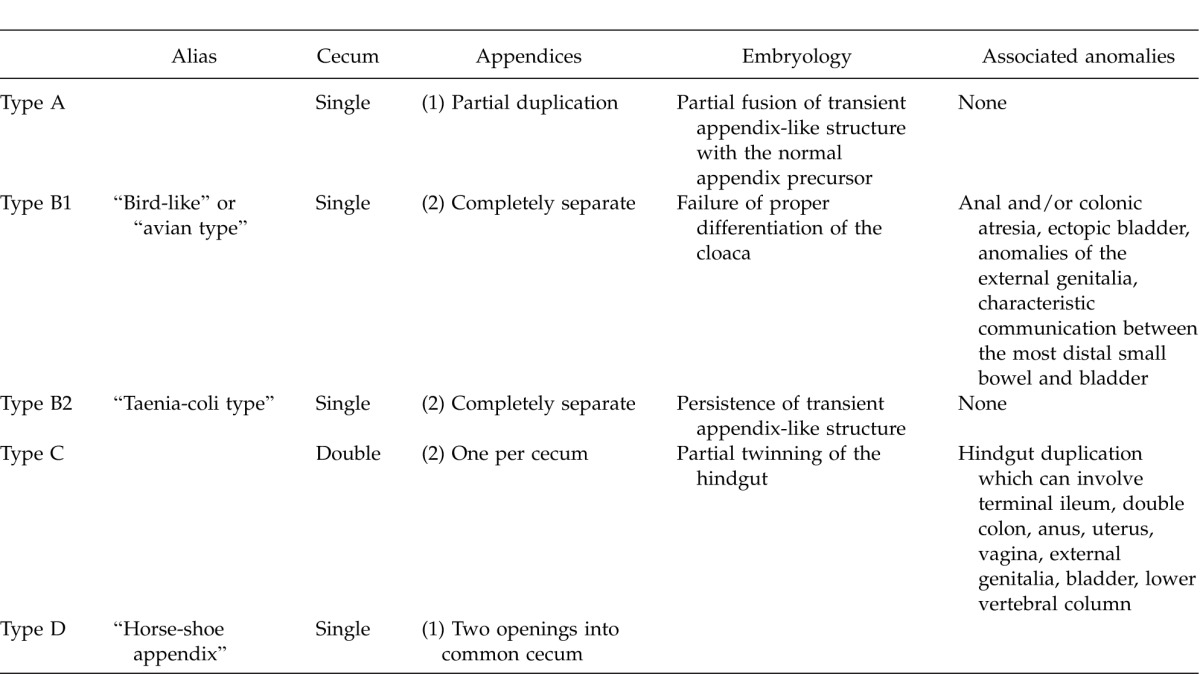
Suspicion of a duplicated appendix should prompt further investigation into the possibility of other congenital anomalies, including duplications or anomalies of the gastrointestinal tract or genitourinary tract,14 gastroschisis,15 and vertebral anomalies,5,16 especially in type B1 and C cases.17 Type B2 duplication is not known to be associated with any other congenital anomalies (Table 1).17
The case described above falls under the Type B2 classification as there were 2 separate appendices attached via separate bases onto the cecum. The duplicate appendix was located over the taenia-coli. Type B2 is the most frequently reported duplication of the appendix.18
Reports of appendicitis in patients with a duplicated appendix are rare in the literature, however, it is likely that many cases are missed simply because the second appendix was never identified. Retrocecal appendices and type B duplications are most likely to remain unnoticed.17 Identification of the anomaly can be further confounded when the clinical presentation mimics other conditions, such as adenocarcinoma of the colon,19 small bowel obstruction, volvulus, or intussusception.20 In cases where appendiceal duplication is suspected, histopathologic examination must show a complete and separate inner circular and outer longitudinal muscle layer and the appropriate amount and arrangement of lymphoid tissue to differentiate a duplicate appendix from an appendiceal or solitary cecal diverticulum.21
Appendiceal duplication should be in the differential diagnosis when a clinical diagnosis of acute appendicitis does not correlate with the operative finding of a normal looking appendix. Although a very rare entity, ensuring its absence would prevent diagnostic ambiguity. It is recommended that if multiple appendices are located, all of them should be removed to avoid any diagnostic ambiguity in the evaluation of abdominal pain in future. This would also avoid any medicolegal ramifications of a “previously removed” appendix.22
Although appendiceal duplication occurs very rarely, awareness of this congenital anomaly and thorough intraoperative inspection are critical to avoid the potential consequences of missing a second appendix, as well as any associated congenital anomalies, and to minimize confusion with other intra-abdominal structures.
References
- 1.Centers for Disease Control and Prevention. National Hospital Discharge Survey: Procedures by selected patient characteristics - Number by procedure category and age. United States; 2010. Health. [Google Scholar]
- 2.Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132(5):910–925. doi: 10.1093/oxfordjournals.aje.a115734. [DOI] [PubMed] [Google Scholar]
- 3.Arda IS, Şenocak ME. Hiçsönmez. A duplication of vermiform appendix: case report and review of the literature. Pediatr Surg Int. 1982;7:221–222. [Google Scholar]
- 4.Macpherson RI. Gastrointestinal tract duplications: clinical, pathologic, etiologic, and radiologic considerations. Radiographics. 1993;13(5):1063–1080. doi: 10.1148/radiographics.13.5.8210590. [DOI] [PubMed] [Google Scholar]
- 5.Collins DC. A study of 50,000 specimens of the human vermiform appendix. Surg Gynecol Obstet. 1955;101(4):437–446. [PubMed] [Google Scholar]
- 6.Kjossev KT, Losanoff JE. Duplicated vermiform appendix. Br J Surg. 1996;83(9):1259. [PubMed] [Google Scholar]
- 7.Cave AJ. Appendix Vermiformis Duplex. J Anat. 1936;70(2):283–292. [PMC free article] [PubMed] [Google Scholar]
- 8.Wallbridge PH. Double appendix. Br J Surg. 1962;50:346–347. doi: 10.1002/bjs.18005022124. [DOI] [PubMed] [Google Scholar]
- 9.Biermann R, Borský D, Gogora M. Die Appendicitis duplexeine pathologische Rarität [in German] Chirurg. 1993;64:1059–1061. [PubMed] [Google Scholar]
- 10.Mesko TW, Lugo R, Breitholtz T. Horseshoe anomaly of the appendix: a previously undescribed entity. Surgery. 1989;106(3):563–566. [PubMed] [Google Scholar]
- 11.Uriev L, Maslovsky I, Mnouskin Y, Ben-Dor D. Triple-barreled type of appendiceal triplication. Ann Diagn Pathol. 2006;10(3):160–161. doi: 10.1016/j.anndiagpath.2005.09.016. [DOI] [PubMed] [Google Scholar]
- 12.Coker DD, Hartong JM, Conklin HB. Duplication of the vermiform appendix: case report. Mil Med. 1975;140(5):331–332. [PubMed] [Google Scholar]
- 13.Schumpelick V, Dreuw B, Ophoff K, Prescher A. Appendix and cecum. Embryology, anatomy, and surgical applications. Surg Clin North Am. 2000;80(1):295–318. doi: 10.1016/s0039-6109(05)70407-2. [DOI] [PubMed] [Google Scholar]
- 14.Jianhong L, Xuewu J, Xianliang H. An exceptional combined malformation: duplication of the urinary and intestinal tracts and the vulva (04-80CR) J Pediatr Surg. 2005;40(3):E5–9. doi: 10.1016/j.jpedsurg.2004.11.003. [DOI] [PubMed] [Google Scholar]
- 15.Gilchrist BF, Scriven R, Nguyen M, Nguyen V, Klotz D, Ramenofsky ML. Duplication of the vermiform appendix in gastroschisis. J Am Coll Surg. 1999;189(4):426. doi: 10.1016/s1072-7515(99)00174-x. [DOI] [PubMed] [Google Scholar]
- 16.Dutta T, George V, Meenakshi PK, Das G. Rare combination of duplication of genito-urinary tract, hindgut, vertebral column and other associated anomalies. Br J Urol. 1974;46(5):577–582. doi: 10.1111/j.1464-410x.1974.tb03859.x. [DOI] [PubMed] [Google Scholar]
- 17.Christodoulidis G, Symeonidis D, Spyridakis M, Koukoulis G, Manolakis A, Triantafylidis G, et al. Acute appendicitis in a duplicated appendix. Int J Surg Case Rep. 2012;3(11):559–562. doi: 10.1016/j.ijscr.2012.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Travis JR, Weppner JL, Paugh JC. Duplex vermiform appendix: case report of a ruptured second appendix. J Pediatr Surg. 2008;43(9):1726–1728. doi: 10.1016/j.jpedsurg.2008.04.023. [DOI] [PubMed] [Google Scholar]
- 19.Bluett MK, Halter SA, Salhany KE, O'Leary JP. Duplication of the appendix mimicking adenocarcinoma of the colon. Arch Surg. 1987;122(7):817–820. doi: 10.1001/archsurg.1987.01400190083016. [DOI] [PubMed] [Google Scholar]
- 20.Iyer CP, Mahour GH. Duplications of the alimentary tract in infants and children. J Pediatr Surg. 1995;30:1267–1270. doi: 10.1016/0022-3468(95)90482-4. [DOI] [PubMed] [Google Scholar]
- 21.Misdraji J, Graeme-Cook FM. Miscellaneous conditions of the appendix. Semin Diagn Pathol. 2004;21(2):151–163. doi: 10.1053/j.semdp.2004.11.006. [DOI] [PubMed] [Google Scholar]
- 22.Mitchell IC, Nicholls JC: Duplication of the vermiform appendix: report of a case: review of the classification and medicolegal aspects. Med Sci Law. 1990;30:124–126. doi: 10.1177/002580249003000208. [DOI] [PubMed] [Google Scholar]