

Abstract
Background
In this edge, medical tourism is not a new idea. Medical treatment is one of the essential demands of human beings and it requires high quality and intensive care. Beside western world, few developing countries are playing key roles as medical tourism destinations. India is one of the leading names among these countries. The purpose of the paper is to find the factors influencing the attractiveness of India as a health tourism destination.
Methods
The study has found the major contributing factors and their relative importance in the attractiveness of the health tourism destination that is India from consumers’ perspectives by conducting survey with an application of structural equation modelling approach.
Results
In Indian context, medical tourists consider service quality and cost mostly to select any medical destination. In addition they also give value to the destination competitiveness but tourist attitude is less important in comparison with other factors affecting their destination choice. Since the study has used structural equation modelling approach to test the hypothesis and figure out the relative importance of the factors, the fundamental indices such as Normed Chi square(less than 3), RMSEA (less than 0.08) and CFI (more than 0.90) values show the overall model fit of the proposed model.
Conclusion
In order to transform a country such as India as an attractive and competitive medical tourist destination in this time of globalization, a step should be taken to control cost ensuring the quality of services.
Keywords: Medical tourism; Destination competitiveness; Factors, India
Introduction
It is not new to venture abroad for health care from different international locations. In this new horizon, medical tourism has great value of interest. Health tourism or medical tourism is not a very concise idea. It may include quality health care services as well as some other facilities like better accommodation, shopping and sometimes recreational arrangements. Desired medical destination nations are not always just western world countries. A new angling phenomenon is people of developed and developing countries visiting medical destination countries around the world for medical care. The major reasons for this may include lengthy waiting time to get visa or medical services in some western countries, high expenses, and lack of medical insurance, or under-insurance. Among the most famous medical tourism destination countries, Asian countries attract more tourists because these are less expensive than those of other parts of the world like US or European countries. As in most Asian countries labour cost is lower thus medical tourists or international customers can save their money from 40% up to 60% (1). Thus the success of some Asian countries like Thailand, India, Malaysia and Singapore are remarkable in this medical tourism industry (2).
Among these countries India is highly competitive. Medical tourism has become one of the most growing sectors of India. The country has an annual growth rate of 30% and it is expecting to become a $2 billion industry by 2015. The major contributing factors behind the success of India in medical tourism may include less costly skilled labour force, latest medical technologies, standard quality medical services and facility of mass use of English language. The only remaining problem can be its infrastructure. But Indian Government is committed to solve this by giving it a higher priority. A study by ASSOCHAM reported that 850,000 tourists came to India in 2011 and they forecasted, by 2015 this number may rise to 3,200,000. The most popular treatments the country provides are, bone-marrow transplant, alternative medicine, cardiac bypass, hip replacement, and eye surgery. Chennai is the most famous city of India for medical tourism (3).
Based on the present condition and future prediction India is a very successful medical destination for the world indeed. But there is no such industry in world which is free from risk. In order to avoid vulnerability, the country should search new competitive advantages continuously. The main focus can be on increasing the number of medical tourists as well as maintaining and enhancing the quality of health care services at reasonable costs and also ensuring ethical issues. Thus it is essential to learn the factors that play the major role in order to succeed in this industry from the point of view of medical or health tourists. Thus other emerging countries can learn and take proper steps accordingly. At the same time the country, India can emphasize on the most important issues to maintain and to enhance the prosperity of medical tourism.
Healthcare in India
Medical sector is a key service sector among other service sectors of India. 4 million people are involved in this. By the end of 2012 the healthcare sector which includes Pharmaceutical and health insurance is expected to reach between US$ 50 billion and US$ 69 billion which was US$ 22.2 billion. Indian medical services include varieties of treatments like Allopathic, Homoeopathy (AYUSH), aYurveda, Unani, Siddha and Tibetan. In addition public health services include primary health centers (PHC), sub-centers, district hospitals and community health centers (CHC) (4-6). 80 percent of health services are provided by the private sector in the country and it consists of private dispensaries, private hospitals, corporate hospitals, charity hospitals, and medical centers managed by NGOs (6).
The healthcare industry of India is expanding at an extraordinary rate. Government investment, private hospitals and foreign aid in the public health programs play the key roles for this boom. 300 million middle class “healthcare consumers” are creating astonishing demand for quality healthcare. Thus India has become a strong medical tourism destination because of its high quality medical services which are available at low cost. During vacation foreigners are attracted to involve in health tourism. Therefore, they get required medical attention and at the same time entertainment and relaxation which can be more costly in their own country or other countries of the world (3).
As stated earlier, India is one of the best health tourism destinations in the world. However, not all the states and cities of India are prominent for this service. Among many, Bangalore in Tamil Nadu and Chennai in Karnataka state are the famous destinations of health tourism in India (7). There are many well-known health service providers in Bangalore such as Apollo Hospitals, Columbia Asia, Fortis Hospitals and Manipal Hospitals that attain the attention of many people all over the world (8).
Tamil Nadu is another outstanding address for the health related service seekers where most of the health service providers are located in Chennai as the capital of the state. Apollo Group, Billroth Hospitals, Frontier Lifeline Hospitals, Global Health City and The Madras Medical Missions are the key points of service for the industry (9). Apart from these two major states, Delhi, Mumbai also attract many local and international health tourists. In many cases, the prime hospitals have their franchise in the important states and the cities of India (8). The following table (table 1) shows the overall picture of infrastructure and human resources in the health sector of India. For each place to become a popular health service destination, it needs to get some distinct advantages (10). There are many underlying reasons that make these cities as popular hubs for the health services. Favorable health care infrastructures, climate, entertainment facilities, positive service quality of health care personnel, reasonable cost for accommodation, transportation and medical fees make the cities compatible as international health care destinations (7-9). In the literature review section, these factors are discussed elaborately in constructive manner.
Table 1.
Infrastructure and human resources
| Category | Number |
|---|---|
| District hospitals | 550 |
| Community Health Centers(CHC) | 3,700 |
| Primary Health Centers (PHC) | 23,000 |
| Sub-centers | 140,000 |
| Medical colleges (including private) | 170 |
| Hospitals (including private) | 15,000 |
| Hospital beds (including private) | 875,000 |
| Retail chemist outlets (including private) | 350,000 |
| Allopathic doctors | 600,000 |
| Practitioners of other systems | 115,000b |
| Nursing staff | 737,000 |
| Traditional dais (midwives) | 700,000 |
| Bonesetters | 60,000 |
| Herbal healers | 80,000 |
Literature Review
The Literature review includes certain factors that influence health tourism industry in India. All these factors are wider than the quality of service, the competitiveness of the destination and various aspects. The descriptions of the key factors affecting medical tourists are given below:
Destination Competitiveness
A desired destination of medical tourism should be a kind of product containing central rewards like commercial infrastructure and environmental factors. Comparative advantage may involve climate, surroundings, flora and fauna, while competing advantage may relate to such produced items such as health and medical care areas, heritage/historic attractions, events, transport sites, govt policy, the actual quality of management and skills of workers (11).
Crouch et al. (12) defined the most aggressive location, which is actually one that is liable to bring finest success; that arranges a surrounding which is the most suitable place for the residents for a certain schedule. Hence, competitiveness of a destination for medical tourism has to last besides, being simply cheap. In addition it should be socially, culturally, politically and environmentally sound and friendly. For that reason, it is always suggested that the most acceptable desired destination could be the one where medical tourists get a friendly environment.
India has achieved a desirable position in medical tourism because of its adaptability with the changing world demand for healthcare and its greater competitiveness. Singapore, Malaysia, Bulgaria and Cuba are also moving in this globalized industry very aggressively. Based on the literatures it is not possible to highlight only one country as the greatest competitor in the field of medical tourism (13).
Service Quality
One of the most crucial factors is the service quality provided by the destination country in medical tourism industry. Medical tourists focus greatly on this issue. Thus the destination country must fulfill the expectations of the medical tourists through quality service and performance (14). In the service providing organizations, service quality is proven as an important determinant of competitiveness (15).
Quality in service organization goes beyond the mere application of quality management into the whole organization (16). Every part of the organization is very much affected and inspired by quality as the way of doing activities. Quality is determined as a critical issue for competitive success. Quality improvement and its potentiality in travel and tourism services are very difficult to implement as it involves people from different countries with different cultural background and demands (17). However, companies can improve service quality by lowering distribution costs and enhancing the service provided.
There are five major dimensions of service that should be emphasized while measuring its quality. These are (14):
-
a)
Reliability;
-
b)
Tangibles;
-
c)
Empathy;
-
d)
Responsiveness;
-
e)
Assurance.
As the quality in service industry is quite different than the quality in manufacturing industry, therefore the meaning of service quality must be defined at first. Zero defects are treated as quality in manufacturing industry (18). On the contrary, three characteristics separate service industry or tourism industry from manufacturing and these are: intangibility, perishability and inseparability (18, 19). Services are intangibles whereas goods are tangibles (15). Intangibility can be clarified if the products cannot be exhibited. Perishability ‘involves the simultaneous production and consumption of the service’ (18, 20). In medical tourism if any country can provide quality healthcare services at low cost then it will definitely attract the world.
In this sector meaning of quality service is a vast issue. It involves the quality of healthcare center as well as the doctors and other staffs. However, healthcare is actually a very individual and critical service and it is not an easy task to define its quality (21).
Human behavior can be modified through the training process. Here new and different types of capabilities can be added. On the other hand, some capabilities which are already possessed by individuals can be extended or enhanced. In the process of training one can learn to behave properly in different situations that ultimately increases capabilities that reflects the nature, variability and intensity of what people are required to do (22).
Customer expectations involve two major factors, quality service and qualified labor force. In these days companies are straggling because customers are demanding high level of excellent services and skilled labor is harder to find and keep (23). Baum and Hagan (24) discuss that the lack of sustained employment, which is the characteristic of seasonal operations, undermines the ability of operators to deliver quality, which the marketplace, increasingly, expects. There is a great correlation between customer satisfaction and employee performance that is well trained and qualified employees (25). In service industry customers evaluate quality based on the behavior and skills of the employees. Customers take the behavior of service providers as the key influencer in order to judge the nature of the service (26). Because of the variability in human beings, consistency of quality service is difficult to ensure (27).
Well skilled workers provide quality service if they are properly trained and perfectly compensated. They are more loyal to the company and require less supervision. Consequently, their customers are also loyal and satisfied and thus they purchase more than they could if they were not contended (28).
Tourist Attitude
In tourism industry customer or tourist attitude towards any destination is very important for its success. It may vary from person to person. This can be different on certain aspects like, customer group, age, gender, income, family structure, race, culture, social class and ethnicity. Food, cloths, politics and religion are crucial factors for human attitudes. Attitude can be defined as individuals’ evaluation of feelings and tendencies toward an object or an idea.
It is attitude which affects people to like or dislike something or to move towards or away from that (29). Thus it is very crucial for any business to develop positive customer beliefs or attitudes toward the product or service or medical tourist destination. According to psychologists, attitudes are developed by individuals through the encounters in their lifetime (30). Attitude is not transitory rather it lasts over time.
Evaluations of various situations can be defined as attitudes. Information achievements produce attitudes. That is attitudes are learned beliefs, feelings, and reaction tendencies (31). Minor or major decisions of consumers are affected greatly by attitudes, such as consumers have attitudes to decide any medical tourism destination country or a specific healthcare centre within the country.
Cost
Consumers are very sensitive regarding the cost of any product or service. This is true for all types of customers especially price sensitive customers. Price of any product or service is a key element to determine the level of satisfaction of any customer. It should not exceed the expectation of customers (32). In addition, competitiveness of any product or service largely depends on the total cost to get that. It may include, actual price of the product, transportation or installation cost, physical cost or hard work to get that and social cost like getting appreciation or criticisms from others and opportunity costs to ignore other products (33). In the sector of tourism, a destination can be attractive to its tourists only when the costs of getting services are reasonable. There can be some exceptional cases but cost affect tourist choice and satisfaction. It involves certain types of expenditures like, accommodation cost, transportation cost, food cost, and other entertainment cost etc. (24). Therefore, in medical tourism cost of medical service or fees, cost of accommodation, cost of food and transportation cost are vital issues for measuring the attractiveness of a destination. On the basis of the above mentioned literatures, figure 1 depicts the conceptual model of the study.
Fig. 1.
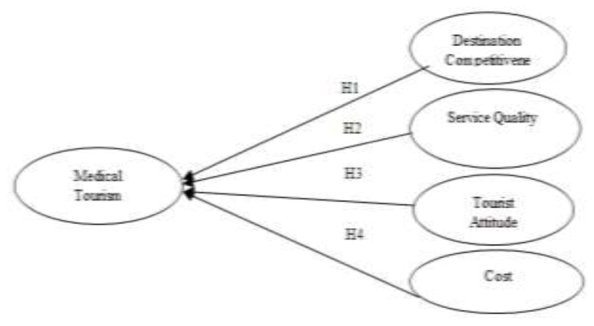
Conceptual model
Hypothesis
H1: Destination Competitiveness has significant influence on Medical Tourism Destination Attractiveness
H2: Service Quality has significant influence on Medical Tourism Destination Attractiveness
H3: Tourist Attitude has significant influence on Medical Tourism Destination Attractiveness
H4: Service Cost has significant influence on Medical Tourism Destination Attractiveness
Methods
The main objective of the study is to measure the relative importance of 4 factors in deciding the attractiveness of medical tourism destination from the point of view of consumers in India.
Thus a self-administered questionnaire was given to 235 international patients in India in order to collect the required primary data. Here convenient sampling was used because of time and cost limitations. According to Mayer (34), convenient sampling can represent the actual characteristics of population like other sampling techniques. As the major hubs for medical tourism may include Chennai and Bangalore in India; therefore from these two places data was collected. For instrument development, 5 point likert scale was used including strongly disagree; disagree; neutral; agree and strongly agree. Among the 235 questionnaires, 202 respondents gave complete and valid data. In order to gain major characteristics factor analysis was conducted. Factor analysis is an appropriate statistical tool through which large data set can be converted into more manageable and organized set, without losing minimum information (35).
Structural Equation Modelling (SEM) was used to clarify the importance of constructs and overall relationships between and among the variables and constructs.
Results and Discussions
Factor Analysis
In order to segment the items under each construct Factor Analysis is used. Principle Component Analysis (PCA) is applied where the number of respondents is 202; number of items is 17. In the analysis, the reliability statistics is satisfactory with the cronbach’s alpha value over .90. Bartlett’s Test of Sphericity and the Kaiser–Mayer–Olkin (KMO) test are used to measure construct validity of the factor analysis. Sample adequacy is measured by KMO and the value of Bartlett’s Test of Sphericity should be significant for the construct validity. All these indicate the study includes adequate sample size. Factor analysis is justified here as KMO value is more than .60 and Bertletts test shows that it is significant to use the factor analysis in the study (Table 2). Under the consideration of factor loading standard rule, variables with 0.30 or greater loading is significant while 0.40 and 0.50 are greater (35). All the items are loaded with more than .55 showed the real fit in factor analysis. According to the Table 3, it is clear that the associations of items to each factor are considerable. High affiliation is indicated by the higher loadings. All of the items are loaded under four constructs and all the values of the loadings prove that none of the loading is trivial.
Table 2.
KMO and Barlett’s test
| KMO and Bartlett's Test | ||
|---|---|---|
| Kaiser-Meyer-Olkin Measure of Sampling Adequacy. | .801 | |
| Bartlett's Test of Sphericity | Approx. Chi-Square | 1611.972 |
| Df | 452 | |
| Sig. | .000 | |
Table 3.
Rotated factor matrix
| Description | F1 | F2 | F3 | F4 |
|---|---|---|---|---|
| Destination Competitiveness: | ||||
| Infrastructure | .766 | |||
| Climate | .787 | |||
| Health Care area | .891 | |||
| Entertainment | .609 | |||
| Service Quality: | ||||
| Reliability | .899 | |||
| Tangibles | .764 | |||
| Empathy | .650 | |||
| Responsiveness | .890 | |||
| Assurance | .792 | |||
| Tourist Attitude: | ||||
| Culture | .782 | |||
| Income | .795 | |||
| Race | .690 | |||
| Religion | .702 | |||
| Service Cost: | ||||
| Medical Fees | .833 | |||
| Accommodation Cost | .720 | |||
| Food Cost | .655 | |||
| Transportation Cost | .701 |
Structural Equation Modelling Approach
SEM or Structural Equation Modelling is a kind of statistical tool to discover relationships among the factors. Here in order to examine any relationship, researchers must determine the overall model fit (36). In this case researchers need to either accept or reject the entire model. Therefore, to justify that the constructs are defined adequately in the model every study should conduct measurement model before the path analysis. To confirm about the validity of the analysis, there should be resemblance between measurement model and the path model.
For complete structural model or path analysis, some statistical evidences are relatively more important. For overall model fit, the research must report on χ2 (Chi square) and the degree of freedom including p-value along with incremental index such as CFI or TLI and one absolute index like RMSEA (36). To assess the overall fit measures, χ2 is used as the fundamental tool. The sample size and the difference between observed and model covariance matrix are very important to calculate chi square value. It means, the lower the value of chi square the better at certain degree of freedom and “P” value. Here, in this study at the given degrees of freedom chi square value is closed to the standard value and p value indicates good fit. P value is also justified by the number of items included in the model. Significant p value is expected based on the number of respondents.
To examine the baseline comparison, CFI or comparative fit index is mostly used. Basically, in a given data set it measures the correlations and the average size. High CFI value means high correlation. The CFI value is .93 which is closed to 1. RMSEA or root mean square error of approximation is used as a complete index to determine the overall fit of the model. The good model fit is indicated, if the value is 0.05; and less on the contrary 0.1 or more is taken as the poor model fit. In the Fig. 2 a full path model is shown that is derived from the alternative model. Some items are omitted here due to the insignificant relationships between the constructs. Table 4 shows the fit measures of the main model where all the values are satisfactory.
Fig. 2.
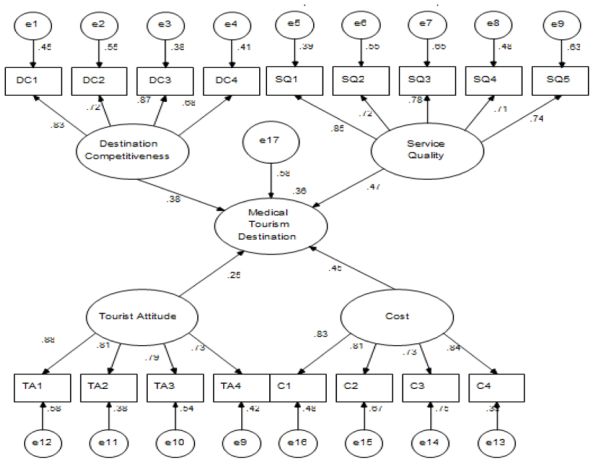
Path model of factors affecting medical tourism destination attractiveness
Table 4.
Fit measures of main model
| Fit measures | Main Model |
|---|---|
| X2 | 19.903 |
| Degree of freedom (df) | 11 |
| P | 0.00 |
| Normed Chi Square | 1.809 |
| Root mean square error of approximation (RMSEA) | 0.37 |
| Comparative fit index (CFI) | 0.963 |
| Goodness-of-fit index (GFI) | 0.987 |
Hypothesis Testing
In the case of Structural Equation Modelling hypothesis is tested by the use of CR value for standard estimation in the main model. If the value is over 1.96 then it is treated as the benchmark to establish the relationship (36). From the Table 5, it is clear by the CR value that every construct has the significant effect on medical tourism destination attractiveness. Therefore, the alternative hypothesis H1, H2, H3 and H4 are not rejected. In addition RMSEA show the overall fitness of the model which indicates that endogenous variable has the significant relationship with the given exogenous variables.
Table 5.
Standard estimation of the main model
| Standardized Regression Weights | Estimate | S.E. | C.R | P |
|---|---|---|---|---|
| Service Quality | .708 | .103 | 6.877 | *** |
| Cost | .540 | .095 | 5.693 | *** |
| Destination Competitiveness | .427 | .102 | 4.195 | *** |
| Tourist Attitude | .289 | .093 | 3.019 | *** |
Though, construct to construct value is 0.20 or more, is considered as the significant for defining the relationship from construct to construct (36), the path model demonstrates that the relationship between destination competitiveness and medical tourism destination; service quality and medical tourism destination; tourist attitude and medical tourism destination; cost and medical tourism destination are significant. Based on the Critical Ratio (CR) of Standard Estimation of the Main Model (Table 5), it is determined that the medical tourists emphasize more on service quality and cost rather than destination competitiveness and tourist attitude in medical tourism destination attractiveness in India.
Validity of the Analysis
Basically SEM or Structural Equation Modelling requires testing three types of validity, such as convergent validity, discriminant validity and nomological validity. Each variable that is attached with the constructs has the factor loading of 0.70 or more in the final analysis. Thus it is proved to have convergent validity as per the requirements. The significant squared correlation value must be considered in order to measure discriminant validity. At the level of 0.001, all the values of the model are perfectly fit. The nomological validity is also satisfactory based on the Overall Fit Indices, sample size and other types of measures.
Conclusion and Limitation
Medical tourism is actually a different kind of market with its specialized attributes. It may range from the core health care services to other infrastructural facilities to other extreme point like entertainment, amusement and shopping. In order to become a highly successful health tourism destination, it requires different types and levels of skilled people along with quality products and services. Beside all these even the climate of the country and individual customer attitude can tune this industry’s success. The major drawback of this industry is some kinds of uncontrollable elements which cannot be changed. But yet there is chance to cope with them to survive and to shine in this worldwide great sector of tourism.
Here, human resource development is a vital issue for the overall prosperity of this sector. Specialized education can train students in way to provide value added services to the visitors and at the same time it will enhance the image of the country in the world. It may include guidance regarding ‘ethics’ and ‘subculture’ (37). Proper training and good rewarding system are essential to produce skilled human products. Cost is another key factor in the satisfaction of any tourist. There should be a step to control cost and at the same time providing quality services at reasonable price. All these efforts can make any country an attractive and competitive medical tourist destination in this time of globalization.
The study is conducted within a short period of time thus in- depth qualitative data could not be collected to reflect the situation more clearly. On the other hand some more relevant factors affecting the choice of medical tourist to select any destination can be included in further research on this area of interest.
Ethical Considerations
Ethical issues like plagiarism, double publication, any falsification in data etc. are absolutely observed by the authors of this paper.
Acknowledgements
As per the declaration of the authors, it is definite that there is no discrepancy of interests between and among the authors of the study.
References
- Kshetri N (2011). The healthcare off-shoring industry in developing economies-institutional and economic foundations: An Indian case. Int J Health Care Qual Assur, 24(6): 453–470. [DOI] [PubMed] [Google Scholar]
- Enderwick P, Nagar S (2011). The competitive challenge of emerging markets: the case of medical tourism. Int J Emerg Market, 6 (4): 329–350. [Google Scholar]
- Ray S, Mukherjee A (2007). Development of a framework towards successful implementation of e-governance initiatives in health sector in India. Int J Health Care Qual Assur, 20 (6): 464–483. [DOI] [PubMed] [Google Scholar]
- Srinivasan S, O’Fallon LR, Dearry A (2003). Creating healthy communities, healthy homes, healthy people: initiating a research agenda on the built environment and public health. American J Publ Health, 93 (9): 1446–1450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lal S (2004). National Oral Health Care Programme (NOHCP) implementation strategies. Indian J Commun Med, 29 (1). [Google Scholar]
- Gupta AS (2008). Medical tourism in India: winners and losers. Indian J Med Ethics, 5 (1): 4–5. [DOI] [PubMed] [Google Scholar]
- Mochi P, Shetty N, Vahoniya D (2013). Medical tourism-destination. Indian Commerce and Manage, 2 (3): 29–39. [Google Scholar]
- Saligram P, Bhattacharjee A, Crooks V, Labonté R, Schram A, Snyder J (2014). An Overview of the Medical Tourism Industry in Bangalore. India-Version 1.0 Canadian Institute of Health Research, Canada. [Google Scholar]
- Madha S, Crooks V, Labonté R, Schram A, Kalaivani R, Nithya S, Snyder J (2014). An Overview of the Medical Tourism Industry in Chennai. India-Version 1.0. Canadian Institute of Health Research, Canada. [Google Scholar]
- Mosbah A, Saleh AA (2014). A Review of Tourism Development in Malaysia. Euro J Bus and Manage, 6 (5): 1–9. [Google Scholar]
- Al-Amin M, Makarem SC, Pradhan R (2011). Hospital ability to attract international patients: a conceptual framework. Int J Pharma Health Market, 5 (3): 205–221. [Google Scholar]
- Crouch GI, Ritchie JR (2005). Application of the Analytic Hierarchy Process to Tourism Choice and Decision Making: A Review and Illustration Applied to Destination Competitiveness. Tourism Anal, 10 (1): 17–25. [Google Scholar]
- Ritchie JR, Crouch GI (2000). The Competitive Destination: A Sustainability Perspective. Tourism Manage, 21 (1): 1–7. [Google Scholar]
- Parasuraman A, Zeithaml VA, Berry LL (1994). Reassessment of expectations as a comparison standard in measuring service quality: implications for future research. J Market, 58: 111–124. [Google Scholar]
- Lewis BR (1989). Quality in the service sector-A review. Int J Bank Mark, 7(5). [Google Scholar]
- Wilkinson A, Witcher B (1991). Quality concerns for managers. Int J Qual Reliab Manage, l9 (2): 64–67. [Google Scholar]
- Hjalager AM (1997). Innovation patterns in sustainable tourism: an analytical typology. Tourism Manage, 18 (1): 35–41. [Google Scholar]
- Buhalis D, Law R (2008). Progress in information technology and tourism management: 20 years on and 10 years after the Internet-The state of e-Tourism research. Tourism Manage, 29 (4): 609–623. [Google Scholar]
- Thwaites E, Williams C (2006). Service recovery: a naturalistic decision-making approach. Manage Serv Qual, 16 (6): 641–653. [Google Scholar]
- Baum T (2007). Human resources in tourism: Still waiting for change. Tourism Manage, 28 (6): 1383–1399. [Google Scholar]
- Berry LL, Bendapudi N (2007). Health care a fertile field for service research. J Serv Res, 10 (2): 111–122. [Google Scholar]
- Joy-Matthews J, Megginson D, Surtees M (2004). Human resource development. 1st ed Kogan Page, London. [Google Scholar]
- D’Annunzio G, Maxwell WA (2002). Human resource management: international perspectives in Hospitality and tourism. 2nd ed Thomson Learning, London. [Google Scholar]
- Baum T, Hagen L (1999). Responses to seasonality: the experiences of peripheral destination. Int J Tour Res, 1: 299–312. [Google Scholar]
- Wiley JW (1990). Customer satisfaction: a supportive work environment and its financial cost. Human Res Plann, 14: 117–27. [Google Scholar]
- Goodwin C, Ross I (1990). Consumer evaluations of responses to complaints: what’s fair and why? J Cons Market, 7 (2): 39–47. [Google Scholar]
- Kamdampully J (1997). Hospitality, Tourism and Leisure Management: issues in strategy and culture. 4th ed Cassell, London. [Google Scholar]
- Schlesinger LA, Hesket JL (1991). The service driven service company, Harvard Bus Rev, 5: 71–81. [PubMed] [Google Scholar]
- Kotler P, Bowen M (2003). Marketing for hospitality and tourism. 3rd ed Pearson Education Inc, New Jersey. [Google Scholar]
- Fazio RH, Zanna MP (1981). Direct experience and attitude-behavior consistency. Advance Exp Soc Psycho, 14: 161–202. [Google Scholar]
- Strethnal CR (1982). Consumer behavior: An information processing perspective. 2nd ed Prentice-Hall, Canada. [Google Scholar]
- Hosseini H (2010). Strategies to contain the high and rising costs of health: Will they increase existing health care disparities and are they ethical? Humanomics, 26 (2): 112–123. [Google Scholar]
- Crooks VA, Turner L, Snyder J, Johnston R, Kingsbury P (2011). Promoting medical tourism to India: Messages, images, and the marketing of international patient travel. Soc Sci Med, 72 (5): 726–732. [DOI] [PubMed] [Google Scholar]
- Meyer D (2000). Applied Research Design for Business and Management 2nd ed McGraw-Hill, Sydney: pp. 52–56. [Google Scholar]
- Hair JF, Anderson RE, Tatham RL, Black WC (1992). Multivariate Data Analysis. 3rd ed Macmillan, New York: pp. 47–82 [Google Scholar]
- Hair JF, Black WC, Babin BJ, Anderson RE (2010). Multivariate Data Analysis 7th ed.Prentice Hall, Upper Saddle River, New Jersey. [Google Scholar]
- Hultsman J (1995). Just tourism: an ethical framework. Annals Tourism Res, 22: 553–567. [Google Scholar]