

Abstract
Objective: To evaluate the diagnostic outcomes of magnetocardiography (MCG) on the patients with coronary artery disease and compared the outcomes between MCG, ECG and Echocardiography. Methods: MCG measurements were performed on 101 patients with coronary artery disease and 116 healthy volunteers with a seven-channel magnetocardiographic system (MCG7, SQUID AG, Germany) installed in an unshielded room. CAD was diagnosed when stenosis ≥ 70% in ≥ 1 vessel. Three quantitative indicators were analyzed, R-max/T-max ratio, R value and á average angle. Results: R-max/T-max ratio of CAD group (6.30 ± 4.07) was much higher than that of healthy group (3.73 ± 1.41) (P < 0.001), R value of CAD group (69.16 ± 27.87)% was significantly higher than that of healthy group (34.96 ± 19.09)% (P < 0.001), á average angle of CAD group (221.46° ± 64.53°) was higher than that of healthy group (24.32° ± 20.70°) (P < 0.01). In 75 of 101 CAD patients (74.26%), MCG had abnormal mapping patterns. The resting ECG examination showed ischemic changes, such as abnormal Q waves and ST-T change in 49 patients (48.51%). Echocardiography revealed abnormal left ventricular wall motion and asynergy in 46 patients (45.54%). Thus, the diagnostic outcomes of MCG for the patients with CAD were much significant than those of ECG and echocardiography (P < 0.001). Conclusions: Our result showed that resting MCG under condition of an advanced data analysis has higher diagnostic outcomes and is superior to ECG or echocardiography for patients with CAD. MCG can detect ST-segment displacement caused by ischemic myocardium, thus helpful in diagnosing coronary artery disease early.
Keywords: Magnetocardiography (MCG), coronary artery disease (CAD), electrocardiogram (ECG), echocardiography, current density distribution map (CDDM), magnetic field map (MFM)
Introduction
Coronary artery disease is one of the most critical diseases as it has very high rate of mortality. Especially in recent years, population aging and changes in life styles are expected to result in more frequent occurrence of atherosclerotic lesions in coronary arteries, leading to an increased rate of morbidity in coronary artery disease.
MCG is a non-invasive technique allowing body surface recording of the magnetic fields generated by the electrical activity of the heart during the cardiocycle. MCG recording allows measurements of the very weak magnetic fields produced by currents flowing within myocardial fibers during cardiac activity. Thus, MCG can detect ST-segment displacement caused by ischemic myocardium and is helpful to diagnose coronary artery disease at early stages.
In the present study, we intended to evaluate the diagnostic outcomes of magnetocardiography for the patients with coronary artery disease by measuring MCG with a seven-channel SQUID system. Also we compared the effectiveness of this approach to that of 12-lead ECG or echocardiography.
Methods
Patients
MCGs were obtained from 101 patients with coronary artery disease (CAD group) and 116 normal subjects (control group). Consent forms were obtained from all patients.
We selected the patients who were hospitalized in Dept. of Cardiology at Rui Jin Hospital from October, 2003 to June, 2007. The CAD group consisted 101 patients (mean age: 59.48 ± 9.26 years old, 68 males and 33 females) with angiographically documented CAD and coronary artery stenosis, defined as a visually estimated lumen narrowing more than 70%, in one or more vessels (42 with one-vessel disease,35 with double-vessel disease, 24 with triple-vessel disease). All patients were in sinus rhythm. Patients with impaired left ventricular function, left ventricle hypertrophy, electrolyte disturbance, disturbance of acid-base balance and arrhythmia, such as bundle branch block or atrial fibrillation were not included in this study.
The control group consisted of 116 healthy subjects (mean age: 56.84 ± 10.80 years old, 65 males and 51 females) with no history of cardiovascular disease. They had normal results on ECG at rest and stress as well as a normal echocardiography at rest.
Data acquisition
MCG examinations were performed by a seven-channel SQUID-magnetometer (MCG7, SQUID AG, Germany) in an unshielded room (Dept. of cardiology of Ruijin Hospital affiliated to Shanghai Second Medical University). Measurements were performed in supine position. Magnetic field registration were carried out in total 36 positions on the basis of a 6 × 6 rectangle grid with a 4 cm pitch over the precordial area and total area of observation was 20 × 20 cm. The sensor was located as close to the thorax as possible, directly over the heart. Data were recorded every 30 seconds. Simultaneously, we recorded the ECG lead II. The signals were then filtered, averaged and the data were stored, analyzed by a personal computer.
For data analysis, an inverse problem solution, such as electrical source calculation based on magnetic field mapping was applied.
Current density distribution maps (CDDM) within ventricular repolartion phase (ST-T interval) were plotted every 12 ms. We analyzed the quantity and direction of vectors areas with an estimated magnitude. Three quantitative indicators were analyzed: R-max/T-max ratio, value and á average angle. We then studied the magnitude, quantity and direction of the vectors within the CDDM.
R-max/T-max ratio
Through the magnetic field maps (MFM) and CDDM reconstructed by Magwin2.5 software package (SQUID AG, Essen, Germany), we analyzed the R-max/T-max ratio, the ratio between the maximal magnetic value of R wave and T wave.
R value
By means of 2.5 software package, each CDDM was classified to 0~4 classes in accordance to the dipole structure and a ratio between vectors directed to sector from 0°~90° and to different direction. Class 0~1 is normal, Class 2 is mildly abnormal and class 3~4 is severe abnormal among these maps. We calculated R value, the ratio of numbers of severe abnormal maps over total maps during the interval of the ST-segment with one map per 12 ms (Figure 2).
Figure 2.
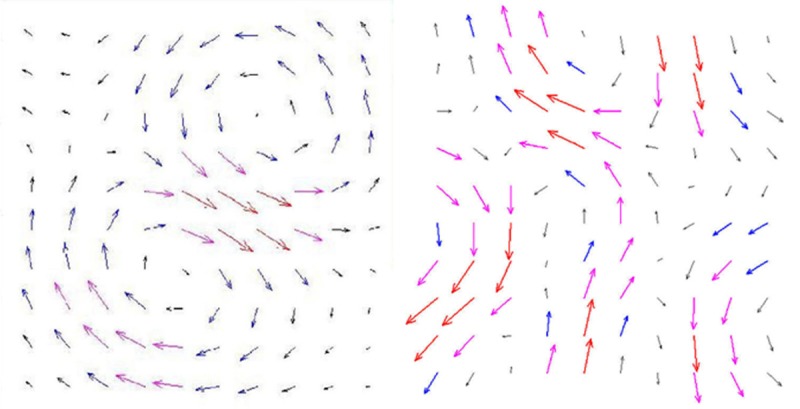
Current density distribution maps of healthy person (left) and CAD patient with triple-vessel disease (Right). Class 0: dopole structure, two vortexes, orientation: 0°~8° (left); Class 4: non-dipole structure, more than two vortexes, non-clear orientation: -20°~110° (Right).
Average angle
We analyzed average direction of maximal vectors during the interval of the ST-segment which includes the second quarter from the J-point to the T wave maximum according to the current density map (Figure 1).
Figure 1.
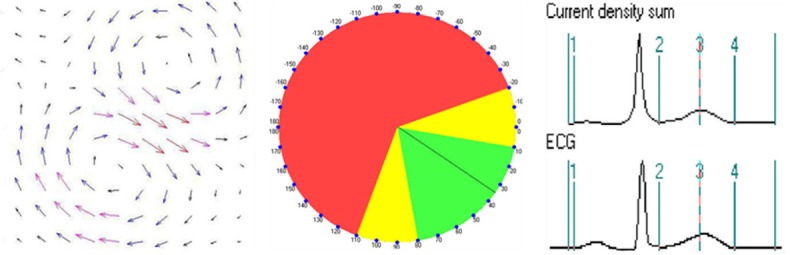
Current density distribution maps of healthy person (left) and transient vectorcardiogram (middle), the direction of the maximal vector is 35 (At the moment of T-wave apex). Note: Green area: normal; Yellow area: critical; Red area abnormal (transient Vectorcardiogram).
Statistical analysis
The independent-samples t test was used for evaluating the difference between CAD patients and controls performed with SPSS statistical software for Windows (Version 10.0). As α average angle belongs to angle data, we used statistical methods of circular distribution. Therefore the α average angle was analyzed by U2 test of average angle between these two groups. P < 0.05 was considered statistically significant.
Results
Clinical characteristics of the two groups
There were no significant differences in age, weight, height or body mass index (BMI) between the CAD patients and control patients (P > 0.05, Table 1).
Table 1.
Clinical characteristics of the two groups (x̅ ± s)
| Group | Chd group (101) | Control group (116) | Statistics | P Value | |
|---|---|---|---|---|---|
|
| |||||
| Χ2 | T | ||||
| Age (Years) | 59.48 ± 9.26 | 56.84 ± 10.80 | 1.938 | 0.054 | |
| Sex (Num, %) | 2.902 | 0.088 | |||
| Male | 68 (67.3) | 65 (56.0) | |||
| Female | 33 (32.7) | 51 (44.0) | |||
| HEIGHT (Cm) | 164.96 ± 7.35 | 165.38 ± 8.07 | 0.397 | 0.691 | |
| WEIGHT (Kg) | 66.85 ± 10.12 | 66.33 ± 11.23 | 0.359 | 0.720 | |
| BMI (Kg/M2) | 24.51 ± 2.99 | 24.16 ± 3.06 | 0.868 | 0.387 | |
Comparison of R-max/T-max ratio, R value and á average angle during the repolarization phase between the patients and control group
The R-max/T-max ratio of CAD group (6.30 ± 4.07) was much higher than that of healthy group (3.73 ± 1.41) (P < 0.001). R value of CAD group (69.16 ± 27.87)% was much higher than that of healthy group (34.96 ± 19.09)% 1 (P < 0.001). á average angle of CAD group (221.46° ± 64.53°) was much higher than that of healthy group (24.32° ± 20.70°, P < 0.01, Table 2).
Table 2.
Comparison of R-max/T-max ratio, R value and á average angle during the repolarization phase between the patients and controls (x̅ ± s)

|
Comparison of using MCG, ECG and echocardiography in diagnosing CAD
In 75 of 101 CAD patients (74.26%), MCG had abnormal mapping patterns. The resting ECG examination showed ischemic changes, such as an abnormal Q wave and ST-T change, in 49 patients (48.51%). Echocardiography revealed abnormal left ventricular wall motion and asynergy in 46 patients (45.54%). The diagnostic outcomes of MCG for the patients with CAD were much higher than those of ECG and echocardiography (P < 0.001).
In 37 of 52 CAD patients, abnormal MCG mapping patterns were present (71.15%). However, in 40 of 55 CAD patients with normal findings of echocardiography, MCG showed abnormal mapping patterns (72.72%).
Discussion
Multichannel MCG is a novel, non-invasive and non-contact mapping technique for studying the electromagnetic function of the heart [2]. The principle of magnetocardiography is based on the measurement of minimal magnetic field, generated by the electrical activity of the heart during the cardiocycle. With extremely sensitive sensors, Superconductive Quantum Interference Device (SQUID), cooled in a cryostat with liquid helium (-269°C), can detect and quantify weak magnetic signals with 2 dimensional resolution. Through the CDDM (Figure 2) and MFM (Figure 3) and reconstructed by Magwin 2.5 software package, weak magnetic fields generated by the electrical activity of the heart could be directly analyzed.
Figure 3.
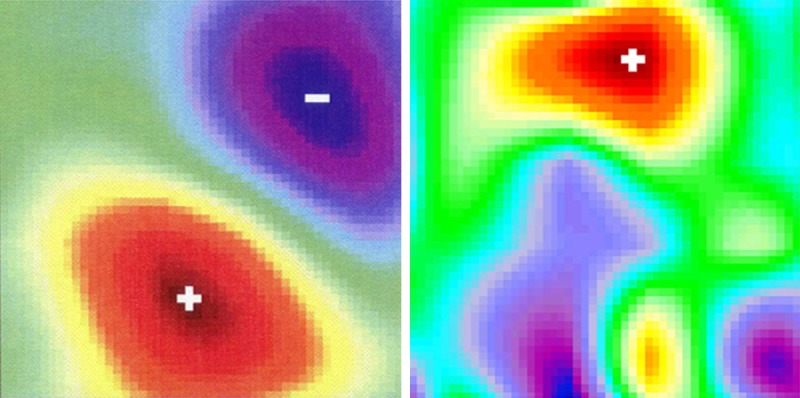
Magnetic field maps of healthy person (left) and CAD patient with triple-vessel disease (right) (At the moment of T-wave apex).
As a promising non-invasive detecting method, MCG might detect abnormal current caused by ischemic myocardium. Therefore, it could avoid the delay of the diagnosis and treatment to ischemic heart disease [3,4]. Myocardial ischemia induces changes in the electrophysiological properties of the myocardium, resulting in a decrease in resting membrane potential and conduction velocity. Also, transmembrane action potential duration is longed in ischemic area. In the normal myocardium, the current flow is almost uniform during ventricular repolarization. When ischemia is present, the current flow becomes less uniformly oriented and seems to become random. This change of current density suggests an inhomogeneity of repolarisation of the myocardial region with insufficient perfusion. Subsequently, the strength of the magnetic field becomes weaker. Therefore local currents appear on border zones of ischemic and normal myocardium. The characteristic feature of MCG is that it’s highly sensitive to tangentially propagated local currents. Thus, these local currents are displayed as additional current areas on CDDMs during ventricular repolarization phase.
As reported by Chaikovsky et al. [5] in a study on ischemic patients, MCG was performed in 49 healthy subjects and in 51 patients with CAD (18 with triple-vessel disease, 17 with double-vessel disease, 6 with one-vessel disease). The study analyzed the MCG data in current density vector maps and current line maps. The result was that maps from control group showed a more homogeneous distribution of currents compared with maps from CAD group. It revealed additional current areas with a deviated direction. The position of additional currents might reflect the anatomy of ischemic areas and associated with the relevant diseased coronary artery. The sensitivity of MCG was 91%, specificity was 84%. Sato et al. [6] reported MCG of 25 patients with CAD documented by coronary arteriography (CAG) (lumen narrowing more than 75%). MCG signals were recorded using 64-channel SQUID system in a shielded room. They found MCG abnormalities were in vector arrow maps and iso-integral maps during the repolarization phase in 88% of patients with severe coronary lesions. The sensitivity of MCG for detecting myocardial ischemia was much higher than that of resting 12-lead ECG and echocardiography.
Other studies [7-9] also reached the same conclusion that MCG could detect ST-segment displacement caused by ischemic myocardium and helpful to diagnose coronary artery disease early.
Our study showed that significant differences in R-max/T-max ratio, R value and á average angle were found between patients and control group for analysis of CDDM. Resting MCG under condition of an advanced data analysis has higher diagnostic value and is superior to Resting 12-lead ECG or Echocardiography in patients with CAD. Our work also suggested that the CDDM of healthy subjects were characterized by only one area of substantial current flow vector and the estimated vectors were directed to the left-downwards (sector from 0°~90°) at the majority of time moments during ventricular repolarization (ST-T interval). Thus, the main parameters of current maps of healthy persons are homogeneity with normal direction of maximal vectors. In contrast, maps from CAD patients showed 1~3 additional current areas with a deviated direction. So the classification was mostly class 0, 1 and 2 in control group, whereas class 3 and 4 mostly in CAD group (Figure 2). These findings are in line with the results of other studies [5,6].
Although the detection of myocardial ischemia is commonly achieved at standard surface ECG either at rest or under stress, the limitation is that the sensitivities are not high enough. In the present study, we showed that MCG was much sensitive than ECG or echocardiography in detecting myocardial ischemia. The MCG contains information complementary to ECG. It is mostly sensitive to currents tangential to the chest and circular currents which can not be detected by ECG [10]. The MCG may display better differentiating power between normal and abnormal myocardial activation than ECG. Therefore, MCG might be a complementary tool to ECG for the detection of ST-segment shift caused by ischemic myocardium. Nevertheless, the MCG signals could be filtered, averaged and the data were stored, analyzed by advanced software, which allows us to analyze all main features of heart electrical activity, such as electrical homogeneity, direction of excitation fronts spreading, intensity of electrical process in the myocardium. Thus, this study shows that resting MCG is superior to ECG and echocardiography in patients with CAD.
In conclusion, MCG under condition of an advanced data analysis has higher diagnostic value and is superior to ECG and echocardiography for patients with CAD. It could be a very useful tool for non-invasive CAD diagnosis in routine craniological practice.
Disclosure of conflict of interest
None.
References
- 1.Kozlovskyy V, Budnyk M, Stadnyuk L, et al., editors. Registration and processing of magnetocardiograms for patients with CAD. Biomag 2002 Proceedings of the 13th International Conference on Biomagnetism; Jena: University of Friedrich-Schiller; 2002. pp. 576–8. [Google Scholar]
- 2.Stroink G, Moshage W, Achenbach S. Cardiomagnetism. In: Andra W, Nowak H, editors. Magnetism in medicine. Berlin: Wiley VCH; 1998. pp. 136–189. [Google Scholar]
- 3.Kandori A, Kanzaki H, Miyatake K, Hashimoto S, Itoh S, Tanaka N, Miyashita T, Tsukada K. A method for detecting myocardial abnormality by using a total current-vector calculated from ST-segment deviation of a magnetocardiogram signal. Med Biol Eng Comp. 2001;39:21–28. doi: 10.1007/BF02345262. [DOI] [PubMed] [Google Scholar]
- 4.Zhang S, Wang Y, Wang H, Jiang S, Xie X. Quantitative evaluation of signal integrity for magnetocardiography. Phys Med Biol. 2009;54:4793–4802. doi: 10.1088/0031-9155/54/15/010. [DOI] [PubMed] [Google Scholar]
- 5.Chaikovsky I, Kohler J, Hecker T, et al., editors. Detection of coronary artery disease in patients with normal or unspecifically changed ECG on the basis of magnetocardiography. Biomag 2000 Proceedings of the 12th International Conference on Biomagnetism; Espoo, Helsinki: University of Technology; 2001. pp. 565–8. [Google Scholar]
- 6.Sato M, Terada Y, Mitsui T, Miyashita T, Kandori A, Tsukada K, editors. Detection of myocardial ischemia by magnetocardiogram using 64-channel SQUID system. Biomag 2000 Proceedings of the 12th International Conference on Bio-magnetism; Espoo, Helsinki: University of Technology; 2001. pp. 523–526. [Google Scholar]
- 7.Hänninen H, Takala P, Korhonen P, Oikarinen L, Mäkijärvi M, Nenonen J, Katila T, Toivonen L. Features of ST segment and T wave in exercise-induced myocardial ischemia evaluated with multichannel magnetocardiography. Ann Med. 2002;34:120–129. doi: 10.1080/07853890252953518. [DOI] [PubMed] [Google Scholar]
- 8.Chaĭkovskiĭ I, Boĭchak M, Sosnitskiĭ V, Miasnikov G, Rykhlik E, Sosnitskaia T, Frolov Iu, Budnik V. Magnetocardiography in clinical practice: algorithms and technologies for data analysis. Lik Sprava. 2011:3–20. [PubMed] [Google Scholar]
- 9.Wu YW, Lee CM, Liu YB, Wang SS, Huang HC, Tseng WK, Jui HY, Wang SY, Horng HE, Yang HC, Wu CC. Usefulness of Magnetocardiography to Detect Coronary Artery Disease and Cardiac Allograft Vasculopathy. Circ J. 2013;77:1783–1790. doi: 10.1253/circj.cj-12-1170. [DOI] [PubMed] [Google Scholar]
- 10.Yang F, Patterson RP. Comparison of magnetocardiography and electrocardiography in diagnosis of cardiac ischemia: A simulation study. Int J Cardiol. 2013;168:3103–3106. doi: 10.1016/j.ijcard.2013.04.073. [DOI] [PubMed] [Google Scholar]