

Abstract
The long gonadotrophin releasing-hormone agonists (GnRH-a) protocol of pituitary down regulation was widely used in controlled ovarian hyperstimulation (COH). Some clinicians prefer to use one cycle of oral contraceptives (OC) pretreatment before the traditional long GnRH-a protocol. This study was aimed to investigate whether such pretreatment could reduce the incidence of ovarian hyperstimulation syndrome (OHSS) for patients with different ovarian responses in IVF/ICSI treatment. Participants undergoing IVF/ICSI treatment with long GnRH-a protocol of pituitary down regulation in luteal phase were recruited by their potential risk of OHSS into one group of suspected high responders (227 participants) and the other group of suspected normal responders (665 participants). As for the suspected high responders, pretreatment with OC could lower the serum LH level, LH/FSH ratio and E2 level right after 14 days of pituitary down regulation. It could also lower the serum E2 level before oocytes retrieval and the count of oocytes collected. The incidence of severe OHSS was also significantly decreased. Such effect of OC on hormone profile, follicular dynamics and incidence of OHSS was not discovered in the group of suspected normal responders.
Keywords: Oral contraceptives, pituitary down regulation, IVF, ovarian hyperstimulation syndrome
Introduction
Since the introduction of gonadotrophins (Gn) into controlled ovarian hyperstimulation (COH), it has played a leading role in the IVF/ICSI procedure [1]. Along with the widespread application of COH, an iatrogenic complication namely ovarian hyperstimulation syndrome (OHSS) has been brought to the forefront of assisted reproductive technologies (ART). Golan et al. divided this disease into three categories and five grades according to its clinical symptoms and laboratory findings [2]. In the latest classification, a mild degree of OHSS was omitted, as mild forms could occur in most patients after ovarian stimulation [3]. The incidence of severe OHSS ranges from 0.5% to 5% [3]. OHSS, especially severe OHSS could significantly threaten patients’ health and even life during IVF/ICSI procedure. Lyons et al. [4] first divided this disease into early OHSS and late OHSS according to the onset of symptoms in 1994. Later, Mathur et al. [5] defined an exact timeline of early and late OHSS. The exact pathogeny of OHSS is so far still ambiguous. Researches showed that it is related with ovarian response, application of exogenous gonadotrophin, use of exogenous hCG and multiple pregnancy [3]. Its widely accepted epidemic factors includes young age, low body mass index (BMI), large antral follicular count (AFC), polycystic ovarian symptom (PCOS), and so on [3,6]. Especially the early OHSS has an intense relationship with drugs used by COH. Thus, precaution of OHSS especially in this population became more and more important during the IVF/ICSI treatment.
The depth and duration of down-regulation in luteal phase could influence the ovarian response on exogenous Gn. Research showed that one cycle of OC pretreatment before the GnRH-a pituitary down regulation could reduce the LH/FSH ratio as well as the serum DHEA-S level of PCOS patients, which could in turn improve their IVF/ICSI outcome [7]. Arbo et al. [8] found that OC pretreatment could obviously reduce the serum FSH, E2 and AMH level, as well as the mean diameter of antral follicle on day 3 of infertile patients with normal ovulation. However, controversy still exist with regard to whether such pretreatment could reduce the OHSS morbidity. Some studies indicated that one cycle of OC pretreatment before pituitary down regulation for high responders could distinctly reduce the cycle cancellation rate and the incidence of OHSS, it could also improve the pregnancy rate of this population [9]. One meta-analysis [10] noted that one cycle of OC pretreatment before GnRH-anta protocol could increase the total dose and duration of Gn, but had no definite impact on the pregnancy outcome. At the same time there were some voice against OC pretreatment claiming that it had no influence on follicular dynamics, serum hormone level, number of oocytes retrieved, number of high quality embryo, pregnancy rate and OHSS morbidity of infertile patients undergoing IVF/ICSI, especially the ones with PCOS [11].
Along with the widespread use of oral contraceptives (OC), its side effect has been also drastically discussed. The universally accepted side effect of OC was venous thrombosis [12,13]. In the same time, pregnancy itself and OHSS could also increase the risk of venous thrombosis. Thus, it is still a controversy about the effect and necessity of using OC during the IVF/ICSI procedure, especially for those who have high risk of OHSS.
This study recruited altogether 892 cycles with GnRH-a long protocol of two groups of different ovarian responders according to the risk of OHSS before IVF/ICSI treatment, one was suspected high responders and the other was suspected normal responders. We further divided this two populations respectively into the pretreatment group with one cycle of OC pretreatment and the control group. The aim of our study was to investigate the impact of OC pretreatment on morbidity of OHSS during controlled ovarian hyperstimulation in IVF/ICSI procedure.
Materials and methods
Objects
This was a prospective, non-randomized, single-center cohort study of primary or secondary infertile patients undergoing IVF/ICSI treatment at reproductive medicine center, Tongji Hospital from February 2013 to September 2013. This study was approved by the ethical committee of Tongji hospital, Tongji medical college, Huazhong University of Science and Technology. A total of 892 first fresh cycles using GnRH-a long protocols were enrolled. As we divided patients into two populations according to their individual risk of OHSS before they started their IVF treatment, the present study consisted of two parts. Part one focused on 227 suspected high responders and part two focused on 665 suspected normal responders.
All the participants were distributed into the pretreatment group or the control group according to their first visiting time and corresponding menstrual day. Those whose first visit time for IVF/ICSI down-regulation treatment was after Day 20 or before Day 5 of their menstrual cycle were distributed into the pretreatment group. And those whose first visiting time was between Day 6 to Day 19 were distributed into the control group. Because the clinicians in this reproductive medicine center routinely prescribe a cycle of OC pretreatment before the using of GnRH-a down regulation in IVF/ICSI treatment for PCOS patients, patients of irregular menses, patients of irregular ovulation (patients showed proliferative phase of endometrium on their day 1 curettage) and patients having corpus luteum cyst or dominant follicle founded by ultrasound on Day3. Thus, those patients were excluded from the present prospective cohort study.
The inclusive criteria for suspected normal responders were as followings: i) those aged between 20 and 40 years old; ii) those with the BMI between 18.5 and 30; iii) those with the AFC ≥ 6 and < 20; iv) those with a normal basal hormone profile, including FSH, LH, P, PRL and T; v) those having a regular menstrual cycle; vi) those without complicating any other internal medicine diseases; vii) those with the first fresh cycle of IVF/ICSI treatment. The inclusive criteria for suspected high responders were as followings: i) those aged between 20 and 40 years old; ii) those with the BMI ≤ 30; iii) those with the AFC ≥ 20; iv) those with a normal basal hormone profile, including FSH, LH, P, PRL and T; v) those having regular menstrual cycle; vi) those without complicating any other internal medicine diseases; vii) those with the first fresh cycle of IVF/ICSI treatment.
Protocol of luteal phase pituitary down regulation and controlled ovarian hyperstimulation
Protocol for the control group: The short-acting form of GnRH-a (Triptorelin Acetate, Diphereline, IPSEN PHARMA BIOTECH, France) was given 0.1 mg per day subcutaneously from the middle luteal phase for 10 days continuously and then was reduced to 0.05 mg per day for 4 days. The dose of GnRH-a was slightly adjusted according to the BMI individually. After 14 days of pituitary suppression, ultrasound was taken and serum hormone levels were tested including E2, LH, P and FSH. The result of B-ultrasound and serum hormone levels would guide the clinicians to judge the time and dose of adding gonadotrophin (Gn, Gonal-F,Merk Serono, Switzerland) and the time of recombinant hCG (Ovidrel, Merk Serono, Switzerland, 0.25 mg intramuscular) injection. Transvaginal ovum pick-up (OPU) was conducted after 34-36 hours from the injection of hCG. ICSI was performed when sperm quality was unexpectedly low on the day of oocytes retrieval. Protocol for OC pretreatment group: OC (Marvelon, Organon, Holland) was given one pill per day for 21 days continuously from the fifth day of menstrual cycle. And GnRH-a was given 0.05 mg per day subcutaneously from the 21st day of the same menstrual cycle for 14 days continuously. Then the ovarian hyperstimulation treatment and the related examinations were the same with the control group. A more intuitional protocol was described in Figure 1.
Figure 1.
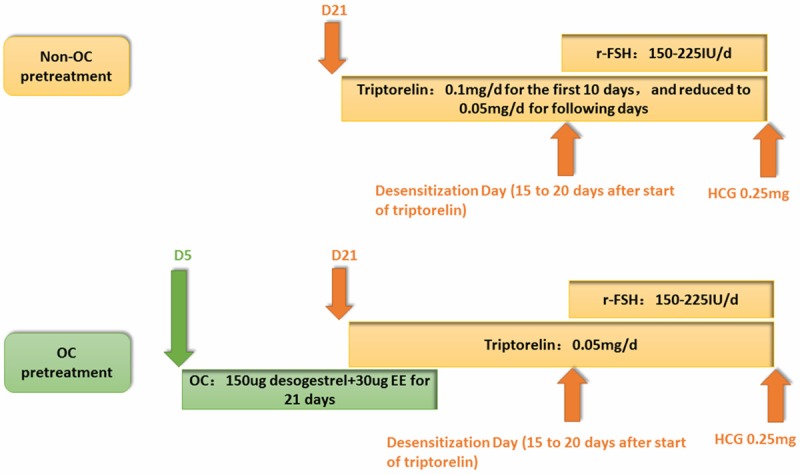
Non-OC or OC pretreatment protocols. Detail protocols were described in the main text.
Two embryos were transferred on the day three after oocytes retrieval. The excessive high-quality embryos were cryopreserved. Injections with 60 mg progesterone were administrated as luteal phase support from the day of oocytes retrieval. Clinical pregnancy was confirmed as the gestational sacs seen on ultrasound 5-7 weeks after embryo transfer.
Observational index
The main observational index in the present study included age, BMI, duration of infertility, basal serum hormone level (FSH, LH, E2, PRL, T), serum hormone level after 14 days of GnRH-a injection (FSH, LH, E2), follicular count and follicular diameters after pituitary down regulation, total dose of GnRH-a, starting dose of Gn, total dose of Gn, follicular count and follicular diameters before oocytes retrieval, number of oocytes larger than 14 mm, serum E2 level and thickness of endometrium on the day of hCG injection, number of oocytes retrieved, number of oocytes of MII phase, time gap between the day of OHSS’s first symptom and the day of oocytes retrieval, days of hospitalization, and the grading of OHSS.
Classification and grading of OHSS
OHSS presenting 9 or fewer days after oocyte retrieval was classified as early OHSS; that presenting later was classified as late OHSS [5]. Moderate OHSS refers to those with an enlargement of ovaries (6-12 cm), distinct abdominal distention and nausea, vomiting and diarrhea with the additional sonographic evidence of ascites. Severe OHSS shows the symptom of moderate OHSS with clinical evidence of hydrothorax, hemoconcentration, coagulation, electrolyte disorder, renal failure and ovarian measurements of > 12 cm [2].
Statistical methods
Statistical analysis was performed using SPSS software version 13.0 × 2 test was used to analyze nominal variables in the form of frequency tables. Normally distributed metric variables were tested with the t-test for independent samples, while non-normally distributed metric variables were analyzed with the Mann-Whitney U-test. All tests were two-tailed with a confidence level of 95% (P < 0.05). Values are expressed as the mean ± SD.
Results
There were altogether 227 cycles in part one for the suspected high responders, including 102 cycles with OC pretreatment and 125 cycles of the control group. In Part two for the suspected normal responders there were 665 cycles in total including 274 cycles with OC pretreatment and 665 cycles of the control group.
Part one: relationship between OC pretreatment and clinical outcomes for suspected high responders
No differences were found in age, BMI, duration of infertility, basal serum hormone level (FSH, LH, E2, T, PRL), AFC, starting dose of Gn, total days of Gn injection and the total dose of Gn (P > 0.05) (See Table 1). We found that one cycle of OC pretreatment for the suspected high responders would significantly deepen the depth of pituitary down regulation by reducing their serum level of LH, E2 (P < 0.05) and the LH/FSH ratio (P < 0.05). Similarly, OC pretreatment could lower the serum E2 level on the OPU day, the number of oocytes retrieved and the number of oocytes in the MII phase (P < 0.05). But the ratio of MII oocytes/number of oocytes were similar between the two groups, indicating that OC pretreatment had no influence on the quality of oocytes while reducing the number of oocytes retrieved. We found no difference in terms of the standard deviation of follicles right after the pituitary down regulation between the two groups, indicating that OC had no great impact on the homogenization of follicles for those who had regular menses (See Table 2).
Table 1.
Basic clinical data of the OC pretreatment group and the control group in the two populations
| Suspected high responders | Suspected normal responders | |||||
|---|---|---|---|---|---|---|
|
|
||||||
| Control (n = 125) | Pretreatment (n = 102) | P value | Control (n = 391) | Pretreatment (n = 274) | P value | |
| Age | 28.0 ± 3.2 | 28.1 ± 3.9 | NS | 30.4 ± 4.2 | 30.2 ± 4.0 | NS |
| BMI | 21.1 ± 2.7 | 21.6 ± 2.8 | NS | 21.7 ± 2.4 | 21.8 ± 2.4 | NS |
| Duration of infertility (years) | 3.5 ± 2.4 | 3.5 ± 2.7 | NS | 4.5 ± 3.2 | 4.4 ± 2.8 | NS |
| Basal FSH (mIU/ml) | 6.4 ± 1.4 | 6.1 ± 1.2 | NS | 6.7 ± 1.5 | 6.7 ± 1.4 | NS |
| Basal LH (mIU/ml) | 5.2 ± 2.4 | 4.9 ± 1.8 | NS | 4.2 ± 1.6 | 4.4 ± 1.8 | NS |
| Basal E2 (pg/ml) | 45.8 ± 16.6 | 43.9 ± 18.6 | NS | 45.8 ± 19.1 | 48.2 ± 18.3 | NS |
| Basal T (ng/dl) | 41.1 ± 14.6 | 40.4 ± 15.7 | NS | 36.0 ± 14.9 | 35.9 ± 15.8 | NS |
| Basal PRL (ng/ml) | 17.3 ± 8.1 | 17.0 ± 7.4 | NS | 16.1 ± 8.6 | 16.6 ± 8.6 | NS |
| AFC | 22.6 ± 2.6 | 22.9 ± 2.4 | NS | 15.2 ± 5.4 | 14.8 ± 5.3 | NS |
| Startinng dose of Gn (IU) | 204.9 ± 27.0 | 199.2 ± 30.5 | NS | 223 ± 34.0 | 219 ± 30.9 | NS |
| Duration of Gn (days) | 9.8 ± 1.4 | 9.6 ± 1.4 | NS | 9.7 ± 1.3 | 9.8 ± 1.3 | NS |
| Total dose of Gn (IU) | 1573.1 ± 474.5 | 1534.8 ± 417.9 | NS | 1904.6 ± 519.4 | 1836.4 ± 512.5 | NS |
NS, non-significant; Values are expressed as the mean ± SD; AFC, antral follicular count; Gn, gonadotrophin.
Table 2.
Clinical data in the procedure of pituitary down regulation and ovarian stimulation of the pretreatment group and control group in different ovarian responders
| Suspected high responders | Suspected normal responders | |||||
|---|---|---|---|---|---|---|
|
|
||||||
| Control (n = 125) | Pretreatment (n = 102) | P value | Control (n = 391) | Pretreatment (n = 274) | P value | |
| FSH (mIU/ml) (a) | 3.3 | 3.4 | NS | 3.6 | 3.6 | NS |
| LH (mIU/ml) (a) | 1.5 | 1.3 | P < 0.05 | 1.45 | 1.35 | NS |
| LH/FSH (a) | 0.5 ± .52 | 0.4 ± 0.2 | P < 0.05 | 0.450.2 | 0.450.2 | NS |
| E2 (pg/ml) (a) | 30.1 | 26.1 | P < 0.05 | 27.6 | 28.1 | NS |
| P (ng/ml) (a) | 0.4 | 0.4 | NS | 0.4 | 0.4 | NS |
| Standard deviation (b) | 0.7 | 0.7 | NS | 0.8 | 0.8 | NS |
| Standard deviation (c) | 2.5 | 2.5 | NS | 2.9 | 2.8 | NS |
| Total count of follicles (d) | 22.9 ± 7.2 | 22.9 ± 7.2 | NS | 18.4 ± 7.2 | 18.4 ± 7.2 | NS |
| Count of mature follicles (e) | 15.6 | 15.9 | NS | 12.9 | 12.7 | NS |
| E2 level (pg/ml) on the OPU day | 8065.9 | 6591.9 | P < 0.05 | 5207.5 | 5009.3 | NS |
| Endometrial thickness on OPU day (mm) | 11.65 | 11.15 | NS | 11.55 | 11.25 | NS |
| Number of oocytes retrieved | 19.4 | 17.0 | P < 0.05 | 12.7 | 12.0 | NS |
| Number of oocytes at the MII phase | 17.1 | 15.2 ± 7.1 | P < 0.05 | 12.41 | 12.21 | NS |
| MII oocytes in all/oocytes in all | 2139/2387 | 1537/1744 | NS | 6379/7201 | 4288/4893 | NS |
Values are expressed as the mean ± SD; (a) hormone levels after down-regulation; (b) Standard deviation of follicles’ diameter after pituitary down regulation; (c) Standard deviation of follicles’ diameter before OPU; (d) Total count of follicles on the OPU day; (e) Count of follicles larger than 14 mm on OPU day.
There were 54 cases of early OHSS and 13 cases of late OHSS in the control group(n = 125), while there were 30 cases of early OHSS and only 2 cases of late OHSS in the group of OC pretreatment (n = 102). The difference in morbidity of both early and late OHSS between the study group and the control group was statistically significant (P < 05). Among them, 15 cases of the control group and 4 cases of the pretreatment group developed into severe OHSS. The rate of severe OHSS and the duration of hospitalization between the two groups (12 days vs. 9.3 days) were statistically significant (P < 0.05) (See Table 3).
Table 3.
Detailed morbidity data of OHSS of the two groups in different ovarian responders
| suspected high responders | suspected normal responders | |||||
|---|---|---|---|---|---|---|
|
|
||||||
| control (n = 125) | pretreatment (n = 102) | P value | control (n = 391) | Pretreatment (n = 274) | P value | |
| Early OHSS (a) (n, %) | 54 (43.2) | 30 (29.4) | P < 0.05 | 107 (27.4) | 69 (25.2) | NS |
| Late OHSS (a) (n, %) | 13 (10.4) | 2 (2.0) | P < 0.05 | 24 (6.1) | 11 (4.0) | NS |
| Severe OHSS (a) (n, %) | 15 (12.0) | 4 (3.9) | P < 0.05 | 17 (7.3) | 8 (5.3) | NS |
| Mean duration of hospitalization (days) | 12 ± 6.5 | 9.3 ± 6.9 | P < 0.05 | 7.9 ± 3.5 | 6.2 ± 4.5 | NS |
(a) Morbidity of different types of OHSS.
Part two: relationship between OC pretreatment and clinical outcomes for suspected normal responders
Similar with part one, no differences were found in age, BMI, duration of infertility, basal serum hormone level (FSH, LH, E2, T, PRL), AFC, starting dose of Gn, total days of Gn injection and the total dose of Gn (P > 0.05) (See Table 1). We also noticed no statistically significant differences in the depth of down-regulation, the E2 level on the OPU day, total follicle count and the mature follicle (> 14 mm) count before oocytes retrieval, number of oocytes retrieved and number of MII oocytes (P > 0.05) between the control group and the pretreatment group, which was not the same as the results in part one. Besides, the homogeneity of follicular growth (standard deviation of follicular diameter after 14 days of down-regulation and on the OPU day) and the endometrial thickness were also similar between these two groups of suspected normal responders. These findings indicated that OC pretreatment might have no influence on the ovulation outcome and the dynamical growth of oocytes for those suspected normal responders (See Table 2).
The morbidity of neither early OHSS, late OHSS nor severe OHSS had any statistical difference between the control group and the pretreatment group (P > 0.05), indicating that pretreatment with OC had no obvious impact on the morbidity of early, late and severe OHSS after controlled hyperstimulation during IVF treatment in the suspected normal responders (See Table 3).
Discussion
According to the current studies, OHSS were commonly accompanied with low age, low BMI, history of PCOS, history of OHSS in previous pregnancy and allergic-prone habitus [3]. It was widely accepted that patients with different states of risk should have been treated individually in the process of pituitary down regulation and ovarian hyperstimulation in order to improve the outcome of IVF and at the same time to avoid OHSS.
Conventional application of OC in the field of ART included following aspects [14]: 1. to prevent the formation of luteal cyst caused by the flare-up effect of the luteal phase GnRH-a injection; 2. to modulate the menstrual cycle for the patients with irregular menstruation; 3. to have a more controlled schedule of the timing of pituitary down regulation and ovarian hyperstimulation. Earlier studies showed that a cycle of OC pretreatment before luteal phase down-regulation could avoid the formation of luteal cyst, cut down the time and dose of GnRH-a consumption by achieving the same depth of down-regulation and improve the pregnancy rate of IVF [15]. Some scholars presumed that while OC pretreatment could make the follicular grow more homogeneously, there could have been more follicles recruited and selected, leading to more oocytes retrieved and a high risk of OHSS. Our study excluded patients of PCOS, patients with irregular menses, patients showed proliferative phase of endometrium on their day 1 curettage and patients with (or had a history of) ovarian cyst. And we used the standard deviation of the follicular diameters of each participant as an index of homogeneity of follicular growth. By analysis of the standard deviation of the follicular diameters in the 892 participants, we found no significant differences between the control group and the pretreatment group neither in suspected high responders nor in suspected normal responders (P > 0.05).
The clinical symptom of OHSS was highly related to the vasoactive substances released by granulosa cells (GCs) which was triggered by HCG [16,17]. In the process of controlled ovarian hyperstimulation in IVF treatment, much more follicles were recruited and selected together with the growth of an extreme amount of GCs in the ovary, which made the patients more risky of OHSS. Early OHSS was highly related with the exogenous HCG induced release of the vasoactive substances by the extreme large amount of GCs, while late OHSS was mainly related with the endogenous HCG induced release of such substances by GCs after embryo implantation [5]. Therefore, both early OHSS and late OHSS had a relationship with the ovarian response, which included the amount of growing GCs, the number of oocytes retrieved and the serum E2 level on the OPU day.
In the current study, participants were divided into two subgroups according to their predicted ovarian response before IVF treatment. In the group of suspected high responders, participants presented a relatively higher sensitivity to the drugs of ovarian hyperstimulation and at the same time a higher risk of OHSS. In these group of patients, pretreatment of OC before the pituitary down regulation could distinctly lower their serum E2 level, LH level and the ratio of LH/FSH after 14 days of down-regulation, as well as the E2 level on the OPU day and the number of oocytes retrieved (P < 0.05), without affecting the duration and dose of Gn (P > 0.05). As OHSS was highly related to the serum level of E2 on the OPU day, the follicular count on the OPU day and the number of oocytes retrieved, it was logical that OC pretreatment could lower the incidence rate of both early and late OHSS (P < 0.05). Furthermore, OC pretreatment could also alleviate the severity of OHSS, by reducing the incidence rate of severe OHSS and the mean duration of hospitalization of the patients. This was connected with its effect on the depth of the down-regulation, the reduction of growing follicles and GCs and the suppression of the ovarian high response. The rate of MII oocytes was not changed with or without OC pretreatment, indicating that the OC pretreatment might have no impact on the quality of the oocytes. Therefore, it was reasonable to draw the conclusion that for the suspected high responders, a cycle of OC pretreatment before the pituitary down regulation could moderately reduce their ovarian high response without influencing the quality of oocytes, thus lowering their risk of OHSS.
For participants of the second group, suspected normal responders, OC pretreatment before pituitary down regulation seemed to have no impact on their depth of down-regulation, the dynamic growth of follicles, as well as the quantity and quality of oocytes (P > 0.05). No impact was also found in the morbidity of neither early nor late OHSS of OC pretreatment for those participants (P < 0.05). Similarly, it had also no obvious influence on the severity and progress of OHSS (P < 0.05). It was not arbitrary to draw the conclusion that OC pretreatment had technically no effect on the prevention of OHSS for patients with a regular menses, no history of ovarian cyst, no accompanying PCO (S) and with a suspected normal ovarian response before IVF treatment.
Robin et al. has reported a single center prospective non-randomized study about the influence of OC pretreatment on the COH outcome of PCO (S) patients, claiming that such pretreatment does not improve the pattern of follicular growth nor the oocyte and embryo quality. But the author found that the OC pretreatment could slightly disturb the endometrial growth during IVF treatment, which needed further confirmation [18]. In our study, we found no differences of endometrial thickness on the OPU day between the control group and the pretreatment group in both suspected high responders and suspected normal responders (P > 0.05).
There were still some limitations of our current work. This was a non-randomized controlled trial, with some probably unknown and uncontrollable confounding factors. Data of IVF and ICSI were mixed analyzed, without recording the vitality and density of sperms on the day of fertilization. Therefore the outcome index of IVF like embryo quality, implantation rate and pregnancy rate were not analyzed in the current study. But such limitation of data did not influence our main observation parameter which was the morbidity, risk and severity of OHSS.
Conclusion
In conclusion, one cycle of OC pretreatment before the pituitary down regulation with GnRH-a for suspected high responders could moderately reduce their ovarian response to gonadotropins and obviously lower the morbidity rate of both early and late OHSS as well as the severe OHSS. However, such pretreatment for suspected normal responders seemed to have no impact on the outcome of ovarian hyperstimulation and the morbidity of OHSS. For both suspected high responders and suspected normal responders, one cycle of OC pretreatment before pituitary down regulation had hardly any influence on the homogeneity and quality of oocytes. To draw a more reliable conclusion about the influence of OC pretreatment on OHSS for different ovarian responders, a well-designed randomized control trial in a much larger and well-powered population is still needed.
Acknowledgements
This work was supported by the National Science Foundation of China (No. 81200474). We gratefully acknowledge the staff at the Reproductive Medicine Center of Tongji Hospital, Wuhan, China for their help in patients grouping and data collecting.
Disclosure of conflict of interest
None.
References
- 1.Navot D, Bergh PA, Laufer N. Ovarian hyperstimulation syndrome in novel reproductive technologies: prevention and treatment. Fertil Steril. 1992;58:249–261. doi: 10.1016/s0015-0282(16)55188-7. [DOI] [PubMed] [Google Scholar]
- 2.Golan A, Ron-el R, Herman A, Soffer Y, Weinraub Z, Caspi E. Ovarian hyperstimulation syndrome: an update review. Obstet Gynecol Surv. 1989;44:430–440. doi: 10.1097/00006254-198906000-00004. [DOI] [PubMed] [Google Scholar]
- 3.Delvigne A, Rozenberg S. Epidemiology and prevention of ovarian hyperstimulation syndrome (OHSS): a review. Hum Reprod Update. 2002;8:559–577. doi: 10.1093/humupd/8.6.559. [DOI] [PubMed] [Google Scholar]
- 4.Lyons CA, Wheeler CA, Frishman GN, Hackett RJ, Seifer DB, Haning RV Jr. Early and late presentation of the ovarian hyperstimulation syndrome: two distinct entities with different risk factors. Hum Reprod. 1994;9:792–799. doi: 10.1093/oxfordjournals.humrep.a138598. [DOI] [PubMed] [Google Scholar]
- 5.Mathur RS, Akande AV, Keay SD, Hunt LP, Jenkins JM. Distinction between early and late ovarian hyperstimulation syndrome. Fertil Steril. 2000;73:901–907. doi: 10.1016/s0015-0282(00)00492-1. [DOI] [PubMed] [Google Scholar]
- 6.Heijnen EM, Eijkemans MJ, Hughes EG, Laven JS, Macklon NS, Fauser BC. A meta-analysis of outcomes of conventional IVF in women with polycystic ovary syndrome. Hum Reprod Update. 2006;12:13–21. doi: 10.1093/humupd/dmi036. [DOI] [PubMed] [Google Scholar]
- 7.Damario MA, Barmat L, Liu HC, Davis OK, Rosenwaks Z. Dual suppression with oral contraceptives and gonadotrophin releasing-hormone agonists improves in-vitro fertilization outcome in high responder patients. Hum Reprod. 1997;12:2359–2365. doi: 10.1093/humrep/12.11.2359. [DOI] [PubMed] [Google Scholar]
- 8.Arbo E, Vetori DV, Jimenez MF, Freitas FM, Lemos N, Cunha-Filho JS. Serum anti-mullerian hormone levels and follicular cohort characteristics after pituitary suppression in the late luteal phase with oral contraceptive pills. Hum Reprod. 2007;22:3192–3196. doi: 10.1093/humrep/dem258. [DOI] [PubMed] [Google Scholar]
- 9.Damario MA. Ovarian hyperstimulation syndrome prevention strategies: oral contraceptive pills-dual gonadotropin-releasing hormone agonist suppression with step-down gonadotropin protocols. Semin Reprod Med. 2010;28:468–474. doi: 10.1055/s-0030-1265673. [DOI] [PubMed] [Google Scholar]
- 10.Griesinger G, Venetis CA, Marx T, Diedrich K, Tarlatzis BC, Kolibianakis EM. Oral contraceptive pill pretreatment in ovarian stimulation with GnRH antagonists for IVF: a systematic review and meta-analysis. Fertil Steril. 2008;90:1055–1063. doi: 10.1016/j.fertnstert.2007.07.1354. [DOI] [PubMed] [Google Scholar]
- 11.de Ziegler D, Gayet V, Aubriot FX, Fauque P, Streuli I, Wolf JP, de Mouzon J, Chapron C. Use of oral contraceptives in women with endometriosis before assisted reproduction treatment improves outcomes. Fertil Steril. 2010;94:2796–2799. doi: 10.1016/j.fertnstert.2010.05.056. [DOI] [PubMed] [Google Scholar]
- 12.de Bastos M, Stegeman BH, Rosendaal FR, Van Hylckama Vlieg A, Helmerhorst FM, Stijnen T, Dekkers OM. Combined oral contraceptives: venous thrombosis. Cochrane Database Syst Rev. 2014;3:CD010813. doi: 10.1002/14651858.CD010813.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.ESHRE Capri Workshop Group. Venous thromboembolism in women: a specific reproductive health risk. Hum Reprod Update. 2013;19:471–482. doi: 10.1093/humupd/dmt028. [DOI] [PubMed] [Google Scholar]
- 14.Bozdag G, Esinler I, Yarali H. Pretreatment with oral contraceptive pills does not influence the pregnancy rate in the long leuprolide acetate protocol. Gynecol Obstet Invest. 2012;73:53–57. doi: 10.1159/000329730. [DOI] [PubMed] [Google Scholar]
- 15.Biljan MM, Mahutte NG, Dean N, Hemmings R, Bissonnette F, Tan SL. Effects of pretreatment with an oral contraceptive on the time required to achieve pituitary suppression with gonadotropin-releasing hormone analogues and on subsequent implantation and pregnancy rates. Fertil Steril. 1998;70:1063–1069. doi: 10.1016/s0015-0282(98)00333-1. [DOI] [PubMed] [Google Scholar]
- 16.Ferrara N. Vascular endothelial growth factor: basic science and clinical progress. Endocr Rev. 2004;25:581–611. doi: 10.1210/er.2003-0027. [DOI] [PubMed] [Google Scholar]
- 17.Elchalal U, Schenker JG. The pathophysiology of ovarian hyperstimulation syndrome-views and ideas. Hum Reprod. 1997;12:1129–1137. doi: 10.1093/humrep/12.6.1129. [DOI] [PubMed] [Google Scholar]
- 18.Decanter C, Robin G, Thomas P, Leroy M, Lefebvre C, Soudan B, Lefebvre-Khalil V, Leroy-Martin B, Dewailly D. First intention IVF protocol for polycystic ovaries: does oral contraceptive pill pretreatment influence COH outcome? Reprod Biol Endocrinol. 2013;11:54. doi: 10.1186/1477-7827-11-54. [DOI] [PMC free article] [PubMed] [Google Scholar]