

Abstract
Intraperitoneal hemorrhage caused by a uterine myoma is rare. A 54-year-old woman was admitted to the emergency room; on admission, she was in cardiopulmonary arrest with pulseless electrical activity. Transabdominal ultrasonography revealed hyperechoic fluid filled almost the entire abdominal cavity. On contrast-enhanced computed tomography, extravasation of contrast material was observed inside the fluid, although the bleeding site was not identifiable. An emergency operation was performed to stabilize the patient. There was pulsating bleeding from a subserosal myoma on the posterior wall of the uterus; the myoma measured approximately 6 cm in maximum diameter. After resection of the myoma, the bleeding stopped. Pathological assessment of the resected specimen revealed a ruptured arterial aneurysm, approximately 8 mm in diameter, situated on the surface of a leiomyoma without degeneration. Spontaneous rupture of a vein or an artery overlying a myoma has been documented in the English literature, though it is extremely rare. Rupture of a vein is a more frequent occurrence than the rupture of an artery. This is the first reported case documenting a ruptured arterial aneurysm overlying a myoma.
Keywords: Uterus, myoma, artery, aneurysm, rupture, hemoperitoneum
Introduction
In a gynecological setting, hemoperitoneum is usually a result of an ectopic pregnancy, a ruptured corpus luteum, or adnexal torsion [1-3]. As a cause of hemoperitoneum, spontaneous rupture of a vein or an artery overlying a myoma has been documented in the English literature, though it is extremely rare [4-13]. Even if cases reported in non-English language publications are included, there have been less than 100 documented cases to date [9]. Cases of rupture of a vein are more frequent [4-11] than those of rupture of an artery [11-13]. Herein, we present the first reported case of a rupture of an arterial aneurysm overlying a myoma, which resulted in cardiopulmonary arrest due to massive intraperitoneal hemorrhage.
In the differential diagnosis of intraperitoneal hemorrhage, rupture of a vessel overlying a myoma should be considered.
Case report
A 54-year-old woman was brought to the emergency room via ambulance. On admission, she was in cardiopulmonary arrest with pulseless electrical activity. Cardiopulmonary resuscitation with chest compressions and intubation were started immediately; saline and an appropriate amount of epinephrine and norepinephrine were administered. She achieved spontaneous circulation after 14 minutes. Transabdominal ultrasonography revealed hyperechoic fluid filling almost the entire abdominal cavity, suggestive of an extremely large hemorrhage. Once the patient was stable, we examined the origin of the bleeding using contrast-enhanced computed tomography (CT). This revealed an extremely large hemorrhage with extravasation of contrast material (Figure 1). Although the exact site of bleeding was not identified, vessels in the pelvic cavity were considered potential candidates. Laboratory tests on admission indicated relatively minor abnormalities, considering the severity of her condition: hemoglobin (Hb), 10.8 g/dL; platelets (Plt), 31.4 × 104/μL; aspartate transaminase (AST), 41 U/L; alanine aminotransferase (ALT), 45 U/L. However, after recovery from cardiopulmonary arrest these results had worsened significantly owing to hypovolemic shock caused by the large intraperitoneal hemorrhage: Hb, 5.3 g/dL; Plt, 175 × 104/μL; AST, 269 U/L; ALT, 362 U/L. Blood transfusion was initiated.
Figure 1.
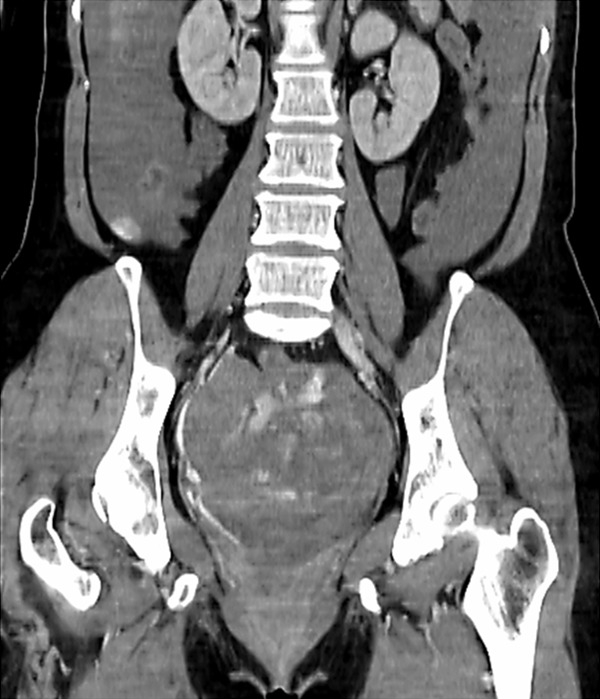
Contrast-enhanced computed tomography. A massive hemoperitoneum is seen, with extravasation of contrast material.
Suspecting a gynecological cause, an emergency operation was planned, to stabilize the patient and make an exact diagnosis. Emergency laparotomy was performed under general anesthesia. On reaching the abdominal cavity, there was evidence of an extremely large hemorrhage, with an estimated blood loss of over 3000 mL. Inspection of the uterus revealed multiple myomas; pulsating bleeding was coming from a subserosal myoma on the posterior wall of the uterus, which measured approximately 6 cm in maximum diameter. Following immediate resection of the myoma, the bleeding stopped, and the patient gradually stabilized. The patient was admitted to the intensive care unit for post-operative care.
Pathological examination of the resected specimen revealed the lesion to be a leiomyoma, without degeneration, with an overlying ruptured arterial aneurysm. The size of the leiomyoma was 6.5 × 6 × 5.5 cm and the diameter of the aneurysm was approximately 8 mm (Figure 2). A point near the rupture site was surrounded with fibrin exudate (Figure 3A). The wall of the artery, continuous with the ruptured aneurysm, contained an internal elastic lamina (Figure 3B); this was considered to be strong evidence of an arterial origin.
Figure 2.

Gross findings. Myoma (Left, uncut specimen; Right, cut surface). Boxed areas indicate the arterial aneurysm, which is clearly visible on the cut surface.
Figure 3.
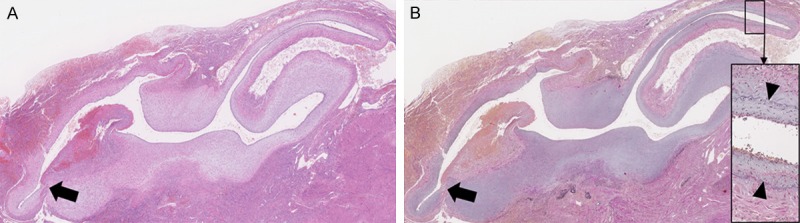
Histopathological findings. A. Point near the site of rupture (arrow), surrounded with fibrin exudate (hematoxylin and eosin stain, ×12.5). B. Point near the site of rupture (arrow). Inset shows a magnified view of the boxed area, which corresponds to the area of the arterial wall that was continuous with the aneurysm; the internal elastic lamina is stained black (arrowheads) (elastica van Gieson stain, ×12.5).
It was possible to make an exact diagnosis of hypovolemic shock and cardiopulmonary arrest, caused by intra-abdominal bleeding, secondary to rupture of an arterial aneurysm on the surface of a subserosal myoma.
The postoperative course was uneventful; the patient’s condition improved and she was discharged 14 days after surgery.
Discussion
Intraperitoneal hemorrhage associated with a uterine leiomyoma is rare, in spite of the fact that uterine myomas are one of the most frequently encountered tumors [14]. Well-known acute complications of myomas include torsion of a subserosal pedunculated myoma, urinary retention, venous thromboembolism, and hemorrhage due to degeneration of a myoma [15]. A large hemorrhage as a result of spontaneous rupture of a vessel overlying a myoma is rare [9].
Several factors have been postulated as causes of spontaneous rupture of a vein or an artery overlying a myoma. One of the probable causes of such a venous rupture is increased venous pressure, as occurs during menstruation, when straining at stool, or when lifting heavy weights [6]. Alternatively, increased abdominal pressure may cause passive venous congestion, and result in the rupture of a superficial vein [9]. Regarding venous rupture, the size of the myoma appears not to be a direct risk factor [5]. In contrast, in the case of an arterial rupture, a large myoma might overstretch the surface artery, resulting in rupture [13]. In addition, it is suspected that increased arterial pressure of a surface artery due to increased abdominal pressure could lead to rupture of the artery. With regard to the present case, we speculate that an increase blood pressure due to an unknown cause may have played a part in the rupture.
Imaging modalities, including ultrasound and CT, may help confirm the differential diagnosis; however, as demonstrated in our case, imaging is unable to detect the site of bleeding [12]. Making an exact diagnosis is often delayed until surgery is performed.
In conclusion, massive hemoperitoneum secondary to the spontaneous rupture of a vessel overlying a myoma is rare. It should, however, be kept in mind when reviewing a female patient with an acute abdomen and hypovolemic shock, especially in a patient with either known or radiologically apparent myomas. While it is a rare event, it may be life-threatening, and needs prompt surgical intervention to stabilize the patient and to establish the diagnosis. Among the types of vessel involved, cases of venous rupture are more frequent than those of arterial rupture. This report is the first to present rupture of an arterial aneurysm overlying a myoma.
Disclosure of conflict of interest
None.
References
- 1.Chen CH, Lee WL, Chiu LH, Sun HD, Liu WM, Wang PH. A cohort study to evaluate the effectiveness of laparoscopic-guided local injection of etoposide in the management of women with unruptured tubal pregnancy. Fertil Steril. 2011;96:654–658. doi: 10.1016/j.fertnstert.2011.06.033. [DOI] [PubMed] [Google Scholar]
- 2.Choi HJ, Kim SH, Kim SH, Kim HC, Park CM, Lee HJ, Moon MH, Jeong JY. Ruptured corpus luteal cyst: CT findings. Korean J Radiol. 2003;4:42–45. doi: 10.3348/kjr.2003.4.1.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Huang BS, Wang PH. Ovarian torsion during pregnancy. Taiwan J Obstet Gynecol. 2011;50:409–410. doi: 10.1016/j.tjog.2011.10.002. [DOI] [PubMed] [Google Scholar]
- 4.Su WH, Cheung SM, Chang SP, Lee WL. Internal bleeding from a ruptured serosal vein covering the myoma surface mimicking upper gastrointestinal bleeding. Taiwan J Obstet Gynecol. 2008;47:352–354. doi: 10.1016/S1028-4559(08)60142-4. [DOI] [PubMed] [Google Scholar]
- 5.Jain P, Pradhan P, Cietak KA, Anyanwu L. Acute abdomen following spontaneous variceal rupture overlying uterine leiomyoma. J Obstet Gynaecol. 2004;24:589. doi: 10.1080/01443610410001722833. [DOI] [PubMed] [Google Scholar]
- 6.Buttery BW. Spontaneous haemoperitoneum complicating uterine fibromyoma. Aust N Z J Obstet Gynaecol. 1972;12:210–213. doi: 10.1111/j.1479-828x.1972.tb00504.x. [DOI] [PubMed] [Google Scholar]
- 7.Mattison DR, Yeh SY. Hemoperitoneum from rupture of a uterine vein overlying a leiomyoma. Am J Obstet Gynecol. 1980;136:415–416. doi: 10.1016/0002-9378(80)90876-5. [DOI] [PubMed] [Google Scholar]
- 8.Dahan MH, Ahmadi R. Spontaneous subserosal venous rupture overlying a uterine leiomyoma. A case report. J Reprod Med. 2002;47:419–420. [PubMed] [Google Scholar]
- 9.Danikas D, Theodorou SJ, Kotrotsios J, Sills C, Cordero PE. Hemoperitoneum from spontaneous bleeding of a uterine leiomyoma: a case report. Am Surg. 1999;65:1180–1182. [PubMed] [Google Scholar]
- 10.Badawy AH. Diffuse intraperitoneal haemorrhage from surface vein of a fibromyoma. Br Med J. 1961;1:717–718. doi: 10.1136/bmj.1.5227.717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Akahira J, Ito K, Nakamura R, Yajima A. Massive intraperitoneal hemorrhage and hypovolemic shock due to rupture of a coronary vessel of a uterine leiomyoma: a report of two cases. Tohoku J Exp Med. 1998;185:217–222. doi: 10.1620/tjem.185.217. [DOI] [PubMed] [Google Scholar]
- 12.Chen CH, Lin JY, Tzeng CR, Chiu LH, Liu WM. Hemoperitoneum secondary to rupture of a superficial uterine artery overlying a subserous myoma with no predisposing factors in a young woman. Taiwan J Obstet Gynecol. 2013;52:133–134. doi: 10.1016/j.tjog.2013.01.018. [DOI] [PubMed] [Google Scholar]
- 13.Horowitz E, Dekel A, Feldberg D, Rabinerson D. Massive hemoperitoneum due to rupture of an artery overlying a uterine leiomyoma: a case report. Acta Obstet Gynecol Scand. 2005;84:408–409. doi: 10.1111/j.0001-6349.2005.0475d.x. [DOI] [PubMed] [Google Scholar]
- 14.Su WH, Lee WL, Cheng MH, Yen MS, Chao KC, Wang PH. Typical and atypical clinical presentation of uterine myomas. J Chin Med Assoc. 2012;75:487–493. doi: 10.1016/j.jcma.2012.07.004. [DOI] [PubMed] [Google Scholar]
- 15.Gupta S, Manyonda IT. Acute complications of fibroids. Best Pract Res Clin Obstet Gynaecol. 2009;23:609–617. doi: 10.1016/j.bpobgyn.2009.01.012. [DOI] [PubMed] [Google Scholar]