

Abstract
Objectives:
To identify, synthesize, and summarize issues and challenges related to the culture and language differences of the health workforce in Saudi Arabia.
Methods:
A comprehensive systematic review was conducted in May 2014 to locate published articles. Two independent researchers in consultation with several experts used 4 electronic databases (ISI Web of Knowledge, Science Direct, PubMed, and Cochrane) to scrutinize articles published from January 2000 - March 2014. Each of the studies was given a quality assessment rating of weak, moderate, or strong, and was evaluated for methodological soundness using Russell and Gregory’s criteria.
Results:
The online literature search identified 12 studies that met the inclusion criteria. Lack of knowledge of non-Muslim nurses or culture in Saudi Arabia, difficulties in achieving cultural competence, and culture shock were documented as cultural difference factors. Issues in language difference include the clarity of language use by health care providers in giving information and providing adequate explanation regarding their activities.
Conclusion:
The available information provided by this review study shows that there is a communication barrier between patients and health care workers such as healthcare workers demonstrate low cultural competency. Despite the fact that the government provides programs for expatriate healthcare workers, there is a need to further improve educational and orientation programs regarding the culture and language in Saudi Arabia.
Effective communication with patients and health care workers is a key process in safe and quality health care.1 Patient and clinician relationships rely on good communication, resulting in improved patient satisfaction, adherence to medical recommendations, and better healthcare outcomes.2 Effective patient and clinician interaction starts from the patient inquiry regarding symptoms of the disease, to discussing the treatment, and management plan of the clinician.2 According to Stewart,3 many healthcare professionals believe that communication is more effective when it is responsive to patient needs, values, and preferences. Factors that influence this communication include cultural differences, low health literacy, and language differences.1 Cultural misunderstanding between patients and predominantly expatriate health care providers is another factor contributing to patient dissatisfaction and poor quality of care. The cultural setting of Saudi Arabia is a unique blend of Arabic with an Islamic influence.4 The beliefs and attitudes of Saudi people are characterized by the Arabic tribal traditions and customs, and the Islamic worldview.4,5 The uniqueness of Saudi culture, coupled with the large number of expatriate health professionals who have a limited knowledge of Saudi culture, aggravate the problem of providing high quality of care and may cause potential cultural conflicts, which may lead to patient dissatisfaction. According to the Ministry of Health (MOH), most healthcare workers in Saudi Arabia such as nurses are expatriates from countries like India, the Philippines, Malaysia, Australia, America, the United Kingdom, South Africa, and other Middle Eastern countries with different cultural backgrounds.6-9 Not only do cultural backgrounds differ among these healthcare workers, language differences also serve as a barrier to effective communication. This language barrier is often not immediately an issue because of their proficiency in English. However, the Arabic language is the primary language in Saudi Arabia and not all patients understand or are proficient in the English language.10 With the increasing number of expatriates’ healthcare workers, effective communication may not occur and the quality of patients’ healthcare as well as their safety will be at risk. Therefore, we aim to perform a systematic review to identify, synthesize, and summarize the issues and challenges of effective communication between patients and health workers, and to provide recommendations for improvements.
Methods
A comprehensive systematic review was conducted in May 2014. We extensively searched electronic databases (ISI Web of Knowledge, Science Direct, PubMed and Cochrane) dating from January 2000 through March 2014. The search terms used were cultural difference, language difference, barriers, health care workers, health workforce, and Saudi Arabia. Grey literature was performed (King Saud University - Central Library) using electronic database and reference list of included articles were scanned for further studies. The electronic search was completed in consultation with several experts and supplemented by several databases. We included studies if they met the following criteria: (1) focus on issues or areas of concern as they relate to cultural and language differences; (2) focus on barriers in quality of care of the health workforce in Saudi Arabia; and (3) studies carried out with different designs and method of analysis - case-control studies or cross-sectional studies and review studies. Following the literature search, titles and abstracts were independently assessed by 2 researchers for inclusion criteria. Studies not carried out in Saudi Arabia were excluded in this phase. After the preliminary screening, the included studies were analyzed and reviewed by a specialist for significance and potential duplication. Details of the author of the study, location of the study, sample, and major findings were extracted from each study that met the inclusion criteria.
Quality appraisal and synthesis of included studies
After the extraction of all included studies, each study was critically appraised by a specialist using the health evidence.org tool for reviews.11 Meta-analysis was not conducted due to different study designs of the included studies. Each of the studies was appraised and was evaluated for methodological soundness using the Russell and Gregory’s criteria.12 Evaluation was based on whether the article answered each of the following questions: 1) Is the research question clear and adequately substantiated? 2) Is the design appropriate for the research question? 3) Was the sampling method appropriate for the research question and design? 4) Was data collected and managed systematically? 5) Was the data analyzed appropriately? A quality score was applied to each study using these guidelines. Each study was given a quality score ranging from 0 to 5, where 5 is the highest, based on whether they met each of the guidelines.
Results
The online literature search yielded 79 results, and 10 references were pre-selected from searching the grey literature and reference list of included articles because they aligned with study objectives. In total, 39 studies passed the preliminary screening and went for more detailed evaluation. After an extensive evaluation, only 12 studies met the inclusion criteria. Figure 1 shows information of the included studies. Descriptions of included studies are presented in Table 1. Details of the quality appraisal and evaluation of included studies are shown in Table 2. We focused on 2 factors that affect this communication such as cultural diversity and language differences. Major findings are presented in Table 3.
Figure 1.

Flow diagram for the selection of studies included in a systematic review from Saudi Arabia.
Table 1.
Description of included studies in a systematic review from Saudi Arabia.
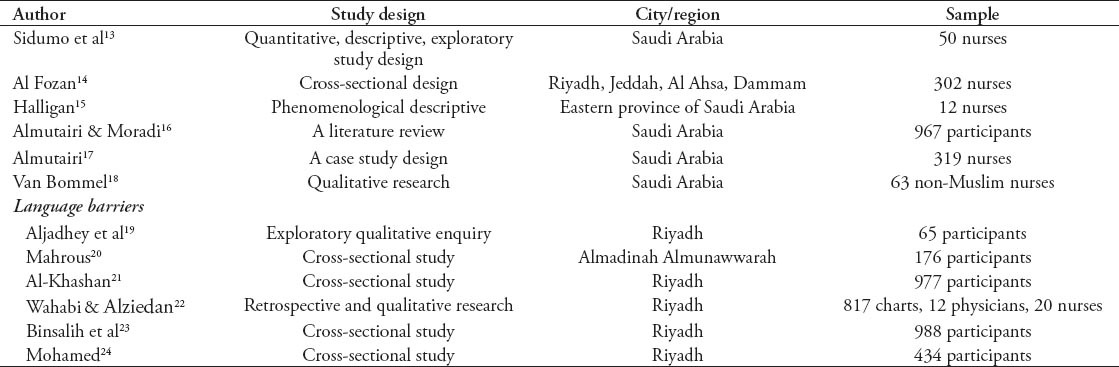
Table 2.
Quality assessment of reviewed studies included in a study in Saudi Arabia.
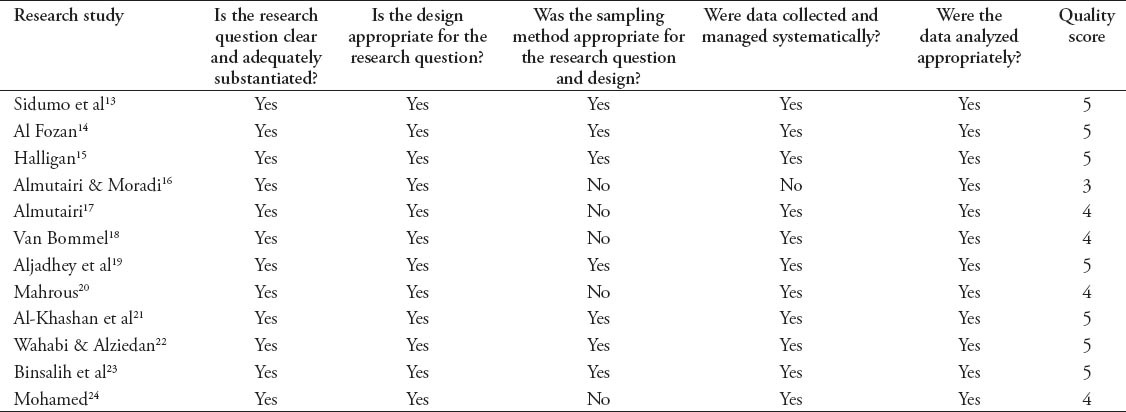
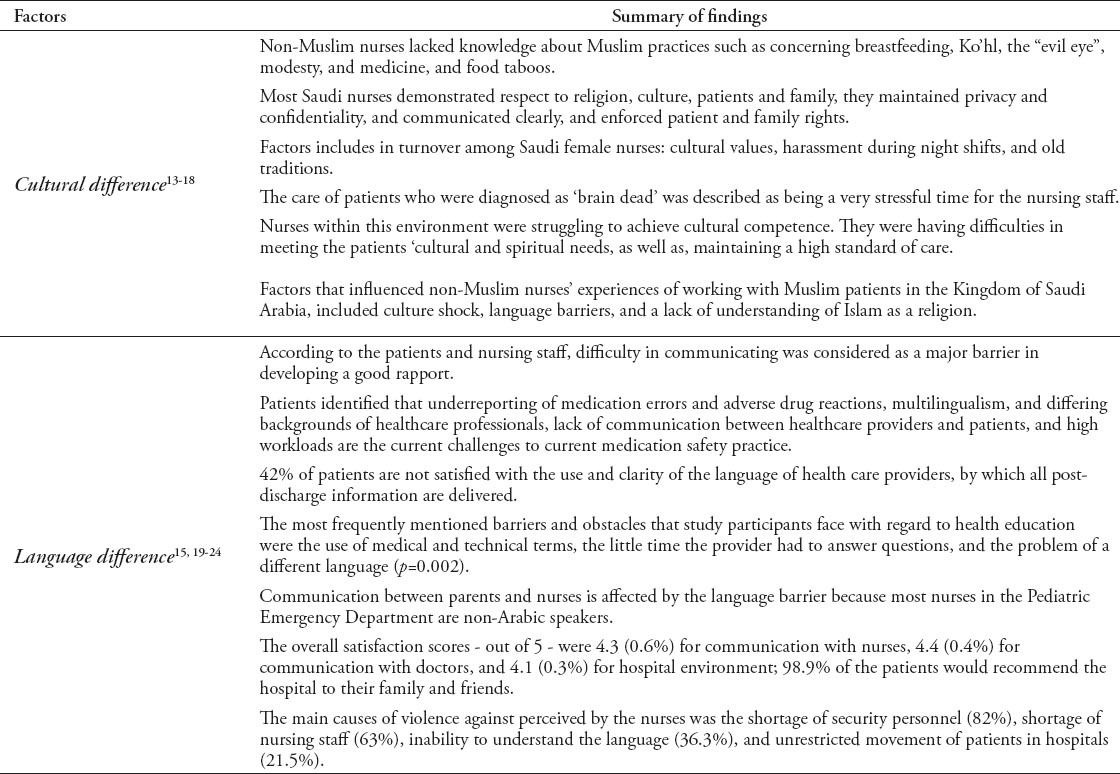
Table 3.
Summary of findings in a study in Saudi Arabia.
Culture
Six studies showed issues of health care workers concerning the influence of cultural diversity on the quality of patient care. A quantitative explorative study13 examined the cultural knowledge of non-Muslim nurses working in an obstetrics unit. The results showed a lacked of knowledge of non-Muslim nurses about Muslim practices such as breastfeeding, Ko’hl, the “evil eye,” modesty, and medicine, and food taboos. A cross-sectional study14 examined patients and family caregiver satisfaction within the care delivered by Saudi nurses in 3 major healthcare facilities in Saudi Arabia. Participants were highly satisfied in areas of respecting religion and culture, maintaining privacy and confidentiality, communication, and professionalism. A qualitative study15 examined the experiences of critical care nurses in caring for patients for individuals who follow Islam. The study found that the care of patients who were diagnosed as brain dead was very stressful as perceived by the nurses. A literature review study by Almutairi and Moradi16 identified and summarized the factors that can cause turnover among Saudi nurses. These factors include family disagreement, different cultural values, mingling with men, and the unwillingness of young people to marry a nurse, harassment during night shifts, and old traditions. A case study by Almutairi17 investigates the influence of cultural diversity and multicultural nursing workforce on quality and safety of patient care. Nurses have difficulties achieving cultural competence, such as meeting the patients’ cultural and spiritual needs and maintaining a high standard of care. Furthermore, there was inadequate support of an organization to manage cultural diversity issue. The qualitative and descriptive study by Van Bommel18 describes the experience of expatriate non-Muslim nurses working in the Cardiac Intensive Care unit. Factors that influenced non-Muslim nurses’ experiences of working with patients include culture shock, language barriers, and a lack of understanding of Islam.
Language differences
Seven studies show issues of health care workers concerning language differences. In a phenomenological descriptive study by Halligan,15 critical care nurses experienced difficulty in communicating due to language differences. This was considered a major barrier in developing a good patient-provider relationship. Nurses described their patients as eager to speak in their own language, although they knew that the nurses did not understand them. Language barriers were also identified in an explorative qualitative study by Aljahdhey et al.19 Communication between healthcare professionals and patients’ multilingualism and different backgrounds of healthcare providers are the challenges to current medication safety practices. A cross-sectional study by Mahrous,20 investigated patients’ perception, and satisfaction regarding discharge information received from health care professionals. The study found that 42% of the patients are not satisfied with the clarity and the use of the language of health care providers in communicating post discharge information. This study was similar to Al-Khashan et al,21 which found that the barriers and obstacles that the participants most frequently experienced with regard to health education, were the use of medical and technical terms, the little time the provider had to answer questions, and the problem of a different language. In a study by Wahabi and Alziedan,22 communication in giving instructions and information between patients’ parents and nurses regarding asthma management, such as the use of inhalers and spacers of pediatric patients is affected by language difference, as most nurses are non-Arabic speakers. In a cross-sectional survey by Binsalih et al23 that investigated the experience and degree of satisfaction of patients among healthcare professionals in a tertiary hospital, higher satisfaction was observed in patients admitted in a Saudi tertiary care hospital in communication skills of doctors and nurses. In a cross-sectional study by Mohamed24 that determined the extent of work-related violence against nurses, 36% of nurses perceived that inability to understand the language was the main causes of violence against them.
Discussion
This study identified and summarized the issues of effective communication between patients and healthcare providers. Barriers in communication between patients and health care workers often cause unnecessary errors, excess pain, poor quality care, and even death. The results of the included studies clearly show that there is a communication issue between patients and health care providers. Lack of knowledge of non-Muslim nurses regarding Saudi Arabian culture, difficulties in achieving cultural competence, and culture shock were documented as cultural difference factors in barriers of effective communication. Each country has its own unique culture that defines the normative values of an individual or a group. This culture determines behavior that outlines all aspects of their lives.25 When a health care provider is knowledgeable of the cultural customs, this empowers them to provide better care and help avoid misunderstandings among co-workers, residents/patients, and families.26 It is significant that a health care provider is knowledgeable and culturally competent and can effectively interact with people of different cultures. Some of the benefits of a culturally competent healthcare and healthcare workforce include less diagnostic errors; successful resident/patient therapeutic education; avoidance of drug complications; greater adherence to medical advice; and access to high quality clinicians.27,28 The National Center for Cultural Competence at Georgetown University provides a checklist to evaluate an organization’s cultural competency.29 This checklist will provide a clearer picture of current strengths and areas of opportunity in an organization. It may also serve as baseline information on what areas should be improved.
Another factor that affects communication among healthcare workers in Saudi Arabia is language barriers.
In this review, 7 studies showed that there is a language barrier or difficulty in communicating between patients and providers, and only one study showed a good communication relationship.15,19-24 Issues include the clarity of language use by health care providers in giving information and providing adequate explanation about their activities. These findings use similar results of research literature and quantitative studies from US populations.29 Language barriers arise across the entire continuum of health care, especially in countries that have a large number of expatriate health care workers. The language proficiency of a patient or a healthcare provider is a significant factor that is needed for effective communication. When a provider’s language differs from his or her patients, preventable adverse events may occur. For example, most healthcare professionals working in Saudi Arabia such as nurses are expatriates from different countries.8 These differences can compromise the quality of healthcare such as adherence in providing information regarding the disease and response to treatment regimens. The government of Saudi Arabia has made efforts to attract and retain more Saudi healthcare workers such as in the nursing profession, according to a 2006 study.30 However, it has been estimated that 25 years will be needed to train enough Saudi nurses in the Kingdom.
The results of this review study indicate a need to improve the communication between patient and healthcare workers in the Kingdom in order to attain high quality and safe health care. Based on a study, communication barriers, aside from poor clinical management, lead to preventable adverse events in health care settings.31 Addressing this communication barrier is a substantial ingredient in formulating strategies such as organizational safety and may bring down health care costs because of the reduction in medical errors and increased access to preventive maintenance.32 According to experts, the initial step in dealing with this issue is to first assess the language and communication needs of the population.33 New and innovative approaches are also necessary to meet the needs of patients, such as training of health professionals that focus on communication skills of intercultural communication between patients with different cultural backgrounds.34,35
There are limitations that should be considered in this review. Most of the included studies were performed using cross-sectional analysis, which only describes association and not the causality. Another limitation of this review was the limited number of included studies that reported each factor, and may not capture all issues related to barriers in communication, which also limits the generalizability of the study. In addition, the number of samples of the included studies cannot determine or represent the whole Kingdom, which may result in study bias. Hence, there is a need for additional and larger studies that will determine these issues and factors that may contribute to communication barriers in the patient and health care provider relationship. Although this study has some limitations, the results may be of interest to investigators because the evidence and results of this literature search highlight the barriers affecting the communication of patient and health care providers in the Kingdom. Hence, it will be beneficial to address these issues and continue to increase the quality of healthcare.
In conclusion, the available information provided by this review study shows that there is a communication barrier between patients and health care workers. Despite the fact that the government provides programs for expatriate healthcare workers, the issues are still rising. Thus, the quality of healthcare and safety of patients and healthcare workers are still at risk. Healthcare workers such as nurses demonstrate low cultural competency, and need additional educational and orientation programs regarding the culture in Saudi Arabia. Health care facilities may also provide language services such as hiring interpreters, using written materials, or communication boards. In addition, the Ministry of Health could also require Arabic language proficiency test for professionals, expatriates, and non-Arabic speakers applying for work in Saudi Arabia. The language proficiency test should cover language knowledge, speaking ability, reading ability, and listening ability.
Footnotes
Related Articles.
Al-Haqwi AI, Al-Wahbi AM, Abdulghani HM, van der Molen HT. Barriers to feedback in undergraduate medical education. Male students’ perspective in Central Saudi Arabia. Saudi Med J 2012; 33: 557-561.
Al-Khathami AM, Kojan SW, Aljumah MA, Alqahtani H, Alrwaili H. The effect of nurse-patient language barrier on patients’ satisfaction. Saudi Med J 2010; 31: 1355-1358.
References
- 1.Schyve PM. Language differences as a barrier to quality and safety in health care: the Joint Commission perspective. J Gen Intern Med. 2007;22(Suppl 2):360–361. doi: 10.1007/s11606-007-0365-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wynia MK, Osborn CY. Health literacy and communication quality in health care organizations. J Health Commun. 2010;15(Suppl 2):102–115. doi: 10.1080/10810730.2010.499981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Stewart M. Towards a global definition of patient centred care. BMJ. 2001;322:444–445. doi: 10.1136/bmj.322.7284.444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Almutairi AF, McCarthy A. A multicultural nursing workforce and cultural perspectives in Saudi Arabia: An overview. theHealth. 2012;3:71–74. Available from: http: //www.thehealthj.com/september_2012/a_multicultural_work_force_in_KSA.pdf . [Google Scholar]
- 5.Littlewood J, Yousuf S. Primary health care in Saudi Arabia: applying global aspects of health for all locally. J Adv Nurs. 2000;32:675–681. doi: 10.1046/j.1365-2648.2000.01527.x. [DOI] [PubMed] [Google Scholar]
- 6.Aldossary A, While A, Barriball L. Health care and nursing in Saudi Arabia. Int Nurs Rev. 2008;55:125–128. doi: 10.1111/j.1466-7657.2007.00596.x. [DOI] [PubMed] [Google Scholar]
- 7.Aboul-Enein FH. Personal contemporary observations of nursing care in Saudi Arabia. Int J Nurs Pract. 2002;8:228–230. doi: 10.1046/j.1440-172x.2002.00370.x. [DOI] [PubMed] [Google Scholar]
- 8.Ministry of Health. Health Statistical Year Book. Riyadh (KSA): Ministry of Health; 2008. Available from: http: //ghdx.healthdata.org/record/saudi-arabia-health-statistical-yearbook-2008 . [Google Scholar]
- 9.World Health Organization. Country Cooperation Strategy for WHO and Saudi Arabia 2006-2011. Cairo (Egypt): World Health Organization, Regional Office for the Eastern Mediterranean; 2006. Available from: http: //www.who.int/countryfocus/cooperation_strategy/ccs_sau_en.pdf . [Google Scholar]
- 10.Al-Khathami AM, Kojan SW, Aljumah MA, Alqahtani H, Alrwaili H. The effect of nurse-patient language barrier on patients’ satisfaction. Saudi Med J. 2010;31:1355–1358. [PubMed] [Google Scholar]
- 11.Health Evidence. Quality assessment tool. Review article. [cited 2014 June] Hamilton (ON): McMaster Innovation; 2010. Available from: http: //health-evidence.org . [Google Scholar]
- 12.Russell CK, Gregory DM. Evaluation of qualitative research studies. Evid Based Nurs. 2003;6:36–40. doi: 10.1136/ebn.6.2.36. [DOI] [PubMed] [Google Scholar]
- 13.Sidumo EM, Ehlers VJ, Hattingh SP. Cultural knowledge of non-Muslim nurses working in Saudi Arabian obstetric units. Curationis. 2010;33:48–55. doi: 10.4102/curationis.v33i3.7. [DOI] [PubMed] [Google Scholar]
- 14.Al Fozan H. Patients and Family caregivers’ satisfaction with care delivered by Saudi Nurses at National Guard Health Affairs Hospitals in Saudi Arabia. Journal of Natural Sciences Research. 2013;3:12. [Google Scholar]
- 15.Halligan P. Caring for patients of Islamic denomination: Critical care nurses’ experiences in Saudi Arabia. J Clin Nurs. 2006;15:1565–1573. doi: 10.1111/j.1365-2702.2005.01525.x. [DOI] [PubMed] [Google Scholar]
- 16.Almutairi DO, Moradi E. Factors influencing turnover among Saudi nurses: A literature review. [cited 2014 May] Malaysia: King Abdulaziz Military Academy University of Teknologi Malaysia; Available from: https: //www.academia.edu/795094/Factors_Influencing_Turnover_Among_Saudi_Nurses_A_Literature_Review . [Google Scholar]
- 17.Almutairi AF. A case study examination of the influence of cultural diversity in the multicultural nursing workforce on the quality of care and patient in a Saudi Arabian hospital. [updated 2012 July 12. Accessed 2014 May] Brisbane (Australia): Queensland University of Technology; 2012. Available from: http: //eprints.qut.edu.au/51580 . [Google Scholar]
- 18.Van Bommel M. Expatriate non-Muslim Nurses Experiences of working in a Cardiac Intensive Care unit in Saudi Arabia. [updated 2011 Nov. accessed 2014 May] Pretoria (SA): University of South Africa; 2011. Available from: http: //uir.unisa.ac.za/handle/10500/5033 . [Google Scholar]
- 19.Aljadhey H, Mahmoud MA, Hassali MA, Alrasheedy A, Alahmad A, Saleem F, et al. Challenges to and the future of medication safety in Saudi Arabia: A qualitative study. Saudi Pharm J. 2014;22:326–332. doi: 10.1016/j.jsps.2013.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mahrous MS. Patient perceptions regarding information given on hospital discharge in Almadinah Almunawwarah, Kingdom of Saudi Arabia. Journal of Taibah University Medical Sciences. 2013;8:105–111. [Google Scholar]
- 21.Al-Khashan HI, Almulla NA, Galil SA, Rabbulnabi AA, Mishriky AM. Gender differences in health education needs and preferences of Saudis attending Riyadh Military Hospital in the Kingdom of Saudi Arabia. J Family Community Med. 2012;19:172–177. doi: 10.4103/2230-8229.102317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Wahabi HA, Alziedan RA. Reasons behind non-adherence of healthcare practitioners to pediatric asthma guidelines in an emergency department in Saudi Arabia. BMC Health Services Research. 2012;12:226. doi: 10.1186/1472-6963-12-226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Binsalih SA, Waness AO, Tamim HM, Harakati MS, Al Sayyari AA. Inpatients’ care experience and satisfaction study. J Family Community Med. 2011;18:111–117. doi: 10.4103/2230-8229.90009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mohamed AG. Work-related assaults on nursing staff in Riyadh, Saudi Arabia. J Family Community Med. 2002;9:51–56. [PMC free article] [PubMed] [Google Scholar]
- 25.Ferrante J. Sociology: A global perspective. Belmont (CA): Thomas Higher Education; 2008. Available from: https: //www.studyblue.com/notes/b/sociology-a-global-perspective/4254/0 . [Google Scholar]
- 26.Hollinger-Smith L Diversity and Cultural Competency in Health Care Settings. [cited 2014 June]; Available from: http: //www.matherlifewaysinstituteonaging.com/wp-content/uploads/2012/03/Diversity-and-Cultural-Competency-in-Health-Care-Settings.pdf . [Google Scholar]
- 27.Administration on Aging. Achieving cultural competence: A guidebook for providers of services to older Americans and their families. U.S. Department of Health and Human Services. [cited 2014 June]; Available from: http: //aoa.dhhs.gov/minorityaccess/ [Google Scholar]
- 28.Andrulis D, Delbanco T, Avakian L, Shaw-Taylor Y The Cultural Competence Self-Assessment Protocol for Health Care Organizations and Systems. [cited 2014 May]; Available from: http: //erc.msh.org/mainpage.cfm?file=9.1g.htm&module=provider&language=English . [Google Scholar]
- 29.Georgetown University. Center for Child and Human Development. National Center for Cultural Competence. Available from: http: //gucchd.georgetown.edu/67212.html . [Google Scholar]
- 30.Abu-Zinadah S. Nursing situation in Saudi Arabia. [cited 2014 May] Riyadh (KSA): SCFHS; 2006. Available from: http: //www.nurse.scfhs.org . [Google Scholar]
- 31.Elder NC, Dovey SM. Classification of medical errors and preventable adverse events in primary care: a synthesis of the literature. J Fam Pract. 2002;51:927–929. [PubMed] [Google Scholar]
- 32.Jacobs EA, Shepard DS, Suaya JA, Stone EL. Overcoming language barriers in health care: costs and benefits of interpreter services. Am J Public Health. 2004;94:866–869. doi: 10.2105/ajph.94.5.866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Promoting effective communication--Language access services in health care. Jt Comm Perspect. 2008;28:8–11. [PubMed] [Google Scholar]
- 34.Taylor SP, Nicolle C, Maguire M. Cross-cultural communication barriers in health care. Nurs Stand. 2013;27:35–43. doi: 10.7748/ns2013.04.27.31.35.e7040. [DOI] [PubMed] [Google Scholar]
- 35.Paternotte E, van Dulmen S, van der Lee N, Scherpbier AJ, Scheele F. Factors influencing intercultural doctor-patient communication: A realist review. Patient Educ Couns. 2015;98:420–445. doi: 10.1016/j.pec.2014.11.018. [DOI] [PubMed] [Google Scholar]