

Abstract
Objectives:
To evaluate the efficacy of preemptive intravenous oxycodone on low-dose bupivacaine spinal anesthesia with intrathecal sufentanil in patients undergoing transurethral resection of the prostate (TURP).
Methods:
In this randomized, double-blinded, placebo-controlled trial, 60 patients undergoing TURP were allocated into 2 groups: oxycodone group (group O, n=30) and a normal saline group (group N, n=30). Oxycodone 0.1 mg/kg, or normal saline 0.1 ml/kg was administered intravenously 10 minutes before surgical procedures in group O, or in group N. All patients received sufentanil 5 µg + bupivacaine 0.5% (0.8 ml) + normal saline 0.7 ml - in total, bupivacaine 0.25% (1.6 ml) intrathecally. Spinal block characteristics, hemodynamic values, the perioperative analgesic requirements, visual analogue scale (VAS) scores, Ramsay sedation scale, and side effects were assessed. The study was carried out at the First Hospital of Jilin University, Jilin, China between March and September 2014.
Results:
The time to 2-segment regression of sensory block, full recovery of sensory block, and first analgesic request was longer in group O. Fewer patients required postoperative analgesics, and the VAS pain scores at 4, 8, 16, and 24 hour after operation were significantly lower in group O.
Conclusion:
Preemptive intravenous oxycodone was an efficient and safe method to decrease postoperative pain and reduce tramadol analgesia in patients under low-dose dilute bupivacaine spinal anesthesia combined with intrathecal sufentanil.
Intrathecal anaesthesia is preferred for transurethral resection of the prostate (TURP) for early recognition of transurethral resection syndrome. Low-dose bupivacaine with intrathecal 5 µg sufentanil can yield adequate anaesthesia with minimal hemodynamic instability for TURP.1 Most patients undergoing TURP are elderly and frequently present with cardiac or pulmonary conditions. Therefore, it is important to decrease and delay postoperative pain to reduce stress reactions, and furthermore to prevent the occurrence of severe adverse effects.2,3 Preemptive analgesia has been shown to be effective in control of postoperative pain by protecting the CNS from deleterious effects of noxious stimuli, which can result in allodynia and increased pain. Oxycodone, a type of opioid, was previously reported to have a preemptive analgesic effect on general anesthesia.4 However, there is a scarcity of information on an association with preemptive analgesic efficacy of intravenous oxycodone on spinal anesthesia. In this prospective, randomized, placebo-controlled, double-blinded clinical trial, the hypothesis was tested that preemptive intravenous oxycodone would enhance this method of spinal anesthesia, reduce postoperative pain, and decrease and delay postoperative analgesic requirement.
Methods
This study was approved by the Institutional Ethics Committee and carried out at the First Hospital of Jilin University, Jilin, China. Written informed consent was obtained from 60 patients with American Society of Anesthesiologists (ASA) physical status I to II undergoing elective TURP for benign prostatic hypertrophy between March and September 2014. The patients were double blindly randomized into 2 groups (oxycodone [group O], n=30; normal saline [group N], n=30). Simple randomization was accomplished with a computer-generated sequence of numbers and sealed envelopes were used to divide patients into 2 groups. One of the researchers prepared the study drug before anesthesia. The anesthetic administrator and the patients were unaware of the group allocation. Patients with histories of substance abuse, mental disturbance and neurological disease, who have allergic reactions to the study drugs, with liver or renal dysfunctions, infection at spinal puncture sites, coagulopathy, and ASA III, and above were excluded from the study.
Routine monitorization including electrocardiogram, noninvasive blood pressure (BP) and oxygen saturation (SpO2) was performed for patients taken to the operation room without premedication. A 16 gauge intravenous canula was sited. Before spinal anesthesia, the patients received 5 ml/kg normal saline over 20 minutes (min). The intravenous infusion was minimally maintained during the surgical procedure to avoid the fluid overloading associated with the absorption of irrigating fluid. Patients received bupivacaine 0.8 ml+sufentanil 0.1 ml (5 µg)+normal saline 0.7 ml - in total, bupivacaine 0.25% (1.6 ml) intrathecally. Spinal puncture was performed at L3-4, or L4-5 with a 25 G Quincke needle with the patient in a right-side lying position. The drug solution was given between 10 to 15 seconds (s) with cephalad orientation of the spinal needle bevel, after spinal puncture was successful. Patients were placed in a supine position, and their heads were tilted up 30°. Ten min. after spinal injection, 0.1mg/kg oxycodone (oxycodone hydrochloride injection, 10 mg/ml, HAMOL Limited, Nottingham, UK) diluted with normal saline to obtain a concentration of 1 mg/ml, or normal saline 0.1 ml/kg was injected slowly into the vein for 2 min in group O, or group N. The operation began 10 min later. Data regarding preoperative ultrasound-estimated prostate volume was collected, and mean blood pressure (MBP) and heart rate (HR) were recorded every 5 min until the end of surgery. Hypotension was defined by a decrease in SBP of <90 mm Hg, or <75% from the baseline value, and bradycardia was defined as HR <45 beat/min. In those cases, 4 mg of ephedrine or 0.5 mg of atropine was intravenously injected. When the patients complained of pain, 100 µg fentanyl was intravenously administered. If additional doses were necessary, the patient was excluded from the study, and general anesthesia was induced. The patients were observed in the recovery room, and in the in-patient clinic for the first 24 hours (h). The sensory block level, defined as the dermatomal segment with loss of pain sense to pin-prick test with a 22 G hypodermic needle on each side of the midthoracic line, was checked every 2 min from the drug injection until it reached the peak level, and then every 10 min during the surgery. The peak block level was selected as the same block level that could last for 4 consecutive tests. In cases with a discrepancy in the sensory block level between the 2 sides, the higher block level was chosen. We recorded the peak sensory block level, time to peak block level from intrathecal injection, time to 2-segment regression, the degree of peak motor block, time to peak motor block, use of supplemental analgesics intraoperatively, and time to the first analgesic request after operation. The degree of motor block was assessed with Bromage scale: 1 - complete motor block; 2 - almost complete motor block: able only to move the feet; 3 - partial motor block: able to move the knees; 4 - detectable weakness of hip flexion: able to raise the leg but is unable to keep it raised; 5 - no detectable weakness of hip flexion: can keep the leg raised for 10 s at least; 6 - no weakness at all.
The time to the first analgesic request (tramadol) was recorded. An independent investigator assessed the pain scales using the visual analogue scale (VAS: 0- no pain; 1, 2, 3 - mild pain; 4, 5, 6 - moderate pain; 7, 8, 9 - severe pain; 10 - the worst pain the patient had ever experienced) and the sedation score using Ramsay sedation scale (1 - anxious and agitated; 2 - cooperative and tranquil; 3 - drowsy but responds to command; 4 - asleep but responds to tactile stimulation; and 5 - asleep and no response). The study ended 24 hours after all data had been obtained. The VAS scores and Ramsay scores were recorded at 1, 2, 4, 8, 16, and 24 hours after the end of surgery. The total number of patients who required analgesics in the first 24 hours postoperatively was recorded. Adverse events such as hypotension, bradycardia, respiratory depression, nausea or/and vomiting, and pruritus were observed and recorded during the surgical procedure, and the first 24 h postoperatively. The incidence of adverse effects was evaluated with a “yes” or “no” survey.
Assuming that preemptive oxycodone would prolong time to the first analgesic request by 30 min. Twenty-three patients in each group were needed to detect the difference with a power of 90% at 5% significance level using the Statistical Package for Social Sciences version 17 (SPSS Inc., Chicago, IL, USA). Thirty patients were enrolled per group for possible dropouts. The results were shown as mean ± standard deviation (SD) and number of patients (percentage). Statistical analysis was performed using SPSS 17.0. Independent sample t-test was used to assess most of the demographic data (age, weight, and height), the duration of the operation, preoperative prostate volume, time to reach peak sensory block level, time to reach peak motor block level, time to 2-segment regression of sensory block, time to full recovery of motor block, time to full recovery of the sensory block, VAS scores, time to the first analgesic request, MBP, and HR at the same time point between groups. Changes in MBP and HR at various time points within each group were tested with ANOVA for repeated measures. The peak motor block level and the peak sensory block level were compared using the Mann-Whitney U-test. Categorical variables, such as American Society of Anesthesiologists physical status, the incidence of ephedrine and analgesic use, and adverse effects were analyzed between 2 groups with either chi-square statistics, or Fisher’s exact test. P<0.05 was considered statistically significant.
Results
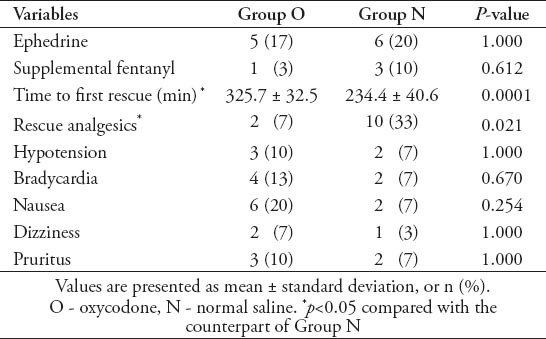
Spinal anesthesia was successfully accomplished in all patients. There were no significant differences between the 2 groups based on demographic characteristics and surgical data (p>0.05) (Table 1). Hemodynamic values at each period are presented in Table 2. Mean blood pressure (MBP) and heart rate (HR) were significantly decreased due to spinal anesthesia in both groups, but there was no difference between the 2 groups. When the 2 groups were compared with respect to peak sensory block level, peak motor block level, time to reach peak sensory block, time to reach peak motor block, and time to reach the Bromage score 6 level, no significant differences were found between group O and group N. The 2-segment regression time and the time to full recovery of sensory block were significantly longer in group O than in group N (p=0.035 and p=0.0001). The motor blockade was observed in all patients in both groups (Table 3). The VAS pain scores at 4, 8, 16, and 24 hours were significantly lower in group O (Table 4). The use of ephedrine was not significantly different between the 2 groups. All patients showed a sedation score <3 at every time point. The perioperative analgesic use and adverse events during the study period (intra- and postoperative period) are shown in Table 5. The number of patients who required postoperative analgesia was significantly different between the groups (p=0.021). There were no significant differences between the 2 groups for supplemental fentanyl use, or any of the adverse events. All the SpO2 and respiration rate data were within the normal range during the study period (93-100% for SpO2, and 12-16 breath/min for respiration rate) in both groups. There were no atropine use, vomit, or respiratory depression perioperatively.
Table 1.
Patient demographics and intraoperative data included in a study in China.
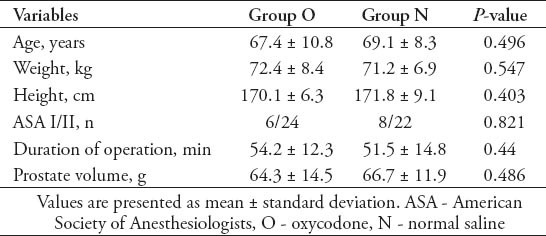
Table 2.
Mean blood pressure and heart rate at various time points of patients included in a study in China.
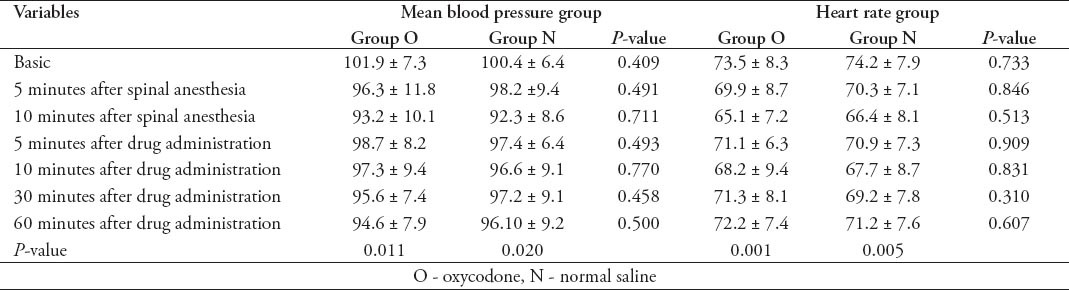
Table 3.
Spinal block characteristics of patients from China.
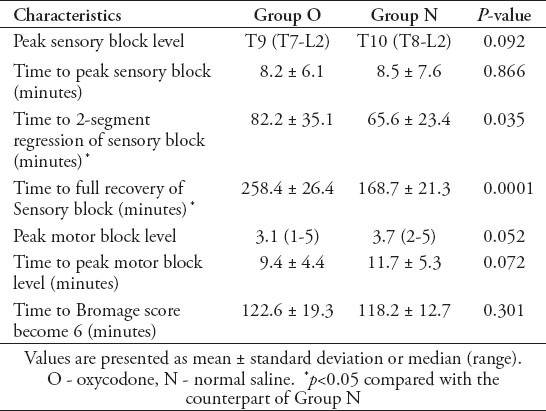
Table 4.
Visual analogue scale scores at different postoperative hours of patients from China.
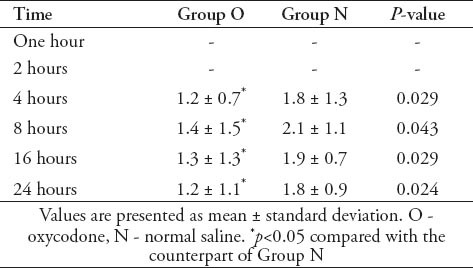
Table 5.
Ephedrine use, perioperative analgesic use and adverse effects on patients from China.
Discussion
Most patients undergoing TURP are elderly and have preexisting cardiopulmonary conditions with relatively high pain threshold, but low pain tolerance.2,3 Therefore, it is important to reduce adverse cardiopulmonary events resulting from high levels of the spinal block in such patients. This study demonstrated that hyperbaric low-dose bupivacaine (7.5 mg) with intrathecal 5 µg sufentanil provided a satisfactory anesthetic condition for TURP with minimal hemodynamic alteration. Spinal anesthesia was successfully accomplished in all patients, and no patient was excluded for inadequate anesthesia in both groups. The results are consistent with a previous published study.1
Sertöz et al5 reported that the effect of postoperative analgesia was brief after intrathecal injection of sufentanil because of its rapid clearance from the cerebrospinal fluid. The preemptive analgesia strategy is an efficient method used for pain management by administering powerful analgesics to patients before the surgical procedure to inhibit central sensitization, which could cause pain feeling expanded and prolonged.6 Preemptive analgesia could not only enhance the effect of spinal anesthesia, but also decrease the postoperative pain.7
Although many drugs have the effect of preemptive analgesia, medications that are likely to prevent the development of central excitability may be of the greatest benefit.8 Oxycodone, a type of opioids, is an interesting option for preemptive analgesia. One hour after oral administration, oxycodone concentration in plasma is 3 times as high as that in cerebrospinal fluid. At the same plasma concentration, oxycodone has a more powerful effect than morphine, which indicates that oxycodone has stronger analgesic effect on the central nervous system, because of its higher concentration in cerebrospinal fluid. However, the mechanism of the analgesic action of oxycodone is still unknown.9,10 The role of preemptive analgesia with oral oxycodone has been reported on general anesthesia.4 So far, the present study is the first clinical trial associated with the effect of preemptive intravenous oxycodone on spinal anesthesia and the postoperative tramadol analgesia in patients undergoing TURP.
In this study, the longer time to 2-segment regression and to full recovery of sensory block in group O might result from the blunt ability of mild pain perception in the central nervous system because of preemptive analgesia. The mild pain was caused by a 22 G hypodermic needle for pin-prick test. Meanwhile, the peak sensory block level was not affected, for which the reason was unknown. The MBP and HR decreased due to spinal anesthesia in both groups, in most cases, still within normal range, and not significantly lower in group O than in group N at each time point. The incidence of adverse effects was low in this study (Table 5). Pruritus has been previously reported as the most common adverse effect of intrathecal sufentanil,11 which was not a problem in our study, but it may not be a problem in elderly patients.1
The limitations of this study are it is small scale and the fact that the types of diseases, and patients were single. Therefore, studies with a larger sample need to be carried out to evaluate the effect of preemptive oxycodone on the quality of spinal analgesia.
In conclusion, the results indicate that preoperative intravenous oxycodone could reduce postoperative pain and postoperative analgesia, without worsening instability in blood circulation, affecting motor block, or increasing any of the adverse effects.
Footnotes
References
- 1.Kim SY, Cho JE, Hong JY, Koo BN, Kim JM, Kil HK. Comparison of intrathecal fentanyl and sufentanil in low-dose dilute bupivacaine spinal anaesthesia for transurethral prostatectomy. Br J Anaesth. 2009;103:750–754. doi: 10.1093/bja/aep263. [DOI] [PubMed] [Google Scholar]
- 2.Imantalab V, Mirmansouri A, Sedighinejad A, Naderi Nabi B, Farzi F, Atamanesh H, et al. Comparing the effects of morphine sulfate and diclofenac suppositories on postoperative pain in coronary artery bypass graft patients. Anesth Pain Med. 2014;4:e19423. doi: 10.5812/aapm.19423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.De Andrés J, Fischer HB, Ivani G, Mogensen T, Narchi P, Singelyn FJ, et al. Postoperative Pain Management - Good Clinical Practice. General recommendations and principles for successful pain management. Available from: http: //polanest.webd.pl/pliki/varia/books/PostoperativePainManagement.pdf . [Google Scholar]
- 4.Fanelli G, Ghisi D, Berti M, Troglio R, Ortu A, Consigli C, et al. Preoperative administration of controlled-release oxycodone as a transition opioid for total intravenous anaesthesia in pain control after laparoscopic cholecystectomy. Surg Endosc. 2008;22:2220–2228. doi: 10.1007/s00464-008-0026-6. [DOI] [PubMed] [Google Scholar]
- 5.Sertöz N, Aysel İ, Uyar M. The effects of sufentanil added to low-dose hyperbaric bupivacaine in unilateral spinal anaesthesia for outpatients undergoing knee arthroscopy. Agri. 2014;26:158–164. doi: 10.5505/agri.2014.51422. [DOI] [PubMed] [Google Scholar]
- 6.Rosero EB, Joshi GP. Preemptive, preventive, multimodal analgesia: what do they really mean? Plast Reconstr Surg. 2014;134(4 Suppl 2):S85–S93. doi: 10.1097/PRS.0000000000000671. [DOI] [PubMed] [Google Scholar]
- 7.Bafna U, Rajarajeshwaran K, Khandelwal M, Verma AP. A comparison of effect of preemptive use of oral gabapentin and pregabalin for acute post-operative pain after surgery under spinal anesthesia. J Anaesthesiol Clin Pharmacol. 2014;30:373–377. doi: 10.4103/0970-9185.137270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Katz J, Clarke H, Seltzer Z. Review article: Preventive analgesia: quo vadimus? Anesth Analg. 2011;113:1242–1253. doi: 10.1213/ANE.0b013e31822c9a59. [DOI] [PubMed] [Google Scholar]
- 9.Mikus G. Urine drug testing for oxycodone and its metabolites as a tool for drug-drug interactions? J Anal Toxicol. 2015;39:81–82. doi: 10.1093/jat/bku111. [DOI] [PubMed] [Google Scholar]
- 10.Hayashi T, Ikehata S, Matsuzaki H, Yasuda K, Makihara T, Futamura A, et al. Influence of serum albumin levels during opioid rotation from morphine or oxycodone to fentanyl for cancer pain. Biol Pharm Bull. 2014;37:1860–1865. doi: 10.1248/bpb.b14-00119. [DOI] [PubMed] [Google Scholar]
- 11.Salarian S, Fathi M, Farzanegan B, Bagheri B. Efficacy and safety of sufentanil and pethidine in spinal anesthesia for painless labor. Drug Res (Stuttg) 2014 Apr 29; doi: 10.1055/s-0034-1372610. Epub. [DOI] [PubMed] [Google Scholar]