

Abstract
Osteoma is a benign osteogenic lesion with a very slow growth, characterized by proliferation of either compact or cancellous bone. Most cases of peripheral osteomas are asymptomatic and produce swelling and asymmetry. Its pathogenesis is unclear but commonly accepted theories propose embryologic, traumatic, or infectious causes. The osteoma may appear in the form of a limited peripheral lesion involving the alveoli or cheek or as a tumoral growth developing inward toward the sinus. Recurrences of osteomas have not been reported in the literature. We report a rare case of maxillary peripheral osteoma with impacted right canine in a 32-year-old female patient.
Keywords: Maxilla, osteoma, peripheral
INTRODUCTION
Osteoma is a slow growing benign lesion which is characterized by proliferation of cancellous or compact bone. It can be classified as solitary or multiple. Multiple osteomas are mainly associated with Gardner's syndrome while solitary osteomas can be further classified as peripheral, central or extra skeletal depending on the origin. Clinically, osteomas are mostly asymptomatic, bony hard tumors which may result in progressive facial asymmetry or malocclusion. I hereby present a case of maxillary compact peripheral osteoma leading to gross facial asymmetry.
CASE REPORT
A 32-year-old female patient reported with the swelling arising from right maxilla. The lesion was initially small in size and has grown slowly to present size. There was no history of trauma and the medical history was non-contributory. Examination revealed a bony hard lesion on the right side of the face in the right maxillary region about 6.3 × 6.3 cm2 [Figure 1]. The overlying skin was stretched and there was no sensory deficit. Intra-oral examination revealed a circumscribed lesion extending from the right maxillary incisors to the right maxillary second molar region. There was normal overlying mucosa and right permanent canine was missing [Figure 2]. All the involved teeth were sent to endodontist for pulp vitality and were found vital.
Figure 1.

Osteoma of unusual size involving right maxilla
Figure 2.

Intraoral extent
Cone-beam computed tomography (CT) showed the lesion involving part of the right maxillary alveolar process, anterior wall of maxillary sinus, infraorbital rim and the right piriform rim measuring 63 × 63 × 65 mm. The right canine is seen in the center of the lesion with a well-defined hypodense tract seen extending 25 mm inferiorly from canine to alveolar process [Figures 3 and 4].
Figure 3.

Cone-beam computed tomography showing size and extent of lesion
Figure 4.
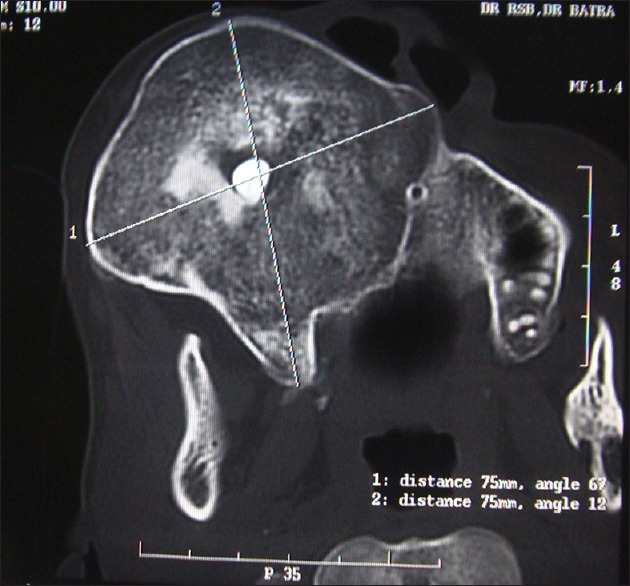
Cone-beam computed tomography showing impacted canine
A differential diagnosis of an ossifying fibroma or osteoma was made and a biopsy confirmed the diagnosis. The histopathology report was that of a cortico cancellous osteoma. As the patient had no obstruction to his breathing, it was decided to surgically remove the protruding part of the lesion, that is in the region of maxilla, alveolar process, piriform rim, infraorbital rim, canine and tract extending from canine to alveolar process was removed.
Intraoperatively, the facially protruding part of the lesion was removed and the involved teeth were spared. Hemostasis was achieved and the surgical site was closed primarily. Postoperative healing was uneventful with no sensory deficit and the involved teeth were not devitalized.
Macroscopically, the lesion consisted of a homogenous bony appearance measuring 5 × 5.5 × 4.5 cm. Microscopically it consisted of dense compact bone with no evidence of inflammation or malignancy and also no features of fibro-osseous proliferation.
DISCUSSION
Osteomas of jaw bone are rare. Some lesions likely to present as true neoplasm of bone, other lesion may be alteration of bone as a response to trauma or infection, although their etiology is unclear. Patients presenting with peripheral osteomas and supernumerary or impacted teeth should be investigated for Gardner's syndrome. The triad of polyposis coli, skeletal abnormalities, such as peripheral and endosteal osteomas, and multiple impacted or supernumerary teeth is consistent with this syndrome.
For osteomas imaging by conventional radiograph can be achieved for diagnostic purpose but CT scan and 3D reconstruction makes it possible to achieve a better resolution and precise localization.[1]
Removal of osteoma is not always necessary. Surgery is indicated only when the lesion is symptomatic, actively growing, or for cosmetic reasons.
Recurrence of osteomas after surgical excision is extremely rare. There are no reports of malignant transformation in the literature.[2]
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Bonder L, Bar-ziv J, Kaffe I. CT of cystic jaw lesions. J Comput Assist Tomogr. 1994;18:22–6. doi: 10.1097/00004728-199401000-00005. [DOI] [PubMed] [Google Scholar]
- 2.Woldenberg Y, Nash M, Bodner L. Peripheral osteoma of the maxillofacial region. Diagnosis and management: A study of 14 cases. Med Oral Patol Oral Cir Bucal. 2005;10(Suppl 2):E139–42. [PubMed] [Google Scholar]