

Abstract
The most commonly reported socially aberrant behavior in postinstitutionalized (PI) children is disinhibited social engagement (DSE; also known as indiscriminate friendliness). There is no gold standard for measurement of this phenomenon or agreement on how to differentiate it from normative behavior. We adopted a developmental psychopathology approach (Cicchetti, 1984) to study this phenomenon by comparing it to normative social development and by studying its patterns over time in 50 newly adopted PI children (16–36 months at adoption) compared with 41 children adopted early from foster care overseas and 47 nonadopted (NA) controls. Using coded behavioral observations of the child’s interaction with an unfamiliar adult, atypical behaviors were differentiated from normative behaviors. Principal components analysis identified two dimensions of social disinhibition. The nonphysical social dimension (e.g., initiations, proximity) showed wide variation in NA children and is therefore considered a typical form of sociability. Displays of physical contact and intimacy were rare in NA children, suggesting that they represent an atypical pattern of behavior. Both adopted groups demonstrated more physical DSE behavior than NA children. There were no group differences on the nonphysical factor, and it increased over time in all groups. Implications for understanding the etiology of DSE and future directions are discussed.
Globally, there are currently between two and eight million orphaned children who spend a significant portion of their early lives in institutions (Williamson & Greenberg, 2010; Save the Children, 2009). These children often face multiple forms of early adversity including malnourishment, physical abuse, sexual abuse and neglect (Gunnar, Bruce, & Grotevant, 2000). Even in the most advanced “model” institutions who provide adequate nutrition, medical care, and stimulation, the lack of consistent caregivers has significant effects on children’s development (Tizard & Hodges, 1978). Beginning in the 1990s, Western families began to adopt increasing numbers of children from institutions overseas in a natural experiment of the potential for families to reverse the negative impacts of early institutional care (Gunnar et al., 2000).
While most post-institutionalized (PI) children function well, as a group they are at risk for socioemotional deficits, cognitive delays, behavior problems, and psychopathology (e.g., Gunnar & van Dulmen, 2007). The most persistent and often profound effects are seen in children’s socioemotional development. Parents rate children’s interpersonal functioning as the area with least progress after adoption (Fisher, Ames, Chisholm, & Savoie, 1997). One of these persistent socioemotional deficits is a general lack of developmentally appropriate reticence around strangers, or what can termed Disinhibited Social Engagement (DSE). Associated characteristics include indiscriminate sociability, failure to check back with a caregiver in a novel situation, willingness to go away with a stranger, and failure to abide by social norms such as personal space. Once the child is verbal, age-inappropriate intrusive, personal questions are also observed, suggesting struggles with conforming to social boundaries. Children also exhibit inappropriate physical intimacy with strangers (hugs upon meeting them, sitting on their lap, etc.). While all of these behaviors have been associated with DSE, they vary in the degree to which they violate social norms, and it is unclear whether they are all specific to children exposed to early deprivation and/or indicative of a problem. The present study aims to clarify the core components of this phenomenon and distinguish them from temperamental sociability using an observational measure. This is the first study to examine DSE behavior proximally to adoption, as well as changes that may occur in the first few months, with the goal of gaining more traction in our understanding. By studying change over time, we can examine which behaviors subside and which persist, and this can further inform clinical and diagnostic efforts.
The etiology for this cluster of behaviors remains under debate. For the remainder of this section, we discuss the hypotheses most often considered to explain the causes of DSE: 1) as a symptom of attachment difficulties with primary caregivers; 2) as an adaptive response to early social neglect; 3) as a consequence of cognitive deficits/delays which impact children’s ability to inhibit their behavior and to understand social boundaries. Lastly, we discuss our novel approach to this problem, namely to deconstruct this set of disinhibited social behaviors and isolate the components that are elevated only in children who experienced early deprivation, teasing them apart from typically-occurring differences in temperamental sociability. We believe that a developmental psychopathology approach -comparing typical and atypical behavior to explain abnormal processes- will be fruitful both for understanding etiology and for clinical diagnosis.
Do DSE Behaviors Relate to Attachment Difficulties?
Previous work has often labeled this constellation of behaviors as indiscriminate friendliness; however, the behavior is neither completely indiscriminate, nor truly friendly. Instead, it is superficial and impersonal; even when children show a strong initial approach to strangers, they do show preference for known caregivers (e.g. O’Connor, Bredenkamp, Rutter, & The ERA Study Team, 1999). Other researchers have referred to this behavior as disinhibited attachment behavior (or a symptom of Reactive Attachment Disorder) or diffuse attachments; however recent research suggests that the behavior may not signal attachment problems as previously thought (Zeanah & Gleason, 2010). For example, some PI children with secure attachments to their adoptive parents continue to show DSE (Chisholm, 1998; O’Connor, Marvin, Rutter, Olrick, & Britner, 2003). Children still living in an institution showed equally high levels of these behaviors despite differences in attachment relationships (Zeanah, Smyke, & Dumitrescu, 2002). In addition, despite improvements in attachment over time, DSE remains evident in PI children for years (Chisholm, 1998; Smyke, Zeanah, Fox, Nelson, & Guthrie, 2010). Consequently, in DSM-V the Disinhibited subtype of Reactive Attachment Disorder will be separated and renamed “Disinhibited Social Engagement Disorder” (American Psychiatric Association, 2013). For consistency, we chose to use the same term: Disinhibited Social Engagement (DSE).
DSE Behaviors as an Adaptive Response to Social Neglect Early in Life
Chisholm (1998) suggested that while children are in institutional care, being overly sociable helps to attract attention and affectionate contact from staff members who have a large number of children to attend to; thus, it may be viewed as adaptive. However, the behavior is hard to extinguish after adoption, very persistent over time in some children, and also maladaptive in the child’s new social environment, thus researchers and clinicians have recognized that this is more than a transient adaptive response. In an attempt to build causal inferences linking social deprivation early in life to DSE, researchers turned to parameters of early deprivation to see if they reliably predict the behavior. In general, DSE is not associated with degree of deprivation (indexed by nutritional deprivation or parent reported deprivation; O’Connor et al., 2003; Chisholm, 1998; Bruce, Tarullo, & Gunnar, 2009). The association between length of institutionalization and DSE has been quite mixed. For example, some studies find a dose-response relationship, with children exposed to longer institutionalization exhibiting more signs of DSE (e.g. O’Connor & Rutter, 2000), while others find no relationship between DSE and duration of deprivation (e.g. Gleason et al., 2011). In addition, even some children who have been institutionalized for long periods show no evidence of these behaviors (O’Connor & Rutter, 2000). High-quality care (including proper nutrition and stimulation) may not prevent the behavior, as Tizard and colleagues (Tizard & Hodges, 1978; Tizard & Rees, 1975) described this behavior even in children adopted out of very high quality institutional settings, who had intact functioning in nearly every other aspect of development. Similarly, Zeanah and colleagues (Zeanah, Smyke, Koga, & Carlson, 2005) explored the correlates of DSE in children living in an institution and found no correlations with observations of care quality. Of course, this might merely mean that even the best quality of institutional care does not adequately meet the social needs of developing infants and young children. Consistent with this argument, DSE is also seen among children in foster care (Oosterman & Schuengel, 2007; Zeanah, Scheeringa, Boris, Heller, Smyke, & Trapani, 2004; Pears Bruce, Fisher, & Kim, 2010), and one study found that it was predicted by the number of different foster homes the child had been in rather than the severity of abuse or physical neglect they had experienced (Pears et al., 2010). Thus it is important to compare children adopted from institutions to adopted children who have experienced family-type care arrangements prior to adoption given their commonalities in experiences as well as their differences due to institution effects. There is also growing evidence that the maintenance of the behavior may be related to some of the persistent self-regulatory deficits that are also associated with early deprivation, particularly attention regulation and inhibitory control (Bruce, et al., 2009; O’Connor, et al., 1999; Pears, et al., 2010; Roy, Rutter & Pickles, 2004). We review some of this evidence next.
DSE Behaviors as a Consequence of Cognitive Deficits/Delays
This kind of disinhibited social behavior is sometimes seen among children with severe cognitive deficits/delays, but findings are mixed in terms of the association with cognitive abilities among PI children. A recent study by Smyke and colleagues (2012) found that this behavior was associated with cognitive ability, with children with lower developmental quotients (DQs) demonstrating more DSE behaviors. However, past studies have not found this association, and have noted this behavior even among children with normal or even high IQs (see review, Gunnar, 2001; Bruce et al., 2009; Lyons-Ruth, Bureau, Riley, & Atlas-Corbett, 2009).
Some studies have focused on specific cognitive skills such as inhibitory control, given its relevance to these concerning behaviors. Indeed, children who had more difficulty stopping themselves from pressing the button on the noGo trials of a Go-noGo task (Bruce et al., 2009) or those who had more difficulty on the Day-Night Stroop task (Pears et al., 2010) also exhibited more DSE. It is possible that general problems with inhibitory control underlie these behaviors. Interestingly, there is some evidence that turnover in caregivers also influences inhibitory control and it is the impact on inhibitory control that influences preschool-aged children’s ability to appropriately regulate social engagement (Pears et al., 2010). Thus, inhibitory control deficits may be one of the mediators for the effect of high caregiver turnover on later social behavior.
Distinguishing Abnormal from Normal DSE Behaviors Soon after Adoption
In light of the mixed evidence in the prior literature and the difficulties inferring the etiology of DSE, we sought to deconstruct these behaviors into normal and abnormal components soon after adoption. We adopted a developmental psychopathology approach (Cicchetti, 1984) to study this phenomenon by comparing it to normative social development and by analyzing its patterns of change over time soon after adoption. Stranger reticence is a normative developmental milestone that appears between 6-12 months of age (Sroufe, 1977). However, some children exhibit little reticence and, indeed, are quite outgoing. Even in studies of PI children, there are some non-PI comparison children who show substantial sociability with strangers. (Chisholm, Carter, Ames, & Morison, 1995; O’Connor et al., 1999; O’Connor & Rutter, 2000). This has also been noted in observational studies of DSE in PI and comparison children (Bruce et al., 2009; O’Connor et al., 2003). It is not clear, however, whether PI and comparison children differ only in quantity of these behaviors or whether there is also a difference in their quality. If there are qualitative differences, this might help isolate those PI children who are a the greatest risk of persisting in these behaviors and of developing other social deficits (Chisholm, 1998; Kreppner et al., 2010; The English and Romanian Adoptees (ERA) Study Team, 2010).
The Measurement of DSE
Despite the extensive research on DSE in PI children, there is no single “gold standard” to measuring and coding DSE behavior, but several methods have proved informative. Many of the classic studies (e.g. Tizard & Rees, 1975), as well as more recent work (e.g. Chisholm, 1998; O’Conner et al., 1999; 2003; Smyke et al., 2012) have used parent interviews, which collect information about everyday situations across a variety of settings, are relatively inexpensive and time-efficient. However, parent interviews may also risk introducing reporter bias, especially when comparing DSE with other parent-reported concerns, such as behavior problems. Lastly, the currently available interviews are designed to be used after a good deal of time in the caregiving situation, with no way of measuring DSE or tracking its course soon after adoption.
Behavioral observations have also been used in a number of studies (e.g. Lyons-Ruth et al., 2009; Gleason et al., 2011; Bruce et al., 2009; O’Connor et al., 2003), and are modestly associated with parent report measures (O’Connor et al., 2003; Gleason et al., 2011). Observational measures allow direct comparison of children’s behavior in a controlled environment, absent of parental bias. This type of measurement is also available for use at any time point, including immediately after a care transition. However, behavioral observations are time-consuming and relatively expensive. One observation protocol called the Stranger at the Door (Gleason et al., 2011) was designed to assess whether a child was willing to go off with a stranger (the experimenter). While informative, such an extensive procedure is not always feasible and it only yielded a dichotomous variable (left with stranger or not).
In terms of laboratory assessments, several studies have coded DSE during a modified Strange Situation Procedure (O’Connor et al., 2003; Lyons-Ruth et al., 2009) or other structured stranger interactions (Bruce et al., 2009). There is little consensus on how to code DSE behaviors in such observations. Some of the behaviors used to measure DSE (e.g. Bruce et al., 2009) are also used to assess individual differences in temperamental social inhibition and disinhibition, which may be why in some studies non-adopted, low-risk children display some evidence of DSE (e.g. Chisholm, 1998; O’Connor & Rutter, 2000). Differentiating atypical responses to strangers from behaviors that may overlap with normative variation in friendliness and studying the developmental course of these behaviors would be an important next step for research in this area.
The Clinical Importance of Understanding DSE
This type of behavior is not just an oddity, but it is related to functional impairments in children. Thus, DSE is associated with a higher rate of receiving both mental health and special education services when compared to non-institutionalized controls (Rutter et al., 2007). These behaviors have also been associated with later aggressive and hyperactive behavior problems (Lyons-Ruth et al., 2009). DSE could also be dangerous for the children (for example, going away with a stranger). In fact, when PI children were invited out with a stranger as part of an assessment, one out of every six left with the stranger. These behaviors could also prove deleterious to the caregiver-child relationship if parents feel their adopted or fostered child is not attached to them. As children develop, these behaviors may lead to difficulties in the children’s peer relationships as well (Hodges & Tizard, 1989). Given these deleterious socioemotional and clinical outcomes, the present study sought to shed further light on the phenomenon.
Aims of the Present Study
Given the complexity and importance of accurately measuring disinhibited social engagement, the first aim of the present analysis was to a) describe the frequencies and mean levels of intensity for behaviors towards strangers that we might identify as being rarely exhibited by non-adopted (NA) children and b) differentiate these behaviors from those that are more common and show wide variation in typically developing children. We expected that behaviors that most strongly violate social norms would be rare in NA children. The second aim was to compare adopted children to NA children on these behaviors, expecting that the groups might not differ on typical sociable behaviors, but only on those that are atypical or violate social norms. The third aim was to determine whether the atypical behaviors were unique to the post-institutionalized (PI) children, or would also occur in children adopted from foster care overseas. Given prior evidence that severity of deprivation is not predictive of DSE and that children in foster care also exhibit DSE behaviors, we anticipated some DSE behaviors in both adopted groups. The fourth aim was to examine changes in DSE behaviors over time to test whether trajectories of typical and atypical social behaviors would differ, as another tool for differentiating them. Finally, the last aim was to investigate correlates of DSE behavior that may help explain the emergence of this behavior. Based on prior literature, we chose to focus on associations with: a) measures of pre-adoptive experiences; b) IQ; and c) temperamental shyness, to test whether high levels of DSE behaviors may overlap greatly with this dimension and simply be an exacerbation of naturally-occurring individual differences in sociability.
Methods
Participants
The participants in this study were 50 PI children, 47 non-adopted (NA) children, and 41 early-adopted/foster care (EA/FC) children. PI and EA/FC children were recruited from the Minnesota International Adoption Clinic, located at the University of Minnesota Hospital, and the Minnesota International Adoption Project Registry, which draws from multiple adoption agencies throughout Minnesota. The International Adoption Clinic provides services such as the initial medical visit after adoption, which is recommended for all families to establish the child’s baseline physical health. All internationally adopted children who fit the inclusion criteria of the study, who were recently adopted into Minnesota during the course of the data collection, and were interested in participating in this research were recruited for participation. NA children were recruited from a departmental list of community families willing to participate in research.
The children in this study were part of a larger study examining physiological, behavioral, emotional and cognitive recovery of children adopted from institutional care. PI children (28 female, 22 male) were adopted between 16-36 months of age (M = 24.2 months, SD = 4.9 months) and had spent between 4-34 months in an institution (M = 17.7 months, SD = 7.5 months; 14-100% of pre-adoption life, median= 94%). PI children were adopted from diverse countries of origin (13 countries), distributed across the following regions: 30% South East Asia, 28% Africa, 30% Russia, Eastern Europe or India, and 12% Latin America. The race of PI children as reported by parents was: 6% Latin American Indian, 36% Asian, 30% African/Black, 20% Caucasian, 4% mixed race, 4% other or unknown. Mean age of PI children was 25.9 months, (SD = 4.9 months) at Session 1, and 32.5 months (SD = 5.1 months) at Session 2. Median income of the adoptive parents of PI children was $100,000-$125,000, with more than 90% of parents graduating from college.
EA/FC children (17 female, 24 male) were adopted between 6 and 12 months of age (M = 9.5, SD = 1.3), as is typical for children from countries that use foster care for wards of the state, and had spent less than 4 months in an institution (32% had no institutional care history, 73% of those that did had less than one month). EA/FC children were adopted from South Korea (n = 31) or Guatemala (n = 10). The race of EA/FC children as reported by parents was: 19% Latin American Indian, 76% Asian, 5% other or unknown. Mean age of EA/FC children was 32.4 months, (SD = 4.9) at Session 1, and 39.8 months (SD = 4.9) at Session 2. Median income of the adoptive parents of EA/FC children was $100,000-$125,000, with approximately 80% of parents earning a bachelors degree or higher. Examination of this group of children allowed assessment of factors common to children who are abandoned, orphaned or removed from their homes and placed for adoption, without the experience of prolonged institutional care.
NA children (24 female, 23 male) were born and raised in their biological families in the Midwestern United States. All NA children were reported by parents to be Caucasian. Mean age of NA children was 27.4 months (SD = 5.6) at Session 1, and 34.4 months (SD = 5.8) at Session 2. Median income of the parents of NA children was $75,000 - $100,000, with more than 85% of parents graduating from college.
NA and EA/FC children were age and sex matched to PI children as closely as possible. Mothers almost always (> 90% of the time) participated in the session with their child, and in every instance, the same primary parent participated in both sessions.
Exclusion criteria
Two layers of exclusion criteria were used for participation in this study. Participants were not recruited if they fell outside of the selected range for age at adoption/length of institutional care criteria or had any congenital or neurological disorders (including seizure disorders, endocrine disorders, heart defects). Additionally, participants who were recruited but excluded from the present analysis in order to focus on the effect of early life deprivation and to rule out prenatal insults (e.g., alcohol exposure) were as follows: PI participants with Fetal Alcohol Syndrome (FAS) or FAS concern (n = 6) and extremely low IQ (n = 1). Two NA participants were excluded from this analysis due to an Autism diagnosis (n = 1) or suspected child abuse (n = 1) in order to recruit a typically-developing comparison group.
Procedure
Each laboratory session consisted of several different tasks for the parent and child and lasted approximately 1.5 hours. Session 1 took place one to three months post adoption (M = 1.6, SD = 0.8) for PI children, and at the age-matched time for EA/FC and NA children. [Note that the EA/FC children were slightly but significantly older than the other two groups, F(2,135)= 19.4, p < .001, but as reported later, age was not a correlate of DSE behavior.] Session 2 took place 8-11 months post adoption (M = 8.3, SD = 0.6).
An observational method for evaluating DSE behaviors was derived from Tizard and Rees (1975), to evaluate children’s tendency to initiate interaction with an unfamiliar adult. At the beginning of each session a scripted stranger interaction (10 minutes total) was conducted. The parent and child were led into the testing room, where the child was given a picture book and told that the parent must complete some paperwork. The parent was present throughout the interaction but was discouraged from interacting with the child and especially from influencing the child’s social behavior toward the stranger. The experimenter (an unfamiliar female adult) then entered the room and greeted the parent, then walked directly to her chair and sat down quietly with a clipboard. Thirty seconds later, the experimenter introduced herself to the child, but then returned her attention to her clipboard. During this time the experimenter responded briefly to the child if the child spoke to her, but did not initiate any communication. After another minute passed, the experimenter offered the child some toys to play with, laid the toys in the middle of the room, and sat down on the floor near her chair. Again the experimenter responded briefly to any initiations by the child, but did not continue to interact. Four minutes into this block, the experimenter then asked the child if he or she would like to play together with the experimenter, brought out additional toys, and attempted to engage the child in interactive play. The experimenter and the child played for four minutes. This interaction was videotaped and later coded for interactions with the experimenter.
Following the stranger interaction there was a modified Strange Situation (separation-reunion) procedure, followed by two 10-minute free and structured play interactions with the parent and child, and four two-minute Laboratory Temperament Assessment Battery (Lab-TAB) vignettes.
Measures
Disinhibited Social Approach
The 10-minute stranger interaction was coded for social behaviors by reliable coders. Using the digital ProCoder program (Tapp, 2003), coders recorded initiations by the child (both verbal and nonverbal) as well as proximity and physical contact to the experimenter. Initiations were defined as any vocalization not directed toward the parent, and any gestures or other preverbal communicative behavior (e.g. wave, pointing to an object) toward the experimenter. Initiations were measured as frequencies and only tallied during the phase prior to the experimenter interacting with the child, so as to capture attempts by the child to engage the stranger, rather than ongoing interaction during play. Proximity was considered within two feet of the experimenter, and was coded throughout. The room was arranged so that the child’s starting position was not proximal to either the parent or the experimenter. The toys were arranged in such a fashion so that the child could play with the toys without necessarily coming into proximity with the experimenter. In addition, even when the experimenter began engaging with the child in the final phase of the interaction, she never positioned herself within two feet of the child, so any proximity was the result of the child entering the experimenter’s space and not vice versa. Proximity was measured as duration (i.e. length of time spent within two feet of the experimenter). Physical contact referred to direct contact between the child and the experimenter (initiated by the child), and was measured in frequencies, duration, and overall degree (see below). Physical contact was also coded during the entire task, as it was always child initiated and represented a violation of social norms throughout the interaction.
Latency variables were also calculated indicating latency to first initiation, first approach, and first touch. Coders also made several broad ratings, capturing the child’s initial reaction to the experimenter’s greeting, to the toy offering, and to the play invitation, as well as overall verbal and physical intimacy. Details of these qualitative codes are found in Appendix A. Coders were blind to group status. Two coders reviewed 20% of the tapes to calculate inter-rater reliability, which produced average kappa’s .71-.98.
Experimenters also rated each child following the 1.5-hour session for verbal and physical intimacy over the entire length of the session using the same coding scale (see Appendix A).
Correlates and Potential Covariates
Length of institutionalization and number of transitions prior to adoption were based on parent report. IQ for PI children was assessed using the Mullen Scales of Early Learning (Mullen, 1995) at 12-months post-adoption. Temperament characteristics were assessed at Session 1 and 2 using Early Childhood Behavior Questionnaire (ECBQ; Putnam, Gartstein, & Rothbart, 2006). The ECBQ is a parent report questionnaire designed to assess temperament in children between the ages of 18 and 36 months, and evaluates temperament along 18 separate dimensions. The “Shyness” scale was selected a priori to represent a social inhibition (and reversed, disinhibition) dimension.
Data Analysis Plan
Data Processing
Observational data from the 10-minute stranger interaction was recorded in ProCoder and was reduced using the MOOSES™ program (Tapp, 2003) to yield discrete variables of the child’s interaction with the unfamiliar adult: frequency of initiations, duration of proximity to experimenter, duration of physical contract, frequency of physical contact, and latency to initiation, approach, and touch. All variables were square root transformed to normalize the distributions, and 99.7% Winsorized to prevent outliers from skewing the results (values higher than 3 standard deviations from the mean were replaced with the value at the 99.7 percentile) The variables were then grand mean centered to allow for comparison of standardized scores over time.
Missing data
There were very few missing data (no more than 5.1% for any variable) and data was Missing Completely at Random (MCAR) in the entire sample according to Little’s MCAR test (χ2(5) = 8.4, p = .14) and also according to the MCAR test within the adopted samples when including variables capturing adoption parameters such as duration of institutionalization (p = .21 for PI, p =.94 for EA/FCs). Given these conditions, missing data were not imputed since estimates would likely not be significantly different.
Statistical Analyses
For the first aim, descriptive statistics were used to present the frequencies and mean levels of specific physical or non-physical social engagement behaviors by adoption status. Then, Principal Components Analysis was used to examine the underlying factor structure of DSE variables and reduce the data. Given insufficient a priori knowledge regarding the factor structure and the specific behaviors loading on each factor, confirmatory factor analysis is not recommended (Brannick, 1995; Gorsuch, 1983; Mulaik, 2010) thus PCA was chosen. For Aims 2 and 3, repeated-measures GLMs were conducted to test the effects of group as a between-subjects factor, time of assessment (1 vs. 2) and DSE type (physical vs. non-physical engagement) as within-subjects factors, with group being coded as having three levels (PI, EA/FC, NA). Correlations were then used to test within-subjects stability in behaviors from Time 1 to Time 2. For the last aim, correlations were computed to investigate associations between DSE and early pre-adoptive experiences, as well as temperament.
Results
Distinguishing Atypical from Typical Behavior
Descriptive statistics for the behaviors of interest are presented by group and session in Table 1.
Table 1.
Descriptive statistics and percentage frequencies for key variables.
| PI n = 50 |
NA n = 47 |
EA/FC n = 41 |
||||
|---|---|---|---|---|---|---|
| Session | Session | Session | ||||
| 1 | 2 | 1 | 2 | 1 | 2 | |
| Frequency of initiations | 5.9 (12.5) | 7.9 (12.4) | 4.9 (7.2) | 4.1 (6.3) | 6.7 (9.8) | 8.4 (9.9) |
| Duration of Proximity in seconds | 174.5 (123.1) | 165.7 (131.6) | 142.1 (115.4) | 176.0 (124.3) | 157.3 (119.0) | 131.9 (118.8) |
| Frequency of touches | 1.1 (1.6) | 0.4 (0.82) | 0.3 (0.8) | 0.3 (1.0) | 0.8 (1.1) | 0.3 (0.6) |
| Duration of Physical contact in seconds | 9.1 (25.4) | 2.5 (6.7) | 0.6 (2.1) | 3.7 (15.7) | 7.8 (27.2) | 1.6 (7.7) |
| Latency to first initiation in seconds | 286.3 (247.2) | 238.9 (241.2) | 254.5 (231.9) | 224.9 (205.8) | 238.1 (233.6) | 180.2 (210.3) |
| Latency to first approach in seconds | 286.7 (203.9) | 252.8 (223.0) | 364.7 (197.7) | 302.1 (193.3) | 316.6 (214.2) | 315.8 (202.5) |
| Latency to first touch in seconds | 503.2 (267.1) | 526.4 (157.0) | 579.2 (49.2) | 572.3 (73.5) | 491.6 (152.7) | 572.0 (65.6) |
|
| ||||||
| Reaction to Experimenter’s Greeting | 0.8 (0.7) | 1.1 (1.0) | 0.8 (0.8) | 1.0 (0.9) | 0.9 (1.0) | 1.2 (1.0) |
| 0: Ignores Completely | 40% | 34% | 47% | 32% | 44% | 34% |
| 1: Orients to Experimenter | 46% | 28% | 30% | 34% | 37% | 29% |
| 2: Brief response | 12% | 26% | 23% | 30% | 7% | 27% |
| 3: Lengthy response | 2% | 12% | 0% | 4% | 12% | 10% |
| Reaction to Toy offering | 2.7 (2.0) | 3.5 (1.8) | 2.6 (1.8) | 3.1 (2.0) | 2.4 (2.2) | 3.2 (2.0) |
| 0: Ignores or Declines | 26% | 14% | 19% | 23% | 34% | 20% |
| 1: Shuts out | 8% | 6% | 13% | 4% | 10% | 7% |
| Experimenter but plays with toy | 0% | 2% | 17% | 2% | 10% | 2% |
| 2: Initially ignores but eventually plays | 24% | 14% | 9% | 6% | 5% | 12% |
| 3: Plays but approaches cautiously | 24% | 34% | 23% | 43% | 17% | 22% |
| 4: Accepts and plays immediately | 14% | 20% | 20% | 17% | 15% | 34% |
| 5: Engages Experimenter | 4% | 10% | 0% | 4% | 10% | 2% |
| 6: Needs Experimenter | ||||||
| Reaction to Play Invitation | 2.0 (1.0) | 2.5 (0.9) | 2.1 (1.2) | 2.5 (1.0) | 2.4 (1.2) | 2.6 (1.0) |
| 0: Ignores or Declines | 12% | 4% | 13% | 9% | 10% | 5% |
| 1: Accepts with encouragement | 14% | 8% | 15% | 4% | 12% | 10% |
| 2: Accepts, more interest in toys | 38% | 24% | 23% | 26% | 24% | 20% |
| 3: Accepts, equal interest in toys and Experimenter | 34% | 58% | 42% | 53% | 39% | 54% |
| 4: Accepts, more interest in Experimenter | 2% | 6% | 6% | 9% | 14% | 12% |
| Physical Intimacy (stranger interaction) | 0.7 (1.0) | 0.4 (0.8) | 0.3 (0.6) | 0.3 (0.7) | 0.7 (0.9) | 0.2 (0.5) |
| 0: None | 58% | 70% | 81% | 81% | 56% | 83% |
| 1: Contact as tool | 24% | 18% | 13% | 11 % | 27% | 12% |
| 2: Low level | 10% | 10% | 4% | 6% | 12% | 5% |
| 3: familiar level | 8% | 2% | 2% | 2% | 5% | 0% |
| Verbal Intimacy (stranger interaction) | 1.4 (0.8) | 1.7 (0.6) | 1.6 (0.8) | 1.9 (0.5) | 1.8 (0.5) | 1.9 (0.4) |
| 0: None | 18% | 6 % | 15% | 4% | 0% | 0% |
| 1: responses only | 20% | 18% | 17% | 6% | 27% | 20% |
| 2: basic initiations | 62% | 76% | 64% | 85% | 71% | 78% |
| 3: Shared personal information | 0% | 0% | 4% | 4% | 2 % | 3% |
| Physical Intimacy (whole session, Experimenter rated) | 1.4 (1.0) | 1.5 (1.3) | 0.5 (0.6) | 0.6 (1.0) | 1.1 (1.1) | 1.1 (1.1) |
| 0: None | 22% | 28% | 60% | 66% | 39% | 37% |
| 1: Contact as tool | 26% | 24% | 34% | 17% | 29% | 27% |
| 2: Low level | 40% | 28% | 6% | 11% | 20% | 29% |
| 3: familiar level | 10% | 14% | 0% | 4% | 10% | 2% |
| 4: intimate level | 2% | 4% | 0% | 2% | 2% | 5% |
| 5: Invaded privacy | 0% | 2% | 0% | 0% | 0% | 0% |
| Verbal intimacy (whole session, Experimenter rated) | 1.7 (0.5) | 2.0 (0.5) | 1.9 (0.6) | 2.1 (0.6) | 1.9 (0.6) | 2.2 (0.6) |
| 0: None | 2% | 0% | 0% | 0% | 0% | 0% |
| 1: responses only | 20% | 14% | 21% | 17% | 24% | 10% |
| 2: basic initiations | 78% | 78% | 64% | 62% | 66% | 63% |
| 3: Shared personal information | 0% | 8% | 15% | 21% | 7% | 24% |
| 4: shared intimate information/asked personal questions | 0% | 0% | 0% | 0% | 2% | 2% |
Note. PI = Post-institutionalized, EA/FC = Early adopted from foster care, NA = Non-adopted. M (SD)
A principal components analysis (PCA) was then used to explore the existence of an underlying factor structure for the variables measuring DSE, including behavioral codes and experimenter ratings summarized in Table 1. A PCA with a varimax rotation was used to reduce the grand mean centered, square root transformed, Winsorized variables. The analysis was first conducted for Session 1. The PCA solution returned three factors with eigenvalues larger than 1; however, the third factor only had an eigenvalue of 1.08 and was only defined by the two experimenter ratings, likely capturing only measurement error. We repeated the analysis requesting up to two factors and obtained a two-factor solution. The first factor was defined by the following items: duration of proximity, frequency of initiations, latency to approach and initiation, coder and experimenter ratings of verbal intimacy, and response to the toy and play invitation (see Table 2). The most highly loading variable was responses to the experimenter’s toy and play invitations (.83), which was a normative behavior in this play context. This factor seemed to be a general sociability dimension. In contrast, the second factor was defined most strongly by physical contact items: duration of touch, frequency of touch, coder and experimenter ratings of physical intimacy, latency to touch, and duration of proximity. The most highly loading variable was coder ratings of physical intimacy (.94). This seemed to be a physical engagement dimension.
Table 2.
Principal Components Results: Rotated Component Matrix
| Session 1 Components | Session 2 Components | |||
|---|---|---|---|---|
|
| ||||
| Physical | Non-physical | Physical | Non-Physical | |
| Frequency Touch Experimenter | .86 | .16 | .97 | .07 |
| Physical Intimacy (stranger interaction) | .94 | .19 | .93 | .06 |
| Duration Touching Experimenter | .86 | .14 | .88 | .07 |
| Latency to Touch Experimenter | .85 | .17 | .88 | .13 |
| Physical Intimacy (Exp. rated1) | .40 | .33 | .34 | .25 |
| Latency to initiation | .20 | .77 | .06 | .80 |
| Frequency of initiation | .26 | .71 | .05 | .78 |
| Response to Experimenter | .19 | .83 | .16 | .77 |
| Verbal Intimacy (stranger interaction) | .17 | .75 | .14 | .72 |
| Latency to Proximity | .35 | .70 | .32 | .70 |
| Duration of Proximity | .32 | .69 | .25 | .60 |
| Verbal Intimacy (Exp. rated1) | -.18 | .57 | -.13 | .43 |
rated over the entire two-hour session
We then examined whether the same factor structure emerged at Session 2. Indeed, precisely the same variables defined the non-physical social engagement factor and the physical engagement factor (see Table 2). In order to create unbiased composites of non-physical and physical engagement that could be calculated in the same way at both sessions by equally weighing each variable, we constructed two scales using the variables loading most highly on each component. Both the non-physical and physical engagement scales had high internal consistency at Session 1 (alphas of .86 and .89, respectively) and at Session 2 (.82 and .87) thus we proceeded to create separate non-physical and physical social engagement composites for each session by averaging the variables identified by the PCA as loading most highly on each dimension.
Group Differences and Change over Time
There were no significant gender differences on either composite, so gender was not considered in subsequent analyses. A repeated-measures GLM was conducted to test the effects of group as a between-subjects factor and session (1 versus 2) and DSE type (non-physical vs. physical engagement) as within-subjects factors. There were no significant main effects of session or type on DSE behavior, but there was a significant effect of group, F(2,135) = 3.90, p =.02, partial η2 = .06, and a significant interaction of group by DSE type, F(2,135) = 7.59, p = .001, partial η2 = .05, as well as a significant interaction of session by DSE type F(2,135) = 20.58, p < .001, partial η2 = .13, thus we did not interpret the main effect of group in the presence of interactions. We followed up on the group by type interaction with univariate GLMs to investigate the effect of group on each DSE subtype. There was a significant main effect of group on mean physical DSE behavior across sessions, F(2,135) = 10.3, p < .001, partial η2 = .13, with Bonferroni post hoc tests indicating pair-wise differences between PIs and NAs (p < .001) on the one hand, and EAs and NAs (p = .02) on the other hand. Both adopted groups (PI and EA/FC) exhibited on average significantly more physical DSE behavior (M = .22, SE = .08 and M = .05, SE = .09, respectively) compared to the non-adopted group (M = -.28, SE = .08). Among adopted children, EAs did not differ significantly from PIs (p = .41). There was no effect of group on non-physical social engagement behavior (F(2,135) = .36, p = .70), with mean levels of the social approach dimension of DSE being almost identical across the three groups.
We then probed the session by type interaction on DSE behavior. Paired-samples t-tests indicated that the interaction effect was due to physical DSE decreasing significantly from Time 1 to Time 2 (t(137)= 2.16, p = .03) in the entire sample, while non-physical social engagement increased significantly from Time 1 to Time 2 in the entire sample (t(137) = -3.27, p = .001). Mean levels of physical and non-physical DSE by adoption group and session are displayed in Figure 1. As illustrated in Fig.1, the PI and EA/FC groups tended to show decrements in physical DSE over time, whereas the non-adopted group did not show any significant changes in physical DSE over time, NA: t(46) = .26, p = .80. All groups showed the same pattern of increasing levels of sociability over time. Given the wide age ranges and the slightly higher age of the EA/FC group, we repeated this analysis controlling for age. Again, there were no significant main effects of session or type on DSE behavior, and there continued to be a significant effect of group, F(2,134) = 3.95, p =.02, partial η2 = .06, and a significant interaction of group by DSE type, F(2,134) = 7.12, p = .001, partial η2 = .10. Results of follow up analyses did not change (i.e. PI and EA/FC continued to differ from NA children [but not from each other] on the physical factor, no group differences on the non-physical factor). The interaction of session by DSE type was no longer significant after controlling for age but there was a non-significant trend for an association between age and DSE type, F(1,134) = 2.77, p = .099, partial η2 = .02.
Figure 1.
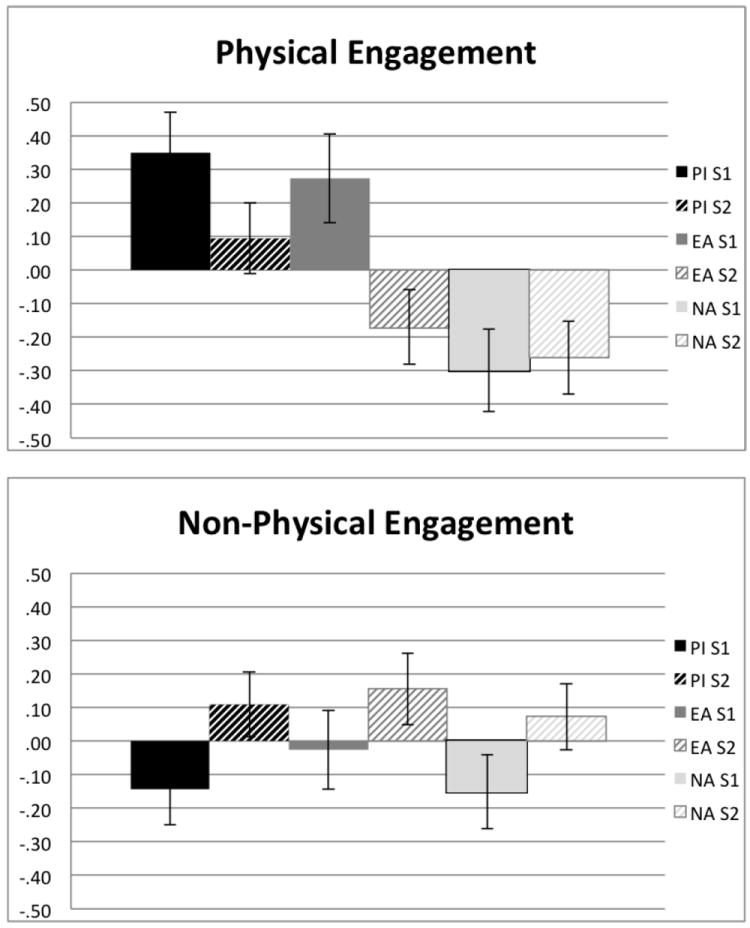
Descriptive levels of grand mean centered physical and non-physical social engagement by adoption group over time. Error bars are SEMs.
To examine within-subjects stability of DSE behaviors over time, we computed correlations between Time 1 and Time 2 levels of these behaviors. Physical DSE behavior was highly unstable across these two time points within each of the three groups (PI: r(48) =.04, p = .77; EA/FC: r(39) = -.11, p = .48, NA: r(45) = -.14, p = .35), whereas the more normative non-physical sociability factor had high stability in the EA/FC (r(39) = .53, p < .001) and NA (r(45) = .50, p < .001) groups, with poorer stability in the PI group (r(48) = .20, p = .17).
Associations with Parent Reported Temperament
To further confirm the distinction between the physical and non-physical DSE factors, the relationship between the composite scores and parent rated temperamental inhibition (“shyness”) was examined. The DSE non-physical composite was inversely correlated with parent rated “shyness” at both time points (r(129)= -.24, p = .006, r(125) = -.25, p = .004; for sessions 1 and 2 respectively), whereas the physical DSE was not associated with temperamental shyness at either session (r(129) = -.09, p = .32, r(125) = .06, p = .48). In a repeated-measures GLM controlling for Time 1 shyness and examining the effects of group, session and type, we obtained a similar pattern of results described, with a main effect of group (F(2,127) = 3.95, p = .022) and a significant interaction of group by type (F(2,127) = 8.41, p <.001). The interaction of type by session now became marginally significant (F(1,127) = 3.41, p = .07). When probing the group × type interaction and still controlling for shyness, we obtained the same results previously mentioned such that there was a main effect of group on the physical engagement dimension (F(2,127) = 10.6, p < .001), with PIs and EAs having higher levels of overall physical engagement than NAs (p <.001 and p = .004, respectively), but groups did not differ on the non-physical dimension (F(2,127) = .18, p = .83).
Correlates of DSE in Adopted Children
We first examined correlations of physical DSE with institutional care variables for the PI children. Bivariate correlations (see Table 3) showed that physical DSE in PI children at Session 1 was not associated with length of institutionalization (r(48) = .10, p = .50), number of transitions prior to adoption (r(48) = -.05, p = .75). IQ was only available for the PI children 12 months post adoption, but physical DSE was not a significant correlate (r(43) = .20, p = .18). Physical DSE at Session 2 was also not associated with any of these variables (p’s > .2). Finally, for both EA/FC and PI children we examined whether there were differences by birth regions. Groups were combined for these analyses to provide sufficient cell sizes. No differences were noted for either type of DSE: Physical- S1: F(3,87) = 1.5, p =.22; S2: F(3,87) = 1.3, p = .27; Non-physical- S1: F(3,87) = 1.4, p = .25, S2: F(3,87) = .96, p = .56.
Table 3.
Correlations between variables of interest.
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | |
|---|---|---|---|---|---|---|---|
|
| |||||||
| 1. Session 1 Physical | - | ||||||
| 2. Session 1 Non-physical | .46** | - | |||||
| 3. Session 2 Physical | .08 | .03 | - | ||||
| 4. Session 2 Non-physical | .19* | .38** | .30** | - | |||
| 5. Parent reported Shyness | -.09 | -.24** | -.04 | -.29** | - | ||
| 6. Age at Session 1 | -.07 | .03 | -.09 | .08 | -.03 | - | |
| 7. IQ | .20 | .17 | -.17 | .09 | -.05 | -.32* | - |
p < .05;
p < .01
Discussion
DSE is one of the most commonly reported socially aberrant behaviors in PI children, but little research has systematically differentiated these behaviors from normative sociability. The current study examined DSE in a group of newly adopted PI children compared with children adopted early from overseas foster care and non-adopted children. Using behavioral observations of an interaction with an unfamiliar adult, this study sought to deconstruct some of the complexities of DSE behavior. The first aim was to distinguish atypical behaviors from behaviors that are prevalent and show wide variation in NA children. Behaviors such as frequency of initiation, approach, and response to the stranger’s initiation, duration of proximity, and latency to approach to the stranger all showed wide variation in NA children, increased over time with normative gains in social development, and were therefore considered typical. Conversely, all measures of non-incidental physical contact and intimacy were rare in NA children and, we argue, would be considered inappropriate by social and cultural standards, suggesting they represent a more atypical pattern of behavior. The two factors drawn from the observed behaviors represent the two dimensions of social engagement. The first factor suggests a temperamental non-physical social engagement dimension while the second factor suggests an atypical physical engagement dimension.
High levels of social approach behavior can be observed, in some settings, among typically developing, non-disordered children. In the present experimental situation the child met a stranger in the presence of their parent. It is not inappropriate to be social with that person and thus, results show a wide variety of non-physical sociality, which could be considered normal temperamental disinhibition or extraversion. This non-physical social engagement behavior is correlated inversely with parent reports of shyness and, indeed, the measures that load on this factor are the same measures which, if coded inversely, would be used to assess shyness. In this situation results showed no group difference; however, it is possible that group differences might arise if children were assessed in a situation where it would be inappropriate to speak to or be social with the stranger (perhaps if the parent had not been present). This possibility remains to be examined. Conversely, physical contact with a stranger is culturally inappropriate in our society. PI and EA/FC children continue to demonstrate this behavior even though there are few situations that we can imagine where intimate contact with a stranger would be normative behavior.
The division between non-physical social engagement behavior and physical DSE is important for the study of DSE and related behaviors. Different measures of DSE may have been picking up different dimensions of social disinhibition. This is likely why some studies (e.g. O’Connor et al., 1999) found the presence of some DSE in non-institutionalized children. It is interesting that there has been a high degree of consistency in the findings on DSE despite this possible measurement issue. It is likely that the measures used thus far have tapped, to some extent, both dimensions of disinhibition.
The second aim of the present study was to examine how atypical and typical behaviors differ between NA, EA/FC and PI children. Examination of the non-physical social disinhibition factor suggests that the groups did not differ significantly on this dimension, extending the evidence that these types of gregarious social behaviors reflect a temperamental social disinhibition rather than problematic DSE behaviors. In line with previous research, PI children did differ from NA children on the physical DSE dimension. PI children showed more physical engagement than NA children at both time points. This pattern of group differences further validates the scales we constructed, and supports the notion that they are different dimensions. As in previous studies of PI children, the differences are driven by a minority of PI children showing excessive DSE behavior (e.g., 5 touches, 84 seconds of physical contact) while other PI children show no abnormal behavior.
The third aim was to examine whether DSE is unique to PI children. Replicating the results of a recent study (Bruce et al., 2009), EA/FC children also showed more physical DSE than NA children, with means falling between NA and PI groups. This may indicate that prenatal factors may be involved in the etiology of DSE behaviors, or that one significant care transition (i.e. adoption) is sufficient to increase rates of this behavior. However, it is also important to note that the EA/FC children also had non-normative early experiences, for example experiencing brief institutionalization, neglectful caregivers, or more frequent transitions, which may have contributed to the development of this behavior.
And finally, our fourth and fifth aims were to evaluate the extent to which DSE changed over time, and how it relates to other child characteristics. Non-physical social disinhibition increased over time, while physical DSE decreased in the adopted children, but not in the NA children who had low levels of physical DSE to begin with. This could suggest there is a developmental course of this type of social engagement, which is supported by the fact that these changes with time became non-significant when age was controlled in the analyses. In addition, reduction in novelty of the situation may also be playing a role. As the situation becomes more familiar (although not the stranger, as there is a unique experimenter at each session), children may be willing to be more social with a stranger, at least when they are in their mother’s presence. In this case, it is possible that novelty was inhibiting sociability at Session 1. Conversely, with the reduction in novelty at Session 2, physical contact decreases. That may suggest that novelty was disinhibiting physical contact. Perhaps the strategy of disinhibited physical engagement is a coping mechanism for anxiety provoking situations for internationally adopted children. Alternatively, perhaps children are decreasing their physical DSE with the developing awareness of social boundary norms.
In terms of correlates of DSE behavior, levels of DSE were not related to length of institutionalization or number of care transitions, which is in contrast with other studies of PI children (e.g. Chisholm, 1998; Bruce et al, 2009). This may be due to the differences between the current samples and prior adoption samples. The current sample is far more diverse in origin and experience than many previous studies, and includes only children adopted at more than 6-months-old (EA/FC) or 16-months-old (PI). Studies reporting no differences in DSE between PI and non-PI children have noted this for children adopted at 6 months or younger (e.g., O’Connor et al., 1999; O’Connor & Rutter, 2000). It may also be due to different methods of measuring DSE, although neither composite was correlated with length of institutionalization or number of transitions. Consistent with prior research (Bruce et al., 2009; O’Connor et al., 1999, O’Connor & Rutter, 2000) results showed no association between DSE and general cognitive ability in PI children. Thus, disinhibited social engagement does not seem to be a manifestation of a general developmental delay.
The current study had several limitations. First, this study did not include measures of DSE reported by the parents, a method commonly used to measure DSE in previous research (e.g. Chisholm, 1998; O’Conner, et al., 1999) and often the basis for seeking clinical services. It will be very important to see how parent-reported DSE relates to the physical and non-physical dimensions of social disinhibition. Currently available parent-report measures are designed to be used after the child has been with the caregiver for an extended amount of time, and therefore were not appropriate to use in the current study. However, we plan to address this limitation as part of the ongoing longitudinal study of these children. In addition, the predictive validity of the current DSE coding scheme was not tested, so future research should evaluate whether observational measures used soon after adoption predict which children will continue to show this behavior years later and whether it is associated with other deleterious outcomes. We also plan to investigate the predictive value of these behaviors for longer-term socio-emotional and clinical outcomes assessed during kindergarten.
It is also important to note that there was a large difference in racial compositions of the three groups. It is unlikely that these affected the results for several reasons. First, when we analyzed the effect of world region of origin, we found no differences in DSE behaviors, despite the racial differences between Southeast Asia, Russia/Eastern Europe and Latin America. Second, despite racial differences between the PI and EA/FC groups, we did not observe significant differences between these groups in DSE behaviors. In addition, many of the PI children were Caucasian, while none of the EA/FC children were, yet the largest mean differences were between the PI and NA groups. Taken as a whole, these data argue against a racial explanation for differences in DSE between the adopted and non-adopted groups.
Finally, while the lack of homogeneity in the adoptive sample can be seen as both a limitation as it introduces complexity, it is also a strength of this study as it increases generalizability of the findings.
A final limitation is the need to verify these two DSE dimensions in a future study using confirmatory factor analysis.
Despite these limitations, the present study provides valuable information regarding the delineation of typical and atypical social behaviors, the differences between PI, EA/FC, and NA children on these behaviors, and how these behaviors change over time. Future research should investigate further correlates of DSE, including aspects of the post-adoption environment that could contribute to the lasting exhibition of this behavior. As DSE has been demonstrated in domestic maltreated children in addition to internationally adopted children, future research should also investigate the possibility that variations in parenting may lead to variation in DSE behavior. This may help us elucidate the etiology of this behavior and offer insights into ways of changing it.
Differentiation of typical and atypical behaviors to strangers may facilitate better identification of emotional, social and neurocognitive correlates of DSE and foster earlier identification of PI children at risk for DSE problems. Furthermore, it may reduce concerns by clinicians and parents about the possibility of a disorder in PI children that only exhibit normative temperamental sociability. Understanding the etiology of DSE behavior will help with creating interventions for these children and preventing DSE behaviors from leading to other socioemotional problems.
Acknowledgments
We thank the families who participated in this research and the International Adoption Project at the University of Minnesota. This study was supported by Grants R01MH080905 and P50MH078105 (to M.R.G.) and partly by the Center for Neurobehavioral Development at the University of Minnesota. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Mental Health or the National Institutes of Health.
Appendix A. Observational qualitative coding scheme
Response to Experimenter Greeting
| 0 | Ignores |
| There is absolutely no positive nonverbal or verbal response to the introduction. Note that a wary child may stare at the experimenter, but this is not to be considered a positive non-verbal response. | |
| 1 | Orients to experimenter |
| Child looks toward the experimenter in response to the introduction, and smiles or otherwise positively and non-verbally acknowledges the introduction. But child does not approach the E and does not attempt more than this brief acknowledgement. | |
| 2 | Brief response to experimenter |
| Child gives a one-word response to the introduction (i.e., “Hi.”). Or child leans towards, takes one or two steps towards, or shows the experimenter something. | |
| 3 | Lengthy response to experimenter |
| Child gives lengthy response following the introduction without pause. Child speaks with or approaches close to the experimenter or engages in prolonged showing of things to the experimenter. | |
| Note that if child has begun to respond to the E before the E has a chance to introduce herself, give the code you would have given, had this level of interaction been occasioned by the introduction. |
Response to Toy Offering
| 0 | Ignores or declines and never plays with toys |
| Child ignores or declines the invitation to play and never plays with the toys during Phase 3. | |
| 1 | Ignores or declines but does play with toys without E |
| Child ignores or declines the invitation and never accepts E and toys. But, child manages to get a toy or two to play with while shutting the E out. This child either moves toys over near mom and turns back on or face away from E, or this child corrals some toys to play with while sitting closer to E but otherwise ignoring and shutting E out. | |
| 2 | Eventually plays with E & toys |
| Child initially ignores or declines the invitation to play, but then eventually plays with the toys in a way that includes acceptance of the E before the end of Phase 3. To get this score, the child must not seem to be shutting the E out. Playing with the toys must seem like an acceptance of the E and her toys, though it takes a while. | |
| 3 | Plays with E & toys |
| Child accepts the invitation, but approaches slowly or cautiously. Once playing the child shows acceptance of E and the toys on a higher level than a “2”. This means the child does not seem to be avoiding looking at the E, although the child may still seem slightly unsure of E. | |
| 4 | Accepts and plays immediately |
| Child nonverbally or verbally accepts the invitation to play and plays immediately (e.g., helps get toys out, plays with first toy put out). This child plays with the toys, but does not actively try to get the E to play with him/her. This can be scored if the child’s response is delayed due to their needing to complete some task that they were already doing when the play invitation was made, but once involved the child acts like a “4”. | |
| 5 | Accepts and plays immediately; Engages E |
| Child accepts and plays immediately, focusing not only on the toys, but actively attempts to engage the E in the toy play. When E does not respond, the child may become unsure and begin acting like a 4. | |
| 6 | Accepts and plays immediately; Needs E |
| Child accepts and plays immediately, actively tries to get E to play, and when E responds minimally, child keeps up and intensifies his/her bids. |
Response to Play Invitation
| 0 | Ignores or declines |
| Child ignores or declines invitation. | |
| 1 | Accepts with encouragement |
| Child accepts invitation with encouragement (i.e., “It’s really fun.”). Child may spend most of this period watching the E play with the toys or engaging in parallel play with the E. Throughout, though, the sense is the child would be happier if the E wasn’t there. Quality of toy play may be lower during this period than when the E was sitting quietly. | |
| 2 | Accepts; more interest in toys than E |
| Child accepts invitation immediately. Child responds avidly to E’s play initiations, but otherwise seems more interested in the toys than in playing WITH the E and the toys. | |
| 3 | Accepts; equal interest in toys & E |
| Child accepts invitation immediately, responds to E’s play initiations and makes play initiations to the E, handing her toys, sharing her experiences with the E verbally and non-verbally. However, the overall sense is that the toys are as important as playing with the E. | |
| 4 | Accepts; more interest in E than toys |
| Child accepts invitation immediately, responds to and initiates interactions with the E. Keeps E responding throughout the together play time. The strong sense is that while the toys are interesting, playing with the E is the child’s bigger goal. |
Verbal Intimacy (0-5)
This scale assesses the child’s level of intimacy in verbal or preverbal communication with the experimenter. Score the highest achieved throughout the DSE task.
| 0 | None |
| The child did not communicate with the experimenter at all. There were no verbalizations or preverbal communications to the experimenter. | |
| 1 | Only verbal or preverbal responses |
| There were only brief responses to the experimenter’s questions (i.e., a one-sentence logical response). Also include preverbal responses, such as looking at what the E is talking about or pointing to. | |
| 2 | Initiated basic communication |
| The child initiated communication on a basic level verbally or preverbally. Child’s verbalizations and/or preverbal communications were designed to initiate or maintain interactions with the experimenter beyond a response to a response to a direct question. However, all initiations involved events within the room. They did not involve divulging of information about the child or his/her family, except for the child’s name or showing off of a pretty shirt or something as a way of starting a conversation. | |
| 3 | Shared some personal information |
| Child’s verbal interactions with the E involved sharing of personal information, but not of the particularly intimate type. The child may have talked about school, the fact they have a dog, or that they were going to McDonalds on the way home. The child didn’t ask intimate questions of the E. If the child asked personal information of the E, this information seemed to be a way of entering a topic the child wanted to talk about: “Do you have a dog? I have a dog…” | |
| 4 | Shared intimate information or asked personal questions |
| Child’s verbal interactions with the E involved sharing of intimate information beyond the usual public kind. This child might have told the E that she wet her bed last night, that her mom and dad had a fight, that her baby brother pooped in the bath tub, and so on. Even if the child didn’t divulge this level of intimate information, score a 4 if the child asked the E questions about her personal life, like “Do you have a dog?” (Unless this is just to introduce a topic the child wants to talk about). Many questions may have followed about the E. The child may not even have stopped to hear the E’s answer. However, the child’s questions were not of the embarrassing kind. | |
| 5 | Shared highly intimate information or asked very personal questions |
| Child’s verbal interactions with the E involve sharing of personal information and/or requests for personal information of the type typically not asked of strangers: “Are you married?”; “Do you have a boyfriend?”; “Are you having a baby?” If at any point the child asks to come home with the E, visit the E’s house, or meet the E’s boyfriend, parents, etc., score the a 5 regardless of the content of the other vocalizations. If the child only invites the E to his/her house or to join them at McDonalds, then base scoring on other aspects of his/her communication with the E, although in this instance the child would not score below a 3. |
Physical Intimacy (0-5)
This scale assesses the child’s level of intimacy in physical contact with the experimenter. Score the highest achieved throughout the DSE task.
| 0 | None |
| Child did not physically contact the experimenters. There was no physical contact between the E and child, except for that which happened by chance or is required to get a task done. | |
| 1 | Physical contact as a tool |
| Physical contact between E and child occurred, but it was as if the E was a tool or a piece of the furniture. Child may have used E as a support in getting to a toy or pushed E’s hand to get her to do something. | |
| 2 | Initiated low-level physical contact |
| Physical contact between E and child occurred and was initiated by child. Child may have leaned against the E while playing, when it was unnecessary. The sense here is not that E was furniture, but that the contact was pleasant to the child. Contact was pretty low level, though, and tended to involve child’s hand, back, leg or arm. There was no evidence of the child initiating contact that would have brought more “intimate” parts of their body into contact with the E. | |
| 3 | Initiated physical contact on a familiar-level |
| Physical contact between the E and child occurred, was initiated by the child and involved contact of the child’s bottom, chest, or face with the E’s body. Sitting in the E’s lap, or leaning of the torso and face against the E’s side/arm counts here. This behavior might seem appropriate if the E were the child’s teacher or a friend of the family with whom the child is very familiar. | |
| 4 | Initiated intimate physical contact |
| Physical contact between the E and child occurred, was initiated by the child, and involved active attempts to snuggle and to get E to respond. This behavior would seem appropriate if the E were the child’s mother, child care provider, close grandparent or aunt/uncle, or someone who is in the circle of “loved ones.” | |
| 5 | Initiated physical contact that invaded the E’s privacy |
| Physical contact between the E and the child occurred, was initiated by the child, and invaded the E’s privacy. This may have involved playing with the E’s face or earrings in a way that required the child to bring his/her face within an inch or so of the E’s face. Touching intimate parts of the E’s body (i.e. breasts, bottom) would certainly count here. Also counting would be lifting of the child’s clothing so that the child’s skin touched the E or if the child rubbed his/her chest, bottom, etc. against the E even if skin was not exposed. This level of physical contact would be odd even with the parent if the child is beyond toddlerhood and with other “loved ones” even for a toddler. It has a sense of being sexually provocative. |
References
- American Psychological Association. Diagnostic and Statistical Manual of Mental Disorders. Fifth Edition. Washington, DC: American Psychiactric Association; 2013. [Google Scholar]
- Brannick MT. Critical comments on applying covariance structure modeling. Journal of Organizational Behavior. 1995;16(3):201–213. [Google Scholar]
- Bruce J, Tarullo AR, Gunnar MR. Disinhibited social behavior among internationally adopted children. Development and Psychopathology. 2009;21(1):157–171. doi: 10.1017/S0954579409000108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cicchetti D. The emergence of developmental psychopathology. Child Development. 1984;55:1–7. [PubMed] [Google Scholar]
- Chisholm K. A three year follow-up of attachment and indiscriminate friendliness in children adopted from Romanian orphanages. Child Development. 1998;69(4):1092–1106. [PubMed] [Google Scholar]
- Chisholm K, Carter MC, Ames EW, Morison SJ. Attachment security and indiscriminately friendly behavior in children adopted from Romanian orphanages. Development and Psychopathology. 1995;7:283–294. [Google Scholar]
- Fisher L, Ames EW, Chisholm K, Savoie L. Problems Reported by Parents of Romanian Orphans Adopted to British Columbia. International Journal Of Behavioral Development. 1997;20(1):67–82. [Google Scholar]
- Gleason MM, Fox NA, Drury S, Smyke A, Egger HL, Nelson CA, et al. Validity of evidence-derived criteria for reactive attachment disorder: Indiscriminately social/disinhibited and emotionally withdrawn/inhibited types. Journal of the American Academy of Child & Adolescent Psychiatry. 2011;50(3):216–231. doi: 10.1016/j.jaac.2010.12.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gorsuch RL. Factor Analysis. 2. Mahwah, NJ: Lawrence Erlbaum Associates; 1983. [Google Scholar]
- Gunnar MR. Effects of early deprivation: Findings from orphanage-reared infants and children. In: Nelson CA, Luciana M, editors. Handbook of Developmental Cognitive Neuroscience. Cambridge, MA: MIT Press; 2001. pp. 617–629. [Google Scholar]
- Gunnar MR, Bruce J, Grotevant HD. International adoption of institutionally reared children: research and policy. Development and Psychopathology. 2000;12(4):677–693. doi: 10.1017/s0954579400004077. [DOI] [PubMed] [Google Scholar]
- Gunnar MR, van Dulmen MH. Behavior problems in postinstitutionalized internationally adopted children. Development and Psychopathology. 2007;19(1):129–148. doi: 10.1017/S0954579407070071. [DOI] [PubMed] [Google Scholar]
- Hodges J, Tizard B. Social and family relationships of ex- institutional adolescents. Journal of Child Psychology and Psychiatry. 1989;30(1):77–97. doi: 10.1111/j.1469-7610.1989.tb00770.x. [DOI] [PubMed] [Google Scholar]
- Kreppner J, Kumsta R, Rutter M, Beckett C, Castle J, Stevens S, et al. IV Developmental course of deprivation-specific psychological patterns: early manifestations, persistence to age 15, and clinical features. Monographs of the Society for Research in Child Development. 2010;75(1):79–101. doi: 10.1111/j.1540-5834.2010.00551.x. [DOI] [PubMed] [Google Scholar]
- Lyons-Ruth K, Bureau JF, Riley CD, Atlas-Corbett AF. Socially indiscriminate attachment behavior in the strange situation: Convergent and discriminant validity in relation to caregiving risk, later behavior problems, and attachment insecurity. Development and Psychopathology. 2009;21:355–367. doi: 10.1017/S0954579409000376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mulaik SA. Foundations of Factor Analysis. 2. Chapman & Hall/CRC; Boca Raton, FL: 2010. [Google Scholar]
- Mullen EM. Mullen Scales of Early Learning. American Guidance Service, Inc.; Circle Pines, MN: 1995. [Google Scholar]
- O’Connor TG, Bredenkamp D, Rutter M The ERA Study Team. Attachment disturbances and disorders in children exposed to early severe deprivation. Infant Mental Health Journal. 1999;20(1):10–29. [Google Scholar]
- O’Connor TG, Marvin RS, Rutter M, Olrick JT, Britner PA. Child-parent attachment following early institutional deprivation. Development and Psychopathology. 2003;15(1):19–38. doi: 10.1017/s0954579403000026. [DOI] [PubMed] [Google Scholar]
- O’Connor TG, Rutter M. Attachment disorder behavior following early severe deprivation: extension and longitudinal follow-up. Journal of the American Academy of Child and Adolescent Psychiatry. 2000;39(6):703–712. doi: 10.1097/00004583-200006000-00008. [DOI] [PubMed] [Google Scholar]
- Oosterman M, Schuengel C. Autonomic reactivity of children to separation and reunion with foster parents. Journal of the American Academy of Child & Adolescent Psychiatry. 2007;46(9):1196–1203. doi: 10.1097/chi.0b013e3180ca839f. [DOI] [PubMed] [Google Scholar]
- Pears KC, Bruce J, Fisher PA, Kim HK. Indiscriminate friendliness in maltreated foster children. Child Maltreatment. 2010;15(1):64–75. doi: 10.1177/1077559509337891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Putnam SP, Gartstein MA, Rothbart MK. Measurement of fine-grained aspects of toddler temperament: The early childhood behavior questionnaire. Infant behavior & development. 2006;29(3):386–401. doi: 10.1016/j.infbeh.2006.01.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roy P, Rutter M, Pickles A. Institutional care: associations between overactivity and lack of selectivity in social relationships. Journal of Psychology and Psychiatry. 2004;45(4):866–873. doi: 10.1111/j.1469-7610.2004.00278.x. [DOI] [PubMed] [Google Scholar]
- Rutter M, Colvert E, Kreppner J, Beckett C, Castle J, Groothues C, et al. Early adolescent outcomes for institutionally-deprived and non-deprived adoptees. I: Disinhibited attachment. Journal of Child Psychology and Psychiatry. 2007;48(1):17–30. doi: 10.1111/j.1469-7610.2006.01688.x. [DOI] [PubMed] [Google Scholar]
- Save the Children. Institutional care: The last resort. Advocacy brief. London: Author; 2009. Retrieved January 29, 2013, from http://resourcecentre.savethechildren.se/content/library/documents/institutional-care-last-resort-policy-brief. [Google Scholar]
- Smyke AT, Zeanah CH, Fox NA, Nelson CA, Guthrie D. Placement in foster care enhances quality of attachment among young institutionalized children. Child development. 2010;81(1):212–223. doi: 10.1111/j.1467-8624.2009.01390.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smyke AT, Zeanah CH, Gleason MM, Drury SS, Fox NA, Nelson CA, Guthrie D. A Randomized Controlled Trial Comparing Foster Care and Institutional Care for Children With Signs of Reactive Attachment Disorder. American Journal of Psychiatry. 2012;169:508–514. doi: 10.1176/appi.ajp.2011.11050748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sroufe LA. Wariness of strangers and the study of infant development. Child Development. 1977;48(3):731–746. [Google Scholar]
- Tapp J. Procoder for Digital Video. Nashville, TN: Vanderbilt Kennedy Center; 2003. Computer software. [Google Scholar]
- The English and Romanian Adoptees (ERA) Study Team. II. Methods and measures used for follow-up at 15 years of the English and Romanian Adoptee (ERA) study. Monographs of the Society for Research in Child Development. 2010;75(1):21–47. doi: 10.1111/j.1540-5834.2010.00549.x. [DOI] [PubMed] [Google Scholar]
- Tizard B, Hodges J. The effect of early institutional rearing on the development of eight year old children. Journal of Child Psychology and Psychiatry. 1978;19(2):99–118. doi: 10.1111/j.1469-7610.1978.tb00453.x. [DOI] [PubMed] [Google Scholar]
- Tizard B, Rees J. The effect of early institutional rearing on the behaviour problems and affectional relationships of four-year-old children. Journal of Child Psychology and Psychiatry. 1975;16(1):61–73. doi: 10.1111/j.1469-7610.1975.tb01872.x. [DOI] [PubMed] [Google Scholar]
- Williamson J, Greenberg A. Families, Not Orphanages. Better Care Network. 2010 Working Paper. [Google Scholar]
- Zeanah CH, Gleason MM. Reactive Attachment Disorder: A Review for DSM-V. 2010 Retrieved from http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=120.
- Zeanah CH, Scheeringa MS, Boris NW, Heller SS, Smyke AT, Trapani J. Reactive attachment disorder in maltreated toddlers. Child Abuse and Neglect: The International Journal. 2004;28:877–888. doi: 10.1016/j.chiabu.2004.01.010. [DOI] [PubMed] [Google Scholar]
- Zeanah CH, Smyke AT, Dumitrescu A. Attachment disturbances in young children: II. Indiscriminate behavior and institutional care. Journal of the American Academy of Child and Adolescent Psychiatry. 2002;41:983–989. doi: 10.1097/00004583-200208000-00017. [DOI] [PubMed] [Google Scholar]
- Zeanah CH, Smyke AT, Koga SF, Carlson E. Attachment in institutionalized and community children in Romania. Child Development. 2005;76(5):1015–1028. doi: 10.1111/j.1467-8624.2005.00894.x. [DOI] [PubMed] [Google Scholar]