

Abstract
Objective
To assess the baseline interest of the public in whole genome sequencing (WGS) for themselves, parents’ interest in WGS for their youngest children, and factors associated with such interest.
Methods
A random sample of adults from a probability-based nationally representative online panel was surveyed. All participants were provided basic information about WGS and then asked their interest in WGS for themselves. Those participants who self-identified as parents were asked about their interest in WGS for their children. The order in which parents were asked about their interest in WGS for themselves and their child was randomized. The relationship between parent/child characteristics and interest in WGS was examined.
Results
Overall response rate was 62% (55% among parents). 58.6% of the total population (parents and non-parents) was interested in WGS for themselves. Similarly, 61.8% of parents were interested in WGS for themselves and 57.8% were interested in WGS for their youngest children. Of note, 84.7% of parents showed an identical interest level in WGS for themselves and their youngest children. Mothers as a whole, and parents whose youngest children had ≥2 health conditions had significantly more interest in WGS for themselves and their youngest children, while those with conservative political ideologies had considerably less.
Conclusions
While U.S. adults have varying interest levels in WGS, parents appear to have similar interests in genome testing for themselves and their youngest children. As WGS technology becomes available in the clinic and private market, clinicians should be prepared to discuss WGS risks and benefits with their patients.
Keywords: whole genome sequencing, public interest, parents, children
Introduction
Whole genome sequencing (WGS) is the process of identifying nearly every base pair in an individual's DNA, or – in the case of whole exome sequencing – bases that encode proteins. Compared to other genetic testing technology, WGS generates significantly more information, much of it of uncertain value. Recently, the cost of WGS has fallen to about $4,000, and many predict the cost will fall to near $1,000 in the near future1-3 – making its routine use within and outside the clinical arena an impending reality.4,5 Whole exome sequencing prices are already on the order of $1,000 at Scienceexchange.com. In addition, the NIH has targeted $15 million dollars for research aimed at reducing the cost of WGS to $1,000 (RFA-HG-10-012), and $6.5 million to clinical research focused on the application of genomic data to patient care (RFA-HG-12-008, RFA-HG-12-009).
WGS raises numerous ethical challenges.6-11 These challenges include privacy protection (both for the child and for the child's relatives), availability of data to researchers, how to address incidental findings of limited utility and predictive value, how to address diseases where our clinical interventions are limited, and how to provide effective informed consent. These issues are further complicated in a pediatric setting where the issues of parents’ autonomy and children's privacy often compete, especially when disease risk may not be relevant for decades, such as in hypertension or Huntington's disease.
Genome sequencing is now being used in the clinic,4,12-14 and parents will likely soon be more frequently making decisions about WGS for their children. There are already a number of examples of how WGS has been used with children and their families.15,16 These testing platforms may identify unknown genetic causes of childhood diseases or help families better understand their child's predisposition to future disorders.
Previous studies on public opinion have explored parental interest in personal genetic testing for their children,17,18 and looked at qualitative perspectives on ethical issues related to WGS.19,20 Levenseller et al. explored such ethical issues in a non-random sampling of children with specific health conditions, parents of such children, and health care providers, and found differences in priorities among these groups.11 Goldenberg et al. specifically examined interest in WGS in the context of newborn screening,21 and found an interest level of about 70%. In addition, a handful of studies have also assessed public interest in personal genetic testing.17,22-28 Despite this interesting work, to the best of our knowledge, no studies have examined a sample of the general population for parents’ interest in WGS for themselves or their children in a general clinical setting, or a correlation of parents’ interest in WGS for themselves with their interest for their children. Such information could both inform use of next generation sequencing technology in the clinical setting and also help clinicians better understand the attitudes and concerns of their patients.
Methods
Study Design
In May 2012, we conducted a cross-sectional, internet-based survey of a nationally representative sample of the US population regarding interest in whole genome sequencing for themselves and, when applicable, for an individual's youngest child. This survey was conducted as part of the C.S. Mott Children's Hospital National Poll on Children's Health (NPCH), a recurring online survey of parents and non-parents,29 that has served as the platform for several peer-reviewed studies of national attitudes, beliefs and self-reported behaviors of the U.S. public.30-33 Prior to conducting our full survey, we ran a pilot study to optimize our survey. The University of Michigan Medical School Institutional Review Board approved this study.
Study Population
The NPCH is conducted using GfK's (Gesellschaft für Konsumforschung, a private market research company) web-enabled KnowledgePanel®, a probability-based panel designed to be representative of the U.S. population.34 Potential participants are identified by a random selection of telephone numbers and residential addresses and then invited by telephone or by mail to participate in the web-enabled KnowledgePanel®. If individuals agree to participate, but do not have internet access, GfK provides them a laptop and internet service provider connection at no cost. Panelists then receive unique login information for accessing surveys online, and receive emails throughout each month inviting them to participate in research.
Survey Administration
The NPCH was pilot-tested for this study by GfK in April 2012 with a separate convenience sample of 105 KnowledgePanel® members. The descriptions were based on information provided by the National Human Genome Research Institute on its website entitled “A Brief Guide to Genomics”.35 Survey background and questions were refined based on pilot testing. A unique KnowledgePanel® sample was drawn for the NPCH that contained the survey items for this study. The introductory email invited participation in a survey about child health. No incentive participation was offered to prospective participation, beyond participation points that GfK panelists receive as part of their routine survey activities. To ensure adequate representation, parents (defined as having child(ren) 0-17 years old living in the household), and particular racial minorities including African Americans and Hispanics were oversampled.
Survey Items
All survey respondents received the following brief explanation of WGS:
Our Health and Our Genes
Staying healthy and getting sick are affected by many things. Our genes – which we inherit from our parents – can affect our health and illness in many ways. Genes are made of DNA, and contain the instructions needed for our bodies to grow and function. All of the genes in a person make up that person's genome.
What is Whole Genome Sequencing?
It is possible to study a person's entire genome. This process is called whole genome sequencing. It may give information about a person's risk of having different diseases in the future.
This language was intended to give participants basic information about genetics and sequencing, representative of the kinds of information they may find outside of the clinic setting.
We then asked all respondents the following question along with a Likert scale of responses (definitely interested/somewhat interested/ not interested/ definitely not interested):
How interested would you be in getting your whole genome sequenced?
In addition, respondents who identified themselves as parents received the following question (completed with the age of their youngest child inserted in the brackets):
How interested would you be in getting your [x-month/year-old] child's whole genome sequenced?
For parents, the order of these two questions was randomized. A four-point Likert scale was chosen so participants be compelled to choose a position and to avoid ambivalence.
We also collected the following information from respondents about themselves: age, sex, race/ethnicity, education, household income, political ideology, rating of personal health, and if they plan to have a child within five years (only asked if respondent < 45 years of age). For parents, we also gathered the following information about all of their children in the household: age, sex, and whether their children have any specific health conditions (see Appendix 1 for list of health conditions).
Statistical Analysis
GfK provided the study team with de-identified data, along with Census-based poststratification weights used to match the US population distribution on sex, age, race/ethnicity, education, census region, income, and political ideology. All analyses were conducted with Stata® 12 (Stata Corp. LP, College Station, TX). All results reflect weighted data unless otherwise indicated. Among completed surveys, there was the following individual item non-response: health of the youngest child (6% nonresponse) and political ideology (4% nonresponse overall and 4.5% nonresponse among parents). All other single question nonresponse rates were less than 2%. Cases with non-response on specific items were dropped from analyses on an item-by-item basis.
Respondent Characteristics
We grouped respondents by parent status (parent vs. non-parent) and calculated frequency distributions for age, race/ethnicity, sex, education level, income, political ideology, personal health, and plans to have children in the next 5 years for parents, non-parents, and the overall survey population (Table 1). Differences in characteristics between parents and non-parents were tested with a Rao and Scott corrected Pearson's chi-square test for categorical characteristics,36 and with a t-test of the means for continuous characteristics. For parents, we also calculated frequencies for the sex, age, and number of health conditions in their youngest children.
Table 1. Characteristics of survey respondents.
| Respondent Characteristics | Weighted Estimates | ||
|---|---|---|---|
|
| |||
| Parents | Non-parents | Overall | |
| 30.4%, n=1539 | 69.6%, n=605 | 100% n=2144 | |
| Age in years, mean (range) ‡ | 38.8 (18-88) | 51.8 (18-94) | 47.8 (18-94) |
| 18-29, % (n) | 17.8(210) | 17.8(72) | 17.8(282) |
| 30-44, % (n) ‡ | 55.6 (872) | 14.7 (95) | 27.1 (967) |
| 45-59 , % (n) | 25.3 (433) | 30.1 (235) | 28.6 (668) |
| 60+, % (n) ‡ | 1.3 (24) | 37.4 (203) | 26.4 (227) |
| Race/ethnicity† | |||
| White (nonHispanic), % (n) ‡ | 62.9 (1,076) | 70.6 (447) | 68.2 (1,523) |
| Black (nonHispanic), % (n) | 11.4 (150) | 11.0 (64) | 11.2 (214) |
| Hispanic, % (n) ‡ | 18.0 (208) | 11.4 (62) | 13.4 (270) |
| Other (nonHispanic), % (n) | 7.7 (105) | 7.0 (32) | 7.2 (137) |
| Female, % (n) | 55.8 (820) | 50.8 (316) | 52.3 (1,136) |
| Education | |||
| High school diploma or less, % (n) | 37.7 (486) | 42.2 (244) | 30.8 (730) |
| Some college, % (n) | 29.4 (498) | 28.6 (170) | 28.8 (668) |
| Bachelor's or greater, % (n) | 32.9 (555) | 29.2 (191) | 30.4 (746) |
| Annual income | |||
| Less than $30,000, % (n) | 24.6 (287) | 29.3 (144) | 27.9 (431) |
| $30,000-$59,999, % (n) | 28.9 (418) | 26.7 (162) | 27.4 (580) |
| $60,000-$100,000, % (n) | 24.1 (421) | 23.7 (144) | 23.8 (565) |
| More than $100,000, % (n) | 22.4 (413) | 20.3 (155) | 20.9 (568) |
| Self-identified political ideology | |||
| Liberal, % (n) | 26.3 (350) | 30.9 (173) | 29.5 (523) |
| Moderate, % (n) | 39.3 (556) | 35.1 (204) | 36.4 (760) |
| Conservative, % (n) | 34.4 (564) | 34.0 (210) | 34.1 (774) |
| Respondent in good or better health, % (n)‡ | 89.0 (1407) | 81.9 (503) | 84.1 (1910) |
| Planning a child within 5 years, % (n) ‡ | 20.9 (265) | 11.2 (51) | 24.1 (316) |
|
| |||
| Child Characteristics | |||
|
| |||
| Female youngest child, % (n) | 47.7 (740) | N/A | N/A |
| Age of youngest child | |||
| <1 year old, % (n) | 7.1 (100) | N/A | N/A |
| 1-5 years old, % (n) | 34.2 (475) | N/A | N/A |
| 6-10 years old, % (n) | 25.2 (399) | N/A | N/A |
| 11-13 years old, % (n) | 12.9 (215) | N/A | N/A |
| 14-17 years old, % (n) | 20.6 (337) | N/A | N/A |
| Health of youngest child | |||
| 0 health conditions, % (n) | 64.8 (940) | N/A | N/A |
| 1 health conditions, % (n) | 23.5 (337) | N/A | N/A |
| 2+ health conditions, % (n) | 11.8 (175) | N/A | N/A |
All n values are unweighted.
Denotes p≤0.05 for parents vs non-parents;
denotes p≤0.01 for parents vs non-parents
Overall Adults’ Interest in WGS for Themselves
We tabulated the overall interest in WGS for each respondent. We then collapsed interest level into two categories (interested=definitely interested/somewhat interested vs. not interested=not interested/ definitely not interested) and tested the association between the two-category interest level in WGS and the respondent characteristics listed in Table 1. Age was tested with binary logistic regression while categorical variables were tested with Rao and Scott corrected Pearson's chi-square tests. Tests with a p-value of ≤0.2 were included in a multivariate logistic regression on respondent characteristics versus two-category interest level in WGS for oneself.
Parents’ Interest in WGS for Themselves and Their Youngest Children
We tabulated parents’ interest in WGS for themselves and for their youngest children, and compared individual responses to both questions. We found no effect of question order on response to either question using Rao and Scott corrected Pearson's chi-square analysis. For both questions, we then collapsed interest level into two categories as we did when analyzing adults. We compared two-category interest level in WGS for one's self and interest level in WGS for one's youngest child with an adjusted Wald test. We tested the association between two-category interest level and the characteristics of the respondent and youngest children listed in Table 1. Age of respondent was tested with binary logistic regression; all other characteristics were tested with Rao and Scott corrected Pearson's chi-square tests. Associations with p≤0.2 were included in a multivariate logistic regression analysis of respondent characteristics versus two-category interest level in WGS for oneself and two-category interest level in WGS for one's youngest child.
Results
Study Population
The survey response rates were 62% overall (parents and non-parents) and 55% among parents only. In Table 1 characteristics from the survey respondents are presented. The majority of respondents reported themselves to be white race, in good or better health, and not planning to have a child in the next five years. Education level, income, and political ideology were evenly distributed for parents and non-parents. Parents were more likely to be between ages 30-44, Hispanic, in at least good health, and planning to have a child in the next 5 years. Non-parents were more likely to be white and >60 years of age.
Two-thirds of the youngest children of respondents had no health conditions. The youngest children were evenly distributed between male and female and across the specified age categories.
Overall Interest in WGS Among U.S. Adults
Respondents were divided in their interest in having their whole genomes sequenced, with about 58.6% of those surveyed expressing at least some interest (Figure 1). In multivariate models of interest in WGS, significantly higher interest in WGS was observed among those planning to have a child in the next five years, Hispanics, and those with bachelor's degrees or higher education versus peers (Table 2), while the ideologically conservative expressed lower interest than ideological moderates. Age, sex, income, and health of the respondent were not significantly associated with population-level WGS interest.
Figure 1. Overall interest among U.S. adults in whole genome sequencing for themselves.

Table 2. Adjusted odds of adults’ interest in whole genome sequencing for themselves – United States, 2012.*.
| Characteristic | Adjusted OR (95% CI) | p |
|---|---|---|
| Age of respondent | 1.00 (0.99, 1.01) | 0.90 |
| Race/ethnicity | ||
| White (nonHispanic) | Reference | |
| Black (nonHispanic) | 1.41 (0.85, 2.34) | 0.18 |
| Hispanic | 1.82 (1.13, 2.94) | 0.01 |
| Other (nonHispanic) | 1.48 (0.79, 2.76) | 0.22 |
| Education | ||
| High school diploma or less | Reference | |
| Some college | 1.14 (0.79, 1.65) | 0.49 |
| Bachelor's or greater | 1.69 (1.15, 2.50) | 0.008 |
| Annual income | ||
| Less than $30,000 | Reference | |
| $30,000-$59,999 | 0.87 (0.58, 1.31) | 0.51 |
| $60,000-$ 100,000 | 0.94 (0.61, 1.46) | 0.80 |
| More than $100,000 | 1.41 (0.88, 2.26) | 0.15 |
| Self-identified political ideology | ||
| Liberal | 1.09 (0.75, 1.59) | 0.65 |
| Moderate | Reference | |
| Conservative | 0.53 (0.37, 0.75) | <.001 |
| Respondent in good or better health | 1.40 (0.88, 2.23) | 0.15 |
| Planning a child within 5 years | 2.01 (1.24, 3.28) | 0.005 |
| Being a Parent | 1.06 (0.78, 1.43) | 0.73 |
2037 observations. Sex of respondent had a crude p-value > 0.2 and was therefore not included in the regression
Parents’ Interest in WGS for Themselves and for Their Youngest Children
Parents expressed a similar level of interest in WGS for themselves and for their youngest children, with about 61.8% being at least somewhat interested in WGS for themselves, and 57.8% being interested in WGS for their youngest child (Figure 2). Furthermore, 84.7% of parents gave identical responses to the two questions. However, interest in WGS for their youngest children was slightly less than interest in WGS for themselves (Figure 2). The difference is statistically significant (adjusted Wald test F statistic of 0.0001).
Figure 2. Parent interest in whole genome sequencing for themselves (solid blue) and their youngest children (open).
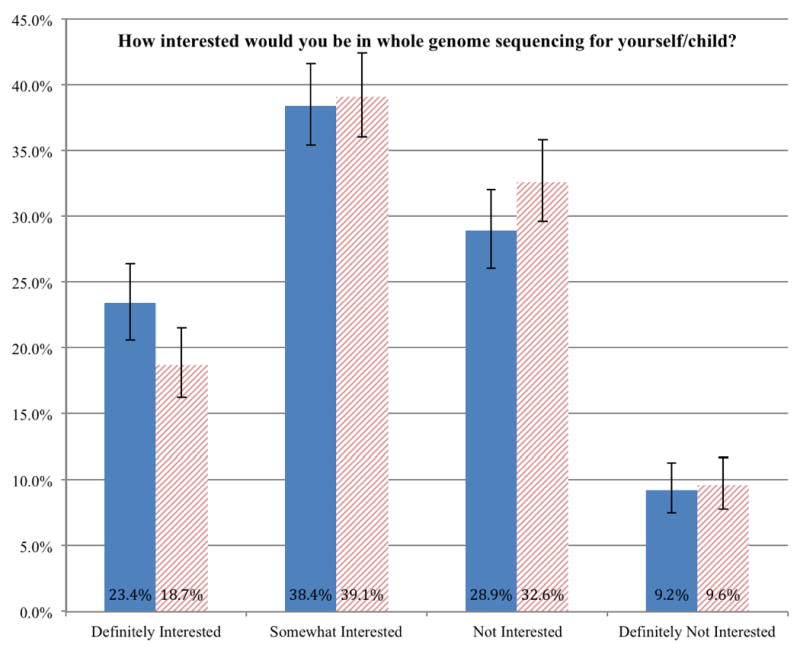
Higher levels of interest in WGS for self and youngest child were seen among women, respondents whose youngest children have 2 or more chronic conditions, and among those educated with bachelor's degrees or more (significant for self-testing only) (Table 3). Ideological conservatives expressed significantly less interest in WGS for both themselves and their youngest children than did ideological moderates. Age, race/ethnicity (including being African American), income, health of the respondent, plans to have a child within 5-years, gender of youngest child, and age of youngest child were not significantly associated with WGS interest for either self or for youngest child.
Table 3. Adjusted odds of parent interest in whole genome sequencing for themselves and their youngest children*.
| Interest in whole genome sequencing | For Self | For Youngest Child | ||
|---|---|---|---|---|
|
| ||||
| Characteristic | Adjusted OR (CI) | p | Adjusted OR (CI) | p |
| Female gender (respondent) | 1.54 (1.15, 2.07) | 0.003 | 1.68 (1.26, 2.24) | <0.001 |
| Education | ||||
| High school diploma or less | Reference | Reference | ||
| Some college | 1.22 (0.86, 1.77) | 0.26 | 1.19 (0.83, 1.71) | 0.33 |
| Bachelor's or greater | 1.58 (1.09, 2.29) | 0.02 | 1.28 (0.89, 1.84) | 0.18 |
| Self-identified political ideology | ||||
| Liberal | 1.13 (0.77, 1.66) | 0.52 | 1.09 (0.75, 1.58) | 0.65 |
| Moderate | Reference | Reference | ||
| Conservative | 0.59 (0.42, 0.82) | 0.002 | 0.58 (0.42, 0.81) | 0.001 |
| Respondent in good or better health | 0.73 (0.41, 1.30) | 0.29 | 0.82 (0.47, 1.42) | 0.3 |
| Planning a child within 5 years | 1.38 (0.92, 2.06) | 0.12 | 1.33 (0.89, 1.98) | 0.16 |
| Health of Youngest Child | ||||
| No health conditions | Reference | Reference | ||
| 1 health conditions | 0.99 (0.71, 1.39) | 0.96 | 1.05 (0.75, 1.47) | 0.77 |
| 2+ health conditions | 2.40 (1.45, 3.98) | 0.001 | 2.05 (1.23, 3.42) | 0.006 |
Discussion
Public Interest in WGS
We found that 60% of the U.S. adult population expressed at least some interest in WGS, a level consistent to what McGuire and colleagues 2009 study of interest in personal genome testing (e.g., single-nucleotide polymorphism array testing),17 and other studies probing interest in genetic testing found in a variety of contexts and populations.25-28 As WGS continues to become more widely available, within and outside the clinical setting (e.g., direct-to-consumer), more individuals may begin to express interest in these tests. The challenge will be for clinicians to convey the complexities of this testing (e.g., unanticipated and unrelated findings or results of uncertain clinical significance) to patients and their families in an understandable and meaningful way.
A main objective of our study was to compare parents’ interest in WGS for themselves with their interest in WGS for their youngest children. We found that parents expressed very similar levels of overall interest in WGS for themselves (61.8%) and their youngest children (57.8%), numbers similar to the McGuire et al study that did not specifically poll parents.3 This level of interest, as well as the fact that 84.7% of parents provided identical responses to both questions (a trend also reported by Tercyak et al with regards to PGT for newborn screening),18 suggests that interest in WGS is a decision made for the family. Parents who did not express interest in WGS may be uneasy about such a strong intrusion into their child's privacy, or may be more concerned than other parents about possible negative outcomes for their children. However, this similarity may be due to poor understanding of WGS, and being unable to differentiate between the two scenarios provided. The effect of more information, or informed consent, on interest level is a notable future area of study.
Factors Associated with Interest in WGS
We also found that parents whose youngest children had two or more medical conditions were significantly more likely to be at least somewhat interested in WGS, both for themselves and for their youngest child. This is consistent with patterns of interest related to newborn screening.18 Greater interest in WGS in households experiencing more childhood illness may be due to parents’ desire to find a reason – either in their own genes or in their children's genes – for those illnesses. This data is notable as WGS continues to grow in use for diagnostic purposes in children with unknown conditions.
We also identified a strong and consistent association between having a conservative ideology and a lower interest in WGS. Although political ideology has been linked to beliefs about healthcare policy (e.g., Patient Protection and Affordable Care Act, abortion, stem-cell research), to the best of our knowledge no literature describes a relationship between ideology and genetic testing issues. One study found that increased attendance at religious services correlated with more negative attitudes towards genetic testing,37 and another found a complex interplay between knowledge, religion, and attitudes towards genetic testing.38 We speculate that the patterns seen in this study and ours may be due to respondents’ association of genetic testing with perinatal genetic testing, pregnancy termination, and stem cell research.
Planning to have a child in the next 5 years was significantly associated with greater interest in WGS among adults overall, but was no longer significant when we focused our analysis on parents. Perhaps having one or more (most likely healthy) children puts parents’ minds at ease concerning their own genetic makeup, compared to new parents who lack this same experience. Finally, we also saw an association between respondents’ Hispanic ethnicity and interest in WGS (a complex pattern reported sporadically in previous literature),33,39 being educated and interest in WGS for oneself, and being a mother versus being a father and interest in WGS (consistent with a study by Tercyak et al).18 The reasons for these relationships are unclear and merit future study.
Notably, we did not find a significant association between race and WGS interest. A focus group study by Yu et al. suggests differences in interest in WGS between African Americans and non-African Americans, though the survey performed was non-random, and survey responses were public to the focus group.20 However, our results certainly do not mean that attitudes, or even interest, in WGS are the same between races. The study by Yu et al. suggests that African Americans have more distrust of medicine and are more community oriented than non-African Americans. The relationship between race and WGS continues to merit further investigation.
Study Limitations and Future Research
Our study has the following limitations. First, we acknowledge that the brief introduction of WGS we gave to respondents did not inform the study participants to the level that would occur in the clinical setting. However, we intended for our study to represent a baseline level of understanding that an average citizen would have when they walk into a clinic to speak with their clinician, or when considering the option to pursue WGS should it be available directly to consumers. This survey was not meant to assess public uptake of actual WGS after an extensive educational or consent process. Studies have found that people have an incomplete knowledge of genetics and genetic testing,37,40-43 and that when low-risk people are faced with the real-life decision to get tested and undergo preparatory genetic counseling, interest in WGS declines.41,44 However, in a real-world 15 minute clinic visit, time for true informed consent is limited, and many of the choices parents make will largely be dictated by their previously held beliefs, a phenomenon clinicians frequently encounter with vaccines. Therefore, we believe an understanding of the baseline reaction of the public to whole genome sequence adds significant value to our knowledge base.
Second, although the survey questions were trialed prior to our study, and were designed to be simple, the questions may have still been confusing to our audience. Third, our Likert scale categories of not interested and somewhat interested are not strict inverses, and may have biased responses towards interest. However, as mentioned in the discussion, our findings on interest in WGS were similar to other studies findings of interest in genetic testing. Furthermore, this should not affect the correlation of interest in WGS for one's self and one's child. Fourth, as with all survey data, non-response is a concern, but our response rate is consistent with other published nationally representative household surveys published from this survey platform.30,31 However, if one group of patients (e.g. those whose youngest child had a health condition) were more likely to respond to the survey, this might affect overall interest level. However, our bivariate analysis should be more robust to a possibly non-representative sample. Fifth, it is likely that there are other demographic and clinical characteristics associated with public and parent interest in WGS. However, our goal in this study was not to generate a fully explanatory model, but rather to generate a launch point for future inquiries. Finally, our study design did not permit us to probe the rationale behind respondents’ interest levels, nor to understand why certain respondent characteristics are associated with more or less interest in WGS. Further research is necessary to better elucidate these reasons, and by so doing to help clinicians better inform their patients about WGS.
Conclusion
As the cost and time necessary for WGS continues to decrease, WGS will presumably become more available, both as a clinical test and as a product offered in direct-to-consumer settings. Next generation sequencing remains a controversial issue, and the indications for testing, utility of testing, and what information should be captured with testing, continue to be hotly debated. Our study provides clinicians with a basic understanding of population and parent interest in WGS, highlighting the need to prepare for a potential increase in future requests they may receive from patients. These data also serve as a starting point for future inquiries into the reasons people have for their interest in WGS. These future studies should delve into the reasons behind the demographic associations we found to provide more informative data on the reasons behind people's attitudes, and thereby give clinicians, both generalists and specialists, data from which they can properly explain WGS to patients and parents, and ensure that their patients have the opportunity to make informed decisions about WGS for themselves and their children.
Acknowledgments
None of the authors have any conflicts of interest to disclose. This research was conducted as part of the CS Mott Children's Hospital National Poll on Children's Health (NPCH), www.MottNPCH.org. Funding for the NPCH is provided by the University of Michigan Health System and the Department of Pediatrics and Communicable Diseases.
Dr. Tarini was supported by the Clinical Sciences Scholars Program at the University of Michigan and a K23 Mentored Patient-Oriented Research Career Development Award from the National Institute for Child Health and Human Development (K23HD057994).
We would like to thank Amy Butchart, Anna Daly Kaufmann, and Sarah Clark for their thoughtful review of questions and editorial suggestions during development of the survey, and Achamyeleh Gebremariam for providing consultation about the statistical analysis.
Funding Source: Dr. Tarini is supported by a K23 Mentored Patient-Oriented Research Career Development Award from the National Institute for Child Health and Human Development (K23HD057994).
Abbreviations
- PGT
Personal genome testing
- WGS
whole genome sequencing
Appendix 1
Health conditions of youngest child. Respondents were asked to endorse all those listed that apply to their children.
| Conditions |
|---|
| Asthma |
| Attention deficit/hyperactivity |
| disorder(ADD/ADHD) |
| Behavioral disorders |
| Birth defects |
| Depression |
| Hearing problems |
| Heart problems |
| Lung disease from |
| prematurity |
| Overweight or obese |
| Seizures |
Footnotes
Financial Disclosure: The authors have no financial disclosures
Conflict of Interest: The views expressed herein do not necessarily represent those of the University of Michigan or Case Western Reserve University. The authors have no conflicts of interest to disclose.
References
- 1.Stone K. Genomic testing update: whole genome sequencing may be worth the money. Ann Neurol. 2012 May;71(5):A7–9. doi: 10.1002/ana.23609. [DOI] [PubMed] [Google Scholar]
- 2.Pareek CS, Smoczynski R, Tretyn A. Sequencing technologies and genome sequencing. J Appl Genet. 2011 Nov;52(4):413–435. doi: 10.1007/s13353-011-0057-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hayden EC. Technology: The $1,000 genome. Nature. 2014 Mar 20;507(7492):294–295. doi: 10.1038/507294a. [DOI] [PubMed] [Google Scholar]
- 4.Saunders CJ, Miller NA, Soden SE, et al. Rapid whole-genome sequencing for genetic disease diagnosis in neonatal intensive care units. Sci Transl Med. 2012 Oct 3;4(154):154–135. doi: 10.1126/scitranslmed.3004041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ashley Ea, Butte AJ, Wheeler MT, et al. Clinical assessment incorporating a personal genome. The Lancet. 2010;375:1525–1535. doi: 10.1016/S0140-6736(10)60452-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Privacy and Progress in Whole Genome Sequencing. Washington DC: Oct, 2012. Presidential Commission for the Study of Bioethical Issues. www.bioethics.gov. [Google Scholar]
- 7.Goldenberg AJ, Sharp RR. The ethical hazards and programmatic challenges of genomic newborn screening. JAMA. 2012 Feb 1;307(5):461–462. doi: 10.1001/jama.2012.68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bunnik EM, Schermer MH, Janssens AC. Personal genome testing: test characteristics to clarify the discourse on ethical, legal and societal issues. BMC Med Ethics. 2011;12:11. doi: 10.1186/1472-6939-12-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Evans JP, Berg JS. Next-generation DNA sequencing, regulation, and the limits of paternalism: the next challenge. JAMA. 2011 Dec 7;306(21):2376–2377. doi: 10.1001/jama.2011.1788. [DOI] [PubMed] [Google Scholar]
- 10.Wilcken B. Ethical issues in genetics. J Paediatr Child Health. 2011 Sep;47(9):668–671. doi: 10.1111/j.1440-1754.2011.02168.x. [DOI] [PubMed] [Google Scholar]
- 11.Levenseller BL, Soucier DJ, Miller VA, Harris D, Conway L, Bernhardt BA. Stakeholders' opinions on the implementation of pediatric whole exome sequencing: implications for informed consent. J Genet Couns. 2014 Aug;23(4):552–565. doi: 10.1007/s10897-013-9626-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Martin HC, Kim GE, Pagnamenta AT, et al. Clinical whole-genome sequencing in severe early-onset epilepsy reveals new genes and improves molecular diagnosis. Hum Mol Genet. 2014 Jun 15;23(12):3200–3211. doi: 10.1093/hmg/ddu030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Scollon S, Bergstrom K, Kerstein RA, et al. Obtaining informed consent for clinical tumor and germline exome sequencing of newly diagnosed childhood cancer patients. Genome Med. 2014;6(9):69. doi: 10.1186/s13073-014-0069-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Priest JR, Ceresnak SR, Dewey FE, et al. Molecular diagnosis of long QT syndrome at 10 days of life by rapid whole genome sequencing. Heart Rhythm. 2014 Oct;11(10):1707–1713. doi: 10.1016/j.hrthm.2014.06.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Roach JC, Glusman G, Smit AF, et al. Analysis of genetic inheritance in a family quartet by whole-genome sequencing. Science. 2010 Apr 30;328(5978):636–639. doi: 10.1126/science.1186802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Worthey EA, Mayer AN, Syverson GD, et al. Making a definitive diagnosis: successful clinical application of whole exome sequencing in a child with intractable inflammatory bowel disease. Genet Med. 2011 Mar;13(3):255–262. doi: 10.1097/GIM.0b013e3182088158. [DOI] [PubMed] [Google Scholar]
- 17.McGuire AL, Diaz CM, Wang T, Hilsenbeck SG. Social networkers' attitudes toward direct-to-consumer personal genome testing. Am J Bioeth. 2009;9(6-7):3–10. doi: 10.1080/15265160902928209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tercyak KP, Hensley Alford S, Emmons KM, Lipkus IM, Wilfond BS, McBride CM. Parents' attitudes toward pediatric genetic testing for common disease risk. Pediatrics. 2011 May;127(5):e1288–1295. doi: 10.1542/peds.2010-0938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sapp JC, Dong D, Stark C, et al. Parental attitudes, values, and beliefs toward the return of results from exome sequencing in children. Clin Genet. 2014 Feb;85(2):120–126. doi: 10.1111/cge.12254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yu JH, Crouch J, Jamal SM, Tabor HK, Bamshad MJ. Attitudes of African Americans toward return of results from exome and whole genome sequencing. Am J Med Genet A. 2013 May;161A(5):1064–1072. doi: 10.1002/ajmg.a.35914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Goldenberg AJ, Dodson DS, Davis MM, Tarini BA. Parents' interest in wholegenome sequencing of newborns. Genet Med. 2014 Jan;16(1):78–84. doi: 10.1038/gim.2013.76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stewart-Knox BJ, Bunting BP, Gilpin S, et al. Attitudes toward genetic testing and personalised nutrition in a representative sample of European consumers. Br J Nutr. 2009 Apr;101(7):982–989. doi: 10.1017/S0007114508055657. [DOI] [PubMed] [Google Scholar]
- 23.Makeeva OA, Markova VV, Puzyrev VP. Public interest and expectations concerning commercial genotyping and genetic risk assessment. Personalized Medicine. 2009;6(3):329–341. doi: 10.2217/pme.09.14. 2009/05/01. [DOI] [PubMed] [Google Scholar]
- 24.Cherkas LF, Harris JM, Levinson E, Spector TD, Prainsack B. A survey of UK public interest in internet-based personal genome testing. PLoS One. 2010;5(10):e13473. doi: 10.1371/journal.pone.0013473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Vermeulen E, Henneman L, van El CG, Cornel MC. Public attitudes towards preventive genomics and personal interest in genetic testing to prevent disease: a survey study. Eur J Public Health. 2014 Oct;24(5):768–775. doi: 10.1093/eurpub/ckt143. [DOI] [PubMed] [Google Scholar]
- 26.Vayena E, Ineichen C, Stoupka E, Hafen E. Playing a part in research? University students' attitudes to direct-to-consumer genomics. Public Health Genomics. 2014;17(3):158–168. doi: 10.1159/000360257. [DOI] [PubMed] [Google Scholar]
- 27.Amin TT, Al-Wadaani HA, Al-Quaimi MM, Aldairi NA, Alkhateeb JM, Al-Jaafari AA. Saudi women's interest in breast cancer gene testing: possible influence of awareness, perceived risk and socio-demographic factors. Asian Pac J Cancer Prev. 2012;13(8):3879–3887. doi: 10.7314/apjcp.2012.13.8.3879. [DOI] [PubMed] [Google Scholar]
- 28.Okayama M, Takeshima T, Ae R, Harada M, Kajii E. Primary care patient willingness for genetic testing for salt-sensitive hypertension: a cross sectional study. BMC Fam Pract. 2013;14:149. doi: 10.1186/1471-2296-14-149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hospital CSMCs. [August 06, 2012];National Poll on Children's Health. 2012 http://mottnpch.org/
- 30.Freed GL, Clark SJ, Butchart AT, Singer DC, Davis MM. Parental vaccine safety concerns in 2009. Pediatrics. 2010 Apr;125(4):654–659. doi: 10.1542/peds.2009-1962. [DOI] [PubMed] [Google Scholar]
- 31.Freed GL, Clark SJ, Butchart AT, Singer DC, Davis MM. Sources and perceived credibility of vaccine-safety information for parents. Pediatrics. 2011 May;127(Suppl 1):S107–112. doi: 10.1542/peds.2010-1722P. [DOI] [PubMed] [Google Scholar]
- 32.Tarini BA, Singer D, Clark SJ, Davis MM. Parents' concern about their own and their children's genetic disease risk: potential effects of family history vs genetic test results. Arch Pediatr Adolesc Med. 2008 Nov;162(11):1079–1083. doi: 10.1001/archpedi.162.11.1079. [DOI] [PubMed] [Google Scholar]
- 33.Tarini BA, Singer D, Clark SJ, Davis MM. Parents' interest in predictive genetic testing for their children when a disease has no treatment. Pediatrics. 2009 Sep;124(3):e432–438. doi: 10.1542/peds.2008-2389. [DOI] [PubMed] [Google Scholar]
- 34.Dennis JM. Summary of KnowledgePanel(R) Design. [Accessed May 15, 2011];2010 http://www.knowledgenetworks.com/ganp/reviewer-info.html.
- 35.Institute NHGR. A Brief Guide to Genomics. [Accessed 10/31/2014, 2014];2014 http://www.genome.gov/18016863.
- 36.Rao JNK, Scott AJ. On Chi-Squared Tests for Multiway Contingency Tables with Cell Proportions Estimated From Survey Data. The Annals of Statistics. 1984;12(1):46–60. [Google Scholar]
- 37.Botoseneanu A, Alexander JA, Banaszak-Holl J. To test or not to test? The role of attitudes, knowledge, and religious involvement among U.S. adults on intent-toobtain adult genetic testing. Health Educ Behav. 2011 Dec;38(6):617–628. doi: 10.1177/1090198110389711. [DOI] [PubMed] [Google Scholar]
- 38.Allum N, Sibley E, Sturgis P, Stoneman P. Religious beliefs, knowledge about science and attitudes towards medical genetics. Public Underst Sci. 2014 Oct;23(7):833–849. doi: 10.1177/0963662513492485. [DOI] [PubMed] [Google Scholar]
- 39.Singer E, Antonucci T, Van Hoewyk J. Racial and ethnic variations in knowledge and attitudes about genetic testing. Genet Test. 2004 Spring;8(1):31–43. doi: 10.1089/109065704323016012. [DOI] [PubMed] [Google Scholar]
- 40.Condit CM. Public attitudes and beliefs about genetics. Annu Rev Genomics Hum Genet. 2010 Sep 22;11:339–359. doi: 10.1146/annurev-genom-082509-141740. [DOI] [PubMed] [Google Scholar]
- 41.Green MJ, Peterson SK, Baker MW, et al. Effect of a computer-based decision aid on knowledge, perceptions, and intentions about genetic testing for breast cancer susceptibility: a randomized controlled trial. JAMA. 2004 Jul 28;292(4):442–452. doi: 10.1001/jama.292.4.442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Leighton JW, Valverde K, Bernhardt BA. The general public's understanding and perception of direct-to-consumer genetic test results. Public Health Genomics. 2012;15(1):11–21. doi: 10.1159/000327159. [DOI] [PubMed] [Google Scholar]
- 43.Haga SB, Barry WT, Mills R, et al. Public knowledge of and attitudes toward genetics and genetic testing. Genet Test Mol Biomarkers. 2013 Apr;17(4):327–335. doi: 10.1089/gtmb.2012.0350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Caulfield T, Wertz D. Creating needs? A review of survey data and concerns relevant to the commercialization of genetic testing. Community genetics. 2001;4(2):68–76. doi: 10.1159/000051160. [DOI] [PubMed] [Google Scholar]