

Abstract
Rare diseases are usually defined as entities affecting less than 1 person per 2,000. About 7,000 different rare entities are distinguished and, among them, rare diseases of the thyroid gland. Although not frequent, they can be found in the everyday practice of endocrinologists and should be considered in differential diagnosis. Rare non-neoplastic thyroid diseases will be discussed. Congenital hypothyroidism’s frequency is relatively high and its early treatment is of vital importance for neonatal psychomotor development; CH is caused primarily by thyroid dysgenesis (85%) or dyshormonogenesis (10-15%), although secondary defects - hypothalamic and pituitary - can also be found; up to 40% of cases diagnosed on neonatal screening are transient. Inherited abnormalities of thyroid hormone binding proteins (TBG, TBP and albumin) include alterations in their concentration or affinity for iodothyronines, this leads to laboratory test abnormalities, although usually with normal free hormones and clinical euthyroidism. Thyroid hormone resistance is most commonly found in THRB gene mutations and more rarely in THRA mutations; in some cases both genes are unchanged (non-TR RTH). Recently the term ‘reduced sensitivity to thyroid hormones’ was introduced, which encompass not only iodothyronine receptor defects but also their defective transmembrane transport or metabolism. Rare causes of hyperthyroidism are: activating mutations in TSHR or GNAS genes, pituitary adenomas, differentiated thyroid cancer or gestational trophoblastic disease; congenital hyperthyroidism cases are also seen, although less frequently than CH. Like other organs and tissues, the thyroid can be affected by different inflammatory and infectious processes, including tuberculosis and sarcoidosis. In most of the rare thyroid diseases genetic factors play a key role, many of them can be classified as monogenic disorders. Although there are still some limitations, progress has been made in our understanding of rare thyroid diseases etiopathogenesis, and, thanks to these studies, also in our understanding of how normal thyroid gland functions.
Keywords: Rare disease, Thyroid gland, Congenital hypothyroidism, Thyroxin binding globulin, Transthyretin, Thyroid hormone resistance, Dysgenesis, Dyshormonogenesis, Mutation
Introduction
Rare diseases are usually defined as entities affecting 5 or fewer per 10,000 (1 person per 2,000), although different thresholds can also be found, e.g. in Japan - fewer than 4 cases per 10,000 or in the United States - fewer than 200,000 patients affected across the country. Despite this rarity, the total number of a people with diagnosis of rare diseases is estimated at 350 million all over the world. Approximately 7,000 distinct rare entities are described, most of them genetically determined [1]. Another term - ultra-rare diseases - is usually referred to diseases that affect less than 1 person per 50,000 [2].
On the basis of prevalence, some thyroid gland diseases can also be classified as rare. They have genetic origin in most cases, often as a result of single gene mutations (monogenic disorders). Rare thyroid diseases should be considered in differential diagnosis of commonly seen thyroid entities, their right diagnosis may be often of vital importance. The aim of this review is therefore to briefly present the spectrum of rare thyroid diseases and underling etiopathogenesis. Rare thyroid diseases can be classified into two main categories: neoplastic and non-neoplastic disorders. Rare thyroid non-neoplastic entities will be discussed further in this paper.
Review
Congenital hypothyroidism
Congenital hypothyroidism (CH) can be classified as primary or secondary. The causes of primary CH are thyroid dysgenesis or dyshormonogenesis. Secondary CH may be: 1) hypothalamic (also called tertiary CH) – TRH gene mutations; 2) pituitary – congenital hypopituitarism with multihormonal insufficiency (some known mutations of transcription factors’ genes such as Pit 1, Prop 1, LHX 3, LHX 4, HESX1, but 80-90% of idiopathic origin) or isolated TSH deficiency (TSHB or rTRH genes mutations). Some cases of congenital thyroid hormones deficiency are transient (the percentage varies between studies, up to 40%) and euthyroidism is achieved within the first months or years of life (maternal antithyroid drug intake, maternal TSHR blocking antibodies, iodine deficiency or excess, some heterozygous mutations of DUOX2 and DUOXA2, congenital liver hemangioma) [3]. Lack of thyroid hormone action at birth may also result from peripheral causes (peripheral congenital hypothyroidism), which will be discussed in subsequent paragraphs.
The general prevalence of CH, regardless of its etiology, is 1:2,000 to 1:4,000 of neonates (primary CH - 1:4,000, secondary CH – 1:66,000) with a female-to-male ratio of 2:1. These values vary between different regions (1:800 in the Greek Cypriot population, 1:2,000 in China, 1:2,300 in the US and 1:10,000 in France) or ethnic groups (highest prevalence in Asians) [3-5]. In Poland it is estimated that CH affects about 1:4,500 of all screened neonates [6]. In iodine sufficient regions, the vast majority of CH cases are caused by thyroid dysgenesis (up to 85%) and dyshormonogenesis (10-15%), while secondary CH is responsible for only 0.0015% of all cases [7]. The genes involved in CH etiopathogenesis are presented in Figure 1.
Figure 1.
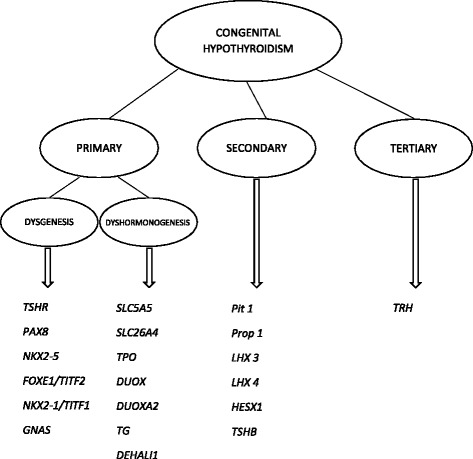
Genetic background of congenital hypothyroidism.
Dysgenesis
The term thyroid dysgenesis includes the ectopic location of the gland (thyroid ectopy), absence (athyreosis) and underdevelopment of the thyroid tissue (hypoplasia). Unilateral thyroid agenesis (hemiagenesis) is also classified as thyroid dysgenesis, although usually with clinical euthyroidism [8]. Within the group of thyroid dysgenesis, ectopy is found most commonly, with lingual, supra- and infrahyoid localization of the gland most frequently seen. Cases of thyroid dysgenesis are usually sporadic, inherited genetic defects are only recognized in about 2% of all cases and result from transcription factor genes mutations (PAX8, NKX2-1/TITF1, NXK2-5, FOXE1/TITF-2) [9]. As these transcription factors are also involved in extrathyroid development, different organs’ congenital anomalies may coexist (Table 1). The thyroid gland is the only organ affected by TSHR gene (14q31.1) mutations, which account for about 1% of all CH cases. As more than 60 different TSHR loss-of-function mutations have been found (Y444X described for the first time in the Polish population), a variable degree of TSH resistance and ongoing clinical presentation are observed (from euthyroid hyperthyrotropinemia to hypoplasia with severe hypothyroidism) [10,11]. TSH resistance is also observed in mutations of GNAS gene (20q13.32), encoding the alpha subunit of G protein, downstream of TSH receptor in the signaling pathway. As G protein is also responsible for signal transduction of other peptide hormones, in these cases resistance is multihormonal and the clinical picture is complex (pseudohypoparathyroidism type 1a) [12]. The role of environmental factors (e.g. intrauterine viral infections) in thyroid dysgenesis is also suggested [13].
Table 1.
Transcription factor genes responsible for thyroid dysgenesis
| Gene | Locus | Type of inheritance | Expression | Clinical manifestation |
|---|---|---|---|---|
| PAX8 | 2q13 | AD | Thyroid, kidney, CNS | Thyroid hypoplasia or athyreosis, agenesis/hemiagenesis of the kidneys |
| NKX2-5 | 5q35.1 | AD | Thyroid, heart, pharynx | Thyroid ectopy, athyreosis, congenital cardiac malformations |
| FOXE1/TITF2 | 9q22.33 | AR | Thyroid, pituitar, tongue, epiglottis, palate, pharynx, thymus and Rathke’s pouch, choanae, hair follicles | Athyreosis, other forms of thyroid dysgenesis, cleft palate, cleft epiglottis, choanal atresia, spiky hair |
| NKX2-1/TITF1 | 14q13.3 | AD | Thyroid, lung, trachea, CNS | Thyroid dysgenesis, dyshormonogenesis due to inhibited TG expression, choreoatetosis, hypotony, respiratory distress |
Dyshormonogenesis
Another reason for primary CH – dyshormonogenesis – arises from defective thyroid hormone synthesis; all its stages may be affected (Figure 2). These monogenic defects are inherited predominantly with an autosomal recessive pattern. Clinically, in addition to the symptoms and signs of thyroid hormone deficiency (rarely euthyroidism), patients may present with goiter.
Figure 2.
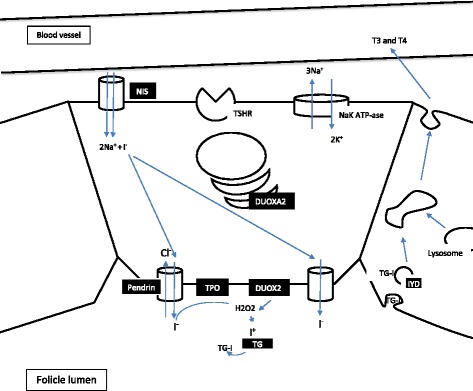
Thyroid hormone biosynthesis (possible genetic defect sites shown in black).
Mutations in the SLC5A5 gene (19p13.11) encoding sodium-iodide symporter (NIS) result in a defect in the active transport of iodide to thyrocytes. NIS glycoprotein is expressed not only in the thyroid follicular cells, but also in some non-thyroid tissues – salivary and lacrimal glands, cancerous breast tissue, the breast during lactation, the intestines, stomach, testes and placenta. To data, at least 12 different loss-of-function mutations in the NIS gene have been described [14]. This relatively rare cause of dyshormonogenesis is characterized by an autosomal recessive pattern of inheritance. Diminished or completely inhibited iodine uptake by the thyroid is characteristic.
Pendrin, encoded by SLC26A4 gene (7q22.3), is an anion transporter expressed primarily in the thyroid (allows iodide efflux into the follicular lumen) but also in the inner ear, kidneys and lungs. Bi-allelic mutations of the SLC26A4 gene (about 470 mutations described to date) lead mainly to two different phenotypes: a) non-syndromic hearing loos with enlarged vestibular aqueduct (EVA) or b) Pendred syndrome (PDS) with congenital bilateral sensorineural hearing loss and thyroid defect (diffuse or multinodular goiter, thyroid hormone status is dependent on iodide intake, with dominance of euthyroidism in iodide sufficient regions) [15-17]. PDS is a rare cause of CH (2-3%), goiter often occurs later, in childhood or early adolescence. Patients with PDS are at increased risk of thyroid cancer development (about 1%), most likely follicular carcinoma [18].
Thyroid peroxidase (TPO) catalyze iodide oxidation, tyrosyl residue iodination and their coupling to iodothyronines [19]. TPO (2p25.3) mutation is considered to be the most prevalent cause of dyshormonogenesis (24-46%), and is found in about 1:60,000 newborns, with about 90 different mutations already described [15,20]. The disease is generally inherited with an autosomal recessive manner, although monoallelic mutations may be a risk factor for transient hypothyroidism.
In the process of iodothyronine synthesis, H2O2 is required, which is produced by the dual oxidase enzyme (DUOX/ThOX). Two variants of DUOX can be distinguished, with type 2 being critical for thyroid hormone synthesis [21]. In the case of DUOX2 (15q21.1), autosomal dominant mode of inheritance is observed, although homozygotes are usually affected more severely. Patients with mono-allelic mutations typically present with transient congenital hypothyroidism, but should be monitored in adulthood in situations characterized by an increased thyroid hormone requirement, such as pregnancy [22]. Defects in another thyroid protein - DUOXA2 (15q21.1), which is indispensable for DUOX2 maturation and translocation, can also cause CH [23].
Thyroglobulin (TG) is essential in thyroid hormone synthesis as it provides tyrosyl residues and enable the storage of hormones and iodine. Since it was first described, more than 50 different mutations that lead to CH have been found [24]. TG (8q24.22) mutations are described as one of the most prevalent causes of dyshormonogenesis ( 1:67,000 to 1:100,000) [24,25]. A characteristically undetectable or very low TG level is observed in these patients, T4 concentration is found to be disproportionately lower than T3 (a result of increased type-2 iodothyronine deiodinase activity) [26].
Although the end products of hormonogenesis are T3 and T4, most iodine particles are embedded to mono- and diiodotyronines (MIT, DIT). Reuse of this iodine is possible due to MIT and DIT deiodination by an iodotyrosine deiodinase (IYD). Mutations in the IYD gene (6q25.1) may lead to goitrous hypothyroidism [27]. A characteristic feature is excessive urinary and blood MIT and DIT concentrations [28].
Inherited thyroid hormone binding protein abnormalities
TBG
Thyroxin binding globulin (TBG) is the main protein that binds T3 and T4 in the blood (70% and 70-80% respectively); other transporting particles (transthyretin and albumin) play a minor role. TBG is encoded by the Serpina 7 gene (Xq22.3) and expressed in the liver [29]. Three different congenital TBG abnormalities are distinguished according to its concentration: complete deficiency (TBG-CD), partial deficiency (TBG-PD) and excess (TBG-E). They are inherited in a X-linked recessive pattern (although a case of autosomal dominant inheritance of TBG-PD has been described) [30]. There are also some TBG polymorphic variants that do not alter the protein concentration.
TBG-CD is diagnosed when the protein level is undetectable by typically used assays (or is lower than 0.03% of the normal mean value), and can be found in hemizygous men and homozygous women. Heterozygous women usually have only a slightly diminished TBG concentration (carriers), although rarely, as a result of selective X chromosome inactivation, TBG-CD may develop [31]. Men with TBG-PD have a significantly decreased serum concentration of globulin, while women are found to have values that may even overlap the normal range. TBG deficiency is estimated to occur in 1:15,000 to 1:5,000 of all newborns in the Caucasian population (there is a higher frequency in the Japanese population), with TBG-CD in one-third of them [32]. At least 22 different TBG-CD and 8 TBG-PD mutations have been described (TBG-CD mutations shown on Figure 3) [33]. Laboratory tests in these generally euthyroid patients show normal TSH, fT3 and fT4 with a low T4, T3 and undetectable TBG level.
Figure 3.
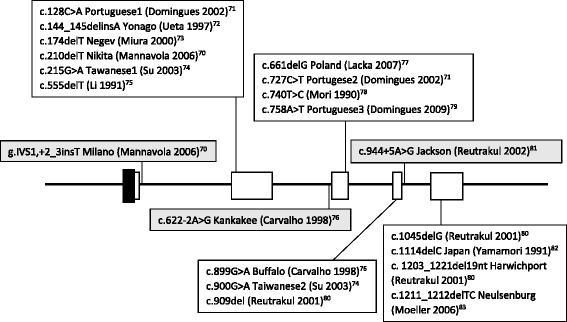
Mutations responsible for TBG-CD (mutations in coding regions shown in white boxes, mutations in non-coding regions shown in grey boxes) [ 70-83 ].
Excessive TBG concentration is typically observed in the course of elevated estrogen level (e.g. pregnancy). Congenital TBG-E occurs rarely, as a consequence of gene duplication or triplication (in 1:6,000 to 1:40,000 of all newborns) [34]. In such cases, the values measured are 2–3 times higher than normal in men and mildly elevated in heterozygous women [35].
TTR
About 20% of T4 and 10-20% of T3 is bound in serum by transthyretin (TTR)/thyroxine binding prealbumin (TBPA), a homotetrameric protein synthetized in the liver. Over 120 different disease-associated mutations have been found in TTR gene (18q12.1), with variable manifestation. Most commonly they lead to amyloid deposition in the cardiac tissue and/or peripheral nerves, without affecting the status of thyroid hormones [15,36]. There is also a group of mutations that lead to a considerably increased affinity for iodothyronines (predominantly T4) and may result in euthyroid dysprealbuminemic hyperthyroxinemia with an elevated serum total T4, rT3 and fT4 index (TSH, fT4, T3 and fT3 unaffected) [37]. Dysprealbuminemic hyperthyroxinemia is transmitted in an autosomal dominant manner and accounts for approximately 2% of all euthyroid hyperthyroxinemia cases [38]. Mutations associated with an increased concentration of TTR do not cause euthyroid hyperthyroxinemia, as an observed augmentation in the protein level is not high enough (although in the course of some malignancies e.g. hepatocellular carcinoma, the TTR concentration may increase significantly and bring about the picture of euthyroid hyperthyroxinemia) [39]. Some of the TTR mutations lead to a decrease in protein blood concentration or a lesser affinity for iodothyronines, although without significant clinical or laboratory changes in thyroid hormones status.
Albumin
Familial dysalbuminemic hyperthyroxinemia (FDH) is another cause of inherited euthyroid hyperthyroxinemia. It results from albumin gene (4q13.3) mutations that lead to an increased affinity for fT4 and is inherited as an autosomal dominant disease. Although relatively rare, FDH is the most prevalent cause of inherited euthyroid hyperthyroxinemia in the Caucasian population (up to 12% of all cases, from 1:10,000 to 17:10,000) [40,41]. The following values are expected in laboratory tests: normal TSH (also after TRH stimulation) fT4, fT3, normal or slightly elevated T3, elevated T4, rT3 (in some cases) and an increased proportion of T4 bound to serum albumin (approximately four times higher than normally) [42]. The diagnostic problem may be falsely elevated fT4, as the laboratory techniques usually used are not accurate enough in that case, which may lead to unnecessary treatment [43]. In most cases, mutations at position 218 of the amino acid chain are present. However, another one was found in codon 66 (L66P) and leads to an increased affinity for fT3 and hypertriiodothyroninemia (FDH-T3) [44].
Thyroid hormone resistance (RTH)
Thyroid hormones act primarily via nuclear receptors (TR): 1) TRα1 encoded by THRA (17q21.1) and 2) TRβ1 or TRβ2 encoded by THRB (3p24.2 ) (different expression pattern of both subtypes). T3 forms a complex with TR, and subsequently binds to the promoter region of the target genes (thyroid hormone response elements), acting as a transcription factor.
Mutations in TR genes lead to thyroid hormone resistance (RTH), disorder transmitted in the majority of cases in an autosomal dominant manner. Although no precise data are available, the prevalence is estimated to be 1:40,000 newborns [45]. In approximately 85-90% of RTH cases, the disease is caused by THRB mutations that lead to a decreased affinity for T3 or impaired interactions with TRβ cofactors. In these cases, elevated fT4 (often also fT3 and rT3) associated with normal or elevated (non-suppressed) TSH level is observed [46]. As a consequence of the variable manifestations observed among patients, RTH was formerly classified into generalized, isolated peripheral and isolated pituitary resistance. Often some evidence of both hyper- and hypothyroidism can be found in one patient (goiter, sinus tachycardia etc. may be associated with learning disabilities and delayed growth or bone age). In rare cases of homozygous THRB mutations, more severe symptoms are observed with coexisting deaf-mutism and color blindness [47].
Mutations in THRA were also described, which lead to different symptoms and thyroid function test results than in THRB defects. The symptoms of thyroid hormone deficiency are restricted to those tissues in which TRα predominates (central nervous system, myocardium, striated muscles, the gastrointestinal tract, cartilages and bones) [48]. Laboratory tests show a decreased fT4, very low rT3 and elevated fT3.
In a group of RTH patients (up to 15%), neither THRB nor THRA gene mutations were found (non TR-RTH), although phenotypically they may be indistinguishable from those with TRβ alterations. This subtype is also inherited in an autosomal dominant manner and expected to result from some TRβ cofactors mutations or defects in receptor regulation, although undefined to date [49].
Recently, the term ‘reduced sensitivity to thyroid hormones’ (RSTH) was introduced, which encompasses RTH and decreased responsiveness to thyroid hormones caused by iodothyronine transmembrane transport defect (mutations of MCT8 gene - SLC16A2 in Xq13.2) or T4 to T3 deiodination defect (mutations of SBP2 gene - SECISBP2 in 9q22.2) [50-52].
Rare causes of hyperthyroidism
Congenital hyperthyroidism, a generally rare disease (overt hyperthyroidism in 1:50,000 newborns), is most often transient and caused by the maternal thyroid stimulating antibodies in the course of Graves’ disease, subsequently transferred to fetal circulation (hyperthyroidism in 0.6-1% of offspring born to GD mothers) [53]. However, in some neonates there are no thyroid antibodies in serum, the mother’s disease is excluded and hyperthyroidism is persistent. This may suggest a condition called non-autoimmune hyperthyroidism (NAH). NAH develops as a result of gain-of-function germline mutation within the TSH receptor gene (TSHR), leading to constitutive TSHR pathway activation. It can be divided into sporadic (SNAH) and familial (FNAH) with an autosomal dominant mode of inheritance [54,55]. To date, at least 21 different mutations of TSHR in FNAH and 12 in SNAH have been found. Similar mutations, but of a somatic type, can be found in toxic thyroid nodules [56]. Clinically, patients with NAH usually present with goiter and hyperthyroidism. Moreover, pharmacologic treatment may be ineffective (frequent relapses are observed) and total thyroidectomy or complete radioiodine ablation is usually necessary.
Hyperthyroidism is also observed in patients with McCune-Albright syndrome (MAS), as a result of the activating somatic mutation of the GNAS gene. As mentioned previously, GSα is a part of the TSHR signaling cascade and its constitutive activation is followed by a cAMP increase, which in turn results in thyrocyte hyperproliferation and iodothyronine excess. GSα is committed to extracellular signals transduction in different tissues as well. As GNAS mutations occur in MAS in the post-zygotic period and patients are mosaic, variable manifestations are observed. The classical triad of symptoms include bone fibrous dysplasia, café-au-lait spots and hyperfunctional endocrinopathies (most frequently peripheral precocious puberty, but also hyperthyroidism, hypercortisolism, hypophyseal hyperfunction and kidney phosphate wasting). MAS prevalence range from 1:100,000 to 1:1,000,000 [57], with functional or morphological changes in the thyroid in approximately 31% of cases [58].
Symptoms of hyperthyroidism may also be observed, albeit rarely, in the course of struma ovari (5-15% of cases), differentiated thyroid cancer (usually methastatic) and an gestational trophoblastic disease [59-61]. Furthermore, central (secondary) hyperthyroidism due to TSH secreting pituitary adenoma can be classified as a rare disease as it accounts for only about 1% of all pituitary adenomas (prevalence of 1:1,000,000) [62].
Rare thyroid inflammatory diseases
Thyroid gland tuberculosis is very rarely observed in the course of generalized disease (even in regions with a relatively high incidence of tuberculosis) and much less frequently as a change isolated or primarily localized in the thyroid. Analyses of surgically removed glands or fine needle aspiration biopsy (FNAB) materials showed a prevalence of 0.1-0.6% [63,64]. Thyroid tuberculosis may present as a single nodule, multinodular goiter or diffused swelling, it may be found as a cold abscess or rarely an acute abscess [65]. Some patients remain symptomless, while others develop dyspnea, dysphagia, hoarseness, pain or tenderness. Typically, the hormonal status of the thyroid gland is unaffected, although hyperthyroidism may occur in some cases, as a result of excessive release of thyroid hormones from damaged tissue. Hypothyroidism, which is extremely rarely observed, may be caused by extensive tissue destruction [66]. To establish the diagnosis, ultrasound-guided FNAB should be performed with Ziehl Neelsen staining, culture and cytological examination (caseating granulomas with epithelioid cells and Langhans giant cells).
Sarcoidosis - a noncaseating granulomatous disorder, may rarely affect the thyroid gland in the course of generalized disease. Usually, extrathyroidal manifestation of the disease precedes the diagnosis of thyroid involvement. Some rare cases of sarcoidosis limited to the thyroid gland can be also found in the literature [67]. In post-mortem studies of patients with previously found systemic sarcoidosis, the thyroid gland was affected in up to 4.5% [68]. Thyroid sarcoidosis usually presents as a progressive painless enlargement of the gland with unaffected hormonal status, although different manifestations are possible (hyperthyroidism, hypothyroidism, acute thyroiditis, multinodular goiter or solitary thyroid nodule, it may sometimes be painful). Cases of hyperthyroidism resistant to both pharmacological and radioiodine treatment were observed in the course of thyroid sarcoidosis, and in these cases surgical removal of the gland is required. Studies also suggest an increased prevalence of high antithyroid antibodies concentration and thyroid autoimmune diseases associated with sarcoidosis, regardless of thyroid gland involvement (an ATD frequency in patients with sarcoidosis 1.9-16,6%) [69].
Conclusions
Most of the rare thyroid diseases presented in this paper have a genetic origin, among them monogenic disorders can be found. Progress in our understanding of their etiology and pathogenesis has been observed in the past years, what also shed new light on how the normal thyroid gland functions and the role of different proteins in this process, although there are still some questions that need answers. Secondly, rare thyroid diseases may be a challenging problem for clinicians because of their rarity and variability in manifestations. They should be kept in mind as a differential diagnosis of other diseases more commonly seen in clinical practice. A correct and undelayed diagnosis is especially important in the case of congenital thyroid function disruptions, as untreated, they may lead to serious consequences.
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contribution
KL designed the study, wrote the manuscript and supervised preparation of the final version of the manuscript. AM was involved in literature review and drafting the manuscript. All authors read and approved the final manuscript.
Contributor Information
Katarzyna Lacka, Email: kktlacka@gmail.com.
Adam Maciejewski, Email: amaciejewski3@gmail.com.
References
- 1.Posada de la Paz M, Villaverde-Hueso A, Alonso V, János S, Zurriaga O, Pollán M, et al. Rare diseases epidemiology research. In: Posada de la Paz M, Groft SC, et al., editors. Rare diseases epidemiology. London, New York: Springer Dordrecht Heidelberg; 2010. pp. 17–40. [DOI] [PubMed] [Google Scholar]
- 2.Hennekam RC. Care for patients with ultra-rare disorders. Eur J Med Genet. 2011;54(3):220–4. doi: 10.1016/j.ejmg.2010.12.001. [DOI] [PubMed] [Google Scholar]
- 3.Rastogi MV, LaFranchi SH. Congenital hypothyroidism. Orphanet J Rare Dis. 2010;5:17. doi: 10.1186/1750-1172-5-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Harris KB. Pass KA Increase in congenital hypothyroidism in New York State and in the United States. Mol Genet Metab. 2007;91:268–77. doi: 10.1016/j.ymgme.2007.03.012. [DOI] [PubMed] [Google Scholar]
- 5.Zhan JY, Qin YF, Zhao ZY. Neonatal screening for congenital hypothyroidism and phenylketonuria in China. World J Pediatr. 2009;5(2):136–9. doi: 10.1007/s12519-009-0027-0. [DOI] [PubMed] [Google Scholar]
- 6.Kumorowicz-Czoch M, Tylek-Lemanska D, Starzyk J. Thyroid dysfunctions in children detected in mass screening for congenital hypothyroidism. J Pediatr Endocrinol Metab. 2011;24(3–4):141–5. doi: 10.1515/jpem.2011.080. [DOI] [PubMed] [Google Scholar]
- 7.Brown RS, Demmer LA. The etiology of thyroid dysgenesis-still an enigma after all these years. J Clin Endocrinol Metab. 2002;87(9):4069–71. doi: 10.1210/jc.2002-021092. [DOI] [PubMed] [Google Scholar]
- 8.Ruchala M, Szczepanek E, Szaflarski W, et al. Increased risk of thyroid pathology in patients with thyroid hemiagenesis: results of a large cohort case–control study. Eur J Endocrinol. 2010;162(1):153–60. doi: 10.1530/EJE-09-0590. [DOI] [PubMed] [Google Scholar]
- 9.Kirmızibekmez H, Güven A, Yildiz M, Cebeci AN, Dursun F. Developmental defects of the thyroid gland: relationship with advanced maternal age. J Clin Res Pediatr Endocrinol. 2012;4(2):72–5. doi: 10.4274/Jcrpe.560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jeziorowska A, Pniewska-Siark B, Brzeziańska E, Pastuszak-Lewandoska D, Lewiński A. A novel mutation in the thyrotropin (thyroid-stimulating hormone) receptor gene in a case of congenital hypothyroidism. Thyroid. 2006;16(12):1303–9. doi: 10.1089/thy.2006.16.1303. [DOI] [PubMed] [Google Scholar]
- 11.Cassio A, Nicoletti A, Rizzello A, Zazzetta E, Bal M, Baldazzi L. Current loss-of-function mutations in the thyrotropin receptor gene: when to investigate, clinical effects, and treatment. J Clin Res Pediatr Endocrinol. 2013;5:29–39. doi: 10.4274/Jcrpe.864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Persani L, Calebiro D, Cordella D, Weber G, Gelmini G, Libri D, et al. Genetics and phenomics of hypothyroidism due to TSH resistance. Mol Cell Endocrinol. 2010;322(1–2):72–82. doi: 10.1016/j.mce.2010.01.008. [DOI] [PubMed] [Google Scholar]
- 13.Miyai K, Inaoka K, Miyagi T. Further studies on episodic occurrence of congenital dysgenetic hypothyroidism in Osaka, Japan. Endocr J. 2005;52(5):599–603. doi: 10.1507/endocrj.52.599. [DOI] [PubMed] [Google Scholar]
- 14.Spitzweg C, Morris JC. Genetics and phenomics of hypothyroidism and goiter due to NIS mutations. Mol Cell Endocrinol. 2010;322(1–2):56–63. doi: 10.1016/j.mce.2010.02.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.The Human Gene Mutation Database . Cardiff University. 2015. [Google Scholar]
- 16.Maciaszczyk K, Lewiński A. Phenotypes of SLC26A4 gene mutations: Pendred syndrome and hypoacusis with enlarged vestibular aqueduct. Neuro Endocrinol Lett. 2008;29(1):29–36. [PubMed] [Google Scholar]
- 17.Kopp P. Mutations in the Pendred Syndrome (PDS/SLC26A) gene: an increasingly complex phenotypic spectrum from goiter to thyroid hypoplasia. J Clin Endocrinol Metab. 2014;99(1):67–9. doi: 10.1210/jc.2013-4319. [DOI] [PubMed] [Google Scholar]
- 18.Nose V. Thyroid cancer of follicular cell origin in inherited tumor syndromes. Adv Anat Pathol. 2010;17:428–36. doi: 10.1097/PAP.0b013e3181f8b028. [DOI] [PubMed] [Google Scholar]
- 19.Kimura S, Kotani T, McBride OW, Umeki K, Hirai K, Nakayama T, et al. Human thyroid peroxidase: complete cDNA and protein sequence, chromosome mapping, and identification of two alternately spliced mRNAs. Proc Natl Acad Sci USA. 1987;84:5555–9. doi: 10.1073/pnas.84.16.5555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Avbelj M, Tahirovic H, Debeljak M, Kusekova M, Toromanovic A, Krzisnik C, et al. High prevalence of thyroid peroxidase gene mutations in patients with thyroid dyshormonogenesis. Eur J Endocrinol. 2007;156(5):511–9. doi: 10.1530/EJE-07-0037. [DOI] [PubMed] [Google Scholar]
- 21.Moreno JC, Bikker H, Kempers MJ, van Trotsenburg AS, Baas F, de Vijlder JJ, et al. Inactivating mutations in the gene for thyroid oxidase 2 (THOX2) and congenital hypothyroidism. N Engl J Med. 2002;347(2):95–102. doi: 10.1056/NEJMoa012752. [DOI] [PubMed] [Google Scholar]
- 22.Alexander EK, Marqusee E, Lawrence J, Jarolim P, Fischer GA, Larsen PR. Timing and magnitude of increases in levothyroxine requirements during pregnancy in women with hypothyroidism. N Engl J Med. 2004;351:241–9. doi: 10.1056/NEJMoa040079. [DOI] [PubMed] [Google Scholar]
- 23.Grasberger H, Refetoff S. Identification of the maturation factor for dual oxidase. Evolution of an eukaryotic operon equivalent. J Biol Chem. 2006;281:18269–72. doi: 10.1074/jbc.C600095200. [DOI] [PubMed] [Google Scholar]
- 24.Targovnik HM, Esperante SA, Rivolta CM. Genetics and phenomics of hypothyroidism and goiter due to thyroglobulin mutations. Mol Cell Endocrinol. 2010;322(1–2):44–55. doi: 10.1016/j.mce.2010.01.009. [DOI] [PubMed] [Google Scholar]
- 25.Hishinuma A, Fukata S, Nishiyama S, Nishi Y, Oh-Ishi M, Murata Y, et al. Haplotype analysis reveals founder effects of thyroglobulin gene mutations C1058R and C1977S in Japan. J Clin Endocrinol Metab. 2006;91:3100–4. doi: 10.1210/jc.2005-2702. [DOI] [PubMed] [Google Scholar]
- 26.Kanou Y, Hishinuma A, Tsunekawa K, Seki K, Mizuno Y, Fujisawa H, et al. Thyroglobulin gene mutations producing defective intracellular transport of thyroglobulin are associated with increased thyroidal type 2 iodothyronine deiodinase activity. J Clin Endocrinol Metab. 2007;92:1451–7. doi: 10.1210/jc.2006-1242. [DOI] [PubMed] [Google Scholar]
- 27.Moreno JC, Klootwijk W, van Toor H, Moreno JC, Klootwijk W, van Toor H, et al. Mutations in the iodotyrosine deiodinase gene and hypothyroidism. N Engl J Med. 2008;358:1811–8. doi: 10.1056/NEJMoa0706819. [DOI] [PubMed] [Google Scholar]
- 28.Afink G, Kulik W, Overmars H, de Randamie J, Veenboer T, van Cruchten A, et al. Molecular characterization of iodotyrosine dehalogenase deficiency in patients with hypothyroidism. J Clin Endocrinol Metab. 2008;93:4894–901. doi: 10.1210/jc.2008-0865. [DOI] [PubMed] [Google Scholar]
- 29.Hayashi Y, Mori Y, Janssen OE, Sunthornthepvarakul T, Weiss RE, Takeda K, et al. Human thyroxine-binding globulin gene: complete sequence and transcriptional regulation. Mol Endocrinol. 1993;7:1049–60. doi: 10.1210/mend.7.8.8232304. [DOI] [PubMed] [Google Scholar]
- 30.Kobayashi H, Sakurai A, Katai M, Hashizume K. Autosomally transmitted low concentration of thyroxine-binding globulin. Thyroid. 1999;9:159–63. doi: 10.1089/thy.1999.9.159. [DOI] [PubMed] [Google Scholar]
- 31.Okamoto H, Mori Y, Tani Y, Nakagomi Y, Sano T, Ohyama K, et al. Molecular analysis of females manifesting thyroxine-binding globulin (TBG) deficiency: selective X-chromosome inactivation responsible for the difference between phenotype and genotype in TBG-deficient females. J Clin Endocrinol Metab. 1996;81(6):2204–8. doi: 10.1210/jcem.81.6.8964852. [DOI] [PubMed] [Google Scholar]
- 32.Mandel S, Hanna C, Boston B, Sesser D, LaFranchi S. Thyroxine-binding globulin deficiency detected by newborn screening. J Pediatr. 1993;122:227–30. doi: 10.1016/S0022-3476(06)80117-4. [DOI] [PubMed] [Google Scholar]
- 33.Refetoff S. Abnormal thyroid hormone transport. In: Thyroid Disease Manager. South Dartmouth, Massachusetts: Endocrine Education; 2012. http://www.thyroidmanager.org/chapter/abnormal-thyroid-hormone-transport/. Accesed 10.02.2015.
- 34.Griffiths KD, Virdi NK, Rayner PHW, Green A. Neonatal screening for congenital hypothyroidism by measurement of plasma thyroxine and thyroid stimulating hormone concentrations. Brit Med J. 1985;291:117–20. doi: 10.1136/bmj.291.6488.117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Mori Y, Seino S, Takeda K, Flink IL, Murata Y, Bell GI, et al. A mutation causing reduced biological activity and stability of thyroxine-binding globulin probably as a result of abnormal glycosylation of the molecule. Mol Endocrinol. 1989;3:575–9. doi: 10.1210/mend-3-3-575. [DOI] [PubMed] [Google Scholar]
- 36.Saraiva MJ. Transthyretin mutations in hyperthyroxinemia and amyloid diseases. Hum Mutat. 2001;17(6):493–503. doi: 10.1002/humu.1132. [DOI] [PubMed] [Google Scholar]
- 37.Moses AC, Lawlor J, Haddow J, Jackson IMD. Familial euthyroid hyperthyroxinemia resulting from increased thyroxine binding to thyroxine-binding prealbumin. N Engl J Med. 1982;306:966–9. doi: 10.1056/NEJM198204223061605. [DOI] [PubMed] [Google Scholar]
- 38.Scrimshaw BJ, Fellowes AP, Palmer BN, Croxson MS, Stockigt JR, George PM. A novel variant of transthyretin (prealbumin), Thr119 to Met, associated with increased thyroxine binding. Thyroid. 1992;2:21–6. doi: 10.1089/thy.1992.2.21. [DOI] [PubMed] [Google Scholar]
- 39.Alexopoulos A, Hutchinson W, Bari A, Keating JJ, Johnson PJ, Williams R. Hyperthyroxinaemia in hepatocellular carcinoma: relation to thyroid binding globulin in the clinical and preclinical stages of the disease. Br J Cancer. 1988;57:313–6. doi: 10.1038/bjc.1988.69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Jensen IW, Faber J. Familial dysalbuminaemic hyperthyroxinemia: a review. J Royal Soc Med. 1988;81:34–7. doi: 10.1177/014107688808100116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Arevalo G. Prevalence of familial dysalbuminemic hyperthyroxinemia in serum samples received for thyroid testing. Clin Chem. 1991;37:1430–1. [PubMed] [Google Scholar]
- 42.Mendel CM, Cavalieri RR. Thyroxine distribution and metabolism in familial dysalbuminemic hyperthyroxinemia. J Clin Endocrinol Metab. 1984;59(3):499–504. doi: 10.1210/jcem-59-3-499. [DOI] [PubMed] [Google Scholar]
- 43.Cartwright D, O'Shea P, Rajanayagam O, Agostini M, Barker P, Moran C, et al. Familial dysalbuminemic hyperthyroxinemia: a persistent diagnostic challenge. Clin Chem. 2009;55(5):1044–6. doi: 10.1373/clinchem.2008.120303. [DOI] [PubMed] [Google Scholar]
- 44.Sunthornthepvarakul T, Likitmaskul S, Ngowngarmratana S, Angsusingha K, Sureerat K, Scherberg NH, et al. Familial dysalbuminemic hypertriiodothyroninemia: a new dominantly inherited albumin defect. J Clin Endocrinol Metab. 1998;83:1448–54. doi: 10.1210/jcem.83.5.4815. [DOI] [PubMed] [Google Scholar]
- 45.Lafranchi SH, Snyder DB, Sesser DE, Skeels MR, Singh N, Brent GA, et al. Follow-up of newborns with elevated screening T4 concentrations. J Pediatr. 2003;143(3):296–301. doi: 10.1067/S0022-3476(03)00184-7. [DOI] [PubMed] [Google Scholar]
- 46.Refetoff S, Weiss RE, Usala SJ. The syndromes of resistance to thyroid hormone. Endocr Rev. 1993;14:348–99. doi: 10.1210/edrv-14-3-348. [DOI] [PubMed] [Google Scholar]
- 47.Ferrara AM, Onigata K, Ercan O, Woodhead H, Weiss RE, Refetoff S. Homozygous thyroid hormone receptor β-gene mutations in resistance to thyroid hormone: three new cases and review of the literature. J Clin Endocrinol Metab. 2012;97(4):1328–36. doi: 10.1210/jc.2011-2642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Lazar MA. Thyroid hormone receptors: multiple forms, multiple possibilities. Endocr Rev. 1993;14:184–93. doi: 10.1210/edrv-14-2-184. [DOI] [PubMed] [Google Scholar]
- 49.Parikh S, Ando S, Schneider A, Skarulis MC, Sarlis NJ, Yen PM, et al. Resistance to thyroid hormone in a patient without thyroid hormone receptor mutations. Thyroid. 2002;12(1):81–6. doi: 10.1089/105072502753452011. [DOI] [PubMed] [Google Scholar]
- 50.Friesema EC, Ganguly S, Abdalla A, Manning Fox JE, Halestrap AP, Visser TJ. Identification of monocarboxylate transporter 8 as a specific thyroid hormone transporter. J Biol Chem. 2003;278:40128–35. doi: 10.1074/jbc.M300909200. [DOI] [PubMed] [Google Scholar]
- 51.Bianco AC, Salvatore D, Gereben B, Berry MJ, Larsen PR. Biochemistry, cellular and molecular biology and physiological roles of the iodothyronine selenodeiodinases. Endocr Rev. 2002;23:38–89. doi: 10.1210/edrv.23.1.0455. [DOI] [PubMed] [Google Scholar]
- 52.Dumitrescu AM, Refetoff S. The syndromes of reduced sensitivity to thyroid hormone. Biochim Biophys Acta. 2013;1830(7):3987–4003. doi: 10.1016/j.bbagen.2012.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Polak M, Legac I, Vuillard E, Guibourdenche J, Castanet M, Luton D. Congenital hyperthyroidism: the fetus as a patient. Horm Res. 2006;65(5):235–42. doi: 10.1159/000092454. [DOI] [PubMed] [Google Scholar]
- 54.Thomas JS, Leclere J, Hartemann P, Duheille J, Orgiazzi J, Petersen M, et al. Familial hyperthyroidism without evidence of autoimmunity. Acta Endocrinol (Copenh) 1982;100:512–8. doi: 10.1530/acta.0.1000512. [DOI] [PubMed] [Google Scholar]
- 55.Kopp P, van Sande J, Parma J, Duprez L, Gerber H, Joss E, et al. Brief report: congenital hyperthyroidism caused by a mutation in the thyrotropin-receptor gene. New England Journal of Medicine. 1995;332:150–4. doi: 10.1056/NEJM199501193320304. [DOI] [PubMed] [Google Scholar]
- 56.Hébrant A, van Staveren WC, Maenhaut C, Dumont JE, Leclère J. Genetic hyperthyroidism: hyperthyroidism due to activating TSHR mutations. Eur J Endocrinol. 2011;164:1–9. doi: 10.1530/EJE-10-0775. [DOI] [PubMed] [Google Scholar]
- 57.Dumitrescu CE, Collins MT. McCune-Albright syndrome. Orphanet J Rare Dis. 2008;19:3–12. doi: 10.1186/1750-1172-3-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Tessaris D, Corrias A, Matarazzo P, De Sanctis L, Wasniewska M, Messina MF, et al. Thyroid abnormalities in children and adolescents with McCune-Albright syndrome. Horm Res Paediatr. 2012;78(3):151–7. doi: 10.1159/000342641. [DOI] [PubMed] [Google Scholar]
- 59.Dunzendorfer T. deLas Morenas A, Kalir T, Levin RM. Struma ovarii and hyperthyroidism. Thyroid. 1999;9(5):499–502. doi: 10.1089/thy.1999.9.499. [DOI] [PubMed] [Google Scholar]
- 60.Damle NA, Bal C, Kumar P, Soundararajan R, Subbarao K. Incidental detection of hyperfunctioning thyroid cancer metastases in patients presenting with thyrotoxicosis. Indian J Endocrinol Metab. 2012;16(4):631–6. doi: 10.4103/2230-8210.98028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Narasimhan KL, Ghobrial MW, Ruby EB. Hyperthyroidism in the setting of gestational trophoblastic disease. Am J Med Sci. 2002;323(5):285–7. doi: 10.1097/00000441-200205000-00012. [DOI] [PubMed] [Google Scholar]
- 62.Beck-Peccoz P, Persani L, Mannavola D, Campi I. Pituitary tumours: TSH-secreting adenomas. Best Pract Res Clin Endocrinol Metab. 2009;23(5):597–606. doi: 10.1016/j.beem.2009.05.006. [DOI] [PubMed] [Google Scholar]
- 63.Rankin FW, Graham AS. Tuberculosis of the thyroid gland. Annals of Surgery. 1932;96:625. doi: 10.1097/00000658-193210000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Das DK, Pant CS, Chachra KL, Gupta AK. Fine needle aspiration cytology diagnosis of tuberculous thyroiditis. A report of eight cases. Acta Cytol. 1992;36(4):517–22. [PubMed] [Google Scholar]
- 65.Majid U, Islam N. Thyroid tuberculosis: a case series and a review of the literature. J Thyroid Res. 2011;2011:359864. doi: 10.4061/2011/359864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Luiz HV, Pereira BD, Silva TN, Veloza A, Matos C, Manita I, et al. Thyroid tuberculosis with abnormal thyroid function--case report and review of the literature. Endocr Pract. 2013;19(2):e44–9. doi: 10.4158/EP12276.CR. [DOI] [PubMed] [Google Scholar]
- 67.Cabibi D, Di Vita G, La Spada E, Tripodo C, Patti R, Montalto G. Thyroid sarcoidosis as a unique localization. Thyroid. 2006;16(11):1175–7. doi: 10.1089/thy.2006.16.1175. [DOI] [PubMed] [Google Scholar]
- 68.Manchanda A, Patel S, Jiang JJ, Babu AR. Thyroid: an unusual hideout for sarcoidosis. Endocr Pract. 2013;19(2):40–3. doi: 10.4158/EP12131.CR. [DOI] [PubMed] [Google Scholar]
- 69.Kmieć P, Lewandowska M, Dubaniewicz A, Mizan-Gross K, Antolak A, Wołyniak B, et al. Two cases of thyroid sarcoidosis presentation as painful, recurrent goiter in patients with Graves' disease. Arq Bras Endocrinol Metabol. 2012;56(3):209–14. doi: 10.1590/s0004-27302012000300010. [DOI] [PubMed] [Google Scholar]
- 70.Mannavola D, Vannucchi G, Fugazzola L, Cirello V, Campi I, Radetti G, et al. TBG deficiency: description of two novel mutations associated with complete TBG deficiency and review of the literature. J Mol Med (Berl) 2006;84(10):864–71. doi: 10.1007/s00109-006-0078-9. [DOI] [PubMed] [Google Scholar]
- 71.Domingues R, Bugalho MJ, Garrão A, Boavida JM, Sobrinho L. Two novel variants in the thyroxine-binding globulin (TBG) gene behind the diagnosis of TBG deficiency. Eur J Endocrinol. 2002;146(4):485–90. doi: 10.1530/eje.0.1460485. [DOI] [PubMed] [Google Scholar]
- 72.Ueta Y, Mitani Y, Yoshida A, Taniguchi S, Mori A, Hattori K, et al. A novel mutation causing complete deficiency of thyroxine binding globulin. Clin Endocrinol (Oxf). 1997;47:1–5. doi: 10.1046/j.1365-2265.1997.2181030.x. [DOI] [PubMed] [Google Scholar]
- 73.Miura Y, Hershkovitz E, Inagaki A, Parvari R, Oiso Y, Phillip M. A novel mutation causing complete thyroxine-binding globulin deficiency (TBG-CD-Negev) among the Bedouins in southern Israel. J Clin Endocrinol Metab. 2000;85(10):3687–9. doi: 10.1210/jcem.85.10.6899. [DOI] [PubMed] [Google Scholar]
- 74.Su CC, Wu YC, Chiu CY, Won JG, Jap TS. Two novel mutations in the gene encoding thyroxine-binding globulin (TBG) as a cause of complete TBG deficiency in Taiwan. Clin Endocrinol (Oxf) 2003;58(4):409–14. doi: 10.1046/j.1365-2265.2003.01730.x. [DOI] [PubMed] [Google Scholar]
- 75.Li P, Janssen OE, Takeda K, Bertenshaw RH, Refetoff S. Complete thyroxine-binding globulin (TBG) deficiency caused by a single nucleotide deletion in the TBG gene. Metabolism. 1991;40(11):1231–4. doi: 10.1016/0026-0495(91)90221-H. [DOI] [PubMed] [Google Scholar]
- 76.Carvalho GA, Weiss RE, Refetoff S. Complete thyroxine-binding globulin (TBG) deficiency produced by a mutation in acceptor splice site causing frameshift and early termination of translation (TBG-Kankakee) J Clin Endocrinol Metab. 1998;83(10):3604–8. doi: 10.1210/jcem.83.10.5208. [DOI] [PubMed] [Google Scholar]
- 77.Lacka K, Nizankowska T, Ogrodowicz A, Lacki JK. A novel mutation (del 1711 G) in the TBG gene as a cause of complete TBG deficiency. Thyroid. 2007;17(11):1143–6. doi: 10.1089/thy.2007.0023. [DOI] [PubMed] [Google Scholar]
- 78.Mori Y, Takeda K, Charbonneau M, Refetoff S. Replacement of Leu227 by Pro in thyroxine-binding globulin (TBG) is associated with complete TBG deficiency in three of eight families with this inherited defect. J Clin Endocrinol Metab. 1990;70(3):804–9. doi: 10.1210/jcem-70-3-804. [DOI] [PubMed] [Google Scholar]
- 79.Domingues R, Font P, Sobrinho L, Bugalho MJ. A novel variant in Serpina7 gene in a family with thyroxine-binding globulin deficiency. Endocrine. 2009;36(1):83–6. doi: 10.1007/s12020-009-9202-2. [DOI] [PubMed] [Google Scholar]
- 80.Reutrakul S, Janssen OE, Refetoff S. Three novel mutations causing complete T(4)-binding globulin deficiency. J Clin Endocrinol Metab. 2001;86(10):5039–44. doi: 10.1210/jcem.86.10.7916. [DOI] [PubMed] [Google Scholar]
- 81.Reutrakul S, Dumitrescu A, Macchia PE, Moll GW, Jr, Vierhapper H, Refetoff S. Complete thyroxine-binding globulin (TBG) deficiency in two families without mutations in coding or promoter regions of the TBG genes: in vitro demonstration of exon skipping. J Clin Endocrinol Metab. 2002;87(3):1045–51. doi: 10.1210/jcem.87.3.8275. [DOI] [PubMed] [Google Scholar]
- 82.Yamamori I, Mori Y, Seo H, Hirooka Y, Imamura S, Miura Y, et al. Nucleotide deletion resulting in frameshift as a possible cause of complete thyroxine-binding globulin deficiency in six Japanese families. J Clin Endocrinol Metab. 1991;73(2):262–7. doi: 10.1210/jcem-73-2-262. [DOI] [PubMed] [Google Scholar]
- 83.Moeller LC, Fingerhut A, Lahner H, Grasberger H, Weimer B, Happ J, et al. C-terminal amino acid alteration rather than late termination causes complete deficiency of thyroxine-binding globulin CD-NeuIsenburg. J Clin Endocrinol Metab. 2006;91(8):3215–8. doi: 10.1210/jc.2005-2261. [DOI] [PubMed] [Google Scholar]