

To the Editor
Medicare is currently dispensing $30 billion in incentives to adapt Electronic Medical Records (EMRs). In 2014, incentives for “meaningful use” of EMRs will require online access by patients and reimbursement penalties up to 5% for non-adoption will begin in 2015.1 Broader use of online patient portals to EMRs is intended to improve care coordination; yet the impact of common problems in Medicare patients, such chronic illness or functional impairment, on internet use is unknown.
Methods
We used the Health and Retirement Study (http://hrsonline.isr.umich.edu), a nationally-representative sample of community-dwelling seniors (limited to Medicare-eligible, age≥65) for cross-sectional analysis of internet use at 2 time-points, 2002 and 2010 (Table). We performed descriptive statistics (chi-square or t-test) and multivariable (MV) regression analysis (modified Poisson) to characterize features of internet use at each time-point.
Table.
Demographics and clinical features of seniors as determinants of internet use in 2002 and 2010
| Characteristic | Internet Use in 2002 (n=9,340) | Internet Use in 2010 (n=9,315) | Percent increase 2002–10 | |
|---|---|---|---|---|
| Overall | (entire sample) | 1892 (21%) | 3481 (42%) | 100% |
| Demographics | Gender | |||
| Male | 915 (25%) | 1562 (46%) | 85% | |
| Female | 977 (18%) | 1919 (39%) | 117% | |
| Ethnicity | ||||
| White | 1767 (23%) | 3101 (46%) | 100% | |
| Non-White | 125 (7%) | 379 (21%) | 200% | |
| Married or Partnered | ||||
| Yes | 1438 (28%) | 2518 (51%) | 84% | |
| No | 453 (12%) | 963 (29%) | 142% | |
| Age | Range 50–109 | Mean 74.6 (±6.9) | Mean 74.6 (±7.3) | |
| 65–70 | 882 (32%) | 1168 (59%) | 84% | |
| 70–75 | 535 (24%) | 1174 (47%) | 92% | |
| ≥75 | 474 (12%) | 1139 (27%) | 127% | |
| Health | Any Chronic Condition | |||
| No | 515 (26%) | 602 (52%) | 102% | |
| Yes | 1377 (19%) | 2879 (40%) | 107% | |
| Self-Rated Health | Fair or Poor | |||
| No | 1612 (25%) | 2938 (47%) | 93% | |
| Yes | 279 (11%) | 543 (25%) | 131% | |
| Functional Status | ADL/IADL Difficulty | |||
| No | 1635 (25%) | 2848 (50%) | 98% | |
| Yes | 257 (10%) | 633 (23%) | 134% | |
Internet use was defined by a “yes” response to the question: “Do you regularly use the World Wide Web, or the Internet, for sending and receiving e-mail or for any other purpose, such as making purchases, searching for information, or making travel reservations?”
ADL = Activities of Daily Living: bathing, toileting, dressing, eating, walking; IADL = Instrumental ADL: shopping, housekeeping, cooking, finances, telephone use, transportation outside the home.
Results
Overall rates of internet use doubled 2002–2010 (21% vs. 42%); however, changes in use differed by demographic and health characteristics. Overall, groups with the lowest rates showed the largest relative increases 2002–2010: non-Whites (7% to 21%; 200% increase), functionally-impaired (10% to 23%), low self-rated health (11% to 25%), age≥75, (12% to 26%), non-married (12% to 29%), and any chronic condition (19% to 40%) (Table).
In MV regressions adjusted for demographics and socio-economic status, those over age 75 or with functional impairments were less likely to use the Internet than all other groups in both 2002 and 2010. Comparing these adjusted ratios in 2002 to 2010, there were significant changes in several low-use groups: age ≥75, non-Whites, and those with poor SRH. There was no significant change, however, for those with functional impairment (Figure).
Figure.
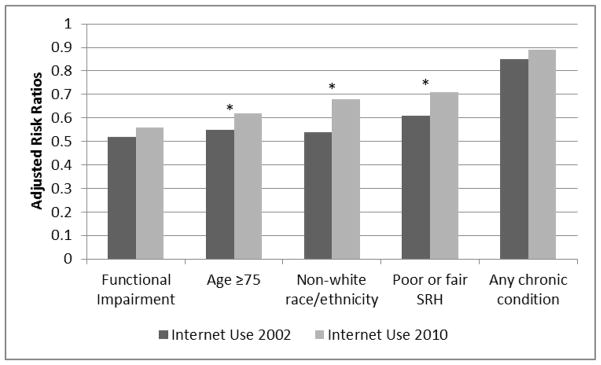
Adjusted Risk Ratios** for Internet Use in 2002 and 2010 in Low-Use Groups
*p<.05 for change in RR from 2002 to 2010; RR of 1.0 indicates no difference from reference group. Reference groups: 1. no functional impairment; 2. age <75; 3. White race; 4. Good or better SRH
**Risk ratios adjusted for demographics (gender, race, marital status) and socio-economic status (education and net worth).
All analyses weighted for differential probability of selection and the complex sampling design of the HRS.
Comment
Internet use has increased in Medicare-eligible patients from 2002–2010 but remains very low for the frailest seniors. Our results suggest functional ability is more predictive of internet non-use than chronic illness, self-rated health, or age which has important implications for patient portal use. While prior studies of the “digital divide” in healthcare have highlighted demographic and SES differences,2 our study demonstrates the additional impact of functional limitations that are prevalent in the Medicare population. If these trends from the early years of EMR use persist into the current era of rapid implementation, the frailest and most vulnerable patients may be at risk for increasingly dis-engaged and un-coordinated care as more aspects of healthcare move online.
Thus, strategies to reduce the “digital divide” in Medicare patients will also need to address functional limitations. Existing disability software can “read” webpages out loud for the visually-impaired and voice-recognition software may improve internet use for those who cannot easily use a mouse or keyboard. Furthermore, emerging mobile technologies such as touchscreens, smartphones, and motion sensors may enable a wide range of body gestures to further expand web-based interactions with the EMR.3 While more evidence is needed to validate outcomes for these approaches,4 it is clear patient portals will require greater agility to adapt to patient needs. Beyond adaptive changes in the technology per se, more training is needed for frail seniors and their caregivers to use portals effectively to engage in care. Indeed, caregivers (often younger and not functionally-impaired) are likely important but overlooked targets for expanding portal use and improving care coordination for frail seniors.5 Without such adaptations, frail seniors who might otherwise benefit the most from portals may be the least likely to engage.
Meaningful use of EMRs will soon require patient portal use by Medicare patients and more seniors are going online now than ever;6 however, our findings highlight the need for providers to address functional barriers to internet use and future research to target digital health interventions to the specific needs of the frailest patients in this aging population.
Acknowledgments
The authors would like to recognize John Boscardin, PhD in the UCSF Divisions of Biostatistics and Epidemiology and Geriatric Medicine for expert statistical advice. Dr. Greysen is supported by National Institute of Aging (NIA) through the Claude D. Pepper Older Americans Independence Center, a Career Development Award (1K23AG045338-01) and the NIH-NIA Loan Repayment Program. Dr. Covinsky is supported by the NIA through a K-24 Career Mentoring Award and an R01 from the National Institute for Nursing Research. Dr. Sudore is supported by the U.S. Department of Veterans Affairs, the National Palliative Care Research Center Foundation, and the National Institute on Aging, 1R01AG045043-01.
Footnotes
Disclosures:
The authors have no conflicts of interest to declare relative to this study. The first author (SRG) had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
References
- 1.Marcotte L, Seidman J, Trudel K, et al. Achieving Meaningful Use of Health Information Technology: A Guide for Physicians to the EHR Incentive Programs. Arch Intern Med. 2012;172(9):731–736. doi: 10.1001/archinternmed.2012.872. [DOI] [PubMed] [Google Scholar]
- 2.Chang BL, Bakken S, Brown SS, Houston TK, Kreps GL, Kukafka R, Safran C, Stavri PZ. Bridging the digital divide: reaching vulnerable populations. J Am Med Inform Assoc. 2004 Nov-Dec;11(6):448–57. doi: 10.1197/jamia.M1535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Steinhubl SR, Muse ED, Topol EJ. Can Mobile Health Technologies Transform Health Care? JAMA. 2013 Dec 11;310(22):2395–6. doi: 10.1001/jama.2013.281078. [DOI] [PubMed] [Google Scholar]
- 4.Kumar S, Nilsen WJ, Abernethy A, et al. Mobile health technology evaluation: the mHealth evidence workshop. Am J Prev Med. 2013 Aug;45(2):228–36. doi: 10.1016/j.amepre.2013.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sarkar U, Bates DW. Care partners and online patient portals. JAMA. 2014 Jan 22–29;311(4):357–8. doi: 10.1001/jama.2013.285825. [DOI] [PubMed] [Google Scholar]
- 6.Zickuhr K, Madden M. [Accessed May 22, 2013];Older Adults and Internet Use: for the first time, half of adults ages 65 and older are online. Available at: http://pewinternet.org/Reports/2012/Older-adults-and-internet-use.aspx.