

Abstract
Background:
This paper aimed to evaluate the application of computer-aided design and computer-aided manufacturing (CAD-CAM) technology and the factors that affect the survival of restorations.
Materials and Methods:
A thorough literature search using PubMed, Medline, Embase, Science Direct, Wiley Online Library and Grey literature were performed from the year 2004 up to June 2014. Only relevant research was considered.
Results:
The use of chair-side CAD/CAM systems is promising in all dental branches in terms of minimizing time and effort made by dentists, technicians and patients for restoring and maintaining patient oral function and aesthetic, while providing high quality outcome.
Conclusion:
The way of producing and placing the restorations made with the chair-side CAD/CAM (CEREC and E4D) devices is better than restorations made by conventional laboratory procedures.
Keywords: chair-side restoration, computer-aided design and computer-aided manufacturing, digital dentistry
Introduction
The idiom “CAD/CAM” in dental technology is an abbreviation for “computer-aided design” and “computer-aided manufacturing,” used to improve the design and creation of dental restorations including crowns, veneers, inlays and onlays, fixed bridges, implants, dentures, and orthodontic appliances. Early efforts of this technology were in the mid-1980s. Dr. Mörmann developed CEREC system; an innovative approach to make same day restorations in the dental clinic at the chair-side.1 Historically, the CEREC System (Sirona) was the first chair-side CAD/CAM system in dentistry and is currently available in its third product generation. In 2006, Mörmann pointed out that the concept of CEREC CAD/CAM is becoming an important part of dentistry.2
CAD/CAM Components
The CAD/CAM systems consist of three major components. The first component is a digitalization tool/scanner, which converts geometry to digital information that can be processed by the computer. The second component is software, which processes information, depending on the application, provides information and data of the product intends to manufacture. The third component is a milling device/production technology that converts the information into the specific product.2
CAD/CAM Systems
The available advanced CAD/CAM systems can be divided into the following three groups based on their production methods:3
In office system: Where a dentist digitally scans the prepared tooth, creates restorations chair-side, and then seats it within a single appointment.
In lab system: Where laboratories could scan models made from physical impressions and use CAD/CAM to produce restorations.
Centralized production: Where a dentist captures chair-side digital impressions then sent data via the internet to the laboratory.
The current existing in-office systems with chair-side milling machines are the CEREC from (Sirona Dental; Charlotte, NC) and E4D from (D4D Technologies; Richardson, TX). Chair-side digital impression systems with transfer of images to the laboratory include the iTero, CEREC and Lava C.O.S. systems. The scanned data can be exported to a laboratory (via CEREC AC Connect or E4D Sky) to have more complicated or advanced restorations fabricated.3
Chair-side CAD/CAM Materials
Several of materials are available for chair-side CAD/CAM restorations, which achieved predictability and longevity. All blocks are either monochromatic or polychromatic form for chair-side CAD/CAM restorations. Studies have proved their predictability and longevity. These materials include esthetic and high-strength ceramics, composite resins, and nanoceramics, which facilitate handling and finishing. Innovations in the CEREC AC system involving the use of materials such as IPS Empress CAD Multi Block and IPS e.max CAD have provided dentists with an efficient and effective delivery style for the routine placement of all-ceramic restorations chair-side.4
Feldspar-based ceramic Vitablocs Mark I (Vident).
High-glass–feldspar-based ceramic Vitablocs Mark II (Vident).
Infiltrated leucite glass-ceramic. ProCAD (Ivoclar Vivadent).
Resin-based composite Paradigm MZ100 blocks (3M ESPE).
Paradigm C (3M ESPE).
Lithium disilicate glass ceramic (IPS e.max CAD, Ivoclar Vivadent) for anterior or posterior crowns, implant crowns, inlays, and onlays or veneers.
CEREC block by Sirona.
These blocks material have strength, dense, high-quality, and excellent esthetic properties superior than traditional material as well these materials exhibit a “chameleon” effect. All recent developments in CAD/CAM materials concern high strength and easy-to-use. The Computer-aided manufacturing procedures will indisputably change many aspects of dentistry in the future, especially with regard to treatment simplicity and production period. Therefore clinicians and technicians must be aware of the advantages and disadvantages of computer-aided manufacturing while such procedures continue to develop and become an integral part of dentistry.5
System development
The CEREC system developed through a combination of software and hardware upgrades since its launch to the dental marketplace as the CEREC 1 system led to a marked improvement in clinical efficiency through allowing for simultaneous design of one restoration while milling a second one. Three-dimensional (3D) design program improved speed and memory of computers, and also improved the clinical workflows of chair-side system.5
New CEREC Omnicam is powder-free and precise 3D continuous images in natural color. CAD/CAM-generated all-ceramic restorations facilitate the rebuilding of deeply destructed teeth regardless of the location of the cavity margins.6
Advantages
Providing a tooth-colored restoration in single visit appointment is the main goal of the chair-side concept with CAD/CAM technology. This system is an advantage for the immediately definitive protection of the tooth without any temporary phase. In-office CAD/CAM allows dentists to provide same-visit indirect restorations that are accurate and esthetically satisfied. Digital impression taking create accurate models, which is used for fabrication of either traditional or CAD/CAM restorations, and needs less chair-side time.3
In-office CAD/CAM systems offer the amazing and distinctive features that give the dentist full control over restorative process; dentist will appreciate the speed of these systems in addition to the significant reduction in lab bills. Chair-side CEREC CAD/CAM is designed to eliminate the need for traditional impression and provisional restorations. The preparation and margin evaluation was performed immediately. Van Zeghbroeck et al. (2012) reported that using the CEREC 3D chair-side CAD/CAM technology shown to be a feasible, precise, esthetic and durable solution in limited cognitive skills patient.7 Most patients prefer the CAD/CAM single-appointment concept to the conventional multi-appointment.8 The dentist could produce restorations use of digital impressions with a high degree of reliability and longevity.9
Touchstone et al. (2010) intensified the smile of a 63-year-old woman that was concerned about the appearance of her existing dental restorations using milled CAD/CAM all-ceramic polylithic restorations. Conclude that digital restorative dentistry has matured. Although previously it was restricted to the chair-side single-visit treatment, now can be utilized to almost any restorative conditions, including rehabilitation of full-mouth.10
CEREC restorations have an acceptable, marginal adaptation and clinical longevity along with reduced chair time and improved esthetics.11 CAD/CAM technologies give dentist The ability to fabricate an chair-side restoration with controlling all of the essential elements of a restoration–from contours and occlusion to finishing and choice of placement–within timetables that are correspond with those of conventional methods.4
Disadvantages
Despite of the previous advantages of chair-side CAD/CAM system we can concludes the disadvantage of this system include cost, the price of investment and maintenance, fear of the unknown, lack of willingness to learn a new concept, refuse of change practicing way, dentists should have additional training in CAD/CAM, negative comments from some peers, the few number of users, reject things that would reduce the stability of the practice, the size of the scanning device and the milling machine, lack of desire to delegate clinical procedures, relationship with previous dental laboratories, concern about color matching, staining, quality and longevity of restorations.11
Application of CAD-CAM technology
Beside its most common application in the restorative treatments (inlay-onlay-crown-veneer-multi units FPD), application of the CAD/CAM technology was performed in Orthodontic occlusal splints, in implant related components,12 and orthodontic treatment planning to measure soft tissues,13 in addition to fabrication of removable complete denture even if the development was slowly.14 Furthermore, CAD/CAM technique is ideal for fabrication of oral and facial prostheses.15
It is a feasible solution in limited cognitive skills patient.7 CAD/CAM-generated all-ceramic restorations facilitate the rebuilding of deeply destructed teeth regardless of the location of the cavity margins.6
The aim of the study
The main objective of this paper was to review the chair-side CAD/CAM clinical performance. The author’s reviewed all valid research material related chair-side CAD/CAM from a database of articles available from 2004 up to 2014. Data sources included PubMed, Medline, Embase, Science Direct and Wiley Online Library. Only relevant literature was considered. This paper gives an in depth insight on chair-side CAD/CAM clinical performance. It gives clinicians a detailed understanding of the advantages, drawbacks, indications, contraindications of chair-side CAD/CAM. Clinicians are able to correlate this knowledge during case selection and placement for better longevity and performance of restorations.
Discussion
Material comparison
Numerous studies compared the materials used in chair-side CAD/CAM system (Table 1). Magne et al. (2010) studied fatigue resistance of CAD/CAM composite resin and ceramic posterior occlusal veneers found that composite resin (Paradigm MZ100) had significantly higher fatigue resistance (P < 0.002) compared to IPS Empress CAD and IPS e.max CAD16 where Schlichting et al. (2011) found that composite resins (MZ100 and XR) increased the fatigue resistance of ultra-thin occlusal veneers (P < 0.001) if compared to the ceramics evaluated (Empress CAD and e.max CAD).17 Vichi et al. (2013) Stated that materials available on the market for CEREC CAD/CAM, had a flexural strength greater than 100 Mpa, therefore, meets the ISO standard.18
Table 1.
The studies that compared the materials used in chair-side CAD/CAM system.
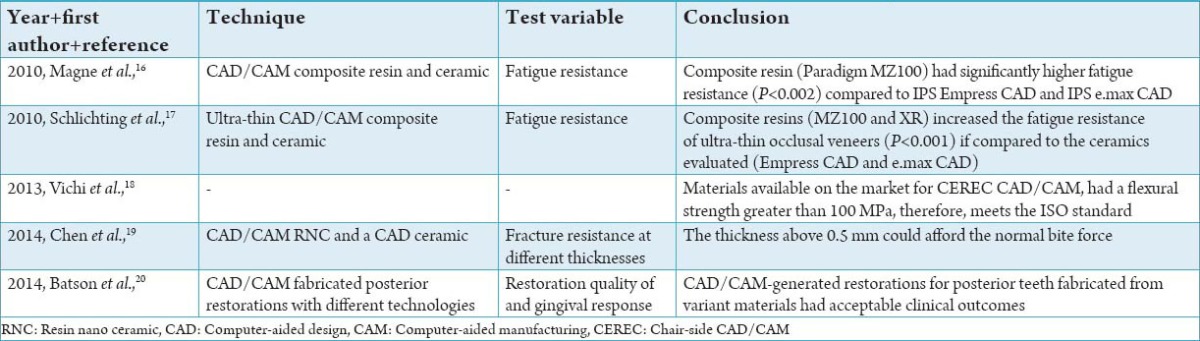
In 2014 researchers, studied the fracture resistance of a CAD/CAM Resin Nano Ceramic and a CAD ceramic at different thicknesses above 0.5 mm which could afford the normal bite force.19 Batson et al., 2014 reported that CAD/CAM-generated restorations for posterior teeth fabricated from variant materials had acceptable clinical outcomes.20
Survival and success
According to scientific literature, they reported success rates for CAD/CAM produced inlays of 90% after 10 years and 85% after 12 and 16 years.21 The survival of CEREC-generated restorations was reported to be about 97 for 5 years and 90% for 10 years.9
Digital impressions and conventional impressions
Many studies investigated digital impressions and conventional impression techniques (Table 2). Digital impression involve taking a digital scan with an intraoral camera of prepared tooth and surrounding soft tissue, the software translate this data into a virtual 3D model instead of die in order to design then mill the restoration, without any need of impression materials, trays, pouring and trimming. This procedure enables immediate evaluation of preparation and margin.4
Table 2.
The studies that investigated digital impressions and conventional impressions technique.
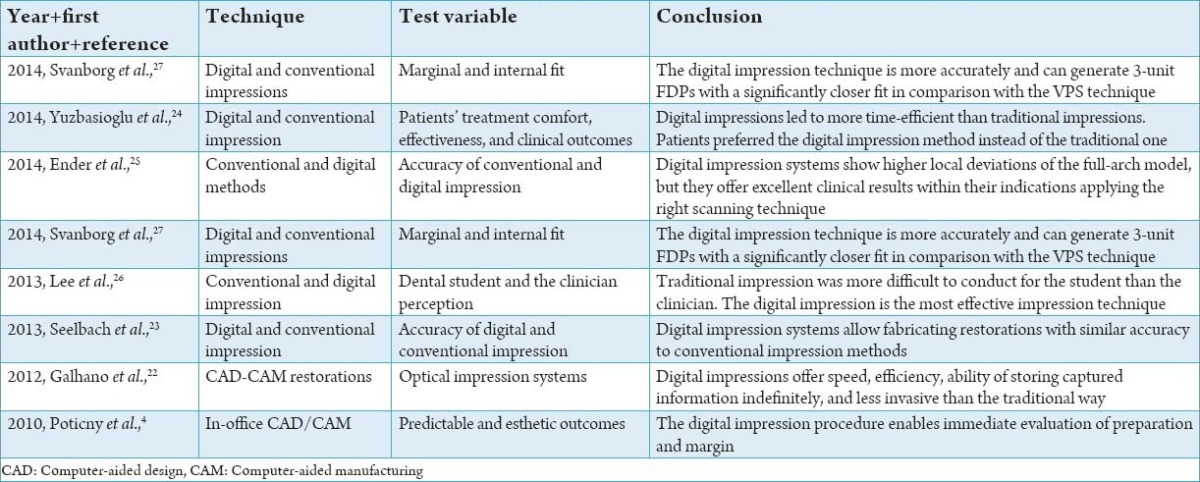
Digital imaging has been constantly improved. CEREC has presented the bluecam with anti-shake features and automatically eliminates any substandard images, which require a light dusting of powder to make imaging easer. In 2012, Sirona introduced the new powder-free CEREC Omnicam, which displaying the 3D data in full color. CAD/CAM images can be taken either through direct or indirect imaging. In The indirect systems, we obtained the digitalization from the impression material or cast, where the direct way the image is taken directly from the mouth using intraoral scanners. In other words, a virtual 3D model is created on the bases of three sets of data (stone cast, impression body, and intraoral) obtained from the scanning process. Digital impressions offer speed, efficiency, ability of storing captured information indefinitely, transferring digital images between the dental office and the laboratory and less invasive than the traditional way.22 Seelbach et al. (2013) stated that digital impression systems allow fabricating restorations with similar accuracy to conventional impression methods.23
Yuzbasioglu et al. (2014) Found that digital impressions are more efficient in minimize the time from the traditional impressions. Patients prefer digital impression technology instead of traditional techniques. They compare two impression techniques from the standpoint of patient predilection and treatment comfort. They found that Digital impressions led to more time-efficient than traditional impressions. Patients preferred the digital impression method instead of the traditional one.24 Ender and Mehl (2014) found that traditional and digital impression methods reveal differences relating full-arch accuracy. Digital impression systems show higher local deviations of the full-arch model, but they offer excellent clinical results within their indications applying the right scanning technique.25
Lee et al. (2013) assessed the level of difficulty and cognition between dental students and experienced clinicians when submitting digital and traditional impressions. They found that traditional impression was more difficult to conduct for the student than the clinician; nevertheless, the difficulty level of the digital impression was the same in both of them; while the student preferred the digital impression as the most effective impression technique, and the clinician had an even distribution in the choice of preferred and effective impression techniques.26 In 2014, Svanborg et al., stated that the digital impression technique is more accurately and can generate 3-unit FDPs with a significantly closer fit in comparison with the VPS technique.27
Comparison of chair-side systems CEREC and E4D
The researchers found that Lithium disilicate crowns manufactured with the CEREC 3D Bluecam scanner CAD/CAM system or the heat-pressing technique has shown a significantly minimum vertical misfit than crowns manufactured with E4D Laser scanner CAD/CAM system.28 Other researcher pointed out that spacer thickness and manufacturing technique affecting the adaptation of ceramic crowns while the heat-press achieved the best marginal and internal crown adaptation outcomes. They recommended 30- or 60-µm spacer thickness for the E4D CAD/CAM system.29
Clinical performance of chair-side CAD/CAM restoration
Numerous studies investigated the clinical performance of chair-side CAD/CAM restorations (Table 3). Song et al. (2013) reported that the marginal gaps of anterior 3-unit zirconia FPD varied in accordance with CAD/CAM systems, but still within clinically acceptable limits in comparison with traditional metal-ceramic restoration.30
Table 3.
The studies that investigated the clinical performance of chair-side CAD/CAM restorations.
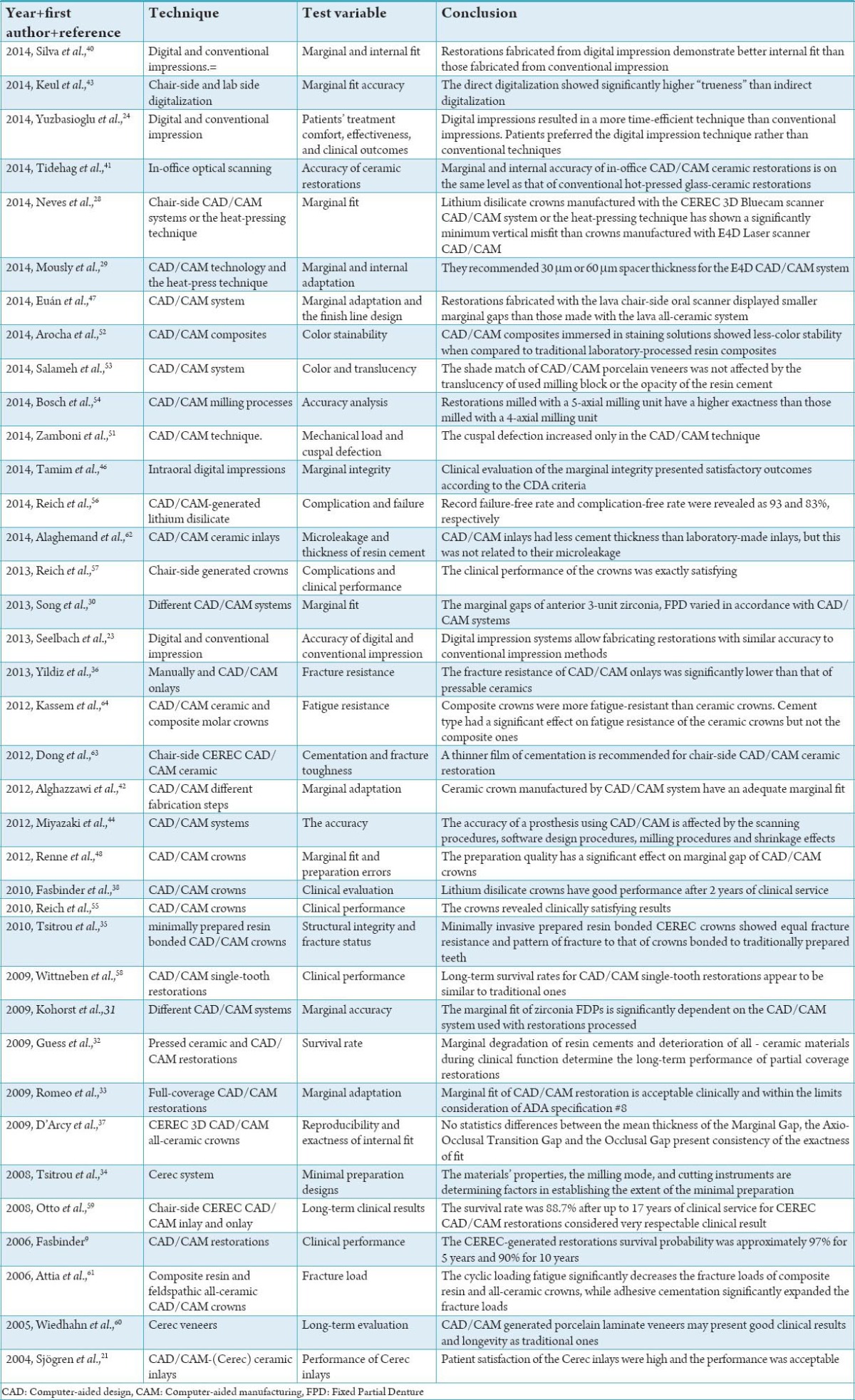
Kohorst et al. (2009) concluded that the marginal fit of zirconia FDPs is significantly dependent on the CAD/CAM system used with restorations processed of fully sintered zirconia showing better fitting accuracy.31 Guess et al. (2009) found that pressed ceramic and CAD/CAM fabricated partial coverage restorations showed a reliable treatment option to restore larger distortions in posterior teeth. Marginal degradation of the resin cement and deterioration of the all-ceramic materials during clinical function determine the clinical long-term performance of partial coverage restorations.32
Romeo et al. (2009) concluded that marginal fit of CAD/CAM restoration is acceptable clinically and within the limits consideration of ADA specification ##8. Hence, milled CAD/CAM crowns can be considered a good alternative for the conventional waxing-investing-casting technique.33
Tsitrou and van Noort (2008) showed that in the minimal preparation only the composite material produced acceptable crowns with intact margins, as ceramic materials required a wider preparation design in order to produce acceptable crowns. It was also found that the materials’ properties, the milling mode, and cutting instruments are determining factors in establishing the extent of the minimal preparation.34
Tsitrou et al. (2010) compared the structural integrity and fracture status of teeth prepared traditionally and minimally invasive to restore with resin bonded CAD/CAM crowns manufacture from one material, they found that minimally invasive prepared resin bonded CEREC crowns showed equal fracture resistance and pattern of fracture to that of crowns bonded to traditionally prepared teeth.35 Others evaluated fracture resistance in lithium disilicate onlays fabricated manually and with CAD/CAM technique, yielded that both can be a viable treatment option.36
D’Arcy et al. (2009) assess the reproducibility and exactness of internal fit using CEREC 3D CAD/CAM all-ceramic crowns and study the proximal contact point areas between the crowns and adjacent teeth. They didn’t found any statistics differences between the mean thickness of the marginal gap, the axio-occlusal transition gap, and the occlusal Gap.37
Seelbach et al. (2013) stated that digital impression systems allow the manufacturing of restorations with a similar exactness as traditional impression techniques.23 Sjögren et al. (2004) reported high patient gratification and espousal of the CEREC inlays, and the performance after 10 years of clinical service was satisfactory, particularly with regard to the inlays luted with the chemically cured resin composite. The characteristics of the luting agents influence the longevity of ceramic inlays.21
Fasbinder (2006) reported that postoperative sensitivity was principally due to occlusal interferences. Long-term postoperative sensitivity was not a reported problem. Restoration fracture is the primary mode of failure for CEREC-generated restorations and similar to other ceramic restorations. Margin wear was seldom reported. The survival possibility of CEREC-generated restorations was reported to be about 97% for 5 years and 90% for 10 years. Low rate of restoration fracture and long-term clinical survive ability document the effectiveness of the CEREC system as a reliable, esthetic restorative option for patients.9 In 2010, Fasbinder et al. pointed out that there was no reported sensitivity at 1 or 2 years.38
Nash (2014) made resurfacing for a natural tooth structure using ceramic laminates in order to solve different aesthetic and/or functional troubles, expected that CAD/CAM ceramic laminates can be last about twice as long as direct composite alternatives, making them an excellent patient treatment option, when indicated.39
Silva et al. (2014) indicated that restorations fabricated from digital impression demonstrate better internal fit than those fabricated from conventional impression.40 In 2014, they found slight differences between the two types of ceramic crowns (CAD/CAM ceramic crowns-conventional hot-pressed glass ceramic crown) with regard to the internal fit.41 Ceramic crown manufactured by CAD/CAM system have an adequate marginal fit, and the process of glass infiltration improves the marginal fit after machining.42
Keul et al. (2014) stated that regarding the accuracy, which leads to better marginal fit the direct digitalization showed significantly higher “trueness” than indirect digitalization.43 The accuracy of a prosthesis using CAD/CAM is affected by the scanning procedures, software design procedures, milling procedures and shrinkage effects.44 Accuracy has been recorded for intra-oral scanners by several authors.45
Tidehag et al. (2014) concluded that marginal and internal accuracy of in-office CAD/CAM ceramic restorations is on the same level as that of conventional hot-pressed glass-ceramic restorations.41 Clinical assessment of the marginal integrity showed satisfactory outcomes according to the CDA criteria.46
Some researchers identified differences in the finish line design were only between the round shoulder and chamfer with the lava all-ceramic system. In another hand, restorations fabricated with the lava chair-side oral scanner showed smaller marginal gaps.47 The preparation quality has a significant effect on marginal gap of CAD/CAM crowns.48
The rounded shoulder finish line show marginal discrepancy values significantly lower than tilted and large chamfer, but large chamfer produced the least internal discrepancy values. Independent of the finish line type, internal discrepancy was the lowest in the axial region followed by the radius and occlusal regions.49 Euán et al. (2012) stated that marginal adaptation was affected by the finish line design. The marginal gap was within the scope of clinical acceptability.50 In 2014, Zamboni et al. noticed increase cuspal defection in the CAD/CAM technique.51
Composites CAD/CAM restorations immersed in staining solutions showed less color stability in comparison to conventional laboratory-processed resin composites.52 The shade match of CAD/CAM porcelain veneers was not affected by the translucency of used milling block or the opacity of the resin cement.53
Bosch et al. (2014) investigated the influence of various milling processes on the accuracy of ceramic restorations. They stated that restorations milled with a 5-axial milling unit have a higher exactness than those milled with a 4-axial milling unit. A rotary cutting instrument with a smaller diameter led in a more exactitude milling process. The 2-step mode is not significantly better than the 1-step mode.54
Lithium disilicate crowns performance was characterized significant after 2 years of clinical service.38 Reich et al. (2010) assessed the clinical performance of chair-side -generated crowns during a preliminary time-period of 2 years. They declared that the crowns showed clinically satisfying outcomes.55
After a mean observation time of 46 months, Reich et al. (2014) recorded the failure-free rate, and complication-free rate were revealed as 93 and 83%, respectively.56 The clinical performance of the crowns was exactly satisfying.57
Roggendorf et al. (2012) reported a total of 96.4% of the restorations revealed sufficient ratings for esthetic properties “anatomic form,” “color match,” “marginal discoloration,” and “marginal integrity.” The survival rate of 86.9% at the 7 years recall indicated that adhesively luted all-ceramic CAD/CAM-generated restorations are suitable for restoration of extended coronal distortion.6
Long-term survival rates for CAD/CAM restorations appear to be similar to the traditional one.58 The survival rate was 88.7% after up to 17 years of clinical service for CEREC CAD/CAM restorations considered very respectable clinical result. A total of (11%) failure was found (62%) to ceramic fractures (14%) tooth fractures (19%) caries and (5%) endodontic problems.59
Wiedhahn et al. (2005) studied the long-term treatment outcome of CAD/CAM generated porcelain laminate veneers. After 9 years, they reported 94% survival rate.60 In another study after a mean monitoring period of 4 years, the failure-free rate was 96.3% one failure presented crown fracture after 2.8 years. Two abutments changed the sensibility from positive to negative within the first 13 months. Two abutment teeth revealed secondary caries below the crown margin.57
Attia et al. (2006) found that the cyclic loading fatigue significantly decrease the fracture loads of composite resin and all-ceramic crowns while adhesive cementation significantly expanded the fracture loads.61
CAD/CAM inlays had less cement thickness than laboratory-made inlays, but this was not related to their microleakage.62 A thinner film of cementation is recommended for Chair-side CAD/CAM ceramic restorations.63 In 2012, Kassem et al., found that composite crowns were more fatigue-resistant than ceramic crowns. Cement type had a significant effect on fatigue resistance of the ceramic crowns but not the composite ones. Microleakage scores of ceramic crowns cemented with PAN (Panavia-F-2.0) were significantly lower.64 Fasbinder et al. (2010) pointed out that there was no concrete change in the crowns during the 2 years study also there was no reported sensitivity at 1 or 2 years or crown fracture or surface chipping. For margin discoloration, the percentage Alfa score was 86.9% for crowns cemented with self-etching, dual-curing cement. All other percentage Alfa scores were greater than 92.0%.38
Conclusion
The application of CAD/CAM technology is promising for the delivery of high-quality devices in all fields of dentistry. It is esthetically pleasing, effective; time-saving and can be applied successfully in private practice. The way of producing and placing the restorations made with the chair-side CAD/CAM (CEREC and E4D) devices is better than restorations made by conventional laboratory procedures.
Footnotes
Conflicts of Interest: None
Source of Support: Nil
References
- 1.Mörmann WH. The origin of the Cerec method: a personal review of the first 5 years. Int J Comput Dent. 2004;7:11–24. [PubMed] [Google Scholar]
- 2.Mörmann WH. The evolution of the CEREC system. J Am Dent Assoc. 2006;137(Suppl):7S–13. doi: 10.14219/jada.archive.2006.0398. [DOI] [PubMed] [Google Scholar]
- 3.Lowe RA. CAD/CAM Dentistry and Chariside Digital Impression Making. [Last accessed on 2012 Aug]. Available from: http://www.ineedce.com .
- 4.Poticny DJ, Klim J. CAD/CAM in-office technology: innovations after 25 years for predictable, esthetic outcomes. J Am Dent Assoc. 2010;141(Suppl 2):5S–9. doi: 10.14219/jada.archive.2010.0356. [DOI] [PubMed] [Google Scholar]
- 5.Fasbinder DJ. The CEREC system: 25 years of chairside CAD/CAM dentistry. J Am Dent Assoc. 2010;141(Suppl 2):3S–4. doi: 10.14219/jada.archive.2010.0354. [DOI] [PubMed] [Google Scholar]
- 6.Roggendorf MJ, Kunzi B, Ebert J, Roggendorf HC, Frankenberger R, Reich SM. Seven-year clinical performance of CEREC-2 all-ceramic CAD/CAM restorations placed within deeply destroyed teeth. Clin Oral Investig. 2012;16(5):1413–24. doi: 10.1007/s00784-011-0642-8. [DOI] [PubMed] [Google Scholar]
- 7.Van Zeghbroeck L. CAD/CAM treatment for the elderly – a case report. Gerodontology. 2012;29(2):e1176–9. doi: 10.1111/j.1741-2358.2011.00521.x. [DOI] [PubMed] [Google Scholar]
- 8.Christensen GJ. In-office CAD/CAM milling of restorations: the future? J Am Dent Assoc. 2008;139(1):83–5. doi: 10.14219/jada.archive.2008.0025. [DOI] [PubMed] [Google Scholar]
- 9.Fasbinder DJ. Clinical performance of chairside CAD/CAM restorations. J Am Dent Assoc. 2006;137:22S–31. doi: 10.14219/jada.archive.2006.0395. [DOI] [PubMed] [Google Scholar]
- 10.Touchstone A, Nieting T, Ulmer N. Digital transition: the collaboration between dentists and laboratory technicians on CAD/CAM restorations. J Am Dent Assoc. 2010;141(Suppl 2):15S–9. doi: 10.14219/jada.archive.2010.0353. [DOI] [PubMed] [Google Scholar]
- 11.Santos GC, Jr, Santos MJ, Jr, Rizkalla AS, Madani DA, El-Mowafy O. Overview of CEREC CAD/CAM chairside system. Gen Dent. 2013;61(1):36–40. [PubMed] [Google Scholar]
- 12.Kwon SY, Kim Y, Ahn HW, Kim KB, Chung KR, Kim Sunny SH. Computer-Aided Designing and Manufacturing of Lingual Fixed Orthodontic Appliance Using 2D/3D Registration Software and Rapid Prototyping. Int J Dent. 2014;2014:164164. doi: 10.1155/2014/164164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ronay V, Sahrmann P, Bindl A, Attin T, Schmidlin PR. Current status and perspectives of mucogingival soft tissue measurement methods. J Esthet Restor Dent. 2011;23(3):146–56. doi: 10.1111/j.1708-8240.2011.00424.x. [DOI] [PubMed] [Google Scholar]
- 14.Mantri SS, Thombre RU, Pallavi D. Prosthodontic rehabilitation of a patient with bilateral auricular deformity. J Adv Prosthodont. 2011;3(2):101–5. doi: 10.4047/jap.2011.3.2.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Yuan FS, Sun YC, Wang Y, Lü PJ. Accuracy evaluation of a new three-dimensional reproduction method of edentulous dental casts, and wax occlusion rims with jaw relation. Int J Oral Sci. 2013;5(3):155–61. doi: 10.1038/ijos.2013.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Magne P, Schlichting LH, Maia HP, Baratieri LN. In vitro fatigue resistance of CAD/CAM composite resin and ceramic posterior occlusal veneers. J Prosthet Dent. 2010;104(3):149–57. doi: 10.1016/S0022-3913(10)60111-4. [DOI] [PubMed] [Google Scholar]
- 17.Schlichting LH, Maia HP, Baratieri LN, Magne P. Novel-design ultra-thin CAD/CAM composite resin and ceramic occlusal veneers for the treatment of severe dental erosion. J Prosthet Dent. 2011;105(4):217–26. doi: 10.1016/S0022-3913(11)60035-8. [DOI] [PubMed] [Google Scholar]
- 18.Vichi A, Sedda M, Del Siena F, Louca C, Ferrari M. Flexural resistance of Cerec CAD/CAM system ceramic blocks. Part 1: Chairside materials. Am J Dent. 2013;26(5):255–9. [PubMed] [Google Scholar]
- 19.Chen C, Trindade FZ, de Jager N, Kleverlaan CJ, Feilzer AJ. The fracture resistance of a CAD/CAM Resin Nano Ceramic (RNC) and a CAD ceramic at different thicknesses. Dent Mater. 2014;30(9):954–62. doi: 10.1016/j.dental.2014.05.018. [DOI] [PubMed] [Google Scholar]
- 20.Batson ER, Cooper LF, Duqum I, Mendonça G. Clinical outcomes of three different crown systems with CAD/CAM technology. J Prosthet Dent. 2014;112(4):770–7. doi: 10.1016/j.prosdent.2014.05.002. [DOI] [PubMed] [Google Scholar]
- 21.Sjögren G, Molin M, van Dijken JW. A 10-year prospective evaluation of CAD/CAM-manufactured (Cerec) ceramic inlays cemented with a chemically cured or dual-cured resin composite. Int J Prosthodont. 2004;17(2):241–6. [PubMed] [Google Scholar]
- 22.Galhano GÁ, Pellizzer EP, Mazaro JV. Optical impression systems for CAD-CAM restorations. J Craniofac Surg. 2012;23(6):e575–9. doi: 10.1097/SCS.0b013e31826b8043. [DOI] [PubMed] [Google Scholar]
- 23.Seelbach P, Brueckel C, Wöstmann B. Accuracy of digital and conventional impression techniques and workflow. Clin Oral Investig. 2013;17(7):1759–64. doi: 10.1007/s00784-012-0864-4. [DOI] [PubMed] [Google Scholar]
- 24.Yuzbasioglu E, Kurt H, Turunc R, Bilir H. Comparison of digital and conventional impression techniques: evaluation of patients’ perception, treatment comfort, effectiveness and clinical outcomes. BMC Oral Health. 2014;14:10. doi: 10.1186/1472-6831-14-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ender A, Mehl A. In-vitro evaluation of the accuracy of conventional and digital methods of obtaining full-arch dental impressions. Quintessence Int. 2015;46(1):9–17. doi: 10.3290/j.qi.a32244. [DOI] [PubMed] [Google Scholar]
- 26.Lee SJ, Macarthur RX, 4th, Gallucci GO. An evaluation of student and clinician perception of digital and conventional implant impressions. J Prosthet Dent. 2013;110(5):420–3. doi: 10.1016/j.prosdent.2013.06.012. [DOI] [PubMed] [Google Scholar]
- 27.Svanborg P, Skjerven H, Carlsson P, Eliasson A, Karlsson S, Ortorp A. Marginal and internal fit of cobalt-chromium fixed dental prostheses generated from digital and conventional impressions. Int J Dent. 2014;2014:534382. doi: 10.1155/2014/534382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Neves FD, Prado CJ, Prudente MS, Carneiro TA, Zancopé K, Davi LR, et al. Micro-computed tomography evaluation of marginal fit of lithium disilicate crowns fabricated by using chairside CAD/CAM systems or the heat-pressing technique. J Prosthet Dent. 2014;112(5):1134–40. doi: 10.1016/j.prosdent.2014.04.028. [DOI] [PubMed] [Google Scholar]
- 29.Mously HA, Finkelman M, Zandparsa R, Hirayama H. Marginal and internal adaptation of ceramic crown restorations fabricated with CAD/CAM technology and the heat-press technique. J Prosthet Dent. 2014;112(2):249–56. doi: 10.1016/j.prosdent.2014.03.017. [DOI] [PubMed] [Google Scholar]
- 30.Song TJ, Kwon TK, Yang JH, Han JS, Lee JB, Kim SH, et al. Marginal fit of anterior 3-unit fixed partial zirconia restorations using different CAD/CAM systems. J Adv Prosthodont. 2013;5(3):219–25. doi: 10.4047/jap.2013.5.3.219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kohorst P, Brinkmann H, Li J, Borchers L, Stiesch M. Marginal accuracy of four-unit zirconia fixed dental prostheses fabricated using different computer-aided design/computer-aided manufacturing systems. Eur J Oral Sci. 2009;117(3):319–25. doi: 10.1111/j.1600-0722.2009.00622.x. [DOI] [PubMed] [Google Scholar]
- 32.Guess PC, Strub JR, Steinhart N, Wolkewitz M, Stappert CF. All-ceramic partial coverage restorations – midterm results of a 5-year prospective clinical splitmouth study. J Dent. 2009;37(8):627–37. doi: 10.1016/j.jdent.2009.04.006. [DOI] [PubMed] [Google Scholar]
- 33.Romeo E, Iorio M, Storelli S, Camandona M, Abati S. Marginal adaptation of full-coverage CAD/CAM restorations: in vitro study using a non-destructive method. Minerva Stomatol. 2009;58(3):61–72. [PubMed] [Google Scholar]
- 34.Tsitrou EA, van Noort R. Minimal preparation designs for single posterior indirect prostheses with the use of the Cerec system. Int J Comput Dent. 2008;11(3-4):227–40. [PubMed] [Google Scholar]
- 35.Tsitrou EA, Helvatjoglu-Antoniades M, van Noort R. A preliminary evaluation of the structural integrity and fracture mode of minimally prepared resin bonded CAD/CAM crowns. J Dent. 2010;38(1):16–22. doi: 10.1016/j.jdent.2009.07.003. [DOI] [PubMed] [Google Scholar]
- 36.Yildiz C, Vanlioglu BA, Evren B, Uludamar A, Kulak-Ozkan Y. Fracture resistance of manually and CAD/CAM manufactured ceramic onlays. J Prosthodont. 2013;22(7):537–42. doi: 10.1111/jopr.12037. [DOI] [PubMed] [Google Scholar]
- 37.D’Arcy BL, Omer OE, Byrne DA, Quinn F. The reproducibility and accuracy of internal fit of Cerec 3D CAD/CAM all ceramic crowns. Eur J Prosthodont Restor Dent. 2009;17(2):73–7. [PubMed] [Google Scholar]
- 38.Fasbinder DJ, Dennison JB, Heys D, Neiva G. A clinical evaluation of chairside lithium disilicate CAD/CAM crowns: a two-year report. J Am Dent Assoc. 2010;141(Suppl 2):10S–4. doi: 10.14219/jada.archive.2010.0355. [DOI] [PubMed] [Google Scholar]
- 39.Nash RW. Resurfacing tooth structure with ceramic laminates. Dent Today. 2014;33(8):68–71. [PubMed] [Google Scholar]
- 40.Almeida e Silva JS, Erdelt K, Edelhoff D, Araújo É, Stimmelmayr M, Vieira LC, et al. Marginal and internal fit of four-unit zirconia fixed dental prostheses based on digital and conventional impression techniques. Clin Oral Investig. 2014;18:515–23. doi: 10.1007/s00784-013-0987-2. [DOI] [PubMed] [Google Scholar]
- 41.Tidehag P, Ottosson K, Sjögren G. Accuracy of ceramic restorations made using an in-office optical scanning technique: an in vitro study. Oper Dent. 2014;39(3):308–16. doi: 10.2341/12-309-L. [DOI] [PubMed] [Google Scholar]
- 42.Alghazzawi TF, Liu PR, Essig ME. The effect of different fabrication steps on the marginal adaptation of two types of glass-infiltrated ceramic crown copings fabricated by CAD/CAM technology. J Prosthodont. 2012;21(3):167–72. doi: 10.1111/j.1532-849X.2011.00803.x. [DOI] [PubMed] [Google Scholar]
- 43.Keul C, Stawarczyk B, Erdelt KJ, Beuer F, Edelhoff D, Güth JF. Fit of 4-unit FDPs made of zirconia and CoCr-alloy after chairside and labside digitalization – a laboratory study. Dent Mater. 2014;30(4):400–7. doi: 10.1016/j.dental.2014.01.006. [DOI] [PubMed] [Google Scholar]
- 44.Miyazaki T, Hotta Y. CAD/CAM systems available for the fabrication of crown and bridge restorations. Aust Dent J. 2011;56(Suppl 1):97–106. doi: 10.1111/j.1834-7819.2010.01300.x. [DOI] [PubMed] [Google Scholar]
- 45.Ender A, Mehl A. Full arch scans: conventional versus digital impressions – an in-vitro study. Int J Comput Dent. 2011;14(1):11–21. [PubMed] [Google Scholar]
- 46.Tamim H, Skjerven H, Ekfeldt A, Rønold HJ. Clinical evaluation of CAD/CAM metal-ceramic posterior crowns fabricated from intraoral digital impressions. Int J Prosthodont. 2014;27(4):331–7. doi: 10.11607/ijp.3607. [DOI] [PubMed] [Google Scholar]
- 47.Euán R, Figueras-Álvarez O, Cabratosa-Termes J, Oliver-Parra R. Marginal adaptation of zirconium dioxide copings: influence of the CAD/CAM system and the finish line design. J Prosthet Dent. 2014;112(2):155–62. doi: 10.1016/j.prosdent.2013.10.012. [DOI] [PubMed] [Google Scholar]
- 48.Renne W, McGill ST, Forshee KV, DeFee MR, Mennito AS. Predicting marginal fit of CAD/CAM crowns based on the presence or absence of common preparation errors. J Prosthet Dent. 2012;108(5):310–5. doi: 10.1016/S0022-3913(12)60183-8. [DOI] [PubMed] [Google Scholar]
- 49.Souza RO, Özcan M, Pavanelli CA, Buso L, Lombardo GH, Michida SM, et al. Marginal and internal discrepancies related to margin design of ceramic crowns fabricated by a CAD/CAM system. J Prosthodont. 2012;21(2):94–100. doi: 10.1111/j.1532-849X.2011.00793.x. [DOI] [PubMed] [Google Scholar]
- 50.Euán R, Figueras-Álvarez O, Cabratosa-Termes J, Brufau-de BarberàM, Gomes-Azevedo S. Comparison of the marginal adaptation of zirconium dioxide crowns in preparations with two different finish lines. J Prosthodont. 2012;21(4):291–5. doi: 10.1111/j.1532-849X.2011.00831.x. [DOI] [PubMed] [Google Scholar]
- 51.Zamboni SC, Nogueira L, Bottino MA, Sobrinho LC, Valandro LF. The effect of mechanical loading on the cusp defection of premolars restored with direct and indirect techniques. J Contemp Dent Pract. 2014;15(1):75–81. doi: 10.5005/jp-journals-10024-1191. [DOI] [PubMed] [Google Scholar]
- 52.Arocha MA, Basilio J, Llopis J, Di Bella E, Roig M, Ardu S, et al. Colour stainability of indirect CAD-CAM processed composites vs. conventionally laboratory processed composites after immersion in staining solutions. J Dent. 2014;42(7):831–8. doi: 10.1016/j.jdent.2014.04.002. [DOI] [PubMed] [Google Scholar]
- 53.Salameh Z, Tehini G, Ziadeh N, Ragab HA, Berberi A, Aboushelib MN. Influence of ceramic color and translucency on shade match of CAD/CAM porcelain veneers. Int J Esthet Dent. 2014;9(1):90–7. [PubMed] [Google Scholar]
- 54.Bosch G, Ender A, Mehl A. A 3-dimensional accuracy analysis of chairside CAD/CAM milling processes. J Prosthet Dent. 2014;112(6):1425–31. doi: 10.1016/j.prosdent.2014.05.012. [DOI] [PubMed] [Google Scholar]
- 55.Reich S, Fischer S, Sobotta B, Klapper HU, Gozdowski S. A preliminary study on the short-term efficacy of chairside computer-aided design/computer-assisted manufacturing- generated posterior lithium disilicate crowns. Int J Prosthodont. 2010;23(3):214–6. [PubMed] [Google Scholar]
- 56.Reich S, Endres L, Weber C, Wiedhahn K, Neumann P, Schneider O, et al. Three-unit CAD/CAM-generated lithium disilicate FDPs after a mean observation time of 46 months. Clin Oral Investig. 2014;18(9):2171–8. doi: 10.1007/s00784-014-1191-8. [DOI] [PubMed] [Google Scholar]
- 57.Reich S, Schierz O. Chair-side generated posterior lithium disilicate crowns after 4 years. Clin Oral Investig. 2013;17(7):1765–72. doi: 10.1007/s00784-012-0868-0. [DOI] [PubMed] [Google Scholar]
- 58.Wittneben JG, Wright RF, Weber HP, Gallucci GO. A systematic review of the clinical performance of CAD/CAM single-tooth restorations. Int J Prosthodont. 2009;22(5):466–71. [PubMed] [Google Scholar]
- 59.Otto T, Schneider D. Long-term clinical results of chairside Cerec CAD/CAM inlays and onlays: a case series. Int J Prosthodont. 2008;21(1):53–9. [PubMed] [Google Scholar]
- 60.Wiedhahn K, Kerschbaum T, Fasbinder DF. Clinical long-term results with 617 Cerec veneers: a nine-year report. Int J Comput Dent. 2005;8(3):233–46. [PubMed] [Google Scholar]
- 61.Attia A, Abdelaziz KM, Freitag S, Kern M. Fracture load of composite resin and feldspathic all-ceramic CAD/CAM crowns. J Prosthet Dent. 2006;95(2):117–23. doi: 10.1016/j.prosdent.2005.11.014. [DOI] [PubMed] [Google Scholar]
- 62.Alaghemand H, Abolghasemzadeh F, Pakdel F, Judi Chelan R. Comparison of microleakage and thickness of resin cement in ceramic inlays with various temperatures. J Dent Res Dent Clin Dent Prospects. 2014;8(1):45–50. doi: 10.5681/joddd.2014.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Dong YT, Wang XY, Gao XJ. Effect of cementation on fracture toughness of chair-side CAD/CAM ceramic. Beijing Da Xue Xue Bao. 2012;44(2):299–302. [PubMed] [Google Scholar]
- 64.Kassem AS, Atta O, El-Mowafy O. Fatigue resistance and microleakage of CAD/CAM ceramic and composite molar crowns. J Prosthodont. 2012;21(1):28–32. doi: 10.1111/j.1532-849X.2011.00773.x. [DOI] [PubMed] [Google Scholar]