

Abstract
Background:
This study aimed at investigating the impact of an educational intervention based on transtheoretical model to increase physical activity and improve metabolic syndrome indicators in women.
Methods:
In this quasi-experimental study, 142 women with metabolic syndrome were randomly assigned to the case and control group (each group 71 participants). SECQ (Marcus), processes of change (Marcus), decisional balance (Bandura) and self-efficacy (Nigg) questionnaires and International Physical Activities Standard Questionnaire in preintervention, 3 and 6 months after intervention were completed. Furthermore, abdominal obesity, triglycerides (TG), and high-density lipoprotein (HDL) were measured. Physical activity intervention based on transtheoretical model (TTM) was performed in the case group. Finally, data were analyzed by SPSS (16) (SPSS Inc., Chicago, IL, USA) and repeated measure ANOVA, independent t-test and Freidman was used. A two-tailed P value, lower than 0.05, was considered to be statistically significant.
Results:
After the intervention, physical activity level increased in the intervention group, and they also progressed in stages of change, but the people in the control group had regressed. All changes in TTM constructs were significant in the intervention group during the time and differences in pros and cons were not significant in the control group. Abdominal obesity and TG has significantly reduced, and HDL has increased in the intervention group. In the control group, there was a significant increase in TGs and a decrease in HDL.
Conclusions:
Physical activity training based on TTM can improve physical activity and metabolic syndrome indicators in women.
Keywords: Decisional balance, metabolic syndrome, physical activity, process of change, self-efficacy, stage of change, transtheoretical
INTRODUCTION
Metabolic syndrome is a group of risk factors, including obesity, resistance to insulin, serum fat disorders, and hypertension, for noncommunicable diseases such as cardiovascular diseases and type 2 diabetes mellitus.[1]
According to the definition by Adults Treatment Panel (ATP III), existence of three or more risk factors is referred to as “metabolic syndrome”.[2]
Abdominal obesity, according to waist size of men to be > 120 cm and of women: >88 cm
Serum triglyceride (TG): >150 mg/dl
Serum high-density lipoprotein (HDL) for men: <40 mg/dl and for women: <50 mg/dl
Blood pressure: >130/85
Consuming the medicine for reducing blood sugar or anti-hypertension medicine or the rate of blood sugar before breakfast: >110 mg/dl.
The literature indicate that the presence of metabolic syndrome increases the risk of cardiovascular diseases and type II diabetes.[3,4,5,6,7,8] Furthermore, the people affected by this syndrome are exposed to a higher risk of death from cardiovascular diseases and death due to every other cause.[9] In general, the death increases 20–80% due to the metabolic syndrome.[10]
Cross-sectional and prospective studies have reported various data about prevalence and immergence of this syndrome that are different with regards to their definitions.[11,12] Prevalence of metabolic syndrome is reported to be 43.5% in 60 years of age and older in the U.S.A.[13] Prevalence of this disease is also high in Spanish and American-African individuals.[14]
Prevalence of this disease is also increasing in Asia.[15] The prevalence of MS is 36% in Korean people aged from 30 to 79 years and also it is higher in Taiwanese Women (56.7%) followed by Taiwanese men (43.3%).[16,17] According to selected studies and the definitions by ATP, prevalence of metabolic syndrome is estimated to be 33.2% in Iran.[18] Different studies in Iran have reported that the prevalence of the MS in Iranian women is higher than men. Sarrafzadegan et al. found that the prevalence of metabolic syndrome in Iranian women is 35.1% and 10.7% in men[19] and Ghorbani's study have also indicated the prevalence of MS is higher in Iranian women than men.[20] Extensive prevalence of this disease has made different countries to propose different approaches for its prevention and consistent control, with the aim to gradually reduce the main risk factors of this disease and interventions for improving nutrition and increasing physical activities have been in prior plans considered in this regard. The results of fulfilled interventions have shown that changing the lifestyle by emphasis on increasing physical activities has been effective in reducing the prevalence of metabolic syndrome and other risk factors for cardiovascular diseases.[21,22]
Nowadays, several studies have indicated that the physical activity interventions could successfully reduce metabolic syndrome.[23,24,25] It has also been defined that theoretical-based physical activity interventions are preferred to traditional and conventional interventions.[26,27,28] Theories and models are considered as the basis for the interventions, by which the intervening effects could be measured, and the relevant behaviors predicted.
In fact, the theories identify the main factors that influence the behavior and relationships between these factors. Therefore, they are useful in identifying the elements that should be more focus on interventions.
One of the most popular models for studying physical activity behavior is the transtheoretical model (TTM) and researches support the use of this model of behavior change because it is a simple and effective model for classifying the target population to be intervened and planned for.
This model indicates that an individual would have extensive efforts before having success in changing the physical activity behavior to pass from the stages of change. The relations of these stages with other structures include processes of change, self-efficacy, and decision-making balance.[29] The stages of change in the mentioned model are as follows:
Precontemplation stage: The individuals who are at this stage have no present or the future (up to 6 months) intentions to change or make decisions for their health behaviors
Contemplation stage: The individuals who are at this stage have apparent present or the future (up to 6 months) intentions to change behaviors
Preparation stage: The people at this stage have the intention to change their attitudes in the near future (generally 30 days)
Action stage: The individual will clearly have changes in his/her behaviors in 6 months
Maintenance stage: To avoid returning, the person has peculiar efforts. The duration of this stage is variable according to the behavior and is more than 6 months.[30]
The second structured model includes the processes of change, consisted of activities and strategies that help the individuals to proceed in the stages of change. It is categorized into cognitive and behavioral processes.
The third structured model between the conceptual advantages for deciding for a new behavior and the problems or obstacles in deciding for a new behavior (pros and cons) is referred to as decision-making balance. When the pros are more than cons, the transformation is done from precontemplation to contemplation stages.[31] The fourth structured model is self-efficacy that is derived from Bandura's theory.[32]
So far, the TTM has been successfully applied on different groups such as students, affected people by hypertension, diabetes, osteoporosis, and cancer, but this model has not yet been used in women with metabolic syndrome in the city of Esfahan.[26,27,33,34,35,36] Hence, this study aimed at investigating the impact of an educational intervention based on transtheoretical model to increase physical activity and improve the metabolic syndrome’ indicators in women with symptoms of metabolic syndrome.
METHODS
Study design and participants
This quasi-experimental study was done on 142 women with metabolic syndrome in the city of Esfahan (2013) in the first phase of the study two urban health centers were randomly selected and placed into the case and control group finally, individuals are randomly assigned to intervention and comparison groups Ability to read and write, marriage, lack of medical prohibition for physical activities, affected by metabolic syndrome and placement of the participant in the contemplation, preparation, and action stages for doing physical activities according to the stages of change were the criteria for inclusion to the study. The criteria for leaving the study included a lack of desire to participation and medical prohibition for physical activities.
The number of participants for each of the intervention and control groups was 71 that with regards to 20% of loss of participants, they were 28 people for the precontemplation stage, 23 people for the preparation stage, and 20 people for the action stage. Informed consent form was assigned by all participants too.
Variable assessment and study instruments
In addition to demographic information such as age, level of education, history of disease, and number of children, level of physical activity, abdominal obesity, TG, and HDL were also collected using a multi-part questionnaire, as follows:
First questionnaire
International Physical Activities Standard Questionnaire. Three types of questions are asked in this questionnaire about intense and intermediate activities and walking, and the participant identifies the performed action in each group in days per week and minutes per day basis. Finally, the total physical activities (in metabolic equivalents [METS]) were obtained as the total intense physical activities *8, intermediate physical activities *4 and walking *3.3.[37]
Second questionnaire
It is a 5-item questionnaire for determining change processes stage of exercise change questionnaire (SECQ), prepared by Marcus et al.[38] There is a question in this questionnaire that is asked from individuals whether they have regular physical activities or not! Finally, according to the selections, the participant would be placed in the stages (precontemplation, contemplation, preparation, action, and maintenance).
Third questionnaire
It is the processes of change questionnaire, prepared by Marcus et al.[39] This questionnaire includes 40 items in cognitive and behavioral strategies and the selecting answers include: Never, rarely, sometimes, often, and always and 0–4 scores will be given to each item, respectively.
Fourth questionnaire
This questionnaire is for measuring the structure of decision-making balance. It includes 43 items defined by 4-scaled criteria (from “I quite disagree” to “I totally agree”). Zero to 3 scores is given to each item, respectively.
Fifth questionnaire
It is prepared to identify self-efficacy and consists of 16 items with 4 scales (from “not quite sure” to “I’m quite sure”). Zero to 30 scores is given to each item, respectively.[41]
After translation and back-translation processes, the questionnaires were given to experts to determine the reliability measures. After obtaining their views, the CVI index was obtained for each questionnaire. It was then given to a group of 30 women who did not enter the study, to determine the validity of the questionnaire. The value for Cronbach's alpha was 0.84 for decisional making, 0.77 for the self-efficacy and 0.91 for change processes.
This study was done in three stages: Before the intervention, 3 months after intervention and 6 months after intervention. After obtaining the required samples for each stage of change in the first stage, the samples were introduced to a laboratory for the blood test (TG and HDL). The questionnaires were completed in self-administered method and the measures such as abdominal obesity were also determined. Then, the educational interventions were designed and implemented for subjects in different stages (contemplation, preparation, and action), according to Table 1 in the intervention group.
Table 1.
Applied strategies in the stages of change (contemplation, preparation, and action)
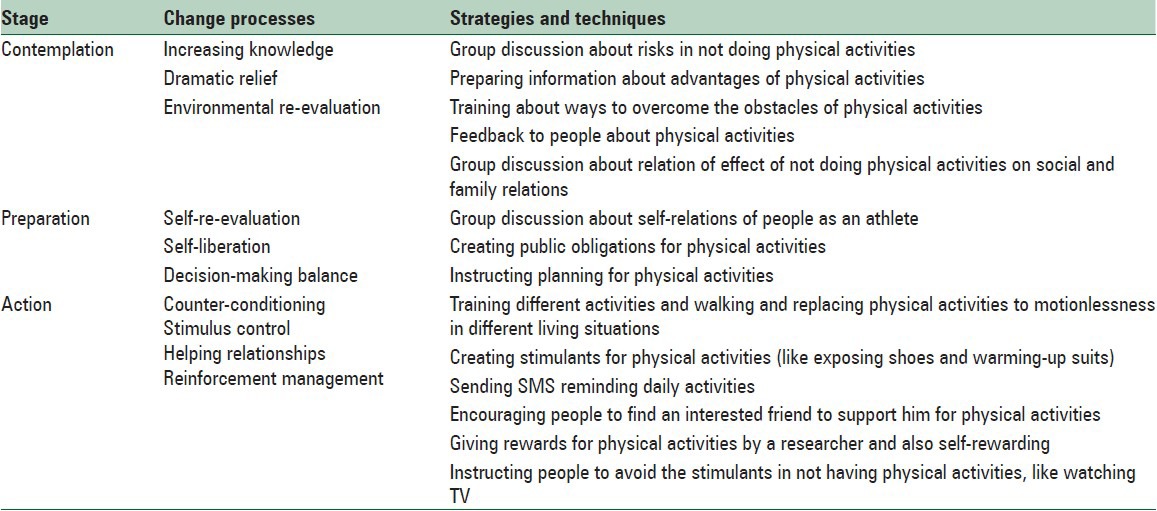
The emphasis of the intervention differed in each group depending on the stage. The interventions about physical activities included educational sessions by experienced coach in 5 sessions (each session, 60 min), these sessions held in health center and local park. Different warming-up exercises, enduring exercises, flexibility, and balancing, energetic and contraction exercises were instructed in the first session and the way to walk properly was also trained to the women. Finally, a DVD (author-made) including the training instructions regarding physical activity was given to every woman.
Three months after intervention in the second stage of the study, the questionnaires were filled, and a TG and HDL level were measured again. A training session was also held in the third stage for the control group in the health center, and all of the relevant resources regarding physical activity were given to individuals in the intervention group. Physical activity levels and all of the mentioned variables were measured using the same procedure as at baseline and all of the postintervention stages (3 and 6 months after intervention).
Statistical analysis
Data analysis was performed using SPSS 16 software (SPSS Inc., Chicago, IL, USA) by using descriptive statistics such as mean, standard deviation, and analytical statistics such as, repeated measure ANOVA and independent t-test were used for comparing the changes between the two groups in each stage.
Friedman test was used for comparing the qualitative variables (stages of change) in each of the control and intervention groups. A two-tailed P value, lower than 0.05, was considered to be statistically significant.
RESULTS
Totally, 142 women with metabolic syndrome participated in the study with the average age of 52.49 ± 5.46 for the case group and mean of age was 50.91 ± 6.08 for the control group and the independent t-test showed that the mean of age has no significant differences, statistically.
Regarding education, 53 women (74.6%) in the case group had only high school education but not the diploma, and the rest were high school certificates. Chi-square test showed that no significant difference exists for the education between the two groups.
The placement of people according to the stages of change prior to intervention in both groups was such that 28 (39.4%) people were in the contemplation stage, 24 women (33.8%) were in preparation stage, and 19 people (26.8%) were in action stage. The changes during the stages of 3 and 6 months after intervention could be observed in Table 2. Friedman test showed that the occurred changes during the period are significant for both the case and control groups.
Table 2.
Distribution of participants in stages of change, 3 and 6 months after intervention for case and control groups

The mean of physical activity in case and control group was 225/98 ± 370/55 METS and 203/86 ± 349/55, respectively, in preintervention. Independent t-test showed there were no significant differences between two groups.
Three months after the intervention, the mean of physical activity has increased in the intervention group (748/29 ± 696/95), and 6 months after the intervention was 863/44 ± 809/43. Repeated measure ANOVA showed no statistically significant difference in times (f = 29.159, P = 000).
Three and six months after the intervention, the means of physical activity had decreased 174/44 ± 442/09and 152/15 ± 346/86, respectively, in the control group.
Repeated measure ANOVA showed no statistically significant difference in times (f = 1.368, P = 0.266) [Figure 1].
Figure 1.
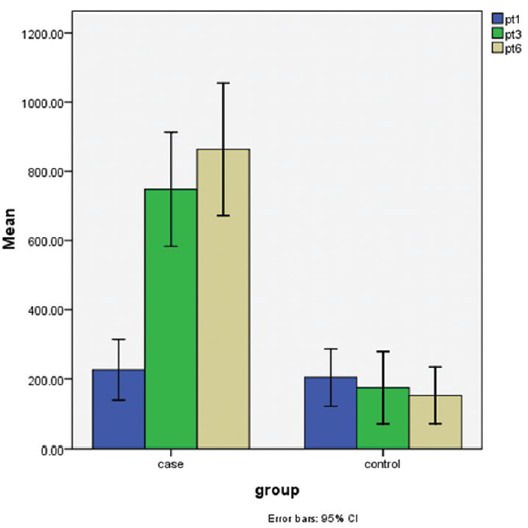
The mean of physical activity level in preintervention, 3 and 6 months after intervention for case and control group
The ANOVA test showed the means of processes of change, self-efficacy, pros, and cons were significant in the intervention group. But, the mean of pros and cons was not significant in the control group [Table 3].
Table 3.
Comparison of TTM structure means in preintervention, 3 and 6 months after intervention for case and control groups

In intervention group, physical activity has also increased 3 and 6 months after intervention, however, in the control group has been decreased. Figure 1 shows these differences.
Regarding the related measures with serum lipids, TG and HDL changes were significant in the intervention group but, the changes in the control group were not significant [Figures 2 and 3].
Figure 2.
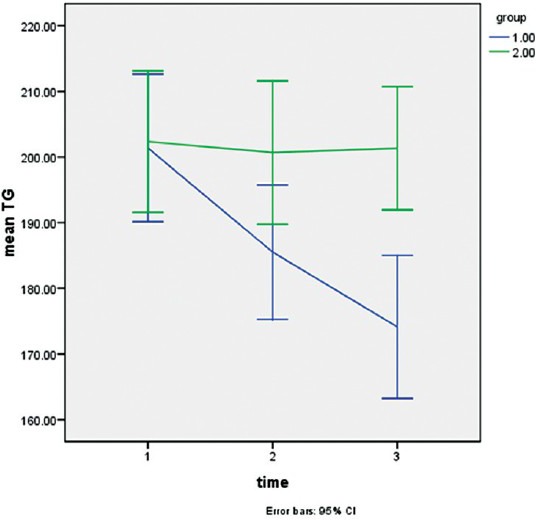
The mean of triglycerides level in preintervention, 3 and 6 months after intervention for case and control group
Figure 3.
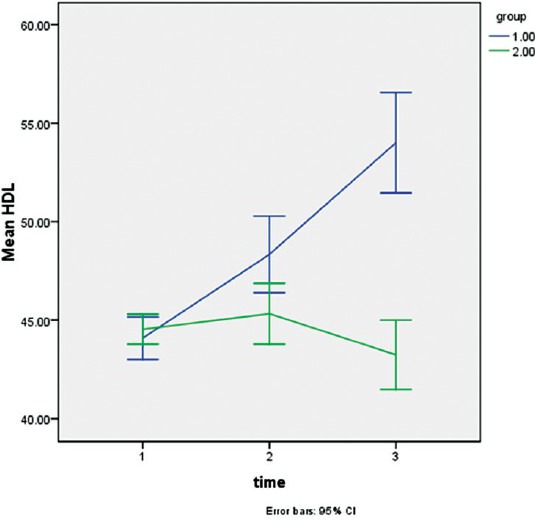
The mean of high-density lipoprotein level in preintervention, 3 and 6 months after intervention for case and control group
In Figure 4, the changes occurred in abdominal fat are definite for both groups during the relevant time. ANOVA test showed that the changes for the intervention groups were significant.
Figure 4.
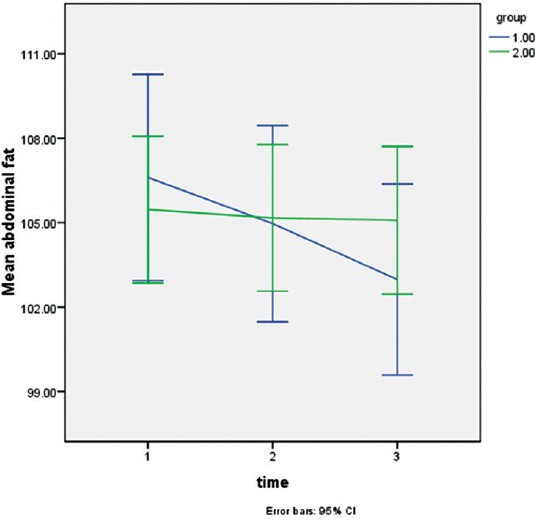
The mean of abdominal fat in preintervention, 3 and 6 months after intervention for case and control group
DISCUSSION
This study was done with the aim of determining the application of the TTM to physical activity in women with metabolic syndrome in Isfahan city.
After 3 months, in the present study, a high rate of people in the intervention group were in the preparation and action stages for the physical activities, and the trend was continued 6 months after intervention. The development in the change stages is in consisting with the studies by Lach et al.[42,43,44] Following transformations in the changes in the stages, increasing physical activities was also observed, such that the findings showed that the people in the intervention group had positive changes in physical activities, 3 and 6 months after intervention. The findings indicate that the intervention based on TTM together with instructing physical activities could be effective in the moving of people toward more active life. The positive effects due to using this model are in consist with the studies done by Opender, Dallow, Kirk, and Speck.[28,45,46,47] On the other hand, no significant difference was observed in the level of individuals’ physical activities, after 6 months from intervention in Tabatabaei's study. It is worth to notify that they did not apply any model in their intervention.[48]
Moreover, giving instructing DVDs and providing instructions for correct ways of exercising have led to increasing physical activity in women and majority of them have also been placed in action group. This caused most of the activities to be done at home and the barriers such as time, shortage of resources, lack of necessary skill and fatigue, referred in different studies as the most important reasons of not having exercises, to be overcome.[49,50,51]
In addition to increasing physical activities, increase in the processes of changes was also observed in the intervention group and ANOVA test has shown the changes from the beginning to 3 and 6 months after intervention to be significant. Since the intervention was based on the TTM and the instructing people for health have used these processes in their teachings, it is clear that positive changes are created in the intervention group and people use these strategies for changing their attitudes and stabilizing their behaviors. This finding is consist with the finding by Moeini study that was done on the women affected by type II diabetes.[26]
Another effective factor in behavioral changes is self-efficacy, defined as an assurance that people have with regards to their capabilities in confronting with a risking situation. The mean of self-efficacy rate is also increased in time, in this study. This finding is consist with the finding by Dallow.[27]
The mean of the pros showed a significant increase in the intervention group, in this study. This finding is similar to other studies fulfilled about physical activity.[52] In contrast to the increase in the average conceptual advantages, a significant decrease in the hindrances is also observed in the experimental group. This finding is consist with the studies by Gorely and Mohammadi-Zeidi.[53,54]
Regarding the considered measures in this research, TG level showed a significant decrease in the intervention group that is consist with the study by Yoo et al.,[55] but not in consist with the results concluded by Shahrjerdi, et al.[56,57,58,59] It seems that the differences are because of different exploiting times of each investigation and the types of trained physical activities.
High-density lipoprotein is also the other measure factor that has had a significant increase during the intervention. This is consist with the findings of Gerstel et al. and Dutheil.[24,25]
Following the reduction of serum fat, abdominal obesity had a significant decrease in the passage of time, in the intervention group. It is consist with various studies in this regard.[59,60] The measuring ratio of waist to hip was not significant after enduring exercises, in the study by Nikpour et al., and he considered the insignificance due to short exercising time and not controlling the diet.[61]
Research limitations
This study required completion of the questionnaires in three different periods, and since the number of questions was too many, it was time-consuming. Almost to the end, the participants showed no inclination to fill the questionnaires. On the other hand, the physical activities were measured and considered only through the questionnaire that was completed in a self-administered method. Thus, it seems that brief questionnaires and more subjective tools such as pedometers should be used in considering physical activities, in the future. It is recommended that in future studies, five groups of people are entered, and results are compared with them.
CONCLUSIONS
According to the obtained results, it was defined that training physical exercises according to TTM increases physical activities in women affected by metabolic syndrome and improving abdominal indices, TG, and HDL. Thus, this model could be used to train such people for treatments or even preventing a lot of chronic and cardiovascular diseases.
ACKNOWLEDGEMENTS
This study was granted by the Isfahan University of Medical Sciences, Isfahan, Iran. This was a Ph. D degree thesis approved in the school of health by thesis no: 392283.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Dumith SC, Gigante DP, Domingues MR. Stages of change for physical activity in adults from Southern Brazil: A population-based survey. Int J Behav Nutr Phys Act. 2007;4:25. doi: 10.1186/1479-5868-4-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Alberti KG, Zimmet P, Shaw J IDF Epidemiology Task Force Consensus Group. The metabolic syndrome – A new worldwide definition. Lancet. 2005;366:1059–62. doi: 10.1016/S0140-6736(05)67402-8. [DOI] [PubMed] [Google Scholar]
- 3.Gami AS, Witt BJ, Howard DE, Erwin PJ, Gami LA, Somers VK, et al. Metabolic syndrome and risk of incident cardiovascular events and death: A systematic review and meta-analysis of longitudinal studies. J Am Coll Cardiol. 2007;49:403–14. doi: 10.1016/j.jacc.2006.09.032. [DOI] [PubMed] [Google Scholar]
- 4.Dekker JM, Girman C, Rhodes T, Nijpels G, Stehouwer CD, Bouter LM, et al. Metabolic syndrome and 10-year cardiovascular disease risk in the Hoorn Study. Circulation. 2005;112:666–73. doi: 10.1161/CIRCULATIONAHA.104.516948. [DOI] [PubMed] [Google Scholar]
- 5.Lorenzo C, Williams K, Hunt KJ, Haffner SM. The National Cholesterol Education Program – Adult Treatment Panel III, International Diabetes Federation, and World Health Organization definitions of the metabolic syndrome as predictors of incident cardiovascular disease and diabetes. Diabetes Care. 2007;30:8–13. doi: 10.2337/dc06-1414. [DOI] [PubMed] [Google Scholar]
- 6.Malik S, Wong ND, Franklin SS, Kamath TV, L’Italien GJ, Pio JR, et al. Impact of the metabolic syndrome on mortality from coronary heart disease, cardiovascular disease, and all causes in United States adults. Circulation. 2004;110:1245–50. doi: 10.1161/01.CIR.0000140677.20606.0E. [DOI] [PubMed] [Google Scholar]
- 7.Hunt KJ, Resendez RG, Williams K, Haffner SM, Stern MP. San Antonio Heart Study. National Cholesterol Education Program versus World Health Organization metabolic syndrome in relation to all-cause and cardiovascular mortality in the San Antonio Heart Study. Circulation. 2004;110:1251–7. doi: 10.1161/01.CIR.0000140762.04598.F9. [DOI] [PubMed] [Google Scholar]
- 8.Girman CJ, Rhodes T, Mercuri M, Pyörälä K, Kjekshus J, Pedersen TR, et al. The metabolic syndrome and risk of major coronary events in the Scandinavian Simvastatin Survival Study (4S) and the Air Force/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS) Am J Cardiol. 2004;93:136–41. doi: 10.1016/j.amjcard.2003.09.028. [DOI] [PubMed] [Google Scholar]
- 9.Sundström J, Risérus U, Byberg L, Zethelius B, Lithell H, Lind L. Clinical value of the metabolic syndrome for long term prediction of total and cardiovascular mortality: Prospective, population based cohort study. BMJ. 2006;332:878–82. doi: 10.1136/bmj.38766.624097.1F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ford ES. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: A summary of the evidence. Diabetes Care. 2005;28:1769–78. doi: 10.2337/diacare.28.7.1769. [DOI] [PubMed] [Google Scholar]
- 11.Isomaa B, Almgren P, Tuomi T, Forsén B, Lahti K, Nissén M, et al. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care. 2001;24:683–9. doi: 10.2337/diacare.24.4.683. [DOI] [PubMed] [Google Scholar]
- 12.Munakata M, Honma H, Akasi M, Araki T, Kawamura T, Kubota M, et al. Japanese study to organize proper lifestyle modifications for metabolic syndrome (J-STOP-MetS): Design and method. Vasc Health Risk Manag. 2008;4:415–20. doi: 10.2147/vhrm.s1932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: Findings from the third National Health and Nutrition Examination Survey. JAMA. 2002;287:356–9. doi: 10.1001/jama.287.3.356. [DOI] [PubMed] [Google Scholar]
- 14.Ford ES, Li C, Zhao G. Prevalence and correlates of metabolic syndrome based on a harmonious definition among adults in the US. J Diabetes. 2010;2:180–93. doi: 10.1111/j.1753-0407.2010.00078.x. [DOI] [PubMed] [Google Scholar]
- 15.Lim S, Shin H, Song JH, Kwak SH, Kang SM, Won Yoon J, et al. Increasing prevalence of metabolic syndrome in Korea: The Korean National Health and Nutrition Examination Survey for 1998-2007. Diabetes Care. 2011;34:1323–8. doi: 10.2337/dc10-2109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Choi SH, Ahn CW, Cha BS, Chung YS, Lee KW, Lee HC, et al. The prevalence of the metabolic syndrome in Korean adults: Comparison of WHO and NCEP criteria. Yonsei Med J. 2005;46:198–205. doi: 10.3349/ymj.2005.46.2.198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wang SH, Hsiao PC, Hsiao CK, Liu PH, Chien KL, Lin SR, et al. Multilevel analysis of habitual physical activity and metabolic syndrome in Northern Taiwan. Prev Med. 2011;53:34–8. doi: 10.1016/j.ypmed.2011.04.017. [DOI] [PubMed] [Google Scholar]
- 18.Azizi F, Salehi P, Etemadi A, Zahedi-Asl S. Prevalence of metabolic syndrome in an urban population: Tehran Lipid and Glucose Study. Diabetes Res Clin Pract. 2003;61:29–37. doi: 10.1016/s0168-8227(03)00066-4. [DOI] [PubMed] [Google Scholar]
- 19.Sarrafzadegan N, Kelishadi R, Baghaei A, Hussein Sadri G, Malekafzali H, Mohammadifard N, et al. Metabolic syndrome: An emerging public health problem in Iranian women: Isfahan Healthy Heart Program. Int J Cardiol. 2008;17(131):90–6. doi: 10.1016/j.ijcard.2007.10.049. [DOI] [PubMed] [Google Scholar]
- 20.Ghorbani R, Abtahinaeini B, Eskandarian R, Rashidy-Pour A, Khamseh ME, Malek M. Prevalence of metabolic syndrome according to ATPIII and IDF criteria in the Iranian population. Koomesh. 2012;14:65–75. [Google Scholar]
- 21.Panagiotakos DB, Pitsavos C, Chrysohoou C, Skoumas J, Tousoulis D, Toutouza M, et al. Impact of lifestyle habits on the prevalence of the metabolic syndrome among Greek adults from the ATTICA study. Am Heart J. 2004;147:106–12. doi: 10.1016/s0002-8703(03)00442-3. [DOI] [PubMed] [Google Scholar]
- 22.Gharipour M, Baghei A, Boshtam M, Rabiei K. Prevalence of metabolic syndrome among the adult of central of areas of Iran (as part of Isfahan healthy heart study) BUMS. 2006;13:56–63. [Google Scholar]
- 23.Stewart KJ, Bacher AC, Turner K, Lim JG, Hees PS, Shapiro EP, et al. Exercise and risk factors associated with metabolic syndrome in older adults. Am J Prev Med. 2005;28:9–18. doi: 10.1016/j.amepre.2004.09.006. [DOI] [PubMed] [Google Scholar]
- 24.Gerstel E, Pataky Z, Busnel C, Rutschmann O, Guessous I, Zumwald C, et al. Impact of lifestyle intervention on body weight and the metabolic syndrome in home-care providers. Diabetes Metab. 2013;39:78–84. doi: 10.1016/j.diabet.2012.07.003. [DOI] [PubMed] [Google Scholar]
- 25.Dutheil F, Lac G, Courteix D, Doré E, Chapier R, Roszyk L, et al. Treatment of metabolic syndrome by combination of physical activity and diet needs an optimal protein intake: A randomized controlled trial. Nutr J. 2012;11:72. doi: 10.1186/1475-2891-11-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Moeini B, Hazavehei SM, Jalilian M, Moghimbeigi A, Seresht NT. Factors affecting physical activity and metabolic control in type 2 diabetic women referred to the diabetes research center of Hamadan: Applying trans-theoretical model. Sci J Hamadan Univ Med Sci. 2011;18:31–7. [Google Scholar]
- 27.Shirazi KK, Wallace LM, Niknami S, Hidarnia A, Torkaman G, Gilchrist M, et al. A home-based, transtheoretical change model designed strength training intervention to increase exercise to prevent osteoporosis in Iranian women aged 40-65 years: A randomized controlled trial. Health Educ Res. 2007;22:305–17. doi: 10.1093/her/cyl067. [DOI] [PubMed] [Google Scholar]
- 28.Dallow CB, Anderson J. Using self-efficacy and a transtheoretical model to develop a physical activity intervention for obese women. Am J Health Promot. 2003;17:373–81. doi: 10.4278/0890-1171-17.6.373. [DOI] [PubMed] [Google Scholar]
- 29.Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: Toward an integrative model of change. J Consult Clin Psychol. 1983;51:390–5. doi: 10.1037//0022-006x.51.3.390. [DOI] [PubMed] [Google Scholar]
- 30.Glanz KA, Rimer B.K, Lewis F.M. 4th ed. San Farancisco: Josey-Bass; 2008. Health Behavior and Health Education Theory-Research and Practice. [Google Scholar]
- 31.Marshall SJ, Biddle SJ. The transtheoretical model of behavior change: A meta-analysis of applications to physical activity and exercise. Ann Behav Med. 2001;23:229–46. doi: 10.1207/S15324796ABM2304_2. [DOI] [PubMed] [Google Scholar]
- 32.Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol Rev. 1977;84:191–215. doi: 10.1037//0033-295x.84.2.191. [DOI] [PubMed] [Google Scholar]
- 33.Farmanbar RA, Niknami SH, Heidarnia AR. Effect of an integrated transtheoretical model and self –Determination theory on the promotion and maintenance of exercise behavior. J Guilan Univ Med Sci. 2002;21:46–56. [Google Scholar]
- 34.Chang L, McAlister AL, Taylor WC, Chan W. Behavioral change for blood pressure control among urban and rural adults in Taiwan. Health Promot Int. 2003;18:219–28. doi: 10.1093/heapro/dag017. [DOI] [PubMed] [Google Scholar]
- 35.Loprinzi PD, Cardinal BJ, Si Q, Bennett JA, Winters-Stone KM. Theory-based predictors of follow-up exercise behavior after a supervised exercise intervention in older breast cancer survivors. Support Care Cancer. 2012;20:2511–21. doi: 10.1007/s00520-011-1360-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Pinto BM, Rabin C, Dunsiger S. Home-based exercise among cancer survivors: Adherence and its predictors. Psychooncology. 2009;18:369–76. doi: 10.1002/pon.1465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.IPAQ. Guidelines for Data Processing and Analysis of the International physical Activity Questionnaire (IPAQ)-Short form. 2005. 2014. Jul 25, [Last accessed on 2014 Aug 25]. Available from: http://www.ipaq.ki.se .
- 38.Marcus BH, Rakowski W, Rossi JS. Assessing motivational readiness and decision making for exercise. Health Psychol. 1992;11:257–61. doi: 10.1037//0278-6133.11.4.257. [DOI] [PubMed] [Google Scholar]
- 39.Marcus BH, Forsyth LH, Blaire S. Human Kinetics. United States of America: 2003. Motivating People to be Physically Active. [Google Scholar]
- 40.Pender NJ, Walker SN, Sechrist KR, Frank-Stromborg M. Predicting health-promoting lifestyles in the workplace. Nurs Res. 1990;39:326–32. [PubMed] [Google Scholar]
- 41.Nigg CR, Riebe D. The transtheoretical model: Research review of exercise behavior and older adults. In: Burbank PM, Riebe D, editors. Promoting Exercise and Behavior Change in Older Adults: Interventions with the Transtheoretical Model. New York: Springer; 2002. pp. 147–80. [Google Scholar]
- 42.Lach HW, Everard KM, Highstein G, Brownson CA. Application of the transtheoretical model to health education for older adults. Health Promot Pract. 2004;5:88–93. doi: 10.1177/1524839903257305. [DOI] [PubMed] [Google Scholar]
- 43.Woods C, Mutrie N, Scott M. Physical activity intervention: A transtheoretical model-based intervention designed to help sedentary young adults become active. Health Educ Res. 2002;17:451–60. doi: 10.1093/her/17.4.451. [DOI] [PubMed] [Google Scholar]
- 44.Pan FC, Chen CH. Application of the transtheoretical model of exercise behavior change plan in high school students. World Acad Sci Eng Technol. 2010;43:172. [Google Scholar]
- 45.Kirk A, MacMillan F, Webster N. Application of the transtheoretical model to physical activity in older adults with type 2 diabetes and/or cardiovascular disease. Psychol Sport Exerc. 2010;11:320–4. [Google Scholar]
- 46.Opdenacker J, Bourdeaudhuij ID, Auweele YV, Boen F. Psychosocial mediators of a lifestyle physical activity intervention in women. Psychol Sport Exerc. 2009;10:595–601. [Google Scholar]
- 47.Speck BJ, Looney SW. Effects of a minimal intervention to increase physical activity in women: Daily activity records. Nurs Res. 2001;50:374–8. doi: 10.1097/00006199-200111000-00008. [DOI] [PubMed] [Google Scholar]
- 48.Tabatabaei SA, Taghdisi M, Sadeghi A, Nakhaei N. The effect of education in physical activities on knowledge, attitude and behavior of Kerman health center's staff. J Res Health. 2012;2:55–62. [Google Scholar]
- 49.Hoebeke R. Low-income women's perceived barriers to physical activity: Focus group results. Appl Nurs Res. 2008;21:60–5. doi: 10.1016/j.apnr.2006.06.002. [DOI] [PubMed] [Google Scholar]
- 50.Nishida Y, Suzuki H, Wang DH, Kira S. Psychological determinants of physical activity in Japanese female employees. J Occup Health. 2003;45:15–22. doi: 10.1539/joh.45.15. [DOI] [PubMed] [Google Scholar]
- 51.Sit CH, Kerr JH, Wong IT. Motives for and barriers to physical activity participation in middle-aged Chinese women. Psychol Sport Exerc. 2008;9:266–83. [Google Scholar]
- 52.Lee YM, Park NH, Kim YH. Process of change, decisional balance, self-efficacy and depression across the stages of change for exercise among middle aged women in Korea. Taehan Kanho Hakhoe Chi. 2006;36:587–95. doi: 10.4040/jkan.2006.36.4.587. [DOI] [PubMed] [Google Scholar]
- 53.Gorely T, Bruce D. 6-month investigation of exercise adoption from the contemplation stage of the transtheoretical model. Psychol Sport Exerc. 2000;1:89–101. [Google Scholar]
- 54.Mohammadi Zeidi I, Ziaeiha M, Safari Variyani A, Khalaj M, Mohammadi Zeidi B, Morshedi H. Predicting the stages of change in physical activity behavior of QUMS students with Pender's model. J Qazvin Univ Med Sci. 2010;14:58–66. [Google Scholar]
- 55.Yoo S, Kim H, Cho HI. Improvements in the metabolic syndrome and stages of change for lifestyle behaviors in Korean older adults. Osong Public Health Res Perspect. 2012;3:85–93. doi: 10.1016/j.phrp.2012.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Shahrjerdi SH, Shavandi N, Hoseini RS. The effect of aerobic exercise on metabolic factors, quality of life (QOL) and mental health (MH) in women with type II diabetes. Arak Med Univ J. 2010;12:25–35. [Google Scholar]
- 57.Moghadasi M, Mohebbi H, Nematollah ZMMA. Effect of 12 weeks life-style activity modification on serum oxidized LDL-C in obese men. Iran J Endocrinol Metab. 2012;13:486–92. [Google Scholar]
- 58.Alizadeh Z, Kordi R, Hossein-Zadeh Attar MJ, Mansournia MA. The effects of continuous and intermittent aerobic exercise on lipid profile and fasting blood sugar in women with a body mass index more than 25 kg/m2: A randomized controlled trial. Tehran Univ Med J. 2011;69:235–59. [Google Scholar]
- 59.Askari A, Askari B, Fallah Z, Kazemi SH. Effect of eight weeks aerobic training on serum lipid and lipoprotein levels in women. J Gorgan Uni Med Sci. 2012;14:26–32. [Google Scholar]
- 60.Tonstad S, Alm CS, Sandvik E. Effect of nurse counselling on metabolic risk factors in patients with mild hypertension: A randomised controlled trial. Eur J Cardiovasc Nurs. 2007;6:160–4. doi: 10.1016/j.ejcnurse.2006.07.003. [DOI] [PubMed] [Google Scholar]
- 61.Nikpour S, Rahimiha F, Haghani H. Comparing the status of sport activities in women and men working at Iran university of medical sciences and health services. Razi J Med Sci. 2006;13:205–16. [Google Scholar]