

Abstract
Background
Randomized controlled trials (RCTs) of endovascular therapy for acute ischemic stroke have had inconsistent results. We evaluated the efficacy and safety of endovascular therapy in published RCTs.
Methods
We performed a systematic review of RCTs of endovascular therapy with thrombolytic or mechanical reperfusion compared with interventions without endovascular therapy. Primary outcome was the frequency of good functional outcome (modified Rankin scale (mRS) of 0-2 at 90 days) and secondary outcomes were mortality at 90 days and symptomatic intracranial hemorrhage (sICH). Random-effects meta-analysis was performed and the Cochrane risk of bias assessment was used to evaluate quality of evidence.
Results
Ten studies involving 1,612 subjects were included. Endovascular therapy was not significantly associated with good functional outcome (Relative Risk [RR] =1.17; 95% CI, 0.97 to 1.42; p=0.10 and Absolute Risk Difference [ARD] =7%; 95%CI -0.1% to 14%; p=0.05); heterogeneity was moderate among studies (I2=30%). Mortality was unchanged with endovascular therapy (RR=0.92; 95 % CI, 0.75 to 1.13; p=0.45) and there was no difference in sICH (RR=1.20; 95 % CI, 0.79 to 1.82; p=0.39). The quality of evidence was low for all outcomes and the recommendation is weak for the use of endovascular therapy as per GRADE methodology.
Conclusions
Intra-arterial therapy did not show significant increase in good outcomes and no changes in either mortality or sICH in patients with acute ischemic stroke. We need further RCTs with better design and quality to evaluate the true efficacy of endovascular therapy.
Introduction
Acute endovascular reperfusion is becoming an important part of acute ischemic stroke therapy, but randomized controlled trials (RCTs) have had inconsistent results. Prolyse in Acute Cerebral Thromboembolism 2 trial (PROACT-2), showed that the intra-arterial (IA) thrombolysis with pro-urokinase for middle cerebral artery (MCA) occlusion increased the likelihood of good outcome defined by modified Rankin scale (mRS) 2 or less.[1] A subsequent study of IA thrombolysis, MELT Japan, was underpowered as only were analyzed 114 patients out of the 200 planned. This study was aborted because of approval of intravenous infusion of recombinant tissue plasminogen activator in Japan and the primary outcome, the proportion of patients with favorable outcomes (mRS scores of 0 to 2) at 90 days did not reach statistical significance.[2] Since 2004 several mechanical thrombectomy devices have been approved by government regulatory authorities according to the results of the non-randomized studies.[3–7]. These uncontrolled studies have reported higher likelihood of good outcomes among those who achieved good recanalization compared to those in whom the arterial occlusion could not be opened. In 2013, three RCTs have been published to test the efficacy of mechanical thrombectomy.[8–10]
Three prior systematic reviews of RCTs focused on the question of IA thrombolysis compared to placebo or intravenous (IV) thrombolysis. However these analyses did not include a large number of subjects with mechanical thrombectomy approach.[11–13] With the recent publication of the three RCTs using mechanical thrombectomy, we performed a systematic review and meta-analysis of RCTs comparing endovascular treatment for acute ischemic stroke with control treatment.
Methods
Data sources and searches
A comprehensive literature search using PubMed-Medline, The Cochrane library, The Web of Science, and Scopus from database inception through July 24, 2013 was conducted by three investigators (OT, VP and AD). The following keywords were used: acute ischemic stroke, endovascular therapy, intra-arterial therapy, catheter-based therapy, Merci, Penumbra, Solitaire, Trevo, stent, GpIIb/IIIa antagonist, and randomized controlled trial. The search strategy of PubMed is available as Appendix A in S1 File.
Study selection and data extraction
The following predetermined inclusion criteria were used: (i) RCTs, (ii) studies evaluating the efficacy of endovascular treatments for acute ischemic stroke in comparison with a control group without endovascular treatment (placebo, intravenous therapy, standard care [i.e. usual clinical practice at the time of the trial]); (iii) study in any language. Our exclusion criteria were: (i) no control group; (ii) outcome measures data were not available or could not be extracted from the study groups. A list of retrieved articles was reviewed independently by 3 investigators (OT, VP and AD) in order to choose potentially relevant articles, and disagreements about particular studies were discussed and resolved by consensus.
Two reviewers (OT and VP) independently extracted data from studies. The following information was extracted: age, study years, geographic location, study phase, blinding, and requirement of arterial occlusion for randomization, time to randomization, time to endovascular therapy, allocated therapy, and National Institutes of Health Stroke Scale (NIHSS) score at baseline. Outcome data of interest were mRS at 90 days, mortality, and symptomatic ICH (sICH). We defined good functional outcome as mRS between 0 and 2 points. One other author (AVH) reviewed the extractions for inconsistencies, and the three investigators (AVH, OT and VP) reached consensus.
The Cochrane risk of bias evaluation
The risk of bias for each study was evaluated using the Cochrane Collaboration tool for assessing risk of bias in randomized controlled trials. [14] The following items were evaluated:
Generation of the allocation sequence (selection bias)
Concealment of the allocation sequence (selection bias)
Blinding (detection and performance bias), blinding of participants and personnel and blinding of outcome assessment
Incomplete outcome data (attrition bias)
Selective outcome reporting (reporting bias)
Other biases
For each randomized controlled trial each item was described as: low risk of bias, high risk of bias and unclear risk of bias.[14] As secondary source of evaluation of quality of evidence, we also used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach per randomized controlled trial (Appendix B in S1 File). One other author (AVH) reviewed the evaluations for inconsistencies, and the three investigators (AVH, OT and VP) reached consensus.
Data synthesis and analysis
Our systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Table A in S1 File).[15] We used the Mantel-Haenszel (MH) method to calculate pooled Relative risks (RRs) and Absolute Risk Differences (ARD) and their 95% CIs. Statistical heterogeneity was evaluated with the Cochran χ2 and the I2 statistics. I2 values of 30–60% represented a moderate level of heterogeneity. A P value of < 0.1 for χ2 was defined as indicating the presence of heterogeneity. Some degree of heterogeneity was expected and therefore to take into account sources of heterogeneity, several subgroup meta-analyses were pre-specified: (i) type of endovascular therapy (IA thrombolysis or mechanical thrombectomy), (ii) type of comparator (IV thrombolysis or no requirement for IV thrombolysis), and (iii) vessel occlusion status (required demonstrated vessel occlusion for randomization or not). We also used cumulative meta-analysis to show the evolution of risks over time. DerSimonian and Laird random effects models were used for meta-analyses.[16] To examine bias in the results of the meta-analyses, the Egger’s test was used to evaluate asymmetry of the funnel plots. We used Review Manager (RevMan 5.0, Oxford, UK; The Cochrane Collaboration, 2008) and R metafor software (www.metafor-project.org).
Results
Eligible studies
Our search identified 1857 publications. After removing duplicates and screening titles of the studies, 428 articles were selected based on relevance to the study topic. After screening the abstracts of these potentially relevant articles, 20 were selected for full-text review based on relevance to the study topic (Fig 1). Ten RCTs involving 1,612 subjects that reported outcomes data of endovascular therapy in acute ischemic stroke in comparison to a control (no endovascular therapy) were included in the systematic review and meta-analyses. The reasons for exclusion of the remaining 10 articles are listed in Fig 1. Reference lists of all included studies were also searched and no relevant articles were identified for inclusion.
Fig 1. Flow diagram of selected studies.

Study characteristics
Table 1 summarizes the main characteristics of the included studies. Of the 10 trials included, 7 trials[1,2,17–21] had IA thrombolysis only in the active treatment arms, while 3 trials[8–10] allowed mechanical thrombectomy devices in the active treatment arms. Five trials required that vessel occlusion was necessary for inclusion of patients (3 studies of MCA occlusions[1,2,8,18], 1 of anterior circulation occlusions including MCAs [10,20], 1 limited to cerebral vessel occlusion located in posterior circulation.[21] Five trials did not require the cerebral vessel occlusion [9,17,19]. Outcomes were determined by using mRS 0–2 at 90 days in 8 studies. Remaining 2 studies used mRS 0–1 and 0–3 as primary outcomes and did not report the distribution between groups. For one study mRS 0–2 was reported in a secondary publication[18]. Thus we excluded one study reporting primary outcome as mRS 0–3, when we evaluate good functional outcome. Various mechanical devices were used in the studies which compared mechanical thrombectomy with control treatment. Broderick et al[8] allowed the use of Merci retrieval, Penumbra system or Solitaire FR. Kidwell et al[10] permitted the treatment with Merci retrieval or Penumbra. Ciccone et al [9] did not reveal the brand of mechanical thrombectomy device. A total of 1,612 patients were included in the meta-analysis with sample sizes ranging from 16 to 656 (Table 1).
Table 1. Patient characteristics in studies included in the meta-analysis.
| Study reference, Year | Study name | Study years | Study location | Study phase | Blinding | Arterial occlusion required | Time to randomization; endovascular therapy | Allocation | Study population, n | Allocated therapy | Symptom onset to therapy time, h, median (IQR) | Age, mean (SD) | Baseline NIHSS median (range) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| del Zoppo GJ, 1998[18] | PROACT | 1994–1995 | Canada, USA | 2 | Double-blind | Yes | within 6 hrs; within 6 hrs | Controls | 14 | heparin | 5.7 | 69.6 (11.1) | 19 |
| Cases | 26 | IA r-pro UK | 5.4 | 66.5 (11.0) | 17 | ||||||||
| Furlan A, 1999[1] | PROACT II | 1996–1998 | Canada, USA | 3 | Open design with blinded follow-up | Yes | NA; within 6 hrs | Controls | 59 | heparin | NA | 64 (14) | 17 (4–28) |
| Cases | 121 | IA r-pro UK + heparin | 5.3 | 64 (14) | 17 (5–27) | ||||||||
| Keris V, 2001[20] | 1997–1998 | Latvia | NA | Open-label | No | NA; within 6 hrs | Controls | 33 | heparin | NA | 65 (8) | 26 (5) † | |
| Cases | 12 | IA/IV tPA + heparin | 4.0 | 53 (9) | 25 (3) † | ||||||||
| Ducrocq X, 2005[19] | 1995–1997 | France | NA | Open design with blinded follow-up | No | NA; within 6 hrs | Controls | 14 | IV UK | 4.1 | 58 | 14.6 † | |
| Cases | 13 | IA UK | 5.3 | 59.5 | 15.2 † | ||||||||
| Macleod MR, 2005[21] | Australian Urokinase Stroke Trial | 1996–2003 | Australia, New Zealand | NA | Open design with blinded follow-up | Yes | NA; within 24 hrs | Controls | 8 | heparin | 12.5 (3.4–22.5) § | 63.7 (12.3) | 18 (5–29) |
| Cases | 8 | IA UK + heparin | 11.8 (5.8–21.8) § | 64.2 (11.1) | 23 (7–29) | ||||||||
| Ogawa A, 2007[2] | MELT | 2002–2005 | Japan | NA | Open-label | Yes | within 6 hrs; within 6 hrs | Controls | 57 | heparin | NA | 67.3 (8.5) | 14 (6.8) ‡ |
| Cases | 57 | IA UK + heparin | 3.8 † | 66.9 (9.3) | 14 (8.0) ‡ | ||||||||
| Ciccone A, 2010[17] | SYNTHESIS pilot | 2004–2008 | Italy | NA | Open design with blinded follow-up | No | NA; within 6 hrs | Controls | 29 | IV tPA | 2.6 (2.3–2.8) | 64.0 (11.7) | 16 (3–24) |
| Cases | 25 | IA tPA | 3.3 (2.8–4.0) | 60.6 (13.7) | 17 (2–26) | ||||||||
| Broderick JP, 2013[8] | IMS III | 2006–2012 | Australia, Canada, Europe, USA | 3 | Open design with blinded follow-up | No | within 3 hrs 40 min; within 5 hrs | Controls | 222 | IV tPA | 2.0 (0.6) † | 68 (23–84)* | 16 (8–30) |
| Cases | 434 | IV tPA + thrombectomy | 2.0 (0.6) † | 69 (23–89)* | 17 (7–40) | ||||||||
| Ciccone A, 2013[9] | SYNTHESIS | 2008–2012 | Italy | NA | Open design with blinded follow-up | No | within 4.5 hrs; within 6 hrs | Controls | 181 | IV tPA | 2.5 (2.2–3.2) | 67 (11) | 13 (3–24) |
| Cases | 181 | IA tPA + thrombectomy | 3.5 (3.1–4.2) | 66 (11) | 13 (2–26) | ||||||||
| Kidwell CS, 2013[10] | MR RESCUE | 2004–2011 | Canada, USA | 2 | Open design with blinded follow-up | Yes | within 8 hrs; within 8 hrs | Controls | 54 | standard care | NA | 67.1 (16.5) | 17 † |
| Cases | 64 | IA tPA + thrombectomy | 64.2 (12.8) | 17 † |
NA = not available; IA = intra-arterial; IV = intravenous; r-pro UK = recombinant pro- urokinase; tPA = tissue plasminogen activator; h = hours; IQR = interquartile range;
* = median (range);
† = mean (SD);
‡ = median (IQR);
§ = mean (range).
The Cochrane risk of bias evaluation
Most of studies had low risk of bias in most of the assessed items (Table 2). One trial had high risk of bias in 4 items [20] and three trials had high risk of bias in 2 items [8,17,19]. Blinding of participants and personnel was the item with more studies having high risk of bias [8–10,17,19,20]; randomization sequence generation was unclear in four studies [17–19,21].
Table 2. Cochrane assessment of bias risk of randomized controlled trials.
| Del Zoppo GJ 1998[18] | Furlan A 1999[1] | Keris V 2001[20] | Ducrocq X 2005[19] | Macleod MR 2005[21] | Ogawa A 2007[2] | Ciccone A 2010[17] | Broderick JP 2013[8] | Ciccone A 2013[9] | Kidwell CS 2013[10] | |
|---|---|---|---|---|---|---|---|---|---|---|
| Randomization sequence generation | Unclear | Low | High | Unclear | Unclear | Low | Unclear | Low | Low | Low |
| Allocation concealment | Low | Low | High | Low | Low | Low | Low | Low | Low | Low |
| Blinding of participants and personnel | Low | Low | High | High | Low | Low | High | High | High | High |
| Blinding of outcome assessment | Low | Low | High | High | Low | Low | Low | Low | Low | Low |
| Incomplete outcome data | Low | Low | Low | Low | Low | Low | High | Low | Low | Low |
| Selective outcome reporting | Low | Low | Low | Low | Low | Low | Low | Low | Low | Low |
| Other sources of bias | Low | Low | Low | Low | Low | Low | Unclear | High | Unclear | Low |
GRADE Quality of the Evidence
The quality of evidence for the effect of IA therapy on critical outcomes like mRS ≤2, mortality and sICH was low (Appendix B in S1 File).
Meta-analysis of benefits and harms of endovascular therapy in ischemic stroke
We did not find a significant higher probability of beneficial outcome defined as mRS ≤2 with endovascular therapy in comparison to controls (RR = 1.17; 95% CI 0.97–1.42; p = 0.10). There was moderate heterogeneity among studies (I2 = 30%) (Fig 2A). Cumulative meta-analysis showed that the significant association between IA therapy and the beneficial primary outcome went towards zero and became non-significant over time (Fig A in S1 File). In absolute terms, there was no higher proportion of good outcomes (ARD 7%; 95% CI -0.1% to 14%; p = 0.05) (Fig 3). There were no significant difference in mortality when endovascular therapy was compared with control groups (RR = 0.92; 95% CI 0.75–1.13; p = 0.45) and no heterogeneity among studies (I2 = 0%) (Fig 4A). Endovascular therapy did not change the rate of sICH when compared with control group (RR = 1.20; 95% CI 0.79–1.82; p = 0.39) and no heterogeneity among studies (I2 = 0%) (Fig 4B). There was a significant higher probability of any ICH in controls in comparison to endovascular therapy group (RR = 1.47; 95% CI 1.14–1.90; p = 0.003; I2 = 45%) (Fig B in S1 File).
Fig 2. Forest plots showing modified Rankin Score 0–2 at 90 days between endovascular therapy and controls.

A: All studies. B: Subgroup 1: IA thrombolysis only versus mechanical device use. C: Subgroup 2: Comparator includes IV thrombolysis versus no thrombolysis. D: Subgroup 3: Studies that required vessel occlusion versus studies did not require vessel occlusion status.
Fig 3. Modified Rankin Score 0–2 at 90 days expressed as absolute risk differences (ARD).
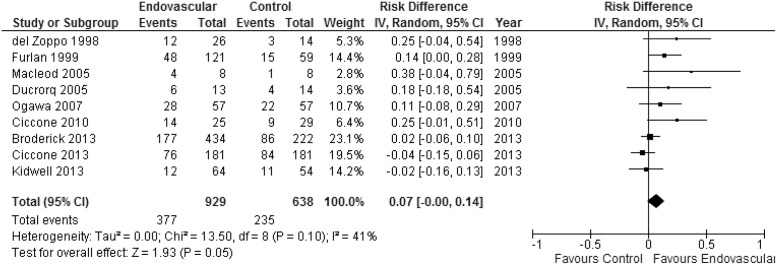
Fig 4.

A: Forest plots showing mortality between endovascular therapy and controls. B: Forest plots showing symptomatic intracranial hemorrhage between endovascular therapy and controls.
There was evidence of asymmetry of the funnel plots for the primary outcome, Rankin < 3 and mortality to suggest publication bias (p = 0.2, p = 0.2, respectively) (Fig F1-2 in S1 File). There was evidence of asymmetry of the funnel plots for the ICH outcomes to suggest publication bias (any ICH p = 0.03, symptomatic ICH p = 0.06) (Fig F3-4 in S1 File). For forest plots of absolute differences for the secondary outcomes (mortality and sICH) please see Fig G1-2 in S1 File.
Subgroup analyses for the primary outcome
IA thrombolysis only was associated with higher chance of good outcome in terms of disability (RR = 1.53; 95% CI 1.18–2.00; p = 0.002) whereas mechanical device usage was not associated with increase in good outcome in terms of disability (Fig 2B). There were no significant differences between control group and endovascular group in the studies that required IV thrombolysis in the comparator. When comparator had no IV thrombolysis, the endovascular group showed a significant beneficial outcome than control group (RR = 1.38; 95% CI 1.04–1.82; p = 0.03) (Fig 2C). Analysis by vessel occlusion demonstrated that endovascular therapy was associated with the increased good outcome (RR = 1.38; 95% CI 1.04–1.82; p = 0.03) in the studies that required vessel occlusion for randomization. There were no significant difference between endovascular group and control group when vessel occlusion status was not required (Fig 2D). Heterogeneity ranged from 0% to 39% on subgroup analyses.
Subgroup analyses for the secondary outcomes
In general there were no differences in subgroup analyses when compared with the main analyses. Forest plots of these subgroup analyses are shown in Fig C-E in S1 File.
Discussion
In our study, ten RCTs were detected and 9 RCTs estimated good outcome defined as modified Rankin scale 2 or less. Endovascular therapy did not increase good outcome, and there was moderate heterogeneity. Similarly, symptomatic ICH and mortality in endovascular groups occur as frequently as those in control groups. Subgroup analyses showed that endovascular therapy increased beneficial outcome without heterogeneity if only IA thrombolysis was included in the active treatment group, if IV thrombolysis was not included in control groups or if subjects in studies required the evidence of vessel occlusion. The quality of evidence was low for all outcomes and the recommendation is weak for the use of IA therapy as per GRADE methodology.
Two prior systematic reviews only focused on the comparison between IA thrombolysis and controls.[11,12] The results of these studies are congruent with our subgroup analysis of endovascular therapy that used IA thrombolytics and demonstrated IA thrombolysis to reduce disability. Lee et al. showed that the patients treated with IA fibrinolysis were significantly more likely to have good clinical outcome defined as mRS 0–2 than conventional treatment without IV thrombolysis. (OR = 2.05; 95% CI 1.33–3.14; p = 0.001) [10]. Fields et al. also reported similar result for the patients with acute ischemic stroke due to MCA occlusion. (OR = 1.9; 95% CI 1.2–3.0).[11] Nam et al. reported a meta-analysis of RCTs comparing endovascular therapy to controls but included only a small number of patients who underwent mechanical thrombectomy.[13] This study included patients treated with IV thrombolysis in the control arms. The results showed that IA thrombolysis reduced poor outcome patients defined as mRS 3–6 compared with control treatments (RR = 0.80; 95% CI 0.67–0.95; p = 0.001), although IA thrombolysis did not have clear benefit over IV thrombolysis (RR = 0.68; 95% CI 0.46–1.00; p = 0.05). [13]
Our subgroup analyses indicated that IA thrombolysis compared to mechanical thrombectomy might be a factor for a study to demonstrate a benefit of endovascular approach. But arterial recanalization rates are lower in IA thrombolysis compared to mechanical thrombectomy and two of the three trials designated as allowing mechanical approach had majority of subjects undergo IA thrombolysis.[8,9,22] Comparing to IV thrombolysis may diminish the effect of IA therapy, especially if cohort includes those without target vessel occlusion or recanalized with IV thrombolysis.[8,9,17] We hypothesize that vessel occlusion is the most important factor. IV thrombolysis has lower recanalization rate and is less effective for recanalization of large vessel occlusion than IA therapy.[23,24] A sub study of IMS3 studied arterial occlusion pre- and post-treatment using CT angiography. Within the subgroup of patients with proximal large arterial occlusion at baseline, good mRS was observed more frequently in the endovascular treatment group than in the control group.[25] Including those without proximal arterial occlusion that are not amenable to endovascular approach dilutes the overall of effect of such approach towards the null. Several used NIHSS cut-offs which is highly correlated with vascular occlusion after IV t-PA ref. However, IMS3 had 19% of patients (80/423) who were randomized to IA arm. This is in accordance with NIHSS of 10 or greater having 70–80% specificity in having vascular occlusion. But 20% may be too high of a rate of including patients who would not qualify for the therapy. Future studies of endovascular therapy should enroll only those with target vessel occlusion.
We found mortality were similar to previous meta-analysis which reported there was no significant difference between endovascular treatment arms and control arms.[11,13] Our finding of no increase in sICH differs from previous reviews.[12] Our study included studies of mechanical thrombectomy and more studies with comparator arms including IV TPA, which is known to increase sICH. It is reported that IA thrombolysis caused more ICH than control treatment without IV thrombolysis;[12] however IA thrombolysis did not increase symptomatic hemorrhage compared with IV thrombolysis.
The quality of evidence of was assessed to be low by GRADE methodology. This may have several reasons. This methodology may have inherent limitations in evaluating this type of therapy and may result in low quality. The acute nature of stroke treatment prevents a double blind design with sham intervention. Risks of sedation or anesthesia should be a part of the endovascular approach and control sham procedure would not suffice. A prospective randomized open blinded endpoint (PROBE) design is the most realistic approach for clinical trials of acute endovascular therapy. The “imprecision” of the outcomes is somewhat inherent with scarce outcomes of ischemic stroke patients. In addition to heterogeneity of the outcomes of any strokes, inclusion of occlusions is another issue. However, the GRADE evaluation points to the need for more uniform approaches and more studies to increase precision of estimate of effects.
There were limitations in this study. First, study design, subject selection, and endovascular techniques varied among studies. For example we didn’t analyze time to treatment because these reviews referred to various time to treatment. Second, not all outcomes we evaluated were reported in the detected trials. Primary outcome defined mRS 0–2 were reported in 9 trials; Keris et al. regarded good outcome as mRS 3 or less and this outcomes was not analyzed 20. Finally, while mortality was described in all trials, not all trials described systematic imaging to detect any intracranial hemorrhage or reported symptomatic hemorrhages.
Supporting Information
Appendix A: PubMed search Strategy. Appendix B: Grading Quality of the Evidence and Recommendations. Table A: PRISMA Checklist. Table B: GRADE evaluation of quality of evidence. Table C: List of excluded studies. Figure A: Cumulative meta-analysis (i.e. effects over time). Figure B: Forest plots showing any intracranial hemorrhage between endovascular therapy and controls. Figure C: Forest plot showing mortality in endovascular therapy vs controls. Figure C1: IA thrombolysis only vs mechanical device use. Figure C2: Comparator includes IV thrombolysis vs no thrombolysis. Figure C3: Studies that required vessel occlusion vs studies did not require vessel occlusion status. Figure D: Forest plot showing any intracranial hemorrhage in endovascular therapy vs controls. Figure D1: IA thrombolysis only vs mechanical device use. Figure D2: Comparator includes IV thrombolysis vs no thrombolysis. Figure D3: Studies that required vessel occlusion vs studies did not require vessel occlusion status. Figure E: Forest plot showing symptomatic intracranial hemorrhage in endovascular therapy vs controls. Figure E1: IA thrombolysis only vs mechanical device use. Figure E2: Comparator includes IV thrombolysis vs no thrombolysis. Figure E3: Studies that required vessel occlusion vs studies did not require vessel occlusion status. Figure F: Funnel Plots and Egger’s test for asymmetry of the funnel plot (p<0.1 for asymmetry). Figure F1: Primary outcome: Rankin <3. Egger’s test: p value = 0.2. Figure F2: Secondary outcome: Mortality. Egger’s test: p value = 0.2. Figure F3: Secondary outcome: Any ICH. Egger’s test: p value = 0.03. Figure F4: Secondary outcome: Symptomatic ICH. Egger’s test: p value = 0.06. Figure G: Absolute risk differences (ARD) for the secondary outcomes. Figure G1: Mortality. Figure G2: Symptomatic ICH.
(DOCX)
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
The authors have no support or funding to report.
References
- 1. Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase C, et al. Intra-arterial prourokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA. 1999;282: 2003–2011. [DOI] [PubMed] [Google Scholar]
- 2. Ogawa A, Mori E, Minematsu K, Taki W, Takahashi A, Nemoto S, et al. Randomized trial of intraarterial infusion of urokinase within 6 hours of middle cerebral artery stroke: the middle cerebral artery embolism local fibrinolytic intervention trial (MELT) Japan. Stroke. 2007;38: 2633–2639. [DOI] [PubMed] [Google Scholar]
- 3. Smith WS, Sung G, Saver J, Budzik R, Duckwiler G, Liebeskind DS, et al. Mechanical thrombectomy for acute ischemic stroke: final results of the Multi MERCI trial. Stroke. 2008;39: 1205–1212. 10.1161/STROKEAHA.107.497115 [DOI] [PubMed] [Google Scholar]
- 4. Smith WS. Safety of mechanical thrombectomy and intravenous tissue plasminogen activator in acute ischemic stroke. Results of the multi Mechanical Embolus Removal in Cerebral Ischemia (MERCI) trial, part I. AJNR Am J Neuroradiol. 2006;27: 1177–1182. [PMC free article] [PubMed] [Google Scholar]
- 5. Penumbra Pivotal Stroke Trial Investigators. The penumbra pivotal stroke trial: safety and effectiveness of a new generation of mechanical devices for clot removal in intracranial large vessel occlusive disease. Stroke. 2009;40: 2761–2768. 10.1161/STROKEAHA.108.544957 [DOI] [PubMed] [Google Scholar]
- 6. Machi P, Costalat V, Lobotesis K, Maldonado IL, Vendrell JF, Riquelme C, et al. Solitaire FR thrombectomy system: immediate results in 56 consecutive acute ischemic stroke patients. J Neurointerv Surg. 2012;4: 62–66. 10.1136/jnis.2010.004051 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Baker WL, Colby JA, Tongbram V, Talati R, Silverman IE, White CM, et al. Neurothrombectomy devices for the treatment of acute ischemic stroke: state of the evidence. Ann Intern Med. 2011;154: 243–252. 10.7326/0003-4819-154-4-201102150-00306 [DOI] [PubMed] [Google Scholar]
- 8. Broderick JP, Palesch YY, Demchuk AM, Yeatts SD, Khatri P, Hill MD, et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med. 2013;368: 893–903. 10.1056/NEJMoa1214300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Ciccone A, Valvassori L, Nichelatti M, Sgoifo A, Ponzio M, Sterzi R, et al. Endovascular treatment for acute ischemic stroke. N Engl J Med. 2013;368: 904–913. 10.1056/NEJMoa1213701 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Kidwell CS, Jahan R, Gornbein J, Alger JR, Nenov V, Ajani Z, et al. A trial of imaging selection and endovascular treatment for ischemic stroke. N Engl J Med. 2013;368: 914–923. 10.1056/NEJMoa1212793 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Lee M, Hong KS, Saver JL Efficacy of intra-arterial fibrinolysis for acute ischemic stroke: meta-analysis of randomized controlled trials. Stroke. 2010;41: 932–937. 10.1161/STROKEAHA.109.574335 [DOI] [PubMed] [Google Scholar]
- 12. Fields JD, Khatri P, Nesbit GM, Liu KC, Barnwell SL, Lutsep HL, et al. Meta-analysis of randomized intra-arterial thrombolytic trials for the treatment of acute stroke due to middle cerebral artery occlusion. J Neurointerv Surg. 2011;3: 151–155. 10.1136/jnis.2010.002766 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Nam J, Jing H, O'Reilly D Intra-arterial thrombolysis vs. standard treatment or intravenous thrombolysis in adults with acute ischemic stroke: a systematic review and meta-analysis. Int J Stroke. 2015. January;10:13–22. 10.1111/j.1747-4949.2012.00914.x [DOI] [PubMed] [Google Scholar]
- 14. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343: d5928 10.1136/bmj.d5928 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6: [e1000097]. 10.1371/journal.pmed.1000097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. DerSimonian R, Laird N Meta-analysis in clinical trials. Control Clin Trials. 1986;7: 177–188. [DOI] [PubMed] [Google Scholar]
- 17. Ciccone A, Valvassori L, Ponzio M, Ballabio E, Gasparotti R, Sessa M, et al. Intra-arterial or intravenous thrombolysis for acute ischemic stroke? The SYNTHESIS pilot trial. J Neurointerv Surg. 2010;2: 74–79. 10.1136/jnis.2009.001388 [DOI] [PubMed] [Google Scholar]
- 18. del Zoppo GJ, Higashida RT, Furlan AJ, Pessin MS, Rowley HA, Gent M. PROACT: a phase II randomized trial of recombinant pro-urokinase by direct arterial delivery in acute middle cerebral artery stroke. PROACT Investigators. Prolyse in Acute Cerebral Thromboembolism. Stroke. 1998;29: 4–11. [DOI] [PubMed] [Google Scholar]
- 19. Ducrocq X, Bracard S, Taillandier L, Anxionnat R, Lacour JC, Guillemin F, et al. Comparison of intravenous and intra-arterial urokinase thrombolysis for acute ischaemic stroke. J Neuroradiol. 2005;32: 26–32. [DOI] [PubMed] [Google Scholar]
- 20. Keris V, Rudnicka S, Vorona V, Enina G, Tilgale B, Fricbergs J. Combined intraarterial/intravenous thrombolysis for acute ischemic stroke. AJNR Am J Neuroradiol. 2001;22: 352–358. [PMC free article] [PubMed] [Google Scholar]
- 21. Macleod MR, Davis SM, Mitchell PJ, Gerraty RP, Fitt G, Hankey GJ, et al. Results of a multicentre, randomised controlled trial of intra-arterial urokinase in the treatment of acute posterior circulation ischaemic stroke. Cerebrovasc Dis. 2005;20: 12–17. [DOI] [PubMed] [Google Scholar]
- 22. Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke. 2007;38: 967–973. [DOI] [PubMed] [Google Scholar]
- 23. Tomsick T, Brott T, Barsan W, Broderick J, Haley EC, Spilker J, et al. Prognostic value of the hyperdense middle cerebral artery sign and stroke scale score before ultraearly thrombolytic therapy. AJNR Am J Neuroradiol. 1996;17: 79–85. [PMC free article] [PubMed] [Google Scholar]
- 24. Qureshi AI Endovascular treatment of cerebrovascular diseases and intracranial neoplasms. Lancet. 2004;363: 804–813. [DOI] [PubMed] [Google Scholar]
- 25. Demchuk AM, Goyal M, Yeatts SD, Carrozzella J, Foster LD, Qazi E, et al. Recanalization and clinical outcome of occlusion sites at baseline CT angiography in the Interventional Management of Stroke III trial. Radiology. 2014;273:202–10. 10.1148/radiol.14132649 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix A: PubMed search Strategy. Appendix B: Grading Quality of the Evidence and Recommendations. Table A: PRISMA Checklist. Table B: GRADE evaluation of quality of evidence. Table C: List of excluded studies. Figure A: Cumulative meta-analysis (i.e. effects over time). Figure B: Forest plots showing any intracranial hemorrhage between endovascular therapy and controls. Figure C: Forest plot showing mortality in endovascular therapy vs controls. Figure C1: IA thrombolysis only vs mechanical device use. Figure C2: Comparator includes IV thrombolysis vs no thrombolysis. Figure C3: Studies that required vessel occlusion vs studies did not require vessel occlusion status. Figure D: Forest plot showing any intracranial hemorrhage in endovascular therapy vs controls. Figure D1: IA thrombolysis only vs mechanical device use. Figure D2: Comparator includes IV thrombolysis vs no thrombolysis. Figure D3: Studies that required vessel occlusion vs studies did not require vessel occlusion status. Figure E: Forest plot showing symptomatic intracranial hemorrhage in endovascular therapy vs controls. Figure E1: IA thrombolysis only vs mechanical device use. Figure E2: Comparator includes IV thrombolysis vs no thrombolysis. Figure E3: Studies that required vessel occlusion vs studies did not require vessel occlusion status. Figure F: Funnel Plots and Egger’s test for asymmetry of the funnel plot (p<0.1 for asymmetry). Figure F1: Primary outcome: Rankin <3. Egger’s test: p value = 0.2. Figure F2: Secondary outcome: Mortality. Egger’s test: p value = 0.2. Figure F3: Secondary outcome: Any ICH. Egger’s test: p value = 0.03. Figure F4: Secondary outcome: Symptomatic ICH. Egger’s test: p value = 0.06. Figure G: Absolute risk differences (ARD) for the secondary outcomes. Figure G1: Mortality. Figure G2: Symptomatic ICH.
(DOCX)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.