

Abstract
Lipoma arborescens is villous proliferation of synovium and is often unilateral in the absence of any systemic disease. We report a case of 54 year old male presenting with bilateral lipoma arborescens associated with osteoarthritis. The diagnosis is often difficult due to similar symptomatology of lipoma arborescens and osteoarthritis.
Keywords: Arthroscopy, Lipoma, Magnetic resonance imaging
1. Introduction
Lipoma arborescens (LA) is a rare, benign intraarticular pathology of knee joint. The aetiology of LA is not known. The lesion is characterised by hypertrophied villi, focal lymphoplasmacytic infiltration and lipocytes.1 It can involve any joint but predisposition is for the knee joint and especially the suprapatellar pouch.2 The diagnosis is usually delayed due to its benign nature and rare occurrence. However it was further complicated in this case due associated osteoarthritis.
2. Case presentation
A 54 year old male presented to our outpatient department with swelling in both knees for the previous one year. The swelling was gradual in onset and involving the right knee followed by left knee. Mild pain was associated with swelling. There was no history of trauma, fever, involvement of other joints or morning stiffness.
On examination, there was fullness in the suprapatellar and parapatellar areas in bilateral knees. The swelling was more prominent in right knee (Fig. 1). There was associated medial joint line tenderness and synovial thickening in suprapatellar region. The range of motion was 0°–120°. The cruciates and collaterals were found to be intact clinically. There were no signs of any mechanical blockage. There was no distal neurovascular deficit. Rest of the clinical examination was unremarkable.
Fig. 1.

Pre operative image showing swelling of both knees more on right side.
The complete rheumatological work up of the patient was done and the patient was investigated for rheumatoid factor, serum uric acid, anti nuclear antibody, anti ds DNA besides the routine blood investigations. All investigations were within normal limits. However radiographic examination of bilateral knees suggested features of osteoarthritis (medial joint space narrowing, osteophytes and loose bodies) and increased soft tissue shadow (Fig. 2). A provisional diagnosis of suprapatellar bursitis was made and ultrasonographic (USG) examination of bilateral knees was done which revealed hyperehoic frond like projections of the synovium with effusion (Fig. 3), suggestive of lipoma arborescens. Magnetic resonance imaging of both the knees showed with joint effusion, synovial proliferation with projections, fat signal intensity on all pulse sequences and suppression of signal with fat selective presaturation (Fig. 4). The patient was advised arthroscopic synovectomy for both knees.
Fig. 2.

Radiograph showing features of osteoarthritis and increased soft tissue shadow in suprapatellar region.
Fig. 3.

Ultrasound examination of both knees revealing joint effusion, synovial proliferation and synovial projections (white arrow).
Fig. 4.

Saggital and transverse section of MRI showing synovial proliferation (white arrows), joint effusion (red-black stars) and synovial projections (yellow arrows).
The patient underwent arthroscopic synovectomy for the more symptomatic right knee. Before undergoing arthroscopy, both knee joints were aspirated and yellowish coloured fluid was obtained and was sent for biochemical examination (especially urate crystals due to the yellowish colour of the fluid) and culture sensitivity. The biochemical and culture sensitivity reports were suggestive of inflammatory pathology. Arthroscopic examination of the right knee revealed numerous yellowish frond like projections in the suprapatellar pouch with degenerative changes in cartilage of medial and lateral compartment (Fig. 5). Arthroscopic synovectomy of the right knee was carried out using 5 mm aggressive shaver with four portal interchanging technique and completion of procedure was ensured (Fig. 6). Histopathological examination of the tissue showed fibrous tissue and adipose cells in the subsynovial region leading to villous expansion. The villi were covered by hyperplastic inflamed synovium (Fig. 7).
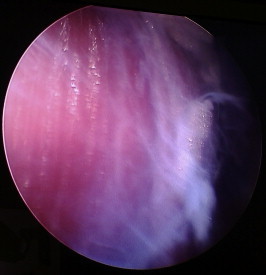
Fig. 5.

Arthroscopic image showing multiple frond like projections and loss of cartilage in the medial and lateral compartment of knee.
Fig. 6.
End point arthroscopic image showing underlying muscle after complete synovectomy in the supra patella pouch.
Fig. 7.

Histopathological image revealing hyperplastic inflammed synovium (black arrow) and fibrous tissue along with adipose cells (black star).
Post operatively, there was decrease in swelling and pain in right knee. Quadriceps exercises were initiated immediately during the post operative period. He was allowed to bear weight on first postoperative day and the patient returned to his previous occupation (college lecturer) in one month. The range of movement at the right knee joint was same as prior to arthroscopic synovectomy. The patient was advised arthroscopic synovectomy of the left knee also, however the same was declined by him as the left knee had mild pain. There was no recurrence at one year follow up.
3. Discussion
Lipoma arborescens is a rare synovial disorder mainly affecting the knee joint and especially the suprapatellar pouch. The patient present with insidious onset of swelling of knee joint followed by pain. Few patients experience mechanical symptoms. LA can involve other joints like elbow, hip, wrist, shoulder and ankle.3–5 It may involve extra articular sites like synovial sheaths of tendon, bicipitoradial6 and sub deltoid bursae.7
The aetiology of this condition is not known. It may associated with rheumatoid arthritis,8 psoriatic arthritis9 or multiple joint involvement in fat metabolism disorders.10 There are many reports of unilateral and bilateral knee involvement with lipoma arborescens but very few cases of bilateral lipoma arborescens of the knee with osteoarthritis have been reported to date. Xiao et al had hypothesised that there is synovial proliferation due to inflammation induced by osteoarthritis and subsequently adipose differentiation of the hypertrophied synovium.11 Al ismail et al12 and Hubscher et al13 had also proposed inflammation and mechanical factors in etiopathogenesis of osteoarthritis secondary to lipoma arborescens. Rao et al14 had proposed that LA could result from inappropriate fat deposition and degenerative disease of the joints. Moreover, the cases described in literature were of older age group in which the osteoarthritis is as such common. The association of osteoarthritis with lipoma arborescens could have been due to mechanical factors or both the entities may have coexisted in the same joint. There is no conclusive evidence to establish cause and effect relationship between osteoarthritis and LA.
Macroscopically lipoma arborescens appears as broad based polyps or villi. These villi are filled with adipocytes and sometimes congestion may be present due to capillary infiltration. The overlying synovium may contain mononuclear cells and enlarged synovial cells with reactive nuclei.15
Ultrasonographic features of this condition are hyper echoic frond like mass especially in the suprapatellar area with effusion. With dynamic compression and manipulations there is bending of the mass which suggests its pliable nature.16
Magnetic resonance imaging is the investigation of choice in diagnosis of this condition.17 The features suggestive of lipoma arborescens are synovial fronds with fat signals on all sequences, joint effusion and absence of magnetic susceptibility effects from haemosiderin. Though the features are highly suggestive but conditions like synovial lipoma, pigmented villonodular synovitis, synovial chondromatosis, synovial heamagioma and rheumatoid arthritis must be kept in the differentials. Pigmented villonodular synovitis presents with diffuse low intensity signals on T1 and T2 weighted images while synovial chondromatosis shows variable intensity signals due to presence of cartilage. The distinction from intraarticular lipoma can be done with both macroscopic and microscopic appearances. Intraarticular lipoma lacks villous fronds on arthroscopic visualisation. Microscopically it can be differentiated from LA by lack of villous proliferation of synovial tissue and fatty replacement of underlying connective tissue.
The treatment includes arthroscopic synovectomy,17 open synovectomy18 and joint replacement in few selected cases of associated advanced osteoarthritis (Table 1). Arthrotomy and synovectomy19 is the recommended treatment in management of LA, however few authors20–22 have recommended arthroscopic synovectomy over open procedure in large joints. Open synovectomy may miss the posterior aspect of knee while arthroscopic procedure can access all areas and is also associated with lesser morbidity.23
Table 1.
Summary of reported cases of bilateral lipoma arborescens with osteoarthritis.
| S. no. | Authors | Year | Number of cases | Age | Sex | Duration of symptoms | Treatment modality | Result |
|---|---|---|---|---|---|---|---|---|
| 1 | Khalid Al-Ismail et al10 | 2002 | 1 | 38 Y | M | Six months | Patient declined surgery and treated conservatively | Not reported |
| 2 | Xiao J et al9 | 2011 | 3 | 66 Y | F | Three years | Left total knee replacement, refused surgery on right side | No recurrence on left side, disease progression on right side |
| 68 Y | M | Three years | Bilateral staged total knee replacement | No recurrence at one year follow up | ||||
| 50 Y | F | Ten years in right and five years in left knee | Bilateral staged total knee replacement | No recurrence at six months follow up | ||||
| 3 | Present case | 2014 | 1 | 54 Y | M | One year | Arthroscopic synovectomy | No recurrence at one year |
LA has been treated by few authors with radiosynovectomy using yttrium-9024 and chemosynovectomy with osmic acid.25 There was no recurrence in both the cases. However these procedures cannot be recommended as standard procedure in the management of LA based upon single case reports.
4. Conclusion
Lipoma arborescens is a rare intrarticular benign tumour. It may be associated with osteoarthritis though the causal relationship has not been established yet. Arthroscopic synovectomy can provide adequate relief in pain and swelling of the knee joint. This entity should be suspected in cases presenting with bilateral knee swelling in the absence of any systemic disease.
Conflicts of interest
All authors have none to declare.
References
- 1.Tamburrini O., Milano C., Arcuri P.P., Mariconda M., Porpiglia H., Perri G. Villous-lipomatous proliferation of synovial membrane of the knee (lipoma arborescens). Magnetic resonance findings. Radiol Med. 1998 Mar;95:143–147. [PubMed] [Google Scholar]
- 2.Kloen P., Keel S.B., Chandler H.P., Geiger R.H., Zarins B., Rosenberg A.E. Lipoma arborescens of the knee. J Bone Joint Surg Br. 1998;80:298–301. doi: 10.1302/0301-620x.80b2.8244. [DOI] [PubMed] [Google Scholar]
- 3.Martin S., Hernandez L., Romero J. Diagnostic imaging of lipoma arborescens. Skeletal Radiol. 1998;27:325–329. doi: 10.1007/s002560050390. [DOI] [PubMed] [Google Scholar]
- 4.Chae E.Y., Chung H.W., Shin M.J., Lee S.H. Lipoma arborescens of the glenohumeral joint causing bone erosion: MRI features with gadolinium enhancement. Skeletal Radiol. 2009;38:815–818. doi: 10.1007/s00256-009-0686-x. [DOI] [PubMed] [Google Scholar]
- 5.Levadoux M., Gadea J., Flandrin P., Carlos E., Aswad R., Panuel M. Lipoma arborescens of the elbow: a case report. J Hand Surg Am. 2000 May;25:580–584. doi: 10.1053/jhsu.2000.6002. [DOI] [PubMed] [Google Scholar]
- 6.Dinauer P., Bojescul J.A., Kaplan K.J., Litts C. Bilateral lipoma arborescens of the bicipitoradial bursa. Skeletal Radiol. 2002;31:661–665. doi: 10.1007/s00256-002-0569-x. [DOI] [PubMed] [Google Scholar]
- 7.Pandey T., Alkhulaifi Y. Bilateral lipoma arborescens of the subdeltoid bursa. Australas Radiol. 2006 Oct;50:487–489. doi: 10.1111/j.1440-1673.2006.01633.x. [DOI] [PubMed] [Google Scholar]
- 8.Coll J.P., Ragsdale B.D., Chow B., Daughters T.C. Best cases from the AFIP: lipoma arborescens of the knees in a patient with rheumatoid arthritis. Radiographics. 2011 Mar-Apr;31:333–337. doi: 10.1148/rg.312095209. [DOI] [PubMed] [Google Scholar]
- 9.Fraser A.R., Perry M.E., Crilly A., Reilly J.H., Hueber A.J., McInnes I.B. Lipoma arborescens coexisting with psoriatic arthritis releases tumour necrosis factor alpha and matrix metalloproteinase 3. Ann Rheum Dis. 2010;69:776–777. doi: 10.1136/ard.2008.106047. [DOI] [PubMed] [Google Scholar]
- 10.Siva C., Brasington R., Totty W., Sotelo A., Atkinson J. Synovial lipomatosis [lipoma arborescens] affecting multiple joints in a patient with congenital short bowel syndrome. J Rheumatol. 2002 May;29:1088–1092. [PubMed] [Google Scholar]
- 11.Xiao J., Xu Y., Wang J., Feng J., Shi Z. Bilateral knee lipoma arborescens combined with osteoarthritis in elderly patients. J Int Med Res. 2011;39:1563–1569. doi: 10.1177/147323001103900448. [DOI] [PubMed] [Google Scholar]
- 12.Al-Ismail K., Torreggiani W.C., Al-Sheikh F., Keogh C., Munk P.L. Bilateral lipoma arborescens associated with early osteoarthritis. Eur Radiol. 2002 Nov;12:2799–2802. doi: 10.1007/s00330-001-1249-2. [DOI] [PubMed] [Google Scholar]
- 13.Hubscher O., Costanza E., Elsner B. Chronic monoarthritis due to lipoma arborescens. J Rheumatol. 1990;17:861–862. [PubMed] [Google Scholar]
- 14.Rao S., Rajkumar A., Elizabeth M.J., Ganesan V., Kuruvilla S. Pathology of synovial lipomatosis and its clinical significance. J Lab Physicians. 2011 Jul–Dec;3:84–88. doi: 10.4103/0974-2727.86839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bernardo A., Bernardes M., Brito I., Vieira A., Ventura F. Synovial lipoma arborescens. Acta Med Port. 2004;17:325–328. [PubMed] [Google Scholar]
- 16.Learch T.J., Braaton M. Lipoma arborescens: high-resolution ultrasonographic findings. J Ultrasound Med. 2000;19:385–389. doi: 10.7863/jum.2000.19.6.385. [DOI] [PubMed] [Google Scholar]
- 17.Yah C.H., Wong J.W.K., Yip D.K.H. Bilateral knee lipoma arborescens: a case report. J Orthop Surg (Hong Kong) 2008;16:107–110. doi: 10.1177/230949900801600125. [DOI] [PubMed] [Google Scholar]
- 18.Tiao W.M., Yeh L.R., Lu Y.C., Liang H.L., Chen C.K. Lipoma arborescens of the knee: a case report. J Formos Med Assoc. 2001;100:412–415. [PubMed] [Google Scholar]
- 19.Hallel T., Lew S., Bansal M. Villous lipomatous proliferation of the synovial membrane (lipoma arborescens) J Bone Joint Surg Am. 1988 Feb;70:264–270. [PubMed] [Google Scholar]
- 20.Blais R.E., LaPrade R.F., Chaljub G., Adesokan A. The arthroscopic appearance of lipoma arborescens of the knee. Arthroscopy. 1995 Oct;11:623–627. doi: 10.1016/0749-8063(95)90144-2. [DOI] [PubMed] [Google Scholar]
- 21.Bernstein A.D., Jazrawi L.M., Rose D.J. Arthroscopic treatment of an intra-articular lipoma of the knee joint. Arthroscopy. 2001 May;17:539–541. doi: 10.1053/jars.2001.22414. [DOI] [PubMed] [Google Scholar]
- 22.Yildiz C., Deveci M.S., Ozcan A., Saraçoğlu H.I., Erler K., Basbozkurt M. Lipoma arborescens (diffuse articular lipomatosis) J South Orthop Assoc. 2003 Fall;12(3):163–166. [PubMed] [Google Scholar]
- 23.Davies A.P., Blewitt N. Lipoma arborescens of the knee. Knee. 2005 Oct;12:394–396. doi: 10.1016/j.knee.2005.01.003. [DOI] [PubMed] [Google Scholar]
- 24.Erselcan T., Bulut O., Bulut S. Lipoma arborescens; successfully treated by yttrium-90 radiosynovectomy. Ann Nucl Med. 2003 Oct;17:593–596. doi: 10.1007/BF03006673. [DOI] [PubMed] [Google Scholar]
- 25.Nisolle J.F., Boutsen Y., Legaye J., Bodart E., Parmentier J.M., Esselinckx W. Monoarticular chronic synovitis in a child. Br J Rheumatol. 1998 Nov;37:1243–1246. doi: 10.1093/rheumatology/37.11.1243. [DOI] [PubMed] [Google Scholar]