

Abstract
To comprehensively evaluate the association between rs7517847 and rs2201841 polymorphisms in the Interleukin-23 (IL-23) receptor gene and ankylosing spondylitis (AS), a meta-analysis was performed. The Pubmed, Embase, MEDLINE, Cochrane, China National Knowledge Infrastructure (CNKI), VIP, Wanfang and China Biology Medicine disc (CBMdisc) databases were searched to identify eligible studies on rs7517847 and rs2201841 polymorphisms in the IL-23 receptor gene and AS that were published through September 2014. Data of interest were extracted from each study, and the meta-analysis was performed using STATA 12.0. Four studies were eligible for the meta-analysis and included a total patient population of 2,465. With regards to rs7517847, the current study showed that the genotype GG and allele G might play a protective role during AS (OR = 0.76, 95% CI [0.59–0.99]; OR = 0.88, 95% CI [0.78–0.99] for homozygote and allelic models, respectively). However, according to the meta-analysis, there was no statistical association between the genotype or allele of rs2201841 and an individual’s susceptibility to AS in all genetic models. In conclusion, it was the IL-23 rs7517847 polymorphism rather than the rs2201841 polymorphism that had a statistical association with AS. Nevertheless, more evidence is needed to confirm this result. Consequently, it is necessary to carry out more high-quality studies to confirm the associations between these two single nucleotide polymorphisms and AS.
Keywords: Ankylosing spondylitis, SNPs, Meta-analysis, Interleukin-23 receptor
Introduction
Ankylosing spondylitis (AS) is an autoimmune disease that features chronic inflammation and ossification of the sacroiliac articulation and enthesis of the tendon. Approximately 0.2% of the general population suffers from AS, and its incidence is 0.1–1.4%, 0.2–0.54%, 0.86%, and 2% in European, Chinese, Caucasian, and HLA-B27-positive populations, respectively (Braun & Sieper, 2007; Zeng et al., 2008; Braun et al., 1998; Goldman & Schafer, 2012). Moreover, when one twin suffers from AS, the probability that the other is also an AS patient is greater than 90% (Brown et al., 1997). An obvious gender tendency has been found in AS, i.e., men are more susceptible to the disease compared with women (Goldman & Schafer, 2012).
The etiology and mechanisms behind AS remain unclear. Scientists have thought that susceptibility to AS is strongly affected by heredity. Although HLA-B27 is a confirmed genetic risk factor, not all AS cases can be explained by genetic association, which implies that other factors are also important (Vegvari et al., 2009). Wang et al. (2010) found that there was a significantly higher mRNA expression of the interleukin-23 receptor (IL-23R) gene in peripheral blood monocytes of AS patients compared with those of normal controls. When IL-23 was overexpressed, CD4- and CD8- T cells were affected (Sherlock et al., 2012), which led to peripheral enthesitis and the formation of new bone (Miceli-Richard, 2004). Another study showed that the IL-17/IL-23 axis could be a potential target for AS treatment (Di Meglio et al., 2013). In accordance with a genome-wide association study (GWAS), it was also shown that there was an association between IL-23R and AS in Caucasian patients (Burton et al., 2007).
Thus far, several meta-analyses have investigated the relationship between several single nucleotide polymorphisms (SNPs) and AS; they have found that several IL-23R SNPs were associated with AS in Caucasian populations but that others were unrelated to AS in Asian patients (Karaderi et al., 2009; Chen et al., 2012; Duan et al., 2012; Pimentel-Santos et al., 2009). No meta-analysis has yet examined the relationship between SNPs rs7517847 and rs2201841 and AS. The association between these two SNPs and AS was borderline significant only (Sáfrány et al., 2009; Dong et al., 2013). These negative results may have been caused by a small included population. The current study uses meta-analysis to determine the association between rs7517847 and rs2201841 in IL-23R SNPs and AS for the first time. This study provides more comprehensive evidence for rheumatologists considering the association between IL-23R SNPs and AS.
Materials and Methods
Search strategy and selection criteria
A comprehensive search of databases such as Pubmed, Embase, Medline, Cochrane, China National Knowledge Infrastructure (CNKI), VIP, Wanfang and China Biology Medicine disc (CBMdisc) databases was conducted. Searches included literature dated from database origin to September 2014, and the following key words were used: “IL-23” OR “interleukin-23”, “Ankylosing Spondylitis” OR “AS”, and “polymorphism” OR “polymorphisms”. In the CNKI, VIP, Wanfang and CBMdisc databases we searched for corresponding words in Chinese characters. The full search strategy for the Embase database is presented in Table 1. No language restrictions were used. A manual search for references beyond those in the above-mentioned databases was also implemented. For studies that did not describe genetic distribution data in detail, email correspondence with the main authors was used to complete the data. Titles and abstracts were independently screened by two authors to identify potentially related studies. Full-text versions of the identified studies were reviewed to select those that met the eligibility criteria. The identified studies were subjected to a final confirmation before inclusion in the meta-analysis.
Table 1. The full search strategy for Embase.
| #1 | ‘interleukin’/exp OR interleukin AND 23 |
| #2 | il AND 23 |
| #3 | #1 OR #2 |
| #4 | ankylosing AND (‘spondylitis’/exp OR spondylitis) |
| #5 | ankylopoietic AND (‘spondylarthritis’/exp OR spondylarthritis) |
| #6 | ankylopoietic AND (‘spondylitis’/exp OR spondylitis) |
| #7 | ankylosing AND (‘spine’/exp OR spine) |
| #8 | ankylosing AND spondylitis |
| #9 | Ankylosing AND (‘spondylarthritis’/exp OR spondylarthritis) |
| #10 | Ankylosing AND (‘spondylarthrosis’/exp OR spondylarthrosis) |
| #11 | ‘ankylosis’/exp OR ankylosis AND (‘spondylitis’/exp OR spondylitis) |
| #12 | Ankylotic AND (‘spondylitis’/exp OR spondylitis) |
| #13 | Bechterew AND (‘disease’/exp OR disease) |
| #14 | Bekhterev AND (‘disease’/exp OR disease) |
| #15 | Morbus AND bechterew |
| #16 | Spinal AND (‘ankylosis’/exp OR ankylosis) |
| #17 | ‘spine’/exp OR spine AND (‘ankylosis’/exp OR ankylosis) |
| #18 | ‘spondylarthritis’/exp OR spondylarthritis AND ankylopoietica |
| #19 | ‘spondylarthritis’/exp OR spondylarthritis AND ankylosans |
| #20 | ‘spondylarthrosis’/exp OR spondylarthrosis AND ankylopoietica |
| #21 | ‘spondylitis’/exp OR spondylitis AND ankylopoetica |
| #22 | ‘spondylitis’/exp OR spondylitis AND ankylopoietica |
| #23 | Spondylitis, AND ankylosing |
| #24 | ‘spondyloarthritis’/exp OR spondyloarthritis AND ankylopoietica |
| #25 | Vertebral and (‘ankylosis’/exp OR ankylosis) |
| #26 | #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 |
| #27 | ‘single nucleotide polymorphism’/exp |
| #28 | Polymorphism, AND single AND (‘nucleotide’/exp OR nucleotide) |
| #29 | Single AND (‘nucleotide’/exp OR nucleotide) AND polymorphism |
| #30 | #27 OR #28 OR #29 |
| #31 | #3 AND #26 AND #30 |
Inclusion criteria
Investigations that met the eligibility criteria were included in the analysis, and any disagreements were resolved by discussion between the authors (Xu B and Ma JX). In cases where a consensus could not be reached, a third author was involved to make a final decision. Studies meeting the following criteria were included in the meta-analysis: (1) investigation evaluating the association between IL-23R rs7517847 or rs2201841 polymorphisms and AS susceptibility; (2) a case-control study or GWAS; (3) sufficiently available public data that could be extracted for further analysis, such as genotype distribution, odds ratio (OR) and 95% confidence interval (95% CI); and (4) a SNP distribution according to Hardy-Weinberg equilibrium (HWE) was included, which means high quality in design and conduct of genetic association studies. In cases where two studies examined the same or overlapping populations, the study with a larger sample size was included in the analysis.
Studies for which contact with the main author could not be reached to supply information about relevant data were excluded.
Data extraction and quality assessment
The relevant characteristics of the included investigations were identified and recorded by two authors, including the first author of the study, publication year, country, ethnicity of subjects, relevant SNPs, patient demographics, test method used for genotype, whether the genotype distribution was in accordance with Hardy-Weinberg Equilibrium (HWE) and source of the samples tested. To acquire precise results for the current study, email contact with the main author of the investigation was performed if the included study did not contain public data. Quality assessment of studies included in the meta-analysis was conducted by two authors using the Newcastle-Ottawa Scale (NOS) (Cota et al., 2013). Scores were given for subject selection (i.e., adequateness of the case definition, representativeness of the cases, selection of controls, and definition of controls) and the comparability of the groups (i.e., comparability of cases and controls on the basis of the design or analysis) as well as measurement of exposure (i.e., ascertainment of exposure, same method of ascertainment for cases and controls, and non-response rate). NOS scores ranged from 0 to 9. Studies with a NOS score ≥6 were considered to be high quality. Higgins I2 was used to evaluate the heterogeneity of the investigations. Subgroup analysis by ethnicity was executed if the number of investigations in each ethnic group was two or more. Gender subgroup analysis could not be done because there was no relevant data. Sensitivity analysis was carried out by evaluating the overall results of meta-analysis when each study was removed to detect the stability of trials included.
Statistical analysis
The strength of the association between IL-23R rs7517847 and rs2201841 polymorphisms and AS susceptibility was evaluated using the Odds Ratio (OR). At the same time, precision was measured by 95% CI. A random-effects model was used in the current study. With respect to rs7517847 and rs2201841, the homozygote model, heterozygote model, recessive model, dominant model and allelic model were used to estimate susceptibility to AS in current study. Statistical analysis of the extracted data was carried out using STATA 12.0.
Results
Search results
As a result of the search strategy presented in Fig. 1, 215 English-language studies and 208 Chinese-language studies were obtained. In addition, one study was added by searching through references (Zhu, Yang & Gao, 2009). Among the search results, 420 trials were excluded for the following reasons: (1) 116 were duplicate articles; (2) 281 did not discuss the association between IL-23R SNPs and AS in the title and abstract; (3) 20 did not discuss the association between rs7517847 and rs2201841 and AS in the full-text; (4) two contained genotype distribution data that were not publicly available, and email contact with the main authors could not be achieved; and (5) two studies assessed overlapping populations (Sáfrány et al., 2009; Szabo et al., 2013). For these studies, those that included a larger sample population were included in the analysis, as conducted by Sáfrány et al. (2009). Finally, four trials (Sáfrány et al., 2009; Dong et al., 2013; Zhu, Yang & Gao, 2009; Rueda et al., 2008) on rs7517847 and two trials (Sáfrány et al., 2009; Zhu, Yang & Gao, 2009) on rs2201841 were included in the current study. The included studies had case-control designs with 1,006 patients in the AS group and 1,190 people in the control group for rs7517847. For rs2201841, 322 patients were included in the AS group, and 255 people were included in the control group in the current study. The basic characteristics of included studies were listed in Table 2. Patients who were diagnosed with AS according to the New York modified criteria (Goei et al., 1985) and healthy people from Chinese, Hungarian and Spanish populations were included in the current study. All trials included in this meta-analysis were replication studies according to HWE. The NOS score of studies included in the meta-analysis ranged from 6 to 7, as presented in Table 3. Moreover, genotype distribution of both SNPs in the AS and control groups is presented in Table 4.
Figure 1. PRISMA flowchart of number of studies.
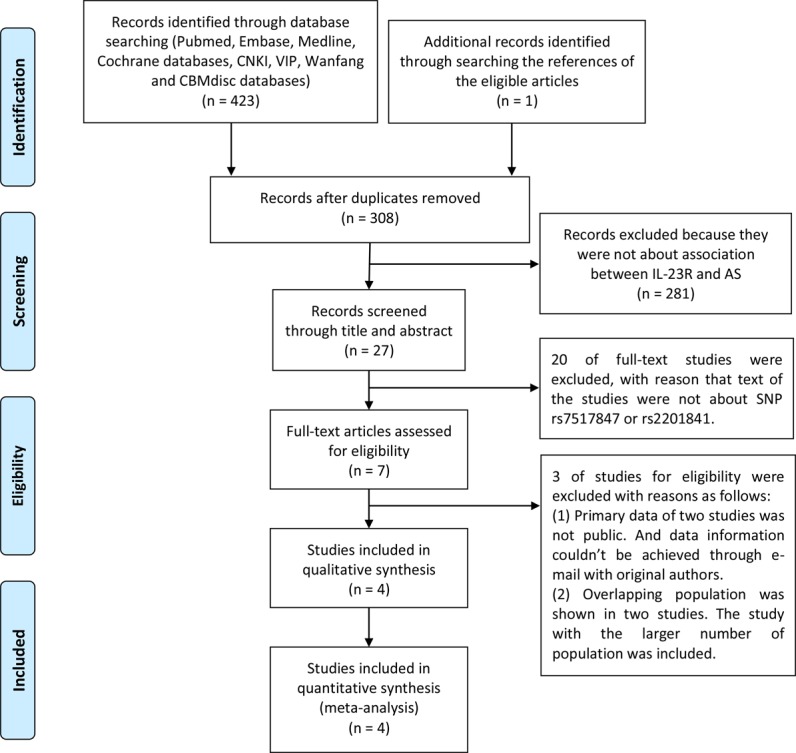
Table 2. Main characteristics of studies included in this meta-analysis.
| Author | Year | Country | Ethnicity | SNP | AS group | Control group | Test method | HWE | Source |
|---|---|---|---|---|---|---|---|---|---|
| Dong H | 2013 | China | Asian | rs7517847 | 291 | 312 | PCR-RFLP | Y | Blood |
| Zhu XQ | 2009 | China | Asian | rs7517847 | 144 | 143 | PCR-HRM | Y | Blood |
| Zhu XQ | 2009 | China | Asian | rs2201841 | 116 | 102 | PCR-HRM | Y | Blood |
| Sáfrány E | 2009 | Hungary | Caucasian | rs7517847 rs2201841 | 206 | 235 | PCR-RFLP | Y | Blood |
| Rueda B | 2008 | Spanish | Caucasian | rs7517847 | 365 | 500 | Taqman | Y | Blood |
Notes.
- Author
- first author
- HWE
- Hardy-Weinberg Equilibrium
Table 3. Quality assessment of studies.
| Study included | Selection | Comparability | Exposure | Total |
|---|---|---|---|---|
| 1. Dong et al. (2013) | 3 | 2 | 2 | 7 |
| 2. Sáfrány et al. (2009) | 3 | 2 | 2 | 7 |
| 3. Zhu, Yang & Gao (2009) | 3 | 1 | 2 | 6 |
| 4. Rueda et al. (2008) | 3 | 1 | 2 | 6 |
Table 4. Genotype distribution of rs7517847 and rs2201841 associated with IL-23.
| rs7517847 | rs2201841 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author | Ethnicity | Group | TT | GT | GG | MAF | CC | CT | TT | MAF |
| Dong H | Asian | AS | 104 | 146 | 41 | 0.39 | – | – | – | – |
| control | 98 | 153 | 61 | 0.44 | – | – | – | – | ||
| Sáfrány E | Caucasian | AS | 67 | 115 | 24 | 0.40 | 26 | 89 | 91 | 0.34 |
| control | 69 | 126 | 40 | 0.44 | 15 | 102 | 118 | 0.28 | ||
| Zhu XQ | Asian | AS | 61 | 59 | 24 | 0.37 | 64 | 40 | 12 | 0.28 |
| control | 48 | 77 | 18 | 0.40 | 54 | 41 | 7 | 0.27 | ||
| Rueda B | Caucasian | AS | 140 | 172 | 53 | 0.38 | – | – | – | – |
| control | 182 | 238 | 80 | 0.40 | – | – | – | – | ||
Notes.
- –
- no available data
- MAF
- minor allelic frequencies
Overall results of the meta-analysis
ORs, P value, 95% CI and heterogeneity evaluation of meta-analysis for rs7517847 and rs2201841 are presented in Table 5 and Fig. 2 and in Table 6 and Fig. 3, respectively. The random effect model was applied to the studies. A comprehensive analysis of relevant SNPs was performed. Based on the meta-analysis results, there was a statistically significant association between the IL-23R rs7517847 polymorphism in the over-all population and AS susceptibility under two genetic models (homozygote model, i.e., GG vs. TT, were OR =0.76, 95% CI [0.59–0.99] and P = 0.038 and the allelic model, G vs. T, i.e., where OR = 0.88, 95% CI [0.78–0.99] and P = 0.032). The heterogeneity among studies under the two genetic models was I2 = 0, PH = 0.547 and I2 = 0, PH = 0.838, respectively, which indicated that there was no statistically significant heterogeneity among the trials for rs7517847. The analytical results presented in Table 6 implied that there was no statistically significant association between the IL-23R rs2201841 polymorphism and AS susceptibility under all of the genetic models tested.
Table 5. Meta-analysis of polymorphisms of rs7517847.
| SNP | n | Genetic model | OR (95% CI) | P | I 2 |
|---|---|---|---|---|---|
| rs7517847 | 4 | Homozygote model GG vs. TT | 0.76 (0.59, 0.99) | 0.038 | 0% |
| Heterozygote model GT vs. TT | 0.87 (0.73, 1.05) | 0.157 | 0% | ||
| Allelic model G vs. T | 0.88 (0.78, 0.99) | 0.032 | 0% | ||
| Recessive model GG vs. (TT + GT) | 0.82 (0.65, 1.03) | 0.090 | 28.2% | ||
| Dominant model (GG + GT) vs. TT | 0.85 (0.71, 1.01) | 0.066 | 0% |
Notes.
- n
- number of studies included
Figure 2. Forest plot of genetic association studies of rs7517847.
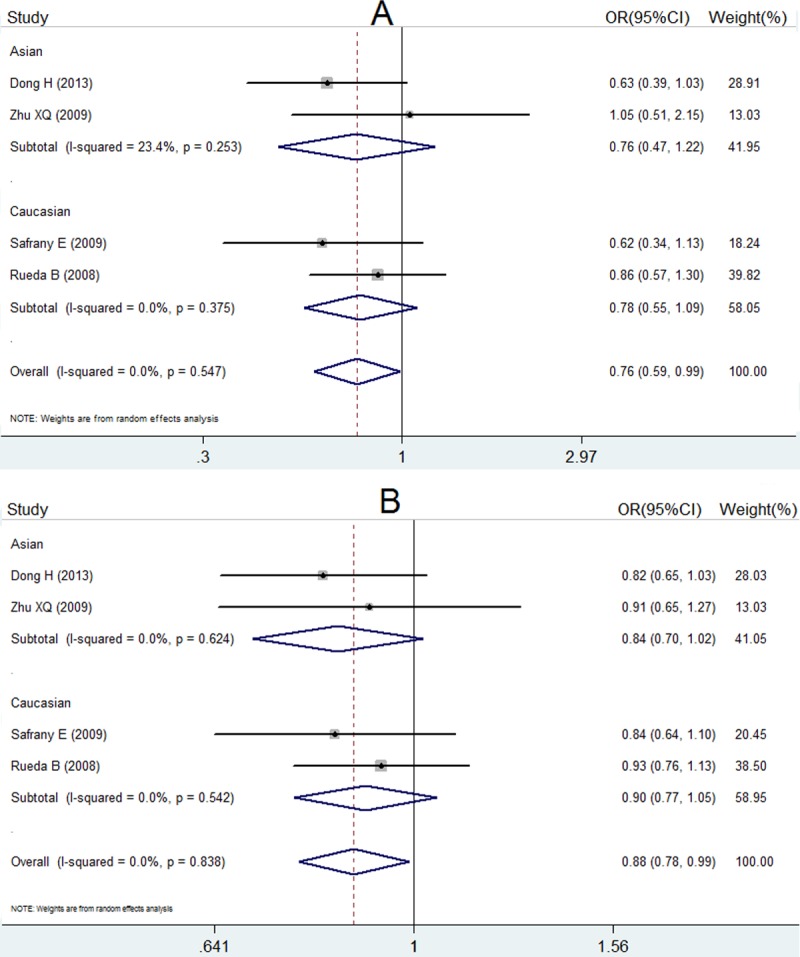
(A) genotype GG vs. TT; (B) allele G vs. allele T. The horizontal axis: axis of Odds Ratio (OR). The dotted line: mean value of overall OR.
Table 6. Meta-analysis of polymorphisms of rs2201841.
| SNP | n | Genetic model | OR (95% CI) | P | I 2 |
|---|---|---|---|---|---|
| rs2201841 | 2 | Homozygote model CC vs. TT | 0.87 (0.50, 1.51) | 0.631 | 0% |
| Heterozygote model CT vs. TT | 0.93 (0.62, 1.40) | 0.726 | 4.70% | ||
| Allelic model C vs. T | 0.99 (0.77, 1.27) | 0.915 | 0% | ||
| Recessive model CC vs. (TT + CT) | 1.04 (0.69, 1.55) | 0.866 | 0% | ||
| Dominant model (CC + CT) vs. TT | 0.94 (0.64, 1.38) | 0.746 | 0% |
Notes.
- n
- number of studies included
Figure 3. Forest plot of genetic association studies of rs2201841 homozygote model (CC vs. TT).

The horizontal axis: axis of Odds Ratio (OR). The dotted line: mean value of overall OR.
Results of subgroup analysis by ethnicity
A subgroup analysis by ethnicity (Asians and Caucasians) was conducted for rs7517847, and contained two trials (one with 435 and 455 people in the case and controls groups and a second with 571 and 735 people in the case and control group, respectively). The random effect model was applied to each genetic model in both the Asian and Caucasian populations.
In accordance with the results of the subgroup analysis, there was no statistically significant association between the IL-23R rs7517847 polymorphism and AS in the Asian or Caucasian populations, as presented in Table 7.
Table 7. Results of subgroup analysis of rs7517847 by ethnicity.
| Ethnicity | |||||
|---|---|---|---|---|---|
| Asian | Caucasian | ||||
| SNP rs7517847 | Genetic model | OR (95% CI) | P value | OR (95% CI) | P value |
| Homozygote model (GG/TT) | 0.74 (0.50–1.10) | 0.140 | 0.78 (0.55–1.09) | 0.143 | |
| Heterozygote model (GT/TT) | 0.79 (0.59–1.05) | 0.109 | 0.94 (0.74–1.20) | 0.613 | |
| Recessive model (GG/ GT + TT) | 0.84 (0.59–1.20) | 0.335 | 0.80 (0.59–1.09) | 0.161 | |
| Dominant model (GG + GT/TT) | 0.78 (0.59–1.02) | 0.071 | 0.90 (0.72–1.13) | 0.373 | |
| Allelic model (G/T) | 0.84 (0.70–1.02) | 0.080 | 0.90 (0.77–1.05) | 0.181 | |
Sensitivity analysis
A sensitivity analysis of trials investigating rs7517847 was carried out, aiming to evaluate the stability of the current study. After removing the study conducted by Sáfrány et al. (2009), we found that the OR for GG vs. TT changed from OR = 0.76 (95% CI [0.59–0.99], P = 0.038) to OR = 0.80 (95% CI [0.60–1.06] and P = 0.120) and the OR for G vs. T changed from OR = 0.88 (95% CI [0.78–0.99], P = 0.032) to OR = 0.88 (95% CI [0.77–1.01] and P = 0.078). After removing the study conducted by Dong et al. (2013), we found that the OR for GG vs. TT changed from OR = 0.76 (95% CI [0.59–0.99], P = 0.038) to OR = 0.82 (95% CI [0.60–1.11] and P = 0.203) and the OR for G vs. T changed from OR = 0.88 (95%CI [0.78–0.99], P = 0.032) to OR = 0.90 (95% CI [0.78–1.04] and P = 0.145). Excluding the other two studies, we found that the results of studies had not changed.
Discussion
As a member of the erythropoietin receptor superfamily, IL-23R influences the differentiation of CD4 T lymphocytes to IL-17-producing Th17 lymphocytes. During inflammation, IL-17 plays a destructive role, such as articulation of the cerebral, heart, lung and intestinal tissues. Several recent studies have indicated an association between IL-23R polymorphism and some autoimmune diseases, such as inflammatory bowel disease, multiple sclerosis and psoriasis (Duerr et al., 2006; Cargill et al., 2007; Nunez et al., 2008). Overall, four relevant meta-analyses about IL-23R and AS have been conducted and provided statistical evidence for the association between IL-23R polymorphisms and AS susceptibility (Karaderi et al., 2009; Chen et al., 2012; Duan et al., 2012; Pimentel-Santos et al., 2009). The results of two meta-analyses of large populations indicated that associations between 7 SNPs and 6 SNPs of IL-23R and AS existed in Britain and 7 other countries, respectively (Karaderi et al., 2009; Duan et al., 2012).
However, no associations existed for some SNPs in a Portuguese population (Pimentel-Santos et al., 2009) or five SNPs in an Asian population (Chen et al., 2012), in studies where fewer than 1,000 individuals were examined. Additionally, a number of other investigations have assessed the association between IL-23R rs7517847 and rs2201841 polymorphisms and AS susceptibility. However, the outcomes were not conclusive. To obtain a statistically credible result, four studies were included in this meta-analysis. In total, four trials (1,006 AS patients and 1,190 people in the control group) and two trials (322 AS patients and 255 people in the control group) were included for rs7517847 and rs2201841, respectively.
Although no statistically significant association between IL-23R rs7517847 and AS were identified in each of the included studies, the results of the current study showed that there was a statistically significant association between rs7517847 and AS in the overall population in the homozygote model and the allelic model after the four studies were pooled. We speculated that negative results shown in each study were due to the small sample sizes. Additionally, no evidence was obtained to prove the association between rs7517847 and ethnicity in the subgroup analysis. After excluding either the study conducted by Sáfrány et al. (2009) or that Dong et al. (2013), which were conducted in Hungary or China, respectively, we found that the P value of the remaining studies changed to be not significant. However, the odds ratio of the studies were actually fairly stable. (Sáfrány et al. (2009): as for GG vs. TT, OR =0.80, 95% CI [0.60–1.06] and P = 0.120; with respect to G vs. T, OR = 0.88, 95% CI [0.77–1.01] and P = 0.078 Dong et al. (2013): GG vs. TT: OR = 0.82, 95% CI [0.60–1.11] and P = 0.203; G vs. T: OR = 0.90, 95% CI [0.78–1.04] and P = 0.145). The sensitivity analysis was affected by removing the result of either Sáfrány et al. (2009) or Dong et al. (2013), possibly because the remaining sample size after removal of these studies was not sufficiently large. Thus, removing a study could greatly reduce the sample size and lead to changes in the sensitivity analysis. Additionally, no significant association between rs2201841 and AS susceptibility was found in any of the genetic models tested in the current study. The results obtained in this study suggest that the rs71517847 polymorphism might be a protective factor for AS in the overall population but that the rs2201841 polymorphism might not be associated with AS susceptibility. The author (Xu B) speculated that the negative results regarding rs2201841 could have been due to small sample size.
The current study has some limitations as follows. (1) The population included in this study was relatively small. Hence, type II error might exist and the credibility of the current study’s results may be weak. (2) A subgroup analysis of rs2201841 by ethnicity could not be conducted because the eligible studies in each ethnicity that were included in this study only involved one trial such that the association between IL-23R rs2201841 and AS by ethnicity was unknown. (3) There was only one country from Asia and two countries from Europe involved in the current study, which implies that the results of the current study are not representative. (4) Unfortunately, there is a lack of information about related studies for the black population. Therefore, the results of the current study are not comprehensive. (5) We were unable to include studies that have not been published, which might affect the publication bias.
Conclusion
In conclusion, the present meta-analysis showed that the IL-23R rs7517847 polymorphism may play a protective role in AS. However, no association between the rs2201841 polymorphism and AS susceptibility was found. Moreover, to obtain a credible and comprehensive conclusion to enable rheumatologists and researchers in related fields to comprehend the association between rs7517847 and rs2201841 and AS susceptibility, it is still essential to implement further investigations with a large number of samples from more countries to assess the associations between these two SNPs and AS.
Supplemental Information
Funding Statement
The authors declare there was no funding for this work.
Additional Information and Declarations
Competing Interests
The authors declare there are no competing interests.
Author Contributions
Bin Xu conceived and designed the experiments, performed the experiments, analyzed the data, wrote the paper, prepared figures and/or tables.
Jian-xiong Ma performed the experiments, analyzed the data.
Xin-long Ma performed the experiments, reviewed drafts of the paper.
Hao-bo Jia, Rui Feng and Li-yan Xu contributed reagents/materials/analysis tools.
References
- Braun et al. (1998).Braun J, Bollow M, Remlinger G, Eggens U, Rudwaleit M, Distler A, Sieper J. Prevalence of spondylarthropathies in HLA-B27 positive and negative blood donors. Arthtitis and Rheumatism. 1998;1(41):58–67. doi: 10.1002/1529-0131(199801)41:1<58::AID-ART8>3.0.CO;2-G. [DOI] [PubMed] [Google Scholar]
- Braun & Sieper (2007).Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007;369:1379–1390. doi: 10.1016/S0140-6736(07)60635-7. [DOI] [PubMed] [Google Scholar]
- Brown et al. (1997).Brown MA, Kennedy LG, Macgregor AJ, Darke C, Duncan E, Shatford JL, Taylor A, Calin A, Wordsworth P. Susceptibility to ankylosing spondylitis in twins: the role of genes, HLA and the environment. Arthtitis and Rheumatism. 1997;10(40):1823–1828. doi: 10.1002/art.1780401015. [DOI] [PubMed] [Google Scholar]
- Burton et al. (2007).Burton PR, Clayton DG, Cardon LR, Craddock N, Deloukas P, Duncanson A, Kwiatkowski DP, McCarthy MI, Ouwehand WH, Samani NJ, Todd JA, Donnelly P, Barrett JC, Burton PR, Davison D, Donnelly P, Easton D, Evans DM, Leung H-T, Marchini JL, Morris AP, Spencer Chris CA, Tobin MD, Cardon LR, Clayton DG, Attwood AP, Boorman JP, Cant B, Everson U, Hussey JM, Jolley JD, Knight AS, Koch K, Meech E, Nutland S, Prowse CV, Stevens HE, Taylor NC, Walters GR, Walker NM, Watkins NA, Winzer T, Todd JA, Ouwehand WH, Jones RW, McArdle WL, Ring SM, Strachan DP, Pembrey M, Breen G, Clair DS, Caesar S, Gordon-Smith K, Jones L, Fraser C, Green EK, Grozeva D, Hamshere ML, Holmans PA, Jones IR, Kirov G, Moskivina V, Nikolov I, O’Donovan MC, Owen MJ, Craddock N, Collier DA, Elkin A, Farmer A, Williamson R, McGuffin P, Young AH, Ferrier IN, Ball SG, Balmforth AJ, Barrett JH, Bishop TD, Iles MM, Maqbool A, Yuldasheva N, Hall AS, Braund PS, Burton PR, Dixon RJ, Mangino M, Stevens S, Tobin MD, Thompson JR, Samani NJ, Bredin F, Tremelling M, Parkes M, Drummond H, Lees CW, Nimmo ER, Satsangi J, Fisher SA, Forbes A, Lewis CM, Onnie CM, Prescott NJ, Sanderson J, Matthew CG, Barbour J, Mohiuddin MK, Todhunter CE, Mansfield JC, Ahmad T, Cummings FR, Jewell DP, Webster J, Brown MJ, Clayton DG, Lathrop MG, Connell J, Dominiczak A, Samani NJ, Marcano CAB, Burke B, Dobson R, Gungadoo J, Lee KL, Munroe PB, Newhouse SJ, Onipinla A, Wallace C, Xue M, Caulfield M, Farrall M, Barton A, Bruce IN, Donovan H, Eyre S, Gilbert PD, Hilder SL, Hinks AM, John SL, Potter C, Silman AJ, Symmons Deborah PM., Thomson W, Worthington J, Clayton DG, Dunger DB, Nutland S, Stevens HE, Walker NM, Widmer B, Todd JA, Frayling TM, Freathy RM, Lango H, Perry JRB, Shields BM, Weedon MN, Hattersley AT, Hitman GA, Walker M, Elliott KS, Groves CJ, Lindgren CM, Rayner NW, Timpson NJ, Zeggini E, McCarthy MI, Newport M, Sirugo G, Lyons E, Vannberg F, Hill AVS, Bradbury LA, Farrar C, Pointon JJ, Wordsworth P, Brown MA, Franklyn JA, Heward JM, Simmonds MJ, Gough Stephen CL., Seal S, Stratton MR, Rahman N, Ban M, Goris A, Sawcer SJ, Compston A, Conway D, Jallow M, Newport M, Sirugo G, Rockett KA, Kwiatkowski DP, Bumpstead SJ, Chaney A, Downes K, Ghori Mohammed JR., Gwilliam R, Hunt SE, Inouye M, Keniry A, King E, McGinnis R, Potter S, Ravindrarajah R, Whittaker P, Widden C, Withers D, Deloukas P, Leung H-T, Nutland S, Stevens HE, Walker NM, Todd JA, Easton D, Clayton DG, Burton PR, Tobin MD, Barrett JC, Evans DM, Morris AP, Cardon LR, Cardin NJ, Davison D, Ferreira T, Pereira-Gale J, Hallgrimsdóttir IB, Howie BN, Marchini JL, Spencer Chris CA., Su Z, Teo YY, Vukcevic D, Donnelly P, Bentley D, Brown MA, Cardon LR, Caulfield M, Clayton DG, Compston A, Craddock N, Deloukas P, Donnelly P, Farrall M, Gough Stephen CL., Hall AS, Hattersley AT, Hill AVS, Kwiatkowski DP, Matthew CG, McCarthy MI, Ouwehand WH, Parkes M, Pembrey M, Rahman N, Samani NJ, Stratton MR, Todd JA, Worthington J, Mitchell SL, Newby PR, Brand OJ, Carr-Smith J, Pearce SHS, Gough SCL, McGinnis R, Keniry A, Deloukas P, Reveille JD, Zhou X, Bradbury LA, Sims A-M, Dowling A, Taylor J, Doan T, Cardon LR, Davis JC, Pointon JJ, Savage L, Ward MM, Learch TL, Weisman MH, Wordsworth P, Brown MA. Association scan of 14,500 nonsynonymous SNPs in four diseases identifies autoimmunity variants. Nature Genetics. 2007;39(11):1329–1337. doi: 10.1038/ng.2007.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cargill et al. (2007).Cargill M, Schrodi SJ, Chang M, Garcia VE, Brandon R, Callis KP, Matsunami N, Ardlie KG, Civello D, Catanese JJ, Leong DU, Panko JM, McAllister LB, Hansen CB, Papenfuss J, Prescott SM, White TJ, Leppert MF, Krueger GG, Begovich AB. A large-scale genetic association study confirms IL12B and leads to the identification of IL23R as psoriasis-risk genes. American Journal of Human Genetics. 2007;80(2):273–290. doi: 10.1086/511051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen et al. (2012).Chen C, Zhang X, Li J, Wang Y. Associations of IL-23R polymorphisms with ankylosing spondylitis in East Asian population: a new case-control study and a meta-analysis. International Journal of Immunogenetics. 2012;39(2):126–130. doi: 10.1111/j.1744-313X.2011.01067.x. [DOI] [PubMed] [Google Scholar]
- Cota et al. (2013).Cota GF, de Sousa MR, Fereguetti TO, Rabello A. Efficacy of anti-leishmania therapy in Visceral Leishmaniasis among HIV infected patients: a systematic review with indirect comparison. PLoS Neglected Tropical Diseases. 2013;7(5):e910. doi: 10.1371/journal.pntd.0002195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Di Meglio et al. (2013).Di Meglio P, Villanova F, Napolitano L, Tosi I, Terranova Barberio M, Mak RK, Nutland S, Smith CH, Barker JNWN, Todd JA, Nestle FO. The IL23R A/Gln381 Allele Promotes IL-23 unresponsiveness in human memory T-helper 17 cells and impairs Th17 responses in psoriasis patients. Journal of Investigative Dermatology. 2013;133(10):2381–2389. doi: 10.1038/jid.2013.170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dong et al. (2013).Dong H, Li Q, Zhang Y, Tan W, Jiang Z. IL23R gene confers susceptibility to ankylosing spondylitis concomitant with uveitis in a han Chinese population. PLoS ONE. 2013;8(6):e910. doi: 10.1371/journal.pone.0067505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duan et al. (2012).Duan Z, Pan F, Zeng Z, Zhang T, Wang S, Li G, Xu S, Xu J, Zhang L. Interleukin-23 receptor genetic polymorphisms and ankylosing spondylitis susceptibility: a meta-analysis. Rheumatology International. 2012;32(5):1209–1214. doi: 10.1007/s00296-010-1769-7. [DOI] [PubMed] [Google Scholar]
- Duerr et al. (2006).Duerr RH, Taylor KD, Brant SR, Rioux JD, Silverberg MS, Daly MJ, Steinhart AH, Abraham C, Regueiro M, Griffiths A, Dassopoulos T, Bitton A, Yang H, Targan S, Datta LW, Kistner EO, Schumm LP, Lee AT, Gregersen PK, Barmada MM, Rotter JI, Nicolae DL, Cho JH. A genome-wide association study identifies IL23R as an inflammatory bowel disease gene. Science. 2006;314(5804):1461–1463. doi: 10.1126/science.1135245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goei et al. (1985).Goei The HS, Steven MM, Van der Linden SM, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis: a comparison of the Rome, New York and modified New York criteria in patients with a positive clinical history screening test for ankylosing spondylitis. Rheumatology. 1985;24(3):242–249. doi: 10.1093/rheumatology/24.3.242. [DOI] [PubMed] [Google Scholar]
- Goldman & Schafer (2012).Goldman L, Schafer AI. Goldman’s cecil medicine. 24th edition. Amsterdam: Elsevier; 2012. pp. 1692–1694. [Google Scholar]
- Karaderi et al. (2009).Karaderi T, Harvey D, Farrar C, Appleton LH, Stone MA, Sturrock RD, Brown MA, Wordsworth P, Pointon JJ. Association between the interleukin 23 receptor and ankylosing spondylitis is confirmed by a new UK case-control study and meta-analysis of published series. Rheumatology. 2009;48(4):386–389. doi: 10.1093/rheumatology/ken501. [DOI] [PubMed] [Google Scholar]
- Miceli-Richard (2004).Miceli-Richard C. Significant linkage to spondyloarthropathy on 9q31-34. Human Molecular Genetics. 2004;13(15):1641–1648. doi: 10.1093/hmg/ddh179. [DOI] [PubMed] [Google Scholar]
- Nunez et al. (2008).Nunez C, Dema B, Cénit M, Polanco I, Maluenda C, Arroyo R, de las Heras V, Bartolomé M, de la Concha EG, Urcelay E, Martínez A. IL23R: a susceptibility locus for celiac disease and multiple sclerosis? Genes and Immunity. 2008;9(4):289–293. doi: 10.1038/gene.2008.16. [DOI] [PubMed] [Google Scholar]
- Pimentel-Santos et al. (2009).Pimentel-Santos FM, Ligeiro D, Matos M, Mourao AF, Sousa E, Pinto P, Ribeiro A, Sousa M, Barcelos A, Godinho F, Cruz M, Fonseca JE, Guedes-Pinto H, Trindade H, Evans DM, Brown MA, Branco JC. Association of IL23R and ERAP1 genes with ankylosing spondylitis in a Portuguese population. Clinical and Experimental Rheumatology. 2009;27(5):800–806. [PubMed] [Google Scholar]
- Rueda et al. (2008).Rueda B, Orozco G, Raya E, Fernandez-Sueiro JL, Mulero J, Blanco FJ, Vilches C, Gonzalez-Gay MA, Martin J. The IL23R Arg381Gln non-synonymous polymorphism confers susceptibility to ankylosing spondylitis. Annals of the Rheumatic Diseases. 2008;67(10):1451–1454. doi: 10.1136/ard.2007.080283. [DOI] [PubMed] [Google Scholar]
- Sáfrány et al. (2009).Sáfrány E, Pazár B, Csöngei V, Járomi L, Polgár N, Sipeky C, Horváth IF, Zeher M, Poór G, Melegh B. Variants of the IL23R gene are associated with ankylosing spondylitis but not with sjögren syndrome in Hungarian population samples. Scandinavian Journal of Immunology. 2009;70(1):68–74. doi: 10.1111/j.1365-3083.2009.02265.x. [DOI] [PubMed] [Google Scholar]
- Sherlock et al. (2012).Sherlock JP, Joyce-Shaikh B, Turner SP, Chao C-C, Sathe M, Grein J, Gorman DM, Bowman EP, McClanahan TK, Yearley JH, Eberl G, Buckley CD, Kastelein RA, Pierce RH, LaFace DM, Cua DJ. IL-23 induces spondyloarthropathy by acting on ROR-γt + MCD3 + CD4-CD8- entheseal resident T cells. Nature Medicine. 2012;18(7):1069–1076. doi: 10.1038/nm.2817. [DOI] [PubMed] [Google Scholar]
- Szabo et al. (2013).Szabo M, Sáfrány E, Pazar B, Melegh BI, Kisfali P, Poor G, Figler M, Szekanecz Z, Czirjak L, Melegh B. Marked diversity of IL23R gene haplotype variants in rheumatoid arthritis comparing with Crohn’s disease and ankylosing spondylitis. Molecular Biology Reports. 2013;40(1):359–363. doi: 10.1007/s11033-012-2068-z. [DOI] [PubMed] [Google Scholar]
- Vegvari et al. (2009).Végvári A, Szabó Z, Szántó S, Glant TT, Mikecz K, Szekanecz Z. The genetic background of ankylosing spondylitis. Joint Bone Spine. 2009;76(6):623–628. doi: 10.1016/j.jbspin.2009.02.006. [DOI] [PubMed] [Google Scholar]
- Wang et al. (2010).Wang X, Huang J, Lin Z, Liao Z, Chao L, Wei Q. Single-nucleotide polymorphisms and expression of IL23R in Chinese ankylosing spondylitis patients. Rheumatology International. 2010;30(7):955–959. doi: 10.1007/s00296-009-1085-2. [DOI] [PubMed] [Google Scholar]
- Zeng et al. (2008).Zeng Q, Chen R, Darmawan J, Xiao Z, Chen S, Wigley R, Le Chen S, Zhang N. Rheumatic diseases in China. Arthritis Research & Therapy. 2008;10(1):R17. doi: 10.1186/ar2368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhu, Yang & Gao (2009).Zhu X, Yang Z, Gao S. Doctoral dissertation. 2009. The candidate gene-association study of ankylosing spondylitis in Chinese north population the study of pathogenesis of DA2B. Available (in Chinese) at http://oversea.cnki.net/kcms/detail/detail.aspx?recid=&FileName=2009150883.nh&DbName=CDFD2009&DbCode=CDFD . [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.